
- Acids Bases And Buffer Notes
- Antidotes in Poisoning Notes
- Antimicrobials Resistance Notes
- Astringent: What is it, Uses, Benefits Notes
- Dental Products Notes
- Expectorants And Emetics Notes
- Haematinics Notes
- List of Gastrointestinal Agents Notes
- Major Extra And Intracellular Electrolytes Notes
- Pharmaceutical Inorganic Chemistry Practicals
- Radiopharmaceuticals Notes
- Types Of Impurities In Pharmaceutical Substances Notes
Pharmaceutical Inorganic Chemistry
Dental Products
Dental Products Introduction
Dental hygiene has been considered as important since long. In India poor dental health is a major problem and has been compounded by ignorance , poor literacy levels, habits like chewing of tobacco ,pan and pan masalas. In oerder to maintain dental hygiene, we have to take care of our teeth.
The teeth are accessory of digestive system. People use their teeth to bite and chew food. The long, sharp canine teeth tear up food, while the wide, flat, molar grinds mash up the
food.
It is the first step in the digestion of food. While chewing food, the tongue pushes it to the teeth and saliva helps in digestion and wets the food.
Tooth: Tooth consists of three layers of calcified tissue namely :
- Dentitle: Which surrounds the pulp cavity and extends through out the entire portion of tooth.
- Cementum : A layer covering the portion of tooth lying buried in the gum.
- Enamel : A white, hard material covering the portion of tooth projecting above the gum.
Vitamin A, C and D are all necessary for proper tooth formation. The deficiency of any of these can harm or affect the teeth. A number of inorganic compounds and their preparations are used in monitoring the oral and dental hygiene.
Most of them are Over-the-counter (OTC) products. Dental products include anticaries agent (dentrifices and fluoride salts), polishing agents and desensitizing agents.
Read and Learn More Pharmaceutical Inorganic Chemistry Notes
Anticaries Agent
Dental caries is the medical term for tooth decay or cavities. It is caused by specific type of bacteria. They produce acid that destroys the tooth’s enamel and the layer under it, the
dentin.
Many different types of bacteria normally live in the human mouth. They build up on the teeth in a sticky film called plaque. This plaque also contains saliva, bits of food and other natural substance.
Plaque forms most easily in certain parts. These include cracks, pits or grooves in the back teeth, in between teeth and near the gum line. Some of the plaque bacteria turn sugar and carbohydrate (starches) of the food into the acids.
The acid dissolves minerals in the hard enamel that covers the tooth crown. The enamel erods or develops spits. They are too small to set at first. But they get larger over time. Adds can also seep through pores in the enamel.
This is how decay begins in the softer dentin layer, the main body of the tooth. As the dentin breaks down, the enamel over it can collapse, forming a cavity. A mucin-rich saliva has less cleansing action on tooth and therefore, helps to the development of caries.
Poor nutrition of the infant and the mother at the time of infancy and childhood results in poor architecture of the teeth which become suspectible to the development of caries in the early age.
Dental caries can be prevented and oral and dental hygiene can be maintained with the help of dentrifices. Dentrifices are the products that enhance the removal of stains and dental plaque by the tooth brush.
The most accepted-approach to prevent caries including flossing and brushing accompanied by administration of fluoride and brushing accompanied by administration of fluoride either internally or topically the teeth.
Newer devices also have been developed to detect tooth decay. They are useful in some situations and rhey do not spread decay. The one most commonly used dental caries is a liquid dye or stain the dentist brushes the non toxic dye over your teeth,then rinse it off with water .
It rinses always cleanly from healthy areas but sticks to the decayed areas. Some dentist also use high tech devices such as layers to detect cavities. Under many conditions,these devices can detect very early tooth decay,which actually can be reversed.
Role Of Fluoride
Fluoride is anticariogenic as it replaces the hydroxyl ion in hydroxy apatite with the fluoride ion to form fluorapatite in the outer surface of the enamel. It can be administrated by two
routes- Orally and Topically.
Fluoride in low concentration (1-2 parts per million), if present in drinking water, also causes, the decrease in development of incidence of caries in the population. Fluoride can also be administrated orally as Sodium Fluoride tablets or drops added in water or fruit juice. But it is not beneficial as such.
A 2% aqueous solution of sodium fluoride and 8% solution of stannous fluoride are extensively used for topical application. Two such well established fluorides are Sodium fluoride and Stannous fluoride.
Role Of Phosphate
Inorganic phosphate salts can also be useful in the prevention of dental caries. Phosphate ions are needed for stronger bone as well as for healthy teeth. Soluble salts of phosphate
such as sodium monohydrogen phosphate, sodium dihydrogen phosphate can cause caries reduction in men. It is also used as cleansing agent.
Sodium Fluoride
Chemical Formula : NaF Molecular Weight: 41.99
It is having not less than 98.0% of NaF and not more than 100.5% of NaF, calculated with refrence to the dried substance.
Preparation
It is prepared by reacting hydrofluoric acid with Sodium Carbonate. Sodium fluoride being not very soluble precipitates out.

Alternatively, the another method involves the double decomposition of Calcium Fluoride with Sodium Carbonate.

Here, insoluble calcium carbonate can be removed by filtration.
Properties
It occurs as colourless, odourless crystals or as white powder. It is soluble in water but is insoluble in alcohol. On acidification of salt solution, hydrofluoric acid is produced. This is weak acid and is poisonous. Aqueous solution of salt yields alkaline solution.
Storage
Aqueous solution of Sodium Fluoride corrodes ordinary glass bottles and hence the solution should be prepared in distilled water and stored in dark, pyrex bottles.
Pharmaceutical uses
It is used in the prevention of dental carles because ol Its lluorldo Ion concentration. tooth constituent of some insecticides and rodenllcides. It Is used In tin* preparation o a
pastes which constitutes about 75% of Sodium Fluoride and 25% of glycerol.
Usual dose
2.2 mg (equivalent to lmg of fluoride Ion)
Applications
1.5-3.0 ppm in drinking water.
Stannous Fluoride
Molecular formula : SnF2 Molecular Weight: 156.69
Synonym: Tin fluoride
Methods of preparation
It is prepared by evaporating a solution of stannous oxide, In Hydrofluoric acid In the absence of oxygen.
Stannous fluoride is prepared by heating Stannous Oxide with gaseous hydrofluoric acid in the absence of oxygen.

Properties
It occurs as a white crystalline powder with a bitter saline unpleasant taste. It Is freely soluble in water; practically insoluble in alcohol, chloroform and ether. Aqueous solution
decomposes within a few hours with the formation of a white precipitate, they slowly attack glass.
Uses
It is used as a preventive for dental caries.
Dentrifices Or Cleaning Agents
A dentrifice is a substance used with a tooth brush for the purpose of cleaning the accessible surfaces of the teeth. Commercial dentrifices are available in the form of pastes and powders. Many dentrifices contain flavours and soap or detergent.
The powders and pastes contain abrasives such as Calcium Carbonate, Calcium Phosphates, Calcium Sulphate, insoluble Sodium Metaphosphate, Calcium Carbonate and Sodium Chloride.
Toothpastes contain liquids (e.g. glycerin, propylene glycol, sorbitol solution, water and alcohol) and thickners (e.g. starch, trageanth, algin and cellulose derivative). Dentrifices or tooth pastes are responsible for physically removing plaque and debris.
They may also contain some sweetening agents. Certain individual may need an abrasive containing dentrifices. The abrasive dislodges the dental plaques and helps to remove them. It should be mildly abrasive for this purpose.
Calcium Carbonate
Chemical Formula: CaC03 Molecular Weight. : 100.09
Synonym
Precipiated Chalk, Precipitated Calcium Carbonate. It is the most abundant and widely distributed in nature as limestone, iceland spar, olomite and shells of sea animals.
Method of Preparation
Calcium carbonate when come in contact with sodium carbonate leads to the formation of calcium carbonate and sodium chloride

Physical Properties
Calcium carbonate occurs as a white, odourless, tasteless, micro crystalline powder which is stable in air. It is practically soluble in dilute hydrochloric acid and nitric acid but is insoluble in water and alcohol.
It dissolves in aqueous phosphoric acid & the solution on evaporation deposits crystals of calcium dihydrogen.
Assay
This is complexometric assay. The sample is dissolved in water and hydrochloric acid and a known excess of 0.1M disodium edetate is added & diluted with watewr. It is neutralised
with strong ammonia solution, ammonia buffer pH 10 and mordant black II mixture are added and the titration is continued till be change of colour from pink to full blue takes place
at the end point.
Calcon mixture consist of calcon (mordant black) and freshly ignited anhydrous sodium sulphate. It gives a purple-red colour with calcium ions in alkaline solution.
Uses
It is used externally as dentrifice, as a dental cleaning polishing agent for most tooth paste and tooth powders. It is used as insecticides. Due to its fast action, calcium carbonate is used
as an antacid, as a calcium supplement in deficiency states; as a food additive. It is also used in the preparation of homoepathic medicine.
Desensitizers
The desensitizers tend to decrease hypersensitivity of the teeth. When applied to their outer surface, especially where erosion has occurred near the gum line, they reduce the senstivity
of the teeth to heat and cold. Inorganic compounds of desensitizers are Strontium Chloride and Zinc chloride
Zinc Eugenol Cement
Zinc Oxide Eugenol (ZOE) is material created by the combination of Zinc Oxide and eugenol contained in oil of cloves. An acid-base reaction takes place with the formation of zinc
eugenol chelate. The reaction is catalyzed by water.
Advantages :
- Dimensional stability
- Good surface
Disadvantages :
- Eugenol allergy in some patients.
- Cannot be used in very deep undercuts.
Composition:
- Liquid
- Eugenol (react with zinc oxide)
- Olive oil (plasticizer)
- Powder
- Zinc oxide (principal ingredient)
- Zinc stearate (accelerator, plasticizer)
- Zinc acetate (accelerator, improve strength)
- White rosin (to reduce brittleness of set cement)
Properties
It is the cement of low strength, low abrasive resistance, and low flow after setting, so it is used for temporary filling not be more then few days.
It has adhesive effect on exposed dentin. It is least irritating than other dental cements.
Uses
- For temporary fillings.
- Pulp-capping agents.
- Zinc oxide eugenol is used as an antimicrobial additive in paint.
- It is used as an impression material during construction of complete dentures and is used in the mucostatic technique of taking impressions.
Dental Products Very Short Answer Questions
Question. 1. Define Dentrifices?
Answer. A Dentirifice is a substance used with a tooth brush for the purpose of cleaning the accessible surface of the teeth.
Question.2.Define Dental Caries?
Answer. Dental caries is the medical term for tooth decay or cavities.
Question 3. What is the role of fluoride?
Answer. Fluoride removes the anticaries as it replaces the hydroxyl ion in hydroxyapatite with the fluoride ion which form fluoroapatite.
Question 4. Does the desensitizer increase or decrease the hypersensitivity of teeth?
Answer. Desensitizer tends to decrease the hypersensitivity of teeth.
Question.5.What is the molecular formula of Dicalcium Phosphate?
Answer.CaHPO4.
Question.6.Name any two inorganic compounds which are used as dental caries?
Answer.
Sodium monohydrogen phosphate
Sodium dihydrogen phosphate
Question 7.What is the another name of sodium metaphosphate?
Answer. Sodium metaphosphate is also known as Madrell’s salt.
Question 8.How is stannous fluoride prepared?
Answer. Stannous fluoride is prepared by heating stannous oxide with gaseous hydrofluoric acid in the absence of oxygen.
SnO + 2HF- ->SnF2 + H20
Question 9. How can dental caries be prevented?
Answer. Dental caries can be prevented by using dentrifices.
Question 10. Name the two inorganic fluoride compounds used in dental products?
Answer.
Sodium fluoride
Stannous fluoride
Dental Products Fill In The Blanks
1. Dentrifices are the compounds that are used for ……………
Answer: Cleaning teeth and. gums
2. The cleaning action of dentrifices depends on their……………….
Answer: Abrasives
3. To prevent dental caries tooth paste containing………………………… should be used.
Answer: Sodium fluoride
4. Soluble salts of phosphate are ……………………..
Answer: Sodium monohydrogen phosphate, Sodium dihydrogen phosphate
5. …………………….. is a medical term for tooth decay or cavities.
Answer: Dental earies
6. Cone, of fluoride in drinking water is…………………
Answer: 1.5–3.0 ppm
7. Stannous fluoride is prepared by heating………………with …………….. in the absence of oxygen.
Answer: Stannous oxide, hydrofluoric acid
8. Chemical formula of Sodium fluoride is ……………and Stannous fluoride is………………..
Answer: NaF and SnF2
9…………….. reduce the sensitivity of the teeth to heat and cold.
Answer: Dentrifices
10. Precipitated chalk is…………………………
Answer: Calcium carbonate
Dental Products Multiple Choice Questions
Question 1. Fluoride inhibits carries formation via
- Downward acid solubility of enamel
- Bacterial inhibition
- Both a) and b)
- None of these
Answer: Both a) and b)
Question 2. Hydroxyapatite is a mixture Ca2+ salt of
- CO3″
- P04′
- OH
- All of these
Answer: All of these
Question 3. Dental caries is a medical term of
- Cleaning action
- Polishing action
- Tooth decay or cavities
- None of these
Answer: Tooth decay or cavities
Question 4. Fluoride can be administrated either
- Orally
- Topically
- Both a) and b)
- None of these
Answer: Both a) and b)
Question 5. Sodium Metaphosphate is also known as
- Precipitated chalk
- MadrelTs salt
- Both a) and b)
- None of these
Answer: MadrelTs salt
Question 6. Desensitizers tend to
- Downward hypersensitivity of the teeth
- Upward hypersensitivity of the teeth
- Bacterial inhibition
- None of these
Answer: Downward hypersensitivity of the teeth
Question 7. Example of Desensitizer is
- Zinc chloride
- Sodium fluoride
- Stannous fluoride
- Calcium carbonate
Answer: Zinc chloride
Question 8. ‘Butter of Zinc’ is also known as
- Zinc chloride
- Zinc carbonate
- Zinc bicarbonate
- None of these
Answer: Zinc chloride
Question 9. Which vitamin is necessary for tooth formation?
- Vitamin A
- Vitamin C
- Vitamind D
- None of these
Answer: None of these
Question 10. Phosphate is used as .
- Cleansing agent
- Flossing agent
- Removing stains
- All of the above
Answer: Cleansing agent
Types Of Impurities In Pharmaceutical Substances
Types Of Impurities In Pharmaceutical Substances Introduction
Pharmaceutical Chemistry is the branch of chemistry which deals with the study of medicines. It includes the main branches of chemistry namely inorganic chemistry, organic chemistry, medicinal chemistry, analytical chemistry and physical chemistry.
The term “Inorganic Chemistry” in shorter sense is called “chemistry of everything else”. It deals with the study of inorganic compounds containing their molecular weight, molecular formula, occurrence, method of preparation, physical and chemical properties, assay and uses as pharmaceutical aids, therapeutic and diagnostic agents.
It has accomplished rapid progress in understanding the properties of all chemical compounds. It is of fundamental importance not only as a basic science but also as one of the most useful source of modem technologies.
The pharmaceutical substances used in the treatment of diseases may be procured from the natural sources such as minerals, salts, purified inorganic chemicals, calcined inorganics (ash or bhasma), plants, animals, microbes and from synthetic chemicals.
In ancient times mercury, gold, copper and silver were also used in medicine. The specification for each pharmaceutical is listed in Pharmacopoeia.
Pharmacopoeia
The term Pharmacopoeia is derived from the Greek word “pharmakon” means drug or medicine and “poiein” is to make. Drugs manufactured in India have to be labelled with the mandatory non-proprietary name with the suffix “I.P”. It provides a collected list of drugs and medicinal substances along with directions for making preparation from them.
Many countries are now publishing pharmacopoeias of their own and by this they are able to control the standards of the drug produced in their countries and also the standards of the drugs imported into their countries and ensure the health of their people.
A drug or a medicinal chemical included in a pharmacopoeia is termed as official and the sections dealing with official drugs, preparation and substances are known as monograph.
Read and Learn More Pharmaceutical Inorganic Chemistry Notes
History of pharmacopoeia
Indian Pharmacopoeia (I.P.)
In India, the first pharmacopoeia had been publishes as “Bengal Pharmacopoeia in 1844.
The Government of India constituted a permanent Indian Pharmacopoeia Committee in 1948 for preparing Indian Pharmacopoeia under the chairmanship of Dr. B. N. Ghosh. The first edition of I.P. was publishes in 1955, followed by a supplement in 1960 which contains large number of crude drugs and their preparation.
List of Publication of various Edition of Indian Pharmacopoeia

