Genetics Of Cleft Lip And Cleft Palate
Molecular Regulation Of The Development Of The Palate
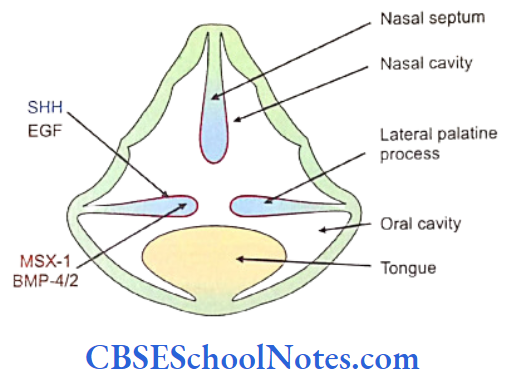
The palate is formed by the fusion of one median palatine process (primary palate) and two lateral palatine processes. The median palatine process is formed by the fusion of right and left medial nasal processes. The fused medial nasal processes form median part of upper lip, the part of upper jaw (which carries four incisors) and the primary palate.
Cleft Lip And Palate Risk Factors
The two lateral palatine processes are formed by shelf-like outgrowths from the maxillary processes in the 6th week of development. The growth of shelf-like process depends upon the interaction between ectoderm and mesenchyme. The following important genes play important role in the development of the palate. The sonic hedgehog (SHH), bone morphogenetic proteins (BMP), fibroblast growth factors (FGF) and members of the transforming growth factor B (TGF B) gene superfamily determine the formation of the palate (Carlson, 2004).
Cleft Lip And Palate Inheritance Pattern
- The mesenchyme of the palatal shelf expresses MSX-1 that stimulates BMP-4 signaling in the mesenchyme.
- This leads to expression of SHH signaling in the apical ectoderm.
- SHH further induces BMP-2 signaling in the underlying mesenchyme.
- Both BMP-2 and BMP-4 stimulate mesenchyme proliferation leading to the growth of the shelf like palate.
- Epidermal growth factor (EGF) stimulates glycosaminoglycan production within the palatal
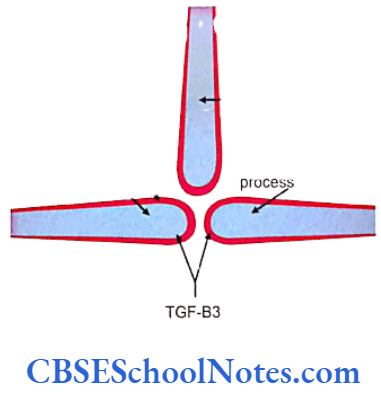

As the right and the left palatal shelves start fusing with each other in the midline, they are covered by epithelium. Some of these fused midline epithelial cells soon disappear by the process of apoptosis, while some other cells transform themselves from epithelial to mesenchymal cells.
Cleft Lip And Palate Risk Factors
Read and Learn More Genetics in Dentistry Notes
This transformation of cells is mediated due to the release of transforming growth factor-83 (TGF-B3). It is well known that TGF-B3 is expressed in the epithelium just before fusion. Mutation of TGF-B3 gene leads to formation of isolated cleft palate.
(The TGF-B3 knock out mouse exhibits an isolated cleft palate due to failure of palatal shelf fusion. Although the palatal shelves otherwise develop normally, they show a marked reduction in the filopodia present on the midline epithelial cell surface and show a down-regulation of chondroitin sulphate proteoglycan on the apical surface of the epithelia. Both of these are required for efficient midline epithelial adhesion).
Cleft Lip And Palate Risk Factors
Thus, it is clear that a tight control of a cascade of genes is required to complete normal palatogenesis. Anteriorly each palatal shelf joins with the primary palate. The fusion between two palatal shelves occurs anteroposteriorly and the process is completed by the 11th or 12th week.