Salient features of First edition of Indian Pharmacopoeia (1955):
- Covers 986 monographs.
- Titles of monograph in Latin language.
- Weight and measures in metric system.
- Doses expressed in both metric and English system.
- List of preparations given at the end of some of the monographs.
- Abbreviated titles used.
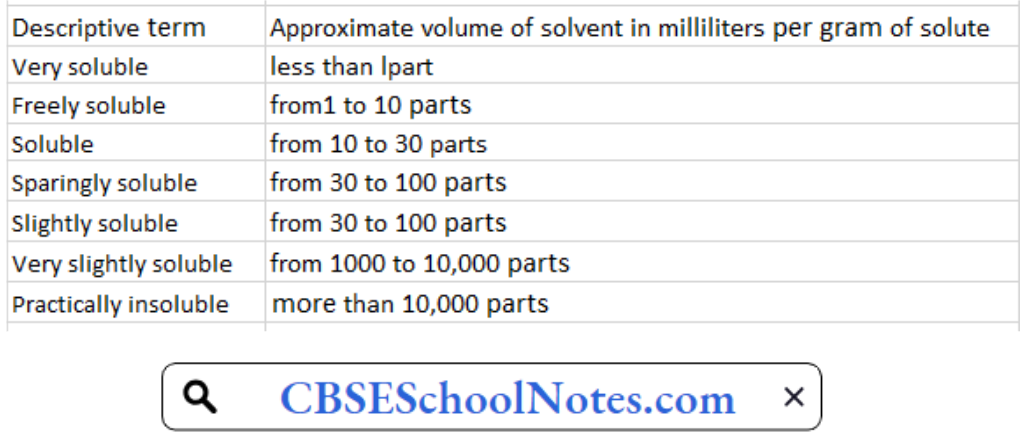
- Descriptive terms used for solubility instead of exact solubility.
Salient features of Second edition of Indian Pharmacopoeia (1966):
- Published in 1966 and its supplement was published in 1975.
- Titles of monographs changed from Latin to English.
- Name of drug comes first in title e.g. Aminophylline Injection.
- Solubility expressed in parts of solvent per unit part of solute.
- 93 new monographs were added.
- New analytical techniques had been included.
- Test for sterility had been modified to detect fungi.
- ‘Usual Strength’-a heading used to represent strength of tablet had been used.
- 214 monographs from I.P. 55 were deleted.
Salient features of Third edition of Indian Pharmacopoeia (1985):
- Published in 1985 with two volumes and nine appendices.
- 260 new monographs were added and 450 were amended.
- New analytical techniques (Flame photometry,
- Electrophoresis, Fluorometry etc.) had been introduced.
- Dissolution had been introduced.
- Microbial limit tests being prescribed for liquid preparation.
- Gas liquid chromatography had been recognized.
- Determination of viscosity have been modified involving use of Ostwald viscometer.
- New appendix “Water for Pharmaceutical Use” had been introduced.
- Drugs renamed and some drugs had been omitted.
- Addendum I to I.P. 1985 was published in 1989, where 46 new monographs were added and 126 amended.
- Addendum II to I.P. 1985 was published in 1991, where 62 new monographs were added and 110 amended.
Salient features of Fourth edition of Indian Pharmacopoeia (1996):
- Published in 1996 under the chairmanship of Dr. Nityan and along with Dr. Parvinder Singh followed by its addendums in 2000 and 2003.
- Contains 1149 monographs and 123 appendices in two volumes.
- Computer generated structural formulae used.
- Infrared and Ultra Violet absorption spectrophotometric tests for identification of drug were added.
- Included 294 new monographs and 110 monographs were deleted.
- High Pressure Liquid Chromatography (HPLC) had been used as analytical method.
- Bacterial endotoxin test were introduced.
- Quantitative method for determining particulate matter in injectable preparation being replaced by qualitative.
- Monographs of ORS, ORS-bicarbonate had been omitted out and ORS-citrate formula had been added.
- Specific biological assay and test were transferred to individual monographs.
- The veterinary supplement of I.P. 1996 contains 208 monographs and four appendices.
Salient features of Fifth edition of Indian Pharmacopoeia (2007):
- Published in 2007 followed by its addendum in 2008.
- Presented in three volumes.
- Volume one contains general notices, structure of IPC, Acknowledgements.
- Volume two and three contains general monographs on dosage forms, drug substances and pharmaceutical aid.
Salient features of Sixth edition of Indian Pharmacopoeia (2010):
- Published in 2010 followed by its addendum in 2012 and DVD of I.P. 2010 was also available.
- Released on 27th December 2011 by Mr. P.K. Pradhan in presence of Mr. L. C. Goyal and Dr. Arun Kumar.
- Consists of three volumes.
- Volume one contains Notices, preface, structure of IPC, general chapters.
- Volume two contains general monographs on dosage form, drug and pharmaceutical aid (A to M).
- Volume three contains general monographs on dosage form, drug and pharmaceutical aid (N to Z).
- Products of biotechnology, herbal products, and additional antiretroviral drugs were included.
- Standards for new drug under NHP were added.
- Microbial contamination chapter updated.
- Chapter on NMR is incorporated in appendices.
- New chapter on Liposomal products is also added.
Salient features of Seventh edition of Indian Pharmacopoeia (2014):
- Published in 2014 and presented in four volumes.
- Contain 2567 monographs of drugs out of which 577 are new monographs.
- Introduced 19 radiopharmaceutical monographs for the first time.
- 10 antibiotic monographs, 31 herbal monographs, 5 vaccine, and immunosera for human use, 6 insulin products and 7 biotechnological products with 19 new general chapters were included.
Salient features of Eighth edition of Indian Pharmacopoeia (2017):
The latest Edition of Indian Pharmacopoeia, IP-2018 has been released on 29th September, 2017 by Sh. C.K. Mishra, Secretary Health & Family Welfare, Govt, of India.
IP-2018 has been brought out in 4 Volumes incorporating 220 new monographs (Chemical Monographs (170), Herbal Monographs (15), Blood and Blood related products (10), Vaccines and Immunosera for Human use monographs (02), Radiopharmaceutical monographs (03), Biotechnology Derived Therapeutic Products (06), Veterinary monographs
(14)), 366 revised monographs and 7 omissions.
Salient Features of IP-2018:-
- General Chemical tests & Thin Layer Chromatography (TLC) for identification of an article have been almost eliminated and more specific infrared, ultraviolet
spectrophotometer and HPLC tests have been given emphasis. The concept of relying on published infrared spectra as a basis for identification has been continued. - The use of chromatographic methods has been greatly extended to cope with the need for more specificity in assays and in particular, in assessing the nature and
extent of impurities in ingredients and products. - Most of the existing Assays and Related Substances Test methods are upgraded by liquid chromatographic in view to harmonize with other International Pharmacopoeia.
- Pyrogen test have been replaced by Bacterial Endotoxin test (BET) in parenteral preparations and other monographs.
- For ease of access to make Pharmacopoeia more user friendly, Index has been incorporated in Volume-I along with that already existing in Volume-IV of IP.
- 53 New Fixed Dose Combination (FDC’s) combination monographs have been included, out of which 25 FDC monographs are not available in any Pharmacopoeia.
- General Chapters on Volumetric Glassware, Conductivity, Dissolution test, Disintegration test, Dimensions of Hard Gelatin Capsule Shells etc. have been revised.
- For Controlling the Microbial quality of all the medicinal product general chapter on Maintenance, Identification, Preservation and Disposal of Microorganism have been
revised.
British Pharmacopoeia (B. P.)
British Pharmacopoeia was published by the health ministers of the United Kingdom. The first edition of B.P. was published in 1864 which consists of two parts “Materia Medica” and
“Preparation and Compound”. Australia and Canada are two of the countries that have adopted the B.P. as their national standard book. The various publication of B.P. comes out in subsequent years as under:
- 1867: Second edition.
- 1885: Third edition.
- 1898: Fourth edition.
- 1914: Fifth edition.
- 1932: Sixth edition.
- 1948: Seventh edition. It contains official 49 tablet preparations and official 75 injections.
- 1951: Addendum to BP 1948 was published.
- 1953: Eighth edition. In this title of drug and preparation was in English instead of Latin and metric system was used.
- 1955: Addendum to BP 1953 was published.
- 1958: Ninth edition.
- 1960: Addendum to BP 1958 was published. It includes monographs on radioactive chemicals.
- 1963: Tenth edition.
- 1968: Eleventh edition.
- 1973: Twelfth edition.
- 1980: Thirteenth edition.
- 1988: Fourteenth edition.
- 1988, 1990, 1991 & 1992: Four addendums were published.
- 1993: Fifteenth edition.
- 2000: Sixteenth edition. It contains veterinary drugs.
The other editions were published in 2004, 2005, 2007-2009 (published in six volumes), 2010 and 2014. The current edition was published in 2015 which includes almost 3500 monographs spread out in six printed volumes.
United State Pharmacopeia (U.S.P.)
United States Pharmacopeia and the National Formulary (USP-NF) are recognized as official compendia for determining the standard of pharmaceutical products. The first USP was published in 1880 under the authority of United State Pharmaceutical Convention (USPC).
National Formulary (NF) was published first in 1888 under the authority of the American Pharmacists Association (APhP). After 1975, both USP and NF are published by USPC in a
combined volume as USP-NF.
USP-NF was published at every ten years interval from 1820-1942. But from 1942-2000, it was published at an interval of five years. After 2000, USP-NF
has been published annually. USP 40 – NF 35 will be officially released in year 2017.
British Pharmaceutical Codex (B.P.C.)
This book was prepared as a reference book for the use of medical practitioners and dispensing pharmacists. In 1903, Pharmaceutical society of Great Britain came up with BPC. The first edition of the BPC was published in 1907.
The subsequent editions were published in 1911, 1923, 1934, 1949, 1954, 1959, 1963, 1968 and 1973. From eleventh edition 1979 onwards BPC was considered as Pharmaceutical Codex only. It comprises of general monographs of drugs and also provides standards of medicaments and materials that not included in BP and British National Formulary (BNF).
Extra Pharmacopoeia (MARTINDALE)
This pharmacopoeia was first issued in 1883 by William Martindale and now it was published by pharmaceutical society of Great Britain.
Pharmacopoeial description
Practically most of the pharmacopoeia consists of three main sections namely:
- General notices
- Monographs of the official drugs
- Appendices
General notices: It is useful information of pharmaceutical progress since last edition as it summarizes the various changes including additions/deletions in the present edition
compared to last edition.
Monographs of the official drugs: The word “Monograph” means the written study of a subject. It is derived from a Greek word (mono=single, grapho = to write). As the medicinal substances are to be used for the cure and prevention of diseases, therefore,these are considered as very important and hence their written studies appear as monograph .
- Titles:- Monograph titles are in English and French in the respective versions and there is a Latin subtitle. It includes the main names of the substance.
- Synonyms: Common names, if any, of the substance.
- Chemical formula and Molecular Weight: If necessary graphic, molecular formula and molecular weight are given at the beginning of the monograph.
- Chemical names:- It is given in the monograph as employed by the International Union of Pure and Applied Chemistry (IUPAC). It does not constitute for the analytical standards such as UV, NMR, IR etc.
- Category: It indicates its use in pharmacy/medicine. It represents pharmacological action of the substance such as antifungal, antimicrobial, anti inflammatory, etc.
- Doses: Doses mentioned in the Indian Pharmacopoeia (I.P.) represent the average range of quantities suitable for adults.
- Description: This include a statement about its general physical properties , i.e. whether the substance is a liquid or solid, coloured or colourless, amorphous or crystalline, its taste, etc.
- Solubility: In terms of solubility the terms used have the following significance referred to a temperature between 15ÿC and 25ÿC. The term “partly soluble” is used to describe a mixture where only some of the components dissolve.
The term “miscible” is used to describe a liquid that is miscible in all proportions with the stated solvent. - Standards: Indian Pharmacopoeia (I.P.) prescribes the standard of purity and strength in the monograph of almost all official substances. A substance is not deemed to be of
standard quality unless it complies with the requirements stated under ‘standard’ of its monograph. - Identification: It includes some specific and non-specific test of the substance.
- Test for purity: Indian Pharmacopoeia (I.P.) prescribes tests for purity of almost all the offcial substances. These tests include boiling point, melting point, limit test for chlorides, sulphates, iron, aresenic, lead, heavy metals, pH of solution, loss on drying, specific optical rotation, etc.
- Assay: Assay is used for the quantitative determination of principal ingredients of the official substances and their preparations.
- Storage:-Indian Pharmacopoeia prescribes the conditions for storage in such a way as to prevent contamination and, as far as possible, deterioration. Where special conditions of storage are recommended, including the type of container and limits of temperature, they are stated in the monograph. The following expressions are used in monographs under Storage with the meaning shown.
- In an airtight contaitter means that the product is stored in an airtight container. Care is to be taken when the container is opened in a damp atmosphere. A low moisture content may be maintained, if necessary, by the use of a desiccant in the container provided that direct contact with the product is avoided.
- Protected from light means that the product is stored either in a container made of a material that absorbs light sufficiently to protect the contents from change induced by such light or in a container enclosed in an outer cover that provides such protection or stored in a place from which all such light is excluded.
- Labelling When the term “label” is used in the Pharmacopoeia, the labelling statements may appear on the container, the package, a leaflet accompanying the package or a certificate of analysis accompanying the article, as decided by the competent authority.
Appendices: General notices and monographs are followed by comprehensive section of appendices.
Appendix- I: It describes about the apparatus needed for various pharmacopoeial tests and assays.
Appendix-ll: It describes about biological tests and assays.
Appendix-Ill: It contains details of various chemical tests and assays.
Appendix-lV: It contains details of microbiological tests and assays.
Appendix-V: It includes physical tests and determinations like loss on drying, pH determination, melting range, etc.
Appendix-Vl: It describes useful directions on cleaning glassware’s.
Appendix-VIl: It describes the reagents and solutions needed for various tests and assays.
Appendix-VIII: It describes about the reference substances.
Appendix-IX: It describes the names and symbols used in the pharmacopoeia and their atomic weights have been described.
Impurity
Impurity is defined as any substance coexisting with the original drug, such as starting material or intermediates or that is formed, due to any side reactions. Chemical purity means
freedom from all foreign materials. Purification of chemicals is expensive and therefore purifying a substance to much higher degree is necessary.
Effects of Impurities
Pure substances are difficult to get and some amount of impurity is always present in the material. So the impurities which are present in the substances may have the following effects:
- Impurities may lower the shelf life of the substances.
- Therapeutic effect can be decreased.
- Impurities may bring about incompatibility with other substances.
- Impurities may cause1difficulties during formulations and use of the substances.
- Sometimes Impurities changes the chemical and physical properties of the substances.
- Shows toxic effect after a certain period.
Sources of Impurity:
A compound having foreign materials is said to be impure. The origin of impurities in drugs is from various sources and phases of the synthetic process and preparation of pharmaceutical dosage forms. Majority of the impurities are characteristics of the synthetic route of the manufacturing process. The pharmaceutical preparation should be free from toxic and other impurities.
The impurities commonly found in medicinal preparations are:
- Impurities due to which substances become incompatible.
- Due to colouring or flavouring substances, e.g., Sodium Salicylate.
- Humidity.
- Chemical and physical properties.
The various sources of impurities in pharmaceutical substances are as follows:
Raw Materials Used in the Manufacturing of Pharmaceutical Process: The source of pharmaceutical substances are either natural or synthesized from chemical starting materials. It is essential to verify the identity of the source material and its quality otherwise it contaminate the final product. Example: lead and heavy metals are found as impurities in many sulphide ores, Rock salt used for the preparation of sodium chloride is contaminated with small amounts of calcium and magnesium chlorides.
Reagents employed in the manufacturing process: Pharmaceutical substances are either isolated from natural sources (mineral sources, plants, animals and microbes) or synthesized from chemical starting materials. If reagents are employed in the manufacturing process are not completely removed by washing, these reagents may be present in final products.
Example: e.g., Magnesium impurities are found in calcium minerals, aluminum ores are usually accompanied by alkali and alkaline earth compounds.
Solvents: Water is the most commonly used solvents in the preparation of inorganic pharmaceuticals. Different types of water containing different types of impurities. Various types of water are:
Tap water: Containing impurities of Magnesium, sodium, calcium, chloride, sulphates and carbonates. +
Softened water: It is prepared from tap water nut it contains more of sodium and chloride ions as impurities.
Demineralized water: It is prepared by ion exchange and it is free from Magnesium,sodium, calcium, chloride, sulphates and carbonates impurities. It contains pyrogens, bacteria and organic impurities.
Distilled water: This water is free from all inorganic and organic impurities. It is best solvent for pharmaceutical preparations.
Action of reagents on reaction vessels: Reaction vessels used in the manufacturing process may be metallic such as iron, cast iron, galvanized iron, copper, silver, aluminium, nickel, zinc and lead.
Atmospheric contamination during manufacturing process: Atmosphere may contain dust (sulphur, aluminum oxide, silica, soot etc.) and some gases like carbon dioxide, sulphur dioxide, arsine and hydrogen sulphide. These may contaminate the final product during the manufacturing process.
Chemical process used in the manufacture: Various chemical reactions such as oxidation, nitration, reduction, halogenations, hydrolysis are involved for the synthesis of drugs. In these chemical reactions various chemicals and tap water is used it is often having Mg+2, Ca+2 and Ch, which are generally found in the substance which is being manufactured.
Defects in the manufacturing process : Defects like incompleteness, pH, pressure, temperature and imperfect mixing in various manufacturing processes produce impurities in chemical compounds.
To prevent these impurities many test such as limit test are carried out to lower the impurities and to make the pharmaceuticals more safe.
Limit Test
Limit test is defined as quantitative or semiquantitative test designed to identify and control small quantity of impurity which is likely to be present in the substance.
Limit test is generally carried out to determine the inorganic impurities present in the compound.
Limit test for chlorides, sulphates, iron, lead and heavy metal are carried out in Nessler cylinders. Nesseler cylinders are made up of borosilicate glass that is colourless. It has the fixed diameter, length as per according to the Indian Pharmacopeia.
Two similar kind of cylinders are required each time i.e. one for the ‘Test’ sample and other for the ‘standard’ to make comparison in the identical manner. The quantities of the sample vary according to the , limits of impurities while the standard remains constant.
No numerical values for ths limits in these tests are prescribed in the pharmacopoeias, as it is not practicable. Generally an aqueous solution of the substance is prepared.
Sometimes a solution of the, substance is prepared by dissolving in an acid or if the solution is alkaline it is neutralized with nitric or hydrochloric acid as specific in the monograph of the pharmacopoeia. The Extent of opalescence, turbidity and colour is affected by other impurities present in the substance.
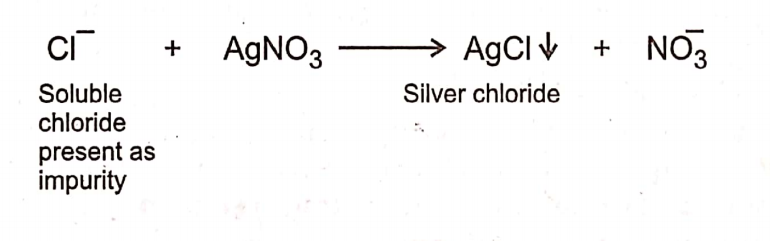
Limit Test for Chloride
Limit test of chloride is based upon the chemical reaction between silver nitrate and soluble chlorides in presence of dilute nitric acid to give opalescence (solid particles) of silver
chloride. Opalescence produced is compared with the standard solution. If the opalescence in the sample is less than the standard, it passes the test. If it is more than the standard, it fails the test.
Procedure
Take two 50 ml Nessler Cylinders.-Label one as “Test” and- the other as ‘Standard’.
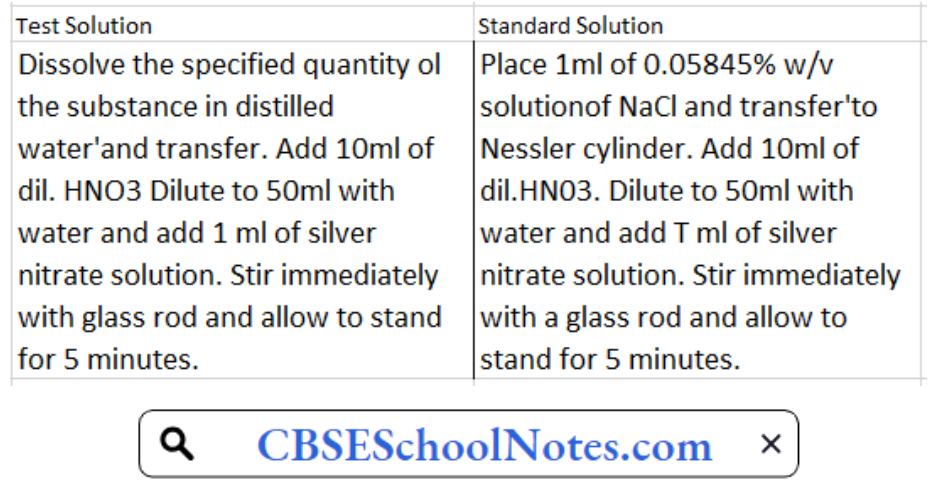
Then observe both Nesseler cylinder from the side and from above against a black background and compare the turbidity. The turbidity developed in the test solution is not thicker than that of standard solution.
Limit Test for Iron
Limit test of iron is based on the reaction of iron with thioglycolic acid in the presence of citric acid and ammonia when pale pink to deep reddish purple colour is produced. Citric acid forms a complex with iron and prevent its precipitation by ammonia as ferric hydroxide. It will result to the formation of purple coloured ferrous salt of thioglycolic acid.
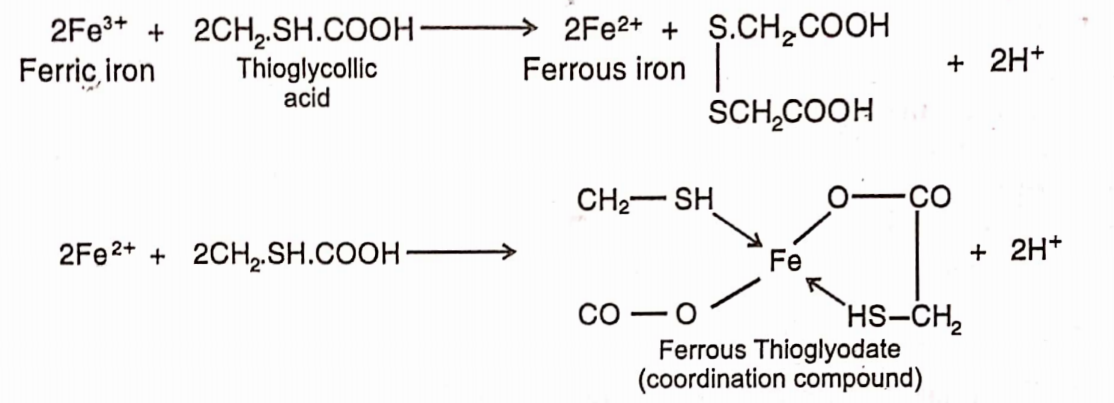
The colour produced is due to the formation of a ferrous compound with thioglycolic acid. It is stable in the presence of air but fades when exposed to air due to oxidation to the
ferric compound.
Standard Iron Solution: Accurately 0.1726g of ferric ammonium sulphate is weighed and dissolved in 10ml of 0.1N sulphuric acid and sufficient water to produce 100ml. Each ml of this solution contains 0.02mg of iron.
Procedure
Take two 50ml Nesseler cylinders. Label one as the ‘Test’ and the other as ‘Standard’.
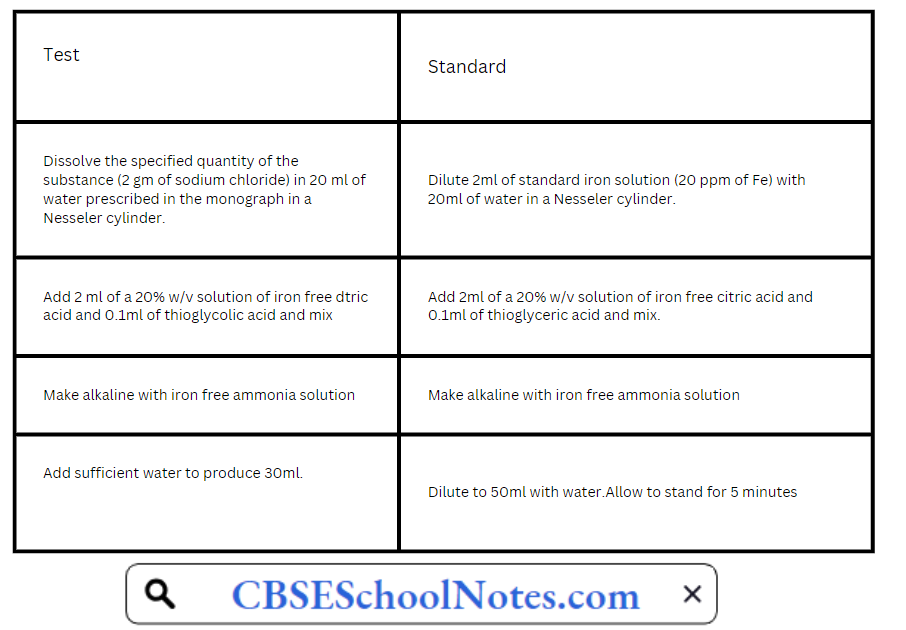
Compare the purple colour in two Nesseler cylinders by viewing vertically downwards. Any colour produced in test solution should not be more intense than the standard solution.
If the intensity of the colour is more in test than in the standard, it means that the sample contains more quantity of iron impurity than the permissible limit and hence the sample is
declared as not of standard quality
The colour in the test and the standard should be compared immediately after five minutes allowed for full development of the colour is over. If there is any delay, the colour
fades due to oxidation and the test becomes unreliable.
List of substances for which limit test of iron is prescribed in I.P. 1996.
- Calcium carbonate
- Calcium chloride
- Zinc oxide
- Zinc sulphate
- Heavy magnesium carbonate
- Light magnesium carbonate
- Sodium acetate
- Sodium bicarbonate
- Sodium chloride
Limit Test for Sulphate
Limit test of sulphate is based on the reaction of soluble sulphate with barium chloride in presence of dilute hydrochloric acid to form barium sulphate which appears as solid particles (turbidity) in the solution.

Hydrochloric add is added to prevent precipitation of other acid radicals such as phosphate, oxalate etc. by common ion effect with barium chloride sol. So that less barium ions are formed.
Reagents:
Barium Sulphate Reagent: 15ml of a 0.5M barium chloride, 55ml of water and 20ml of sulphate-free alcohol are mixed, 5ml of a 0.0181% w/v solution of potassium sulphate are added, diluted to 100ml with water and mixed. Barium sulphate reagent must be freshly prepared.
0.5M Barium Chloride: Barium chloride dissolved in water to contain in 1000ml 122.1g ofBaClÿHjO.
Procedure: Take two 50ml Nesseler cylinders. Label one as “Test” and the other as “Standard”.
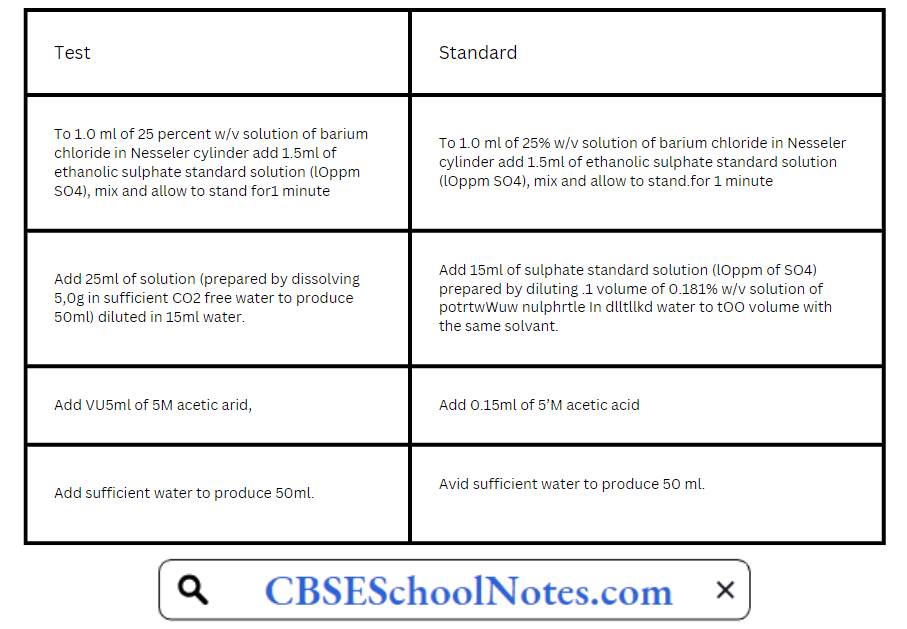
Stirr immediately each solution with a glass rod and allow to stand for 5 minutes, Compare the turbidity transversally against a black background in two Nesscler cylindres. Any colour
produced in test solution should not he more intense than the standard solution.
LimitTest for Heavy Metals
The limit test for heavy metals is based on the reaction between the solution of heavy metals and a saturated solution of Hydrogen sulphides. In acidic media, it produces reddish/black colour with hydrogen sulphide which is compared with standard lead nitrate solution.