Etiology Of Cleft Lip And Cleft Palate
Cleft lip with or without cleft palate (CL/P) and cleft palate (CP) are common birth defects that represent a major public health burden both in the social and medical contexts. The prevalence of CL/P varies from 0.3 to 2.5 per 1000 livebirths Worldwide. Cleft lip and palate (CLP) and cleft lip (CL) comprise 45 and 25% of all children respectively born with an oral cleft.
Environmental Causes Of Cleft Lip And Palate
The population-based studies have shown that 50 to 70% of CL/P births had no other major malformation while upto 30% are associated with other anomalies. 10 to 15% of all CL/P cases report a positive family history. The median cleft lip and lateral facial cleft are rare conditions.
The etiology of CL/P is complex and thought to involve genetic influences with variable interactions from environmental factors. The etiological factors of cleft lip and cleft palate can be grouped as under:

Nongenetic-This includes various environ- mental (teratogenic) risk factors which may cause CL/P.
Genetic-Genetic causes include:
- Syndromic: Here the cleft is associated with other malformations. Usually, it is due to a single gene (monogenic or Mendelian) disorder. The clefting may also occur due to other chromosomal abnormalities due to multiple gene involvement.
- Nonsyndromic: Here the cleft is mostly an isolated feature and occurs in the vast majority of individuals having a cleft-lip or palate (up to 70% cases). In this form of cleft neither a recognized pattern of malformation nor a known cause for the disorder can be identified.
Overall, environmental factors are considered much less important agents than genetic factors in the etiology of oral clefts.
Environmental Causes Of Cleft Lip And Palate
Nongenetic (Environmental) Risk Factors
Scientists have investigated many nongenetic environmental factors (teratogens) that increase the possibility of clefting. The lack of total concordance found in monozygotic twins (Spritz, 2001) indicated environmental etiology. Following is a list of these teratogens:
- Drugs
- Vasoactive drugs – Pseudoephedrine, aspirin, ibuprofen, amphetamine, cocaine.
- Anticonvulsant drugs – Phenobarbitol, trimethadione, valproate, and dilantin.
- Anticancer drug – Aminopterin.
- Antinausea or vomiting drug – Diphenhydrinate.
- Others – Corticosteroids, isotretinoin (Accutane), sulfasalazine, naproxen.
- Maternal smoking-Leads to embryonic hypoxia (Wyazynski et al, 1997).
- Alcohol intake-May also lead to fetal alcohol syndrome (Jones et al, 1973; Goslin et al, 2001).
- Maternal fever
- Exposure to chemicals-Xylene, toluene, acetone, benzene and pesticides.
- Nutrition-Folic acid and vitamin A deficiency during pregnancy (Hartridge et al, 1999). 7. Altitude Hypoxia (Castilla et al, 1999).
- Traumatic stress by releasing hydrocortisone.
Syndromic Form Of CL/P And CP
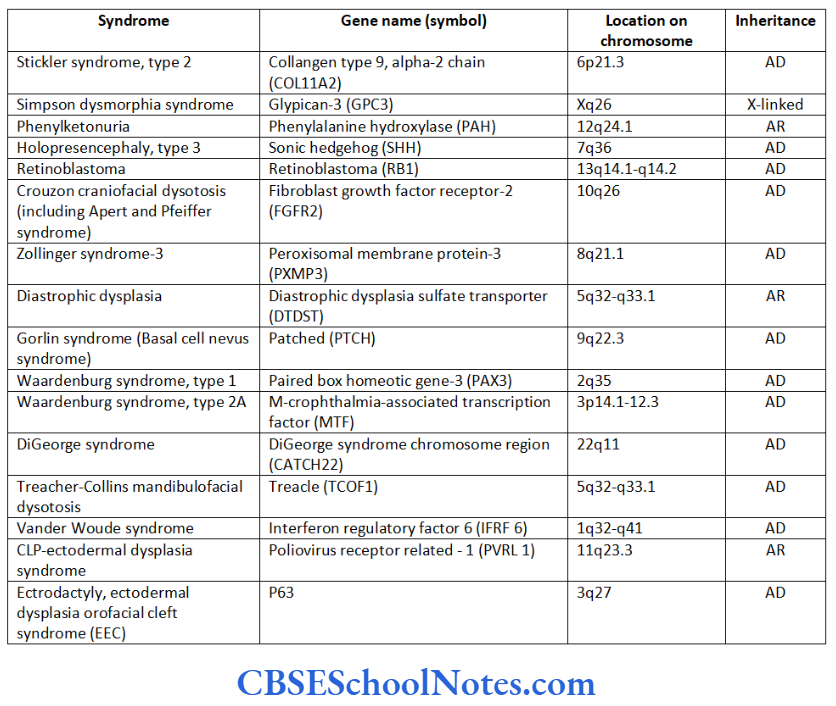
It is monogenic (Mendelian) form of clefting. This form of cleft is associated with syndrome (linked to varieties of other congenital anomalies). Since these syndromes are determined by the mutation in single gene they are of a high-risk type. Over 300 syndromes are known to be associated with cleft lip or palate as an associated feature. The syndromic CL/P can be subdivided into following categories (Table 12.1):