It is designed to determine tire content of metallic impurities that are coloured by sulphide ion, under specified conditions. It is indicated in the individual monographs in terms of lead per million parts of tire substance (by weight), as determined by visual comparison of tire colour produced by the substance with that of a control prepared from a standard lead solution.
The amount of heavy metals is determined by one of tire following methods and as directed in the individual monographs. Method A is used for substances that yield clear, colourless
solutions under the specified test condition.
Method B is used for substances that do not yield dear, colourless solutions under tire test conditions specified for method A, or for substances which, by virtue of their complex nature, interfere with the precipitation of metals by sulphide ion. Method C is used for substances that yield clear, colourless solutions with sodium hydroxide solution.
Method A:

The colour produced in the test solution should not be darker than that produced in the standard solution.
Method B:
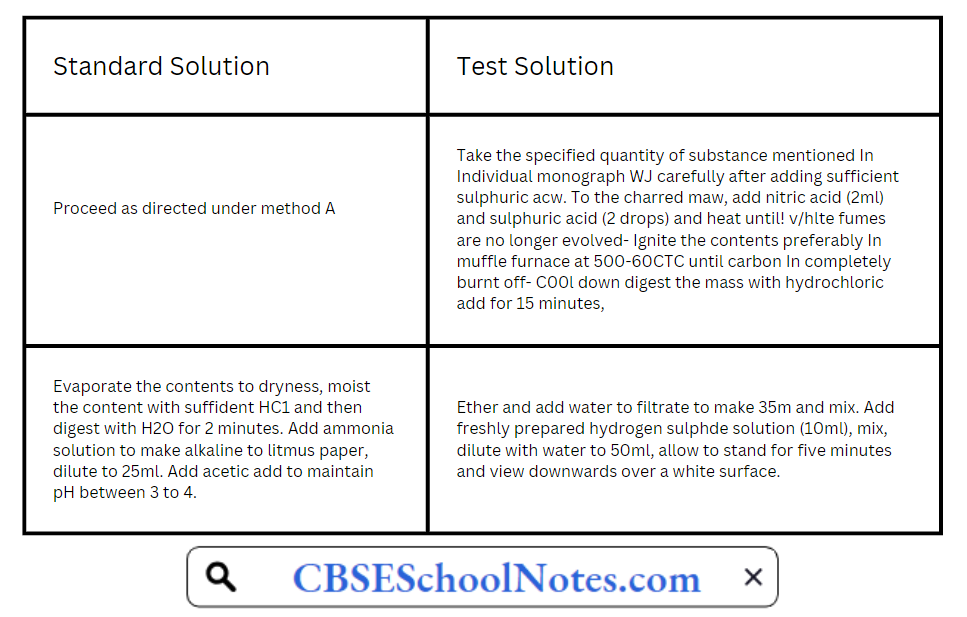
Method C:
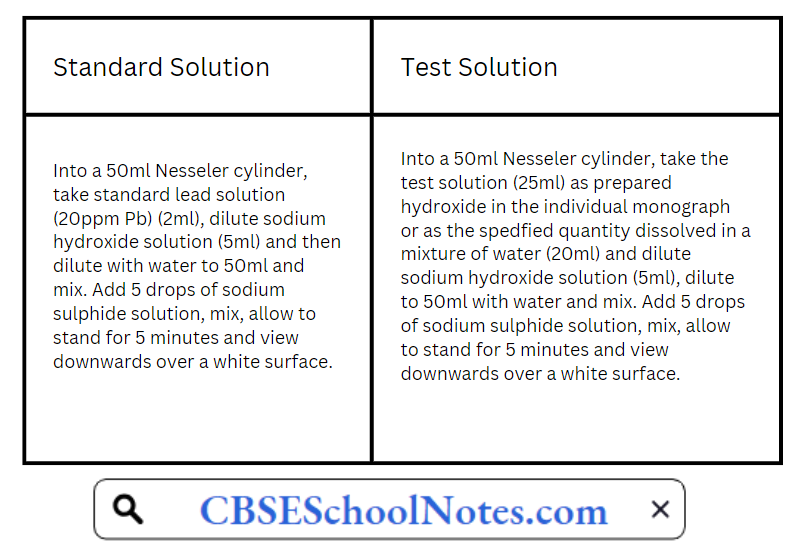
The colour produced in the test solution should not be darker than the colour of the standard solution. Lead standard solution (20ppm Pb) is prepared by diluting 1 volume of lead standard solution (100 ppm Pb) to 5 volume with water.
Lead standard solution (100 ppm) itself is prepared by diluting 1 volume of lead standard solution (0.1% Pb) to 10 volume with water Lead standard solution (0.1% Pb) is prepared by dissolving 0.400 gm of lead nitrate in water containing 2 ml of cone. Nitric acid & adding sufficient water to produce 250 ml.
Limit Test for Lead
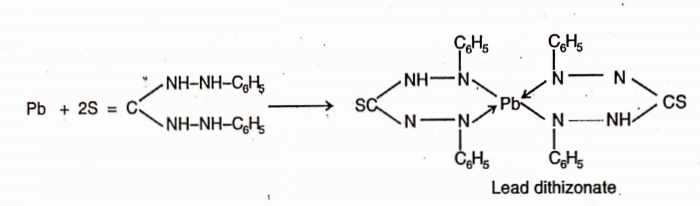
Lead is a toxic substance present in pharmaceutical preparations. The main source of this impurity are sulphuric acid and the lead apparatus. The I.P. and U.S.P. method is based on the reaction between lead and diathizone (diphenylthiocarbazone).
In chloroform solution dithizone extracts lead from an alkaline aqueous solution as lead dithizone which has red colour in chloroform solution. Since dithizone itself imparts a grÿn colour in chloroform, the resultant colour of dithizone and lead dithizone is violet.
The colour produced by a given amount of the sample is compared with that pro uce y a volume of a standard soluHon of lead. If the colour is intense than that produced by the standard, it contains lead in excess of the prescribed limit.
For the test, the lead present as impurity is separated by extracting an alkaline solution of the substance with dithizone extraction solution which removes all the lead in the form of its complex in chloroform layer.
Limit Test for Arsenic
The presence of arsenic in drugs even in the traces is not desirable because it is toxic and cumulative nature. The Indian Pharmacopeia prescribes the limits for the presence of arsenic
as an impurity in various drugs. For example:- Sodium chloride should not contain arsenic more than 1 parts per million.
Chemically, the arsenic impurity is converted in acidic medium into arsenious acid or. arsenic acid depending upon the valency state of arsenic:

The solution is then reacted with a reducing agent like stannous chloride or sulphurous acid to convert the pentavalent arsenic acid into the trivalent arsenious acid which is converted into gaseous arsenious hydride (arsine gas) with the help of nascent hydroeen produced by the acton of zinc with hydrochloric acid.

Arsine gas is carried out through the tube with the help of hydrogen to mercuric chloride paper. Reaction of arsine with mercuric chloride produces a yellow coloured stain. The intensity of the colour is dependent on the quantity of arsenic.

Method:
The volume of the prepared sample in a separator is transferred and unless otherwise directed in monograph, 6ml of ammonium citrate solution sp. and 2ml of hydroxylamine hydrochloride solution sp. are added (for the determination of lead in iron salts use 10ml of ammonium citrate solution sp.).
Two drops of phenol red solution are added and the solution made just alkaline (red in colour) by the addition of strong ammonia solution. The solution is cooled, if necessary and 2ml of potassium cyanide solution sp. are added.
Immediately the solution is extracted with several quantities, each of 5ml of dithiazone extraction solution, draining of each extract into another separating funnel, untill the dithiazone extraction solution retains its green colour.
The combined dithizone solutions are shaken for 30 seconds with 30ml of a 1% w/v solution of nitric acid and the chloroform layer discarded.
To the acid solution exactly 5ml of standard dithiazone solution and 4ml of ammonia cyanide solution sp. are added and shaken for 30 seconds, the color of the chloroform layer is of no deeper shade of violet than that of a control made with a volume of dilute standard lead solution equivalent to the amount of lead permitted in the sample under examination.
All reagents used for the test should have as low a content of lead as practicable. All reagent solutions should be stored in containers of borosilicate glass. Glassware should be rinsed throughly with warm dilute nitric acid, followed by water.
Apparatus:
The apparatus consists of a 100ml bottle or conical flask closed with a rubber or ground glass stopper through which passes a glass tube (about 20cm x 5mm). The lower part of the tube is drawn to an internal diameter of 1.0mm and 15mm from its tip is a lateral orifice 2 to 3mm in diameter.
When the tube is in position in the stopper in the lateral orifice should be at least 3mm below the lower surface of the stopper. The upper end of the tube has a perfectly flat surface atupper right angle to the axis of the tube.
A second glass tube of the same internal diameter and 30mm long, with a similar flat surface, is placed in contact with the first and is the lower tube insert 50 to 60mg of lead acetate cotton, loosely packed or a small plug of cotton and a rolled piece of lead acetate paper weighing 50 to 60mg.
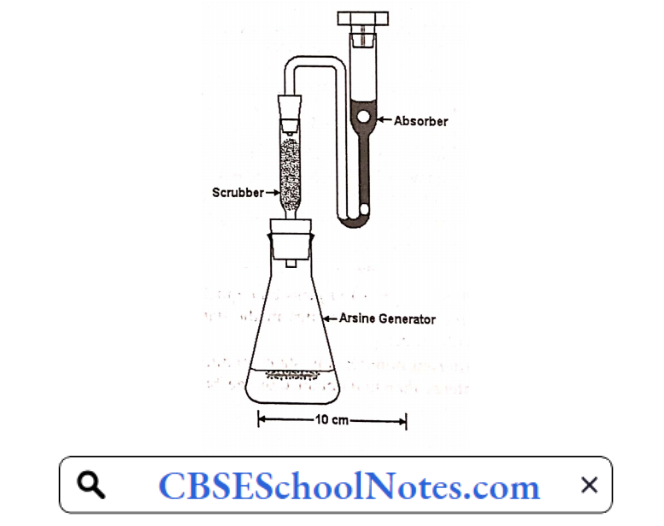
Between the flat surface of the tubes place a disc or a small square of mercuric chloride paper large enough to cover the orifice of the tube (15mm x 15mm). The purpose of lead acetate cotton is to trap any hydrogen sulphide (H2S) gas which would otherwise interfere with this test as it also give some stain with mercuric chloride paper.
The tube is fitted at its upper end with two rubber bungs as shown in figure. A piece of dry mercuricpaper is placed flat on the top of the bung and the other bung is place over it and secured by means of clips in such a manner that the borings of the two bung meet to form a true tube of the same diameter (6.5mm) interrupted by a diaphragm of mercuric chloride paper.
Separate apparatus is used for the test and the standard.
Notes:
- The test is a modification of the Gutzeit test and is, therefore called modified Gutzeit test.
- All the reagents which are used for this test should have a low content of arsenic as possible free from arsenic impurity.
- Potassium iodide is used because it helps in the reduction of pentavalent arsenic acid into trivalent arsenic acid.
- Granulated zinc is used instead of ordinary zinc because evolution of nascent hydrogen is steady and prolonged with granulated zinc.
- The arsenic impurity is expressed in terms of ppm (parts per million). One ppm is lmg in 1kg.
Limit test for Arsenic in Ammonium Chloride:
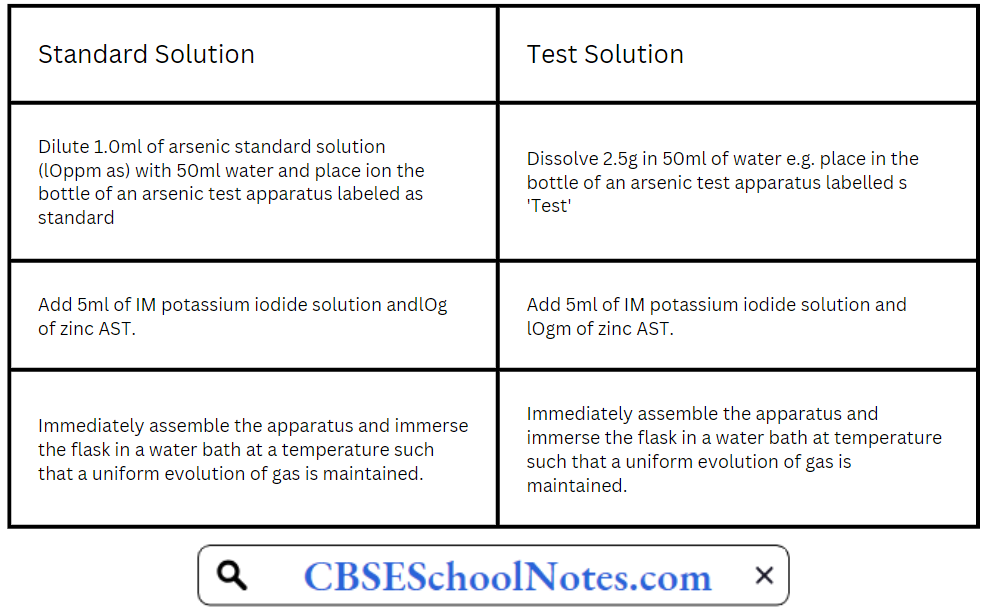
Place the prepared glass tube quickly in position in both the cases and allow the action to proceed for 40 minutes in the dark . compare the yellow stain in the two, in day light without delay.
After 40 minutes any stain produced on the mercuric chloride paper in test is not more intense than that obtained by the ‘Standard’.
Modified procedures for certain limits tests
1. Chloride and Sulphate in Potassium Permanganate
Principle : When limit test of chloride and sulphate are done in usually way, it will be very difficult to make any observation, since the sample itself (Potassium permanganate)
is highly coloured. So the presence of potassium permanganate can be reduced by alcohol. This process is known as PRETREATMENT.
The sample is dissolved in water and heated on a water bath. Alcohol is added. It is filtered to remove the precipitate manganese dioxide. The filterate is colourless & can be used for performing the limit test for chloride and sulphate in the usual way.
Procedure: Dissolve 1.5gm of the sample which is accurately weighed, in 50ml of distilled water. Heat the solution on a water bath and add gradually 6ml of ethanol 95%. Further cool it and dilute to 60ml with distilled water and filter. The filterate (Solution A) is colourless.
For Limit Test for Chlorides
Take 40 ml of solution A and do the limit test for chloride.
For Limit for Sulphate
Take 10 ml of solution A and do the limit test for sulphate.
2. Chloride and Suijp hate in Sodium Bicarbonate
Principle: In the limit test of chloride and sulphate in sodium bicarbonate, the pretreatment consists of neutralising the sodium bicarbonate with an app. Mineral acid and using the neutralised solution for the particular limit test. In the case of limit test for chloride, the sample is dissolved in distilled water & neutralised with nitric acid.
![]()
In the case of limit test for sulphate, the sample is suspended in distilled water and neutralised with HC1.
![]()
In both cases, the solution should be stirred well and the effervescence should be allowed to subside.
Procedure :
For Limit Test of Chloride
Weigh accurately 1.25gm of the sample and dissolve it in 15ml of distilled water. Add 2ml of cone. Nitric acid, then apply the limit test for chloride to this solution
For Limit Test of Sulphate
Weight accurately about lgm of the sample and suspend it in 10ml of distilled water. Neutralise the solution with cone. Hydrochloric acid adding it gradually till the effervescence ceases out. Dilute to 15 ml with distilled water. Do the limit test for sulphate with this solution.
Types Of Impurities In Pharmaceutical Substances Very short answer questions
Question 1. Why only distilled water or purified water is used in performing limit tests?
Answer. In performing limit tests only distilled water or purified water is used because ordinary tap water contains number of ions to validated the test.
Question 2. Why nitric acid is used in performing limit test for chloride?
Answer. Nitric acid is added to prevent precipitation of add radicals such as phosphate, sulphate etc. with silver nitrate because in the presence of nitric add other predpitates are not produced and only chlorides get predpitated.
Question 3. Why HC1 is used in the limit test of sulphate?
Answer. To remove the impurities ofsulphate.
Question 4. Why Barium chloride is used in the limit test of sulphate?
Answer. Barium chloride reacts with a sulphate to produce barium sulphate which can be seen as a white predpitable e.g. therefore can be identified.
Question 5. What is the reagent used in preparingbarium sulphate?
Answer. Sulf + Barium.
Question 6. What do you understand by the term ppm?
Answer. ppm is parts per million. One ppm is lmg in 1kg.
Question 7. Why granulated zinc is used instead of ordinary zinc?
Answer. Granulated zinc is used instead of ordinary zinc because evolution of nascent hydrogen is steady and prolonged with granulated zinc.
Question 8. What do you understand by the term limit tests?
Answer. Limit test is defined as quantitative or semi quantitative test designed to identify and control small quantity of impurity which is likely to be present in the substance.
Question 9. Is there any special apparatus or container required for carrying out limit test?
Answer. Yes Nessler cylinders are required for performing the limit test
Types Of Impurities In Pharmaceutical Substances Fill in the blanks
1. Limit test are qualitative e.g. ………………..test to identify and control small quantities of impurities.
Answer Quantitative
2. Limit test for chloride has been based upon reaction between……… and ……….to obtain silver chloride.
Answer AgN03/Soluble chloride
3. Limit test for sulphate has been based upon the ppt of sulphate with……… in presence of…….
Answer Barium chloride/Hydrochloride
4, Limit test for iron ferrous thioglycolate has stable pink to reddish purple colour in……… medium.
Answer Thioglycolic acid
5. Limit test of iron is based upon reaction of Fe with…………. ammonium citrate
Answer Ferrous mercaptoacetate
6. Limit test for iron purple colour is due to the formation of…….
Answer Alkaline
7. The limit test for arsenic is based upon……..
Answer Guizet test
8. The limit test for arsenic,……… is convertedinto arsenous acid/arsine gas.
Answer Arsine
9. The function of granulated zinc in limit test for arsenic is……
Answer Slow and prolonged evolution of nascent H2 gas.
10. In limit test for heavy metals…… is used for clear colorless/turbid colored solution.
Answer Method A
11. In limit test the change in……..is compared with fixed standard in the pharmacopeia.
Answer Colour, turbidity
12. If the test solution colour, turbidity or opalescence is less than that of the standard solution it……………….the limit test.
Answer Passes or fails
Major Extra And Intracellular Electrolytes
Major Extra And Intracellular Electrolytes Introduction
Electrolyte is a substance that ionizes when dissolved in a suitable ionizing solvents such as water. This includes most soluble acids, bases and gases. An electrolyte may be
defined as concentrated if it has high concentration of ions or dilute if it has low concentration of ions.
Electrolytes are used in replacement therapy and for the correction of acid-base balance in various body fluids. The electrolyte concentration of body fluids have been different in
various body fluid compartments. The various body fluid compartments are:-
1) Intracellular fluid:- This is the fluid which is present inside cell E.g. Cytoplasm. It constitutes 12-15% of body weight and its volume is 30 litres.
2) Extracellular fluid:- This is the fluid which is present between the cells E.g. Blood plasma. This constitutes 12-15 % of body weight and its volume is 10 litres.
3) Plasma (vascular) fluid:- This is the fluid which is present within the blood vascular system. This constitutes 4-5% of body weight and its volume is 3-5 litres.
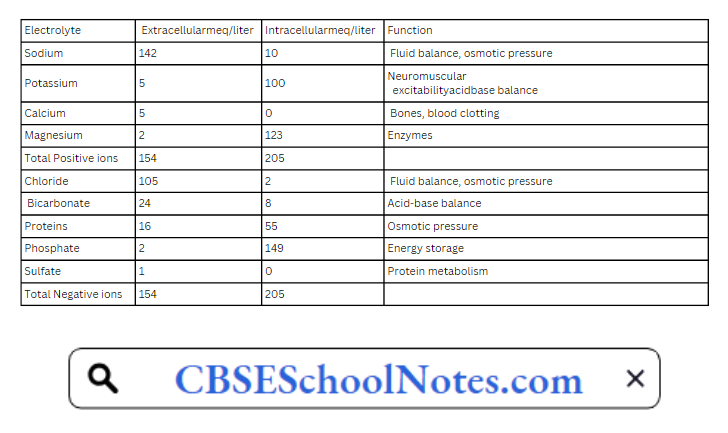
The major electrolytes found in the body are:- Calicum, Potassium, Phosphate, Iron, Magnesium, Chloride, Sodium.
Read and Learn More Pharmaceutical Inorganic Chemistry Notes
Major Physiological Ions
Calicum:- Calicum is an important constitutent of bones and teeth. It is also concerned with the functioning of muscles and clotting mechanism of blood .The main sources of Cal
cium include milk, cheese, green vegetables, egg and fish.
Magnesium:- The total magnesium content in body is about 25 gram of magnesium and the daily requirement is 350 mg. The main sources of magnesium include nuts, soyabeans, wholegrains, seafoods.
It is used for protein synthesis and for the smooth functioning of the neuromuscular system. Its deficiency cause personality changes, loss in body weight and cardiac disturbances. It is the second most cation in concentration in the intracellular fluid compartment.
Chloride:- It is the major extracellular anion. The total chloride ion present in the body is about 50mEq per body weight and body daily requirement is about 5-10 gm as sodium chloride.
The main source of chloride required for the body is table salt which is used in cooking. Chloride ion is excreted through the urine and through the skin during sweating. It is required for maintaining proper hydration, osmotic pressure and normal cation-anion balance.
Potassium:- It is the major intracellular cation present as about 23 times higher than present in the extracellular fluid in the human body. Human body has about 2.6 per kg weight of potassium.
The main source of potassium in food includes milk, certain vegetables, meat and whole grains. Potassium ions are used to maintain the electrolyte composition of various body fluids, help to regulate pH by exchange against for hydrogen ions and in many biochemical activities inside the cell.
Sodium:- It is the most abundant extracellular ion. It constitutes nearly 90% of extracellular cations. The normal sodium content in the body varies from 5to 20 gm and the daily
requirement is in between 3-5 gm.
The main source of sodium required for our body is tablesalt which is used in cooking. Sodium plays an important role in the maintence of osmotic pressure of various body fluids and in the transmission of nerve impulses in the nerve fibre.
Phosphate:- It is the principal anion of the intracellular fluid compartment. The main sources of phosphate are cereals, pulses, nuts and oil-seeds. It is an important buffer system and is also present in the bones.
Iron:- It forms an important component of haemoglobin which acts as a carrier of oxygen in the blood. The main sources of iron include green leafy vegetables, millets like bajra
and ragi. It is necessary for growing children and pregnant women. The deficiency of causes anaemia and goitre.
Electrolyte Distribution
Electrolyte Used In Replacement Therapy
In normal conditions, the body is able to adjust the electrolyte balance while in some conditions such as prolonged fever, severe vomiting or diarrohea, there occurs a heavy loss
of water and electrolyte. So, there is need to administration of lost electrolyte.
There some electrolytes that are used in replacement therapy are sodium chloride and its salts such as sodium chloride injection, hypertonic solution, sodium lactate injection, potassium chloride and its salts.
Sodium Chloride
Chemical formtila:-NaCl Molecular weight;- 58.45
In the nature, it is found in sea water, in seawells, lakes(sambhar in India)and in deposits of rock salts.
Preparation
In the laboratory, it is prepared from common salt(impure) in water by passing hydrochloric acid gas. The crystals are precipitated out. Industrially, it is prepared by evaporation of sea-water in shallow pans.
It contain certain impurities which are removed by dissolving common salt in water in cemented tanks. Some alum and lime are added. The suspended impurities get settle down easily.
Physical Properties
Sodium chloride occurs in the form of colourless, transparent cubes or as a white, crystalline powder.
It is colourless
It has a saline taste
It is slightly hygroscopic
Chemical Properties
1 . Sodium chloride is rather easily oxidised to liberate free chlorine. For e.g. heating with manganese dioxide & cone, sulphuric aied produces chlorine.

2. Sodium chloride when react with silver nitrate gives a curdy precipitate of silver chloride.

The precipitate which is affected by light is soluble in dilute ammonia and insoluble in nitric acid.
Uses
It is used as an electrolyte replenishes emetic. Jt can be used in homeopathetic medicine. Solution of sodium chloride may be used as an eye-drop, nasal drop( to relieve nasal congestion) and as a mouthwash (to remove debris).
Assay
An accurately weighed quantity is dissolved in water & a known excess of 0.1M AgNO solution, dil. HNO and diethyl phthalate are added. It is titrated with 0.1M ammonium
thiocynate solution using ferric ammonium sulphate as indicator.
This is a modified Volhard’s method. Sodium chloride is precipitated as silver chloride by the addition of silver nitrate. Dibutyl phthalate is added to coat the silver chloride so that it will not interfere with the titration off the excess of AgN03 with 0.1M ammonium thiocyanate, since silver chloride reads slowly with ammonium thiocyanate.
Previously (in I.P. 66) sodium chloride was assayed by direct titration in neutral solution with 0.1N silver nitrate using potassium chomate as indicator.

The same cannot be used now since silver chromate formed at the end point is soluble in acid.
Potassium Chloride
Chemical formula:-KCl
Molecular weight:-74.55
In nature it is found as syline (KCl) and camallite contaminated
KCl.MgCL2.6H2O with magnesium sulphate and chloride.
Preparation
Potassium chloride can be prepared by reacting hydrochloric acid with potassium carbonate.

Properties
It occurs as colourless, odourless, cubical and crystalline powder. It is having saline taste. It is soluble in water, glycerol, practically insoluble in alcohol, solvent and ether. It diminish its
solubility in water.
Assay
The assay is based on Mohr’s method of direct volumetric precipitation titration. An aqueous solution of the solution is titrated against a standard solution of silver nitrate using
solution of potassium chromate as indicator.

When whole of NaCl has been precipitated as AgCl, addition of silver nitrate solution gives a brick red colour with the indicator. The end point is change of colour from yellow to red.
An aqueous solution of the weighed substance is titrated with 0.1N AgN03, using K2Cr2O7. solution as indicator. Each ml of 0.1N silver nitrate is equivalent to 0.007455g of KCl.
Uses:
It is used in the treatment of potassium deficiency. It is also used in the treatment of Myasthenia gravis( muscle weakness) and as an antidote for digitalis intoxication. It is used as an
electrolyte replenishes
Calcium Gluconate

Method of Preparation
It is prepared by boiling a solution of gluconic acid with excess of calcium carbonate, filtering and crystallising the substance from filtrate.

Properties
It occurs as odourless, white crystalline powder, tasteless, freely soluble in boiling water, sparingly soluble in water and insoluble in alcohol, ether and chloroform.
Uses: it is Used as a source of calcium ion in the treatment of calcium deficiency and hypocalcaemic tetany.
Assay
The assay is based on complexometric type titration forming a well defined simple complex between calcium and disodium ethylenediamine titracetate (EDTA) using mordant black II
as an indicator. The end point is a change of colour from red to blue. In this assay, a solution of magnesium sulphate is added before the titration to make the end point sharp.
Magnesium also forms a similar complex with EDTA. But these titration have to be carried out in the presence of buffer such as strong ammonia-ammonium chloride solution.