Environmental Causes Of Cleft Lip And Palate
- CL/P associated with syndromes caused by mutation in single gene.
- CL/P associated with syndromes caused by chromosomal abnormalities.
- CL/P associated with syndromes caused due to known teratogens.
- CL/P associated with syndromes whose cause is not known.
About 300 syndromes are known to have clefting of the lip or palate as an associated feature. The following table describes in brief a few well-known syndromic forms of CL/P.
Besides above-mentioned syndromes, X-linked Optiz syndrome (due to mutation in MIDI gene on chromosome Xp22) and mutation in the MSX1 gene and mutation in TBX22 genes are also known to be responsible for syndromic form of clefting.
Genetic Mechanism for Syndromic Form of Clefting
We have started, though recently, to understand genetic mechanisms implicated in some of the syndromic forms of CL/P.
DiGeorge syndrome (arising due to a deletion in chromosome 22q11) results from the failure of migration of neural crest cells in third and fourth branchial arches. These individuals also have associated CP (Seambler, 2000). We now know that the mutation in TBX22 gene encompasses almost all the common features of DiGeorge syndrome (Lindsay et al, 2001).
- The geneTCOF1 in Treacher-Collins syndrome encodes the protein called treacle. The exact function of treacle is unknown at present. It is speculated that treacle is involved in shuttling proteins between nucleolus and cytoplasm of the cell (Marsh et al, 1998). At present we do not know how this function can cause various malformations observed in Treacher-Collins syndrome.
- The mutation of SHH (Sonic hedgehog) gene leads to holoprosencephaly (Belloni et al, 1996). Holoprosencephaly is associated with midline defects like incomplete or deformed forebrain division, cyclopia, etc. The SHH signaling peptides play the role in midline patterning of human embryo.
- The genetic mechanism of CP in Stickler syndrome can be explained on the basis of defective collagen biosynthesis. Stickler syndrome (type I) occurs due to mutation in COL2A1 gene which encodes for type II collagen (Snead et al., 1999). Stickler syndrome (type II) has also been noted to occur due to mutation in the COL11A1 gene encoding type XI procollagen.
Nonsyndromic Clefting
Nonsyndromic cleft lip and/or palate (NSCLP) is a malformation characterized by an incomplete septation between the nasal and oral cavities without any associated anomalies. The distinction between syndromic and nonsyndromic clefting is very easy. In case of syndromic clefting there is always the presence of other associated anomalies in addition to CL/P and CP.
Role Of Genes In Cleft Lip And Palate
In cases of NSCLP the clefting is not associated with any other anomaly. Nonsyndromic orofacial clefts (OFC) are one of the most common malform- ations among livebirths and are composed of two separate entities: cleft lip with or without cleft palate (CL/P) and isolated cleft palate (CP).