An aqueous solution of the substane containing magnesium sulphate and strong ammoniaammonium chloride is titrated with 0.05M disodium ethylenediamine tetraacetate, using
mordant black II as indicator.
From the volume of 0.05M magnesium sulphate is substracted. Each ml o the remainder is equivalent to 0.024420g of CaC12H22O14.H2O.
Official Test for Identity
- Give the reactions characteristic of calcium.
- To a solution of the substance in water, ferric chloride solution is added. A yellow colour is produced.
Oral Rehydration Salt (Ors)
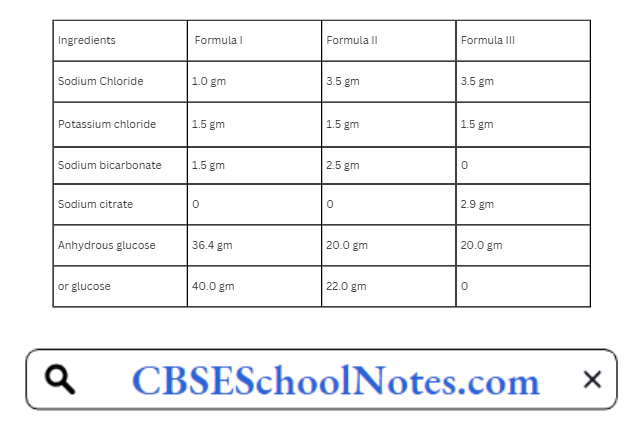
Oral rehydration salt contain anhydrous glucose, sodium chloride, potassium chloride and either sodium bicarbonate or sodium citrate. These dry preparations are to be rrux HI specific amounts of water along with certain flavouring agents and a suitable agents or ee flow of powder.
These are used for oral rehydration therapy. In ancient times, homema e ORS is used which constitutes of one tablespoonful of salt, two tablespoonfuls of sugar in litre of water.
The following three formulations are usually prepared. When glucose is used, sodium bicarbonate is packed separately. The quantities given below are preparing 1 litre solution.
The Oral Rehydration Therapy (O.R.T.) has several advantages :
- Patients strong enough to drink take this easily.
- Vomiting is easily corrected by the therapy itself.
- Solution should be sterile.
- This oral treatment is very cheap.
- It can be given by intravenous mode also.
- It is given easily by the mouth.
The power may be dissolved in boiled water and made up to one litre. It contains the same proportions of electrolyte as in the previous formula except that this powder contains
9.9 mEq/1 of citrate in place of the bicarbonate.
The formulae II and III are recommended by WHO And UNICEF for control in diarrhoeal diseases.
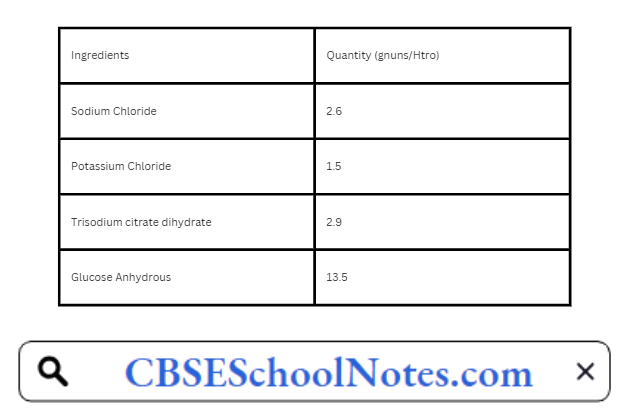
New Formula Oral Rehydration Salts By Who
A new formula for oral rehydration salts (ORS), has been released by the World Health Organization (WHO). The new formula ORS, a sodium and glucose solution, is widely used
to treat children with acute diarrhea.
Since WHO adopted ORS in 1978 as its primary tool to fight diarrhea, the mortality rate for children suffering from acute diarrhea has fallen from
5 million to 1.3 million deaths annually.
The new improved formula fe the result of extensive research sponsored by WHO’s Department of child and adolenscent Health and development and suppoerted by the united states agency for International Development (USAID).
Physiological Acid-Base Balance
Body fluids are having balanced quantity of acids and bases and this quantity is maintained by intricate mechanism. The maintenance of this balance quantity is necessary for biochemical reaction talking places in body, because biochemical reaction are very sensitive to even small change of acids and bases.
Example: LOW pH value in stomach is requiring for functioning of enzyme pepsin which is useful for digestion of food.
The pH values of certain body fluids are:
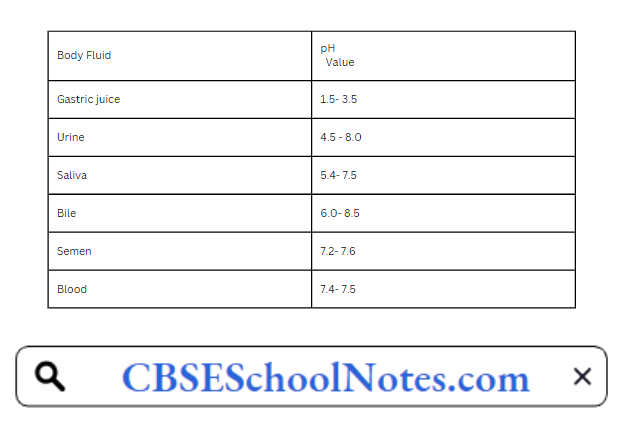
Body is having its own buffer system which prevents little change in the pH value of blood. It also helps to convert strong acids and bases into weak acids or bases. Lungs and kidney the main organ which helps to maintain buffer system in the body.
In case of low respiration, the accumulated carbon dioxide combines with water and forms carbonic acid which releases hydrogen ions and causes respiratory acidosis.
![]()
In over-breathing, excessive excretion of carbon dioxide occurs and causes respiratory alkalosis.
Kidney has ability to generate ammonia which neutralizes acid products of protein metabolism and excrete in urine
Conditions where metabolic alkalosis occurs:
- Loss of chloride ions
- Administration of diuretics
- Excessive ingestion of alkaline drugs
- Endocrine disorder
Conditions where metabolic acidosis occurs:
- Absorption of excess metabolic acids
- Formation of excessive quantities of metabolic acids like carbonic acids
- Failure to excrete metabolic acids
- Loss of base from body fluids
- Diabetes mellitus
- Diarrhoea
- Uremia
- Excess vomiting
Major Extra And Intracellular Electrolytes Very Short Questions and Answers
Question 1. Name the major ions involved in the fluid and electrolyte balance and briefly describe their major location.
Answer.
- Sodium is the most abundant extracellular ion and represents about 90 percent of extracellular cations.
- Potassium is the most abundant cation in the intracellular fluid.
- Calcium is the most abundant ion in the body and is principally an extracellular extracellular electrolyte.
- Magnesium is primarily an intracellular electrolyte.
- Chloride is the major extracellular anion.
- Phosphate is principally an intracellular electrolyte.
Question 2. Name the substances that dissociate in Water and form ions?
Answer. Electrolytes.
Question 3. Name the largest body fluid Compartment?
Answer. Intracellular compartment.
Question 4. What is ORS?
Answer. Oral rehydration salt.
Major Extra And Intracellular Electrolytes Multiple Choice Question And Answers
Question 1. The body fluids found within the cells is called
- plasma.
- extracellular fluid.
- interstitial fluid.
- intracellular fluid.
- water.
Answer: intracellular fluid.
Question 2. Blood plasma belongs to
- intracellular fluid.
- extracellular fluid.
- interstitial fluid.
- Both B and C.
- None of the above.
Answer: interstitial fluid.
Question 3. Most solutes in body fluid are,
- electrolytes.
- proteins.
- sugars.
- amino acids.
- lipids.
Answer: electrolytes.
Question 4. Water lost through the actions of the
- kidneys.
- gastrointestinal tract.
- lungs.
- skin.
- All of the above.
Answer: All of the above.
Question 5. Total fluid output of the body under normal conditions is approximately
- 200 ml/day.
- 2500 ml/day.
- 400 ml/day.
- 1500 ml/day.
- 4300 ml/day.
Answer: 2500 ml/day.
Question 6. Which of the following ions diffuses easily between extracellular and intracellular compartments?
- magnesium
- chlorine
- sodium
- phosphate
- potassium
Answer : chlorine
Question 7. The major route of excretion for sodium ions (under normal conditions) is the
- skin.
- kidney.
- GI tract
- adrenal cortex.
- sweat
Answer : kidney.
Question 8. KC1 is indicated in the treatment of………
- menieres syndrome
- antidote in digitalis intoxication
- myasthenia gravis
- all of the above.
Answer: myasthenia gravis
Question 9. Calicum is essential for…………
- blood pontification to whaler bone
- blood clotting
- Myasthenia gravis
- All of the above
Answer: blood clotting
Question 10. The principal function of chloride is………
- Maintenance of proper hydration.
- Maintenance of osmotic pressure.
- Normal Electrolytic balance
- All of the above
Answer: All of the above
Major Extra And Intracellular Electrolytes Fill In The Blanks
1. Sodium chloride is used as………
Answer. Fluid and electrolyte replenisher
2. …….and…….. are found in plasma and interstitial fluid.
Answer. Na, Cl
3. ……..are found in intracellular fluid.
Answer. K, Mg,P04
4. The basic objective of replacement therapy is….
Answer. to restore the volume and composition of body fluids.
5. Replacement therapy is needed for…………..
Answer.Heavy loss of water,diarrhoea, prolonged fever
6. Electrolytic solution can be given by………..and………….
Answer.Oral, i.v.
7. ORS stands for………..
Answer. Oral rehydration salt
8. Homemade ORS constitutes of ……………
Answer. One half tablespoonful of salt, two tablespoonful of sugar in 1 litre of water
9. The concentration of electrolytes is expressed in,………….
Answer.Milliequivalents per litre
10. Extracellular fluid includes………………..
Answer. Intestinal and vascular fluid.
Acids Bases And Buffer Notes
Acids And Bases
An Acid may be defined ns any substance which has sour taste and its aqueous solution turns blue litmus red.It reacts with Bases to form water and ionic compounds called salts.
A base may be defined ns any substance which has bitter taste and its aqueous solution turns red litmus blue. It reacts with acid to form water and salts.
Arrhenius Concept
The first conceptual theory of acid and bases were given by Arrhenius, also known as Arrhenius theory of Ionization. According to him, ah acid is a substance that dissociates to give hydrogen ions when dissolved in water. Tlius hydrogen chloride gas is an acid because when dissolved in water, it gives hydrogen ions.

A base is a substance that dissociates to give hydroxyl ions when dissolved in water. Thus NaOH is a base because when dissolved in water, it gives hydroxyl ion.
![]()
According to neutralisation reaction, these two ions (H+ and OH-) combine to form solvent (i.c. water) and a salt (NaCl). This can be refered by the following equation:
Read and Learn More Pharmaceutical Inorganic Chemistry Notes
![]()
Limitations
- It is limited only to aqueous solution and not on substance.
- The neutralisation of acids and bases in absence of solvent could not be explained.
- H could not explain the basic nature of substances e.g.NH3, or Na2Co3 which do not contain OH’ ions and acidic nature of substances e.g. Co2 or So2 which do not contain H’ ions.
Bronsted-Lowry Concept (Proton Transfer Theory)
In 1923, J.N. Bronsted (Danish chemist) and J.M. Lowry (British Chemist) independently and suprisingly suggested a more general defination of acids and bases which applies to aqueous as well as non-aqueous solution.
According to him,’111 aci(l any substance (molecular or ionic) which has a tendency to donate a proton to any other substance while a base is any substance (molecular or ionic) which has a tendency to accept a proton (119 from any other substance.
Acid – Proton donor, Base- Proton acceptor
Some example of acids arc as follows :
Some example of bases are as follows :
Conjugate Acid-Base Pairs
Such pairs of substance which can be formed from one another by the gain or loss of a proton are known as conjugate acid base pair.
Thus conjugate of an acid is the substance formed by the loss of proton while conjugate of a base is the substance formed by the gain of a proton.
Let us consider a reaction of acetic acid in water which may be represented as:-

It is evident that acetic acid donates a proton to water and thus acts as an acid. Water accepts a proton and therefore acts as a base. In the reverse reaction, hydronium ion (H30)
donates a proton to the acetate ion and therefore acts as an acid. The acetate ion accepts a proton and therefore behave as a base.
Limitations of Bronsted- Loivry Concept:
- There are a number of acid-base reactions in which no proton transfer takes place e.g.
Thus, it cannot be able to explain the reactions occuring in non-protonic solvents such as CoCl2, S02. - Bronsted-lowry concept lay emphasis on the proton-transfer. Although it is true that most common acids are protonic in nature, yet there are many which are not.
The Lewis Concept- The Electron Donor Acceptor System
In 1923, Lewis (an American Chemist) introduced another concept of acid and base along with the formation of a cordinate bond. [According to him, an acid may be defined as
any species (molecule, radical or ion that can accept an electron pair to form a coordinate bond while a base may be defined as any species (molecule, radical or ion) that can donate
an electron pair to form a coordinate bond].
The chemical reaction between lewis acid and base results in a product that is described as adduct.
For example :
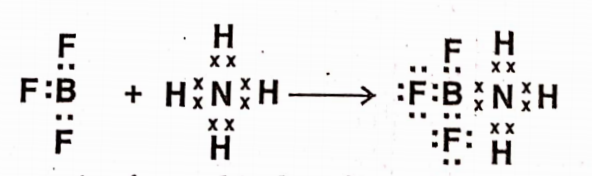
Here, BF3 accepts one lone pair of e- and is therefore a lewis,acid while NH3 donates one lone pair of e~s and is therefore known as lewis base.
Several examples of lewis acid and base are:
Lewis Acid: Ag+, Fe3+
Lewis Base: NH3 H20,OH–,C1–,CN–,etc
Limitations
- An acid-base reaction should be a rapid reaction as it involve electrons. Therefore, however many lewis acid-base reactions which are slow.
- The relative strength of an acid and bases cannot be explained on the basis of lewis concept.
Buffer Solution
The solutions that are able to resist the change in pH values are termed as Buffer solutions. Buffer solution consists of a mixture of weak acid and its salt and weak base and its salt.
Buffer solutions are broadly classified into three categories :
1. Acidic Buffer Solution: The solution having a mixture of weak acid and its salt. For
example : Mixture of Acetic acid and Sodium acetate.
2. Basic Buffer Solution: The solution having a mixture of weak base and its salt.
For example: Mixture of ammonium hydroxide and ammonium chloride.
3. Neutral Buffer Solution: The solution having a mixture of weak acid and weak base.
For example: Mixture of acetic acid and ammonium hydroxide
Buffer Action
The property of buffer solution is to resist any change in its pH value, even when small amount of acid or base is added to it known as”Buffer action”.
Hydrogen Ion Concentration, pH, And pOH
Pure water is considered to ionise to a small degree as per the following equation :
where Kw = Ion product Constant
The ion product constant (Kw) is expressed by involving only the concentration of ionic species on right-hand side of the reaction and has a constant value at 25°C of 1×10-14. It can be
represented as :
[H+] [OH–] = 1×10-14
In pure water, the concentration of both ions are equal each having the value of 1 x 10-7 M
[H+] [OH–] = 1×10-7
The hydrogen ion concentration is greater than hydroxide ion concentration when an acid or base is added to water. The value of hydrogen ion concentration is 10-7g ion/litre.
In Neutral solution [H+]= [OH–]
In Acid solution [H+]>[OH–]
In Alkaline solution [H+]< [OH–]
pH SCALE
Hydrogen ion concentration is usually expressed in terms of mole/litre or gram equivalent/litre. It is very unconvenient to write the expotential power of ten to the power
minus of particular figure. Therefore, Sorenson introduced a practical concept of expressing acidity i.e. pH scale.
The term pH is defined as the negative logarithm (to the base 10) of hydrogen ion concentration. It is represented by the expression :-
The pH scale covers from 0-14 of all the hydrogen ion concentrations. It can be measured by using the pH- meter.
If [H+] is high; the solution is acidic; pH<7 and if [H+] is low; the solution is basic or alkaline the pH founds to be less than 7 (pH>7)
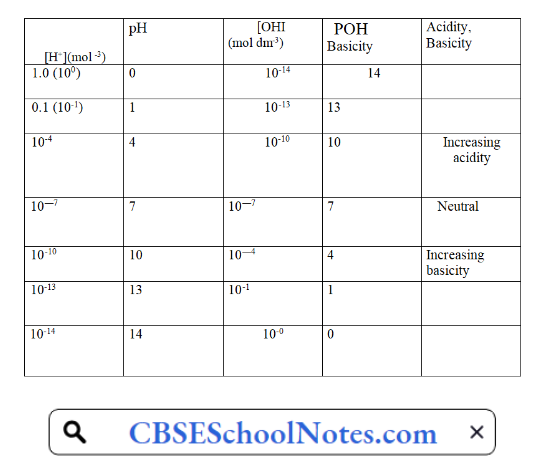
pOH is defined as the negative logarithm of hydroxyl ion concentration.
pH = -log[OH–]
Relationship between pH and pOH
Ionic product of water is given by
Kw=[H3O+][OH–]
Taking log on both sides
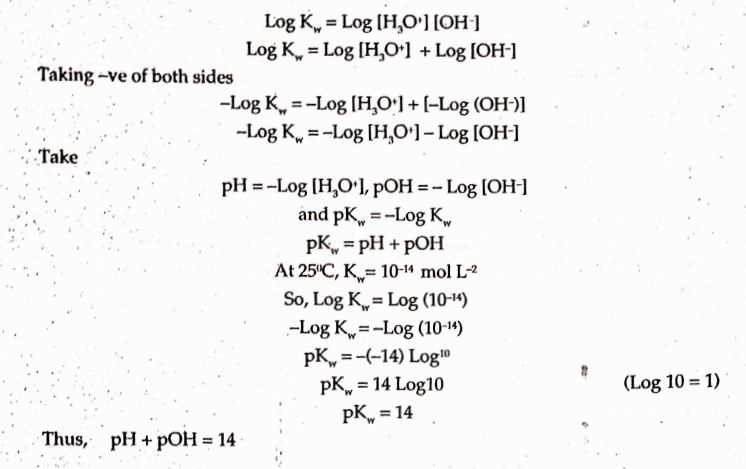
Relationship between pH and [H+] cone., moles/I
Numerical1: Calculate pH and pOH of 0.01N HC1.
Solution: HCl is a strong acid and it dissociate completely so
![Relationship between pH and [H+] cone., moles](https://cbseschoolnotes.com/wp-content/uploads/2024/01/Relationship-between-pH-and-H-cone.-moles-2.png)
![Relationship between pH and [H+] cone., moles](https://cbseschoolnotes.com/wp-content/uploads/2024/01/Relationship-between-pH-and-H-cone.-moles-1-1.png)
Henderson Hesselbach Equation
The hydrogen ion concentration obtainable from the dissociation of a weak acid HA, is given by the equation.
Taking logarithm on both sides :
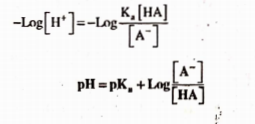
This equation is known as the “Henderson-Hesselbach equadon”,it helps to calculate the pH of the buffer solution of known concentration.
Acid-Base Imbalance
The pH of normal blood ranges between 7.3-7.4. If the pH of the blood falls below 7.3, the condition is termed as Acidosis while if the pH of the blood is higher than 7.3, it is termed as Alkalosis. Both acidosis and alkalosis are primary disorders of bicarbonate. (HC03) ion cone.
Acid-base balance can also affect electrolytes (Na+, K+, Cl ) and hormones.
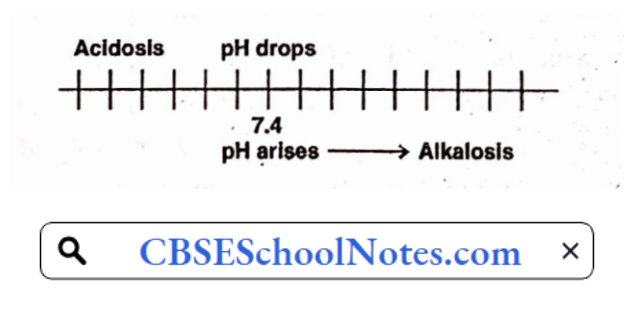
Buffer Capacity (P)
Quantitative measure of this resistance to pH changes is called buffer capacity. Buffer capacity can be defined as the number of moles of H+/OH- ions that must be added to one
liter of the buffer in order to decrease /increase the pH by one unit respectively.
Where [H+] = the hydrogen ion concentration of the buffer, (3 is the buffer capacity, [C] is buffer concentration.
From the above equation the buffer capacity is directly proportional to the buffer concentration.
Buffers In Pharmaceutical System
Buffer solutions are used frequently in pharmaceutical practice, particularly in the formulation of solid, semi solid, parenteral and ophthalmic preparations.
Solid dosage form:
Solid dosage forms such as tablets, capsules and powders buffers have been widely used for controlling the pH of the environment around the solid particles. This has practical application for the drugs that have dissolution rate limited absorption from unbuffered solutions.
One of the special applications of buffers is to reduce the gastric irritation caused by the acidic drugs. For example, magnesium carbonate, sodium bicarbonate and sodium citrate antacids are used for the purpose of reducing toxicity.
Semisolid Dosage Forms: Semisolid preparations such as ointments and creams undergo pH changes upon storage for a long time, resulting in its reduced stability.
Hence; buffers such as sodium citrate and citric acid or phosphoric acid/sodium phosphate are included in these preparations so as to maintain their stability.
Parenteral Products: Use of buffers is common in the parenteral products. Since the pH of blood is 7.4, these products are required to be adjusted to this pH. Change in pH to higher side (more than 10) may cause tissue necrosis while on lower side (below 3) it may cause pain at the site of action.
Commonly used buffers include phthalate, glutamate, citrate and acetate. The pH optimization is generally carried out to have better solubility, stability and reduced irritancy of the product.
Ophthalmic Products: Buffers are used in ophthalmic preparation is to prevent an increase in pH can affect both the stability and solubility of the drug. Buffering agents should be added in preparing on ophthalmic solution must be based on several considerations.
The buffer solutions are not specified in the Monographs of the Pharmacopoeia, but they are mentioned in the Pharmacopoeia under Appendix for solutions and reagents. There are two kinds of buffer solutions:
A. Standard buffer solutions B. Other buffer solutions
Standard Buffer solutions: These buffer solutions having standard pH. They are used for reference purposes in the measurement of pH and carrying out many pharmacopoeial tests which require maintenance of specified pH.
Standard buffer solutions of various pH range values between 1.2- 10.0 may be prepared by appropriate combinations of 0.2 M HC1, 0.2 M NaOH, described below in table:
Standard buffers with their pH range and quantities of ingredients

Other buffer solutions: There are large number of specific buffer solutions mentioned in the Appendix 13.1 of the Indian Pharmacopoeia 1996 with the direction of their preparation.
These buffer solutions are:
Acetate Buffer Solution pH 2.8
Acetate Buffer Solution pH 3.4
Acetate Buffer Solution pH 3.5
Acetate Buffer Solution pH 3.7
Acetate Buffer Solution pH 4.0
Acetate Buffer Solution pH 4.6
Acetate Buffer Solution pH 4.7
Acetate Buffer Solution pH 5.0
Acetate Buffer Solution pH 5.5
Acetate Buffer Solution pH 6.0
Ammonia buffer pH 9.5
Ammonia Buffer pH 10.0
Ammonia Buffer pH 10.9
Phosphate Buffer pH 2.0
Phosphate Buffer pH 2.5
Phosphate Buffer pH 3.6
Phosphate Buffer pH 4.0
Phosphate Buffer pH 4.9
Phosphate Buffer pH 5.0
Phosphate Buffer pH 5.5
Phosphate Buffer pH 6.5
Phosphate Buffer pH 6.8
Phosphate Buffer pH 7.0
Phosphate Buffer pH 7.5
Phosphate Buffer pH 8.0
Buffered Isotonic Solutions
Pharmaceutical solutions that are meant for application to delicate membranes of the body should be adjusted to same osmotic pressure as that of body fluids. Isotonic solutions cause no swelling or contraction.
Isotonic solutions cause no contraction or swelling of the tissues with which they come in contact and produce no discomfort when instilled in the nasal tract, eye, blood, or other body tissues.
There are three types of solutions in our body based on solute concentration:
1. Isotonic 2. Hypertonic 3. Hypotonic
Isotonic Solution: In this type of solution the concentration of solutes is the same both inside and outside of the cell. Example- a small quantity of blood is mixed with a solution containing 0.9 g of NaCl per 100 mL, the cells retain their normal size.
Hypertonic Solution: In this type of solutionthe concentration of solutes is greater outside the cell than inside it. Example- the red blood cells are suspended in a 2.0% NaCl solution, the water within the cells passes through the cell membrane in an attempt to dilute the surrounding salt solution.
This outward passage of water causes the cells to shrink and become wrinkled.
Hypotonic Solution: In this type of solutionhe concentration of solutes is greater inside the cell than outside of it. Example- the blood is mixed with 0.2% NaCl solution or with distilled water, water enters the blood cells, causing them to swell and finally burst
Isosmotic Solution Solutions having same osmolarity are known-as isosmotic solution.
Osmolarity: ft is a colligative property that measures the concentration of the solutes independently of their ability to cross a cell membrane.
Tonicity: ft js a property of a solution in reference to a particular membrane, and is equal lo the sum of the concentrations of the solutes which have the capacity to exert an osmotic force across that membrane. Tonicity, also, depends on solute permeability (permeant solutes do not affect tonicity; impermeant solutes do affect tonicity).
Methods used for the measurement of tonicity:
Many drugs and chemicals are used in pharmaceutical formulations. These substances contribute to the tonicity of the solution. Hence, methods are needed to verify the tonicity
and adjust isotonicity. There are two methods used to determine tonicity valve are:
1. Cryoscopic method 2. Hemolytic method
Cryoscopic method: Isotonicity values properties of the solutions. For this purpose, freezing point depression (ATf) property is most extensively used. The freezing point of water is Of 1C, and when any substance such as sodium chloride is added to it, the freezing point of water decreases.
The freezing point of depression of blood is -0.52DC. Hence, the freezing
point depression value of drug solution must be -0.52DC. This solution shows an osmotic pressure equal to the blood.
Hemolytic method: quantitative method developed by Hunter for the measurement of tonicity. Under this method the effect of various solutions on the drug is observed on the appearance of red blood cells suspended in the solutions, RBC’s are suspended in various solutions and the appearance of RBC’s is observed for shrinking, swelling, bursting, and wrinkling of the blood cells.
In hypotonic solutions, the oxyhemoglobin released is proportional to the number of cells haemolysed; in case of hypertonic solutions, the cells shrink and become wrinkled whereas in case of isotonic solutions the cells do not change their morphology. can be determined from the colligative
Methods Of Adjusting Tonicity
Several methods are used to adjust the isotonicity of pharmaceutical preparations. Isotonicity can be calculated from the colligative properties of drug solutions. If solutions injected or introduced in to nose and eyes, these are to be made isotonic in order to avoid haemolysis of RBC’s and to avoid pain and discomfort.
The amount of adjusting agents to be added is easy to determine by using the appropriate calculations based on colligative properties of solutions. It helps to are overcome the side effects caused from administering solutions which contain adjusting agents more or less than isotonic solutions. The methods are divided into three classes.
In the class I methods’ sodium chloride or some other substance is added to the solution of the drug to lower the freezing point of the solution to -0.52°C and thus make it isotonic with body fluids. Under this class are included ihesodium chloride equivalent method and cryoscopic method.
In the class II methods, water is added to the drug in a sufficient amount to form an isotonic solution. The preparation is then brought to its final volume with an isotonic or a buffered isotonic dilution solution. Included in this class are theMzite-Vincent method.
In class III method L iso and Freezing point depression values for number of drugs are estimated theoretically from the molecular weight of the drug and can be used to calculate the amount of adjusting substance to be added in order to make the solution isotonic
Class I Method:
Sodium chloride equivalent method:
It is also called tonicity equivalent method. This method is used to adjust the tonicity of pharmaceutical solutions. Sodium chloride equivalent (E) of a drug is the amount of sodium chloride that is equivalent to1 gm of the drug.
The percent of sodium chloride required for adjusting the isotonidty can be calculated using the following equation.
PSA = 0.9- (PSM x E of medicament) Where,
PSA = Percent of sodium chloride for adjustment of isotonidty
PSM = Percent strength of medicament
Above equation is used to calculate the amount of adjusting substance (NaCl) required for making the solution isotonic. It is valid for 100 ml solution.
Example:- Calculate the gram of sodium chloride needed to make 50 ml of a 3% isotonic physostigmine salicylate solution using sodium chloride method.
Solution:
E value of physostigmine salicylate = 0.16
PSM =3.0 % Volume of preparation required = 50 ml
For equation
PSA = 0.9- (PSM x E of medicament)
= 0.9- (3.0 x 0.16) = 0.9 – 0.32 = 0.42 %
The above strength is valid for 100 ml since is expressed in percent. It should be prepared from 50 ml of solution
For 100 ml of solution, sodium chloride required = 0.42
For 50 ml of solution, sodium chloride required =?
50 x 0.42/100 = 21/100 =0.21 g of sodium chloride
Cryoscopic method:
According to this method, the quantity of each substance required for an isotonic solution can be calculated from the freezing point depression (AT/ ) values.
A solution which is isotonic with blood has a of 0.52DC. Therefore, the freezing point of drug solution must be adjusted to this valve.
For example, the drug concentration in 100ml solution is a gram, then the weight (in grams) of adjusting substance can be calculated as:
ΔTf/ (for drug solution) = ax
ΔTf/ of1% drug solution = x
If w be in grams of the adjusting substance to be added to 100 Ml of drug solution to make it isotonic then:
ΔT/ for adjusting solution = w x ΔT/ of 1% adjusting substance
= wxb
For making a solution isotonic:
x + wb = 0.52
w = 0.52- x/b
or
If sodium chloride is used as adjusting substance whose ATf of solution is 0.58°C (0.576°C), then
W = 0.52-x/0.58
Sodium chloride equivalent (E) and Freezing point depression values of some drugs added substances:
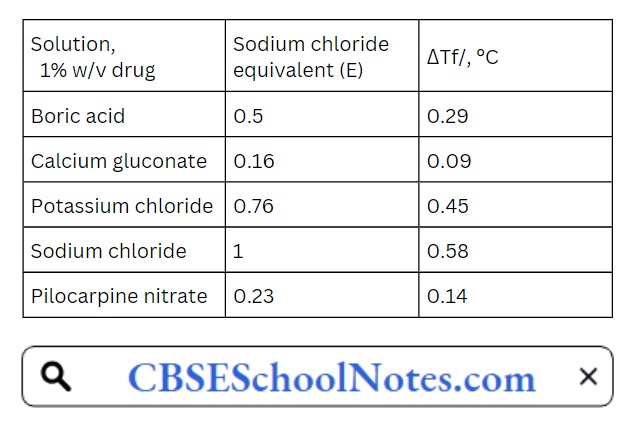
Class-II Method
White-Vincent method:
This method involves the addition of water to the drugs to make an isotonic solution, followed by the addition of an isotonic or isotonic-buffered diluting vehicle to bring the solution to the final volume.
Stimulated by the need to adjust the pH in addition to the tonicity of ophthalmic solutions. White -Vincent developed a simplified equation for calculating the volume V (mis) of osmotic solution prepared by mixing drug with water.
V = wxEx 111.1
Where, w = weight of the drug (gm)
E = sodium chloride equivalent
Class-lll Method
The L ISO Method: According to this method the freezing point depression equation is used to calculate the amount of the isotonicity-adjusting substance that must be added to hypotonic solution of drug to bring to tonicity.
As the freezing than those calculated by the point depression for solutions of electrolytes are equation, ΔTf/= Kfm, a new constant L iso is introduced to account for this deviation.
The equation then becomes
ΔTf = L iso C
The following equation helps to calculate the E Nacl value from L iso value of the substances. The ΔTf of 1 g of drug per 100ml of solution is equal to L iso C.
Therefore,
ΔT/ = L iso l(gm)/M
= L iso/M
Where, M is molecular weight of solute and M and L iso value of Nacl is 3.4,
ΔT/= 3.4 x E/58.45
L ISO Values of the Tonicity adjusting substances
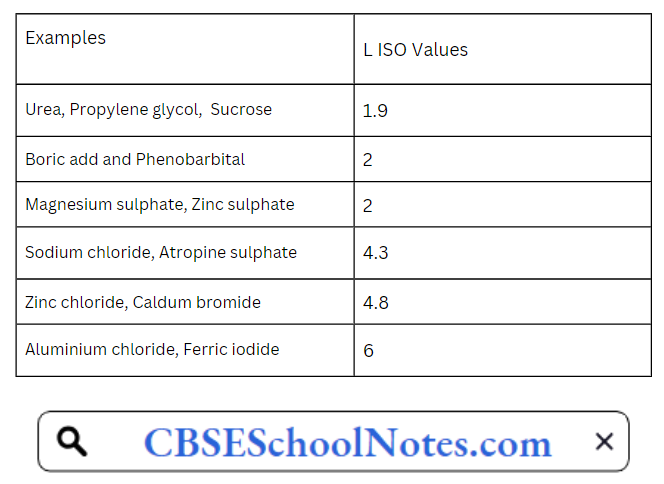
Acids Bases And Buffer Very Short Answer Questions
Question.1. Define the following terms :
- Acid
- Base
- pH
- Buffer solution
Answer.
- Acid is a substance which has sour taste and it turns blue litmus red.
- Base is a substance which has bitter taste and it turns red litmus blue.
- pH is defined as the negative logarithm (to the base 10) of hydrogen ion concentration. It is expressed as:
pH = -log10[H+] - Buffer solutions are defined as those solutions which are able to resist the change in pH value.
Question 2. What are conjugate acid-base pairs?
Answer. Conjugate acid-base pairs are defined as such pairs of substances which can be formed from one another by the gain or loss of proton.
Question 3. What is the pharmaceutical use of calcium hydroxide?
Answer. Calcium hydroxide is used as a substitute for baking soda. It is also used for processing water for alcoholic beverages eg. Soft drinks.
Question .4. What is Acidosis?
Answer. Acidosis is defined as those condition in which the pH of the blood falls below 7.3.
Question 5. How many type of buffer solutions are there? Explain.
Answer. There are many types of Buffer solution :
- Acidic Buffer
- Basic Buffer
Acidic Buffer Solution: The solution having a mixture of weak acid and its salt.
For example: Mixture of Acetic acid and Sodium Acetate.
Basic Buffer Solution: The solution having a mixture of weak base and its salts.
For example: Mixture of ammonium hydroxide and ammonium chloride.
Question.6. Write down the preparation and uses of boric acid?
Answer. Boric acid is prepared by reacting hydrochloric or sulphuric acid with the native borax to produce orthoboric acid.