The nonsyndromic clefting is said to be polygenic in nature. It is produced out of interaction between a number of genes; each producing a small effect that add up together to create the clefting. In other words, a cleft occurs when the total genetic liability of an individual reaches a certain minimal level termed the threshold.
It should be noted that every individual carries some genes that predisposes cleft formation but if the liability due to these genes is less than the threshold or the critical levels, no cleft results.
Role Of Genes In Cleft Lip And Palate
NSCLP is also said to be a complex multifactorial trait with interactions between genetic and environmental factors playing an important role in its causation. As the etiology of NSCLP is complex, many reports in the literature are contradictory (Murray, 1995).
Cleft Lip And Palate Inheritance Pattern
The genetics of nonsyndromic clefting has been investigated by following methods:
- Familial and Segregational Analysis: Many studies have shown an increased risk of clefting in siblings. The risk was found to be 30% higher in siblings as compared to normal population prevalence. This clearly shows that NSCLP is genetically determined. The mode of inheritance of nonsyndromic cleft lip with or without cleft palate (NSCLP) is still a matter of dispute. Many studies have indicated towards a multifactorial mode of inheritance while others are of opinion that the inheritance has a mixture of monogenic and multifactorial patterns.
- Twin Studies: NSCLP has shown higher concordance rates in monozygotic twins. The concordance rate in monozygotic twins is approximately 25 to 45% as opposed to 3-6% in dizygotic twins. On the other hand, lack of complete concordance was also found similar to any other multifactorial trait. This suggested involvement not only of genetic but also of environmental factors in the causation of non- syndromic clefting.
- Linkage Analysis: Linkage analysis is used to map a disease (mutant) gene to specific region on a chromosome. Today we know that mutations in many candidate genes or loci and their chromosomal locations are associated with non- syndromic clefting. (A candidate gene is a gene known to be located in a region of interest in the genome. The product(s) of a candidate gene has/ have biochemical or other properties suggesting that it may be the gene being related to a condition).
- Association studies: Both kinds of the approaches, i.e. candidate gene approach and genome wide association studies are reported for nonsyndromic clefting. Association studies have identified many genes for the clefting.
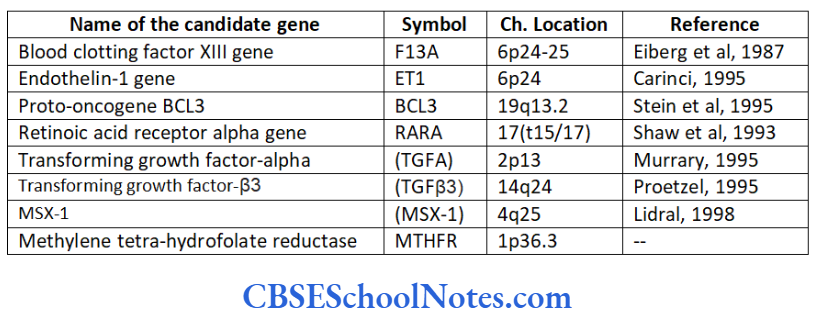
The following candidate genes have been identified as etiological factors of nonsyndromic CL/P.
It has been observed that some of the genes that are responsible for causing syndromic forms of clefting are also responsible for causing nonsyndromic form of clefting. These overlapping genes are MSX-1, IRF 6, PVRL1, CATCH22, TGFß3 and TBX22. It is now becoming apparent that the same genes contribute to the population of nonsyndromic clefts perhaps through variable penetrance or through the action of different modifiers.
Role Of Genes In Cleft Lip And Palate
In conclusion, one may say that genetic analysis of CL/P is quite confusing as mutation screening of specific candidate genes, association studies and even genome-wide scans have largely failed to reveal the exact molecular basis of human clefting. There is also overlapping of genes determining syndromic and non- syndromic forms of CL/P.
Greater efforts are necessary in order to have a complete picture of the main factors involved in lip and palate malformation. These elements will permit us to better understand and better treat patients affected by clefting.