Boric add is for used in dusting powders,lotions and creams.It can be used as an anti spectic for minor burns or cuts and is sometimes used in dressings or shaves.
Question.7.comment on the statement that “All Arrhenius acids are also bronsted acid but all arrhenius bass are not bronsted bases”.
Answer. According to Arrhenius concept, an acid is a substance that dissociated completely to give hydrogen ions when dissolved in water same is with lewis acid which is a proton-donor while a base is a substance that dissociates to give hydroxyl ions when dissolved in water
Question.8 Which concept denis with “Eleclron-Donor-Acceptor System”?
Answer. Lewis Concept deals with the electron donor -acceptor system.
Question 9 Write a balanced equation for a neutralization of acid and base?
Answer. According to neutralisation reaction, these two ions (H+ and OH”) combine to form solvent (i.e. water ) and a salt ( NaCl). these can be represented by the following equation:-
HCL (acid) + NaOH (base)———-> NaCl (salt)+ H2O (water)
Acids Bases And Buffer Short Answer Questions
Question 1. How are acid and bases defined in terms of :
- Arrhenius concept
- Lewis concept? Give suitable examples.
Answer:
1) Acording to Arrhenius concept, an acid is a substance that dissociates to give . hydrogen ions when dissolved in water while a base is a substance that dissociates to give hydroxyl ions when dissolved in water.

2) Lewis acid may be defined as any species (molecule, radical or ion) that can accept an electron pair to form a coordinate bond while a base may be defined as any species ( molecule, radical or ion) that can donate an electron pair to form a coordinate bond.
Question 2. What do you understand by the term “conjugated acid base pair”? Show that “a strong acid has a weak conjugate base and a weak acid has a strong conjugate base”.
Answer:
Conjugate acid- base pairs are the pairs of substances which can be formed from one another by the gain or loss of a proton.Thus conjugate of an acid is the substance which can be formed by the loss of a proton while conjugate of a base is the substance which can be formed by the gain of a proton.
Let us consider a reaction of acetic acid in water which may be represented as:-

Acetic acid donate a proton to water and thus acts as an acid. Water accepts a proton and therefore acts as an base. In the reverse reaction, hydronium ion donate a proton to the acetate ion and therefore acts an acid. The acetate ion accepts a proton and therefore behaves as an base.
Question 3. What is Buffer Solution? How many types of Buffer solutions are there? Explain.
Answer:
Buffer solutions are defined as those solutions which are able to resist the change in pH value. Buffer solution consists of a mixture of weak acid and its weak base and its salt.
There are many types of Buffer solution :
- Acidic Buffer
- Basic Buffer
- Neutral Buffer
Acidic Buffer Solution: The solution having a mixture of weak acid and its salt. For example: Mixture of Acetic acid and Sodium Acetate.
Basic Buffer Solution: The solution having a mixture of weak base and its salts. For example: Mixture of ammonium hydroxide and ammonium chloride.
Neutral Buffer Solution: The solution having a mixture of weak acid and weak base. Forexample: Mixture of acetic acid and ammonium hydroxide.
Question 4. What is Buffer capacity? Explain the mechanism of Buffer action?
Answer:
The property of buffer solution to resist any change in its pH value, even when small amount of acid or base is added to it is known as “Buffer action”.
Question 5.Describe method of preparation, properties and uses of calcium hydroxide?
Answer: Calcium hydroxide
Molecular formula=Ca(OH)2 Molecular Weight =74.09
Calcium hydroxide is prepared by spraying water on to quicklime which is itself prepared by heating limestone. The lumps of quicklime break into powder and heat is evolved
CaCO3 ——–>CaO+CO2
It occurs as odourless. It is having bitter saline taste.
It is internally used as antacid. It is used in dentistry
Acids Bases And Buffer Fill In The Blanks
1. Buffer solutions are those which resist the change in …….
Answer: pH
2. Measurement of pH can be done using…….
Answer: pH-meter
3. pH of blood in human body is about…….
Answer: 73-7.4
4. Add turns…..litmus……
Answer: Blue, red
5. Base has ……..taste.
Answer: Bitter
6. According to Bronsted lowry concept, an acid is…… while base is……
Answer: Proton-acceptor, proton donor
7. Soft acids have…….size while hard base have……size.
Answer: Smaller, larger
8. The value of hydrogen ion cone, is……..while
Answer: 1.0×10-7
9.If [H+] is High; the solution is ————–while If [H+] is low; the solution is…….
Answer: Acidic, basic
10………is also known as slaked lime.
Answer: Calcium hydroxide
Acids Bases And Buffer Multiple Choice Questions
Question 1. Which of the following is not a properties of acid?
- Taste sour
- Turn blue litmus red
- React with base to form water
- Feel slippery on the skin
Answer: Feel slippery on the skin
Question 2. Which of the following is not a property of base?
- Taste bitter
- Turn blue litmus red
- React with salts to form acid
- Feel slippery on the skin
Answer: React with salts to form acid
Question.3.In general when an acid and a base are mixed
- A new add and a salt are formed
- A new base and a salt are formed
- No reaction occurs
- A salt and water are formed
Answer: A salt and water are formed
Question.4.Which of the following equations best represents what happens when hydrogen bromide dissolves in water
Answer:
![]()
Question.5.What is the pH of a solution that has a hydrogen ion cope, of lxJOÿM?
- 4
- 6
- 9
- 3
Answer: 3
Question.6.Which of the following pair is a conjugate acid-base pair?
- CH3COOH and OH-
- HCN and CN-
- HCN and OH-
- HC1 and OH-
Answer: HCN and CN-
Question 7. Which buffer is used for maintaing acid-base balance in the blood?
- Carbonic acid – bicarbonate ion
- Acetic acid and sodium acetate
- Ammonium hydroxide-ammonium chloride
- Formic acid-sodium formate
Answer: Carbonic acid – bicarbonate ion
Question.8. Sodium hydroxide is commonly known as
- Slaked lime
- Spirit of salt
- Caustic soda
- Quick lime
Answer: Spirit of salt
Question.9. If the pH of the blood falls below 7.3, the condition is termed as:-
- Acidosis
- Alkalosis
- Neutral
- None of the above
Answer: Acidosis
Question.10. Strong ammonium hydroxide is prepared by
- Salvay process
- Merck process
- Haber’s process
- Ammonia soda
Answer: Merck process
List of Gastrointestinal Agents
Gastrointestinal Agents
The gastrointestinal tract or digestive tract also referred as the GI tract or the alimentary canal. Gastrointestinal System is responsible for the breakdown and absorption of various foods and liquids needs to sustain life.
GI tract starts with the mouth and proceeds to the esophagus, stomach, small intestine (duodenum, jejunum, ileum), and then to the large intestine (colon), rectum, and terminates at the anus. This section covers the discussion about certain important topics :
- Acidifying Agents or Acidifiers
- Antacids
- Protective and Adsorbents
- Saline Cathartics
Acidifying Agents Or Acidifiers
Acidifying agents are the inorganic chemical substances that either produce or increase acid. These chemicals increase the level of gastric acid in the stomach when ingested, thereby decreasing the stomach pH. It is broadly classified into four categories:-
Read and Learn More Pharmaceutical Inorganic Chemistry Notes
- Gastric Acidifiers: These are the drugs which are used to increase the acidity of the stomach in patients suffering from Achlorhydria or Hypochlorhydria (absence or insufficient quantity of HC1 acid in the gastric secretion). It responds to stimulation by histamine. The Achlorhydria patients are of two types
- Those who do not respond to histamine phosphate stimulation for the release of HC1.
- Those who respond to histamine phosphate stimulation for the release of HC1 in the stomach. In either of the cases, the G.I. disturbances i.e. frequent bowel movement, mild diarrhoea, epigastric pain and sensitivity to spicy foods are the common symptoms. It is used to control the pH of the acidic stomach (pH 1.5-3.5). This condition is best treated by the administration of HC1 acid.
- Urinary Acidifiers: These are the drugs which are used to remove acidic urine from the body or to maintain the pH of the urine. These acidifiers are widely used to cure some types of urinary tract infections.
For example: Many bacterias are grown badly in acidic urine as far as urine is cemed. Hexamine only acts as antiseptic when the urine is acidic. In acidic media, hexamine itself break up into ammonia and formaldehyde. - Systemic acidifiers: These are the drugs which are able to neutralise the alkaline body fluids, especially blood or to maintain the pH of all parts of the body. It is used to treat patients suffering from systemic alkalosis.
- Acid: These are used as pharmaceutical aids in the preparation of medicaments, laboratory quality control.
Hydrochloric Acid
Molecular formula ;HCl Molecular Weight:36.46
Synonym: Spirit of Salt, Muriatic acid
Preparation
It can be prepared by the action of cone. Sulphuric acid on Sodium Chloride and passing the liberated Hydrogen Chloride through water.

In this method, the hydrogen and chlorine obtained in the electrolysis of sodium chloride in the manufacture of caustic soda are burnt, preferably using quartz bunsen burners.

100% pure HC1 is formed in this method
Properties
- It is nearly colourless clear and fuming liquid.
- It possesses pungent odour.
- It is soluble with water and alcohol.
- It is a strong acid and attacks metals, forming the hydrochlorides with the evolution of gas.
Chemical Properties
1. It reacts with Sodium metal which results in the formation of sodium chloride and liberates hydrogen gas.

2. It is oxidised by strong’ oxidising agents liberating chlorine gas.

Assay
An accurately weighed sample of the add is diluted with water and titrated with 1M NaOH using methyl red solution as the indicator. End point is the appearance of a faint yellow colour.
Storage
It is stored in well dosed container of glass or other inert material at a temperature not exceeding 30°C.
Uses
- It is used as a Pharmaceutical Aid.
- It is also employed as an atidifying agent or addifier.
It is also used to inactivate the proteolytic enzyme, pepsin. Certain antadds like Sodium Bicarbonate which are water soluble may raise it pH above 7. The continual hyperacidity may lead to peptic or duodenal ulcer.
Test for Purity
It has to be tested for As, heavy metals, bromides, iodide, sulphate & free iodine.
Ammonium Chloride
Molecular formula: NH4Cl Molecular Weight: 53.9
Ammonium chloride contains not less than 99.5% of NH4C1, calculated with referene to substance dried over silica gel for 4 hours.
Preparation
- It is prepared by purifying the crude product by sublimation or by boiling ammonium sulphate solution with sodium chloride in the equivalent proportions.
- Neutralization of HC1 acid with ammonia and evaporation of solution to dryness yield ammonium chloride.
Properties
- It is white, fine or coarse crystalline powder.
- It is having a cooling saline taste.
- It is odourless.
- It is sligthly hygroscopic.
- It is soluble in 2.6 parts of H20, 1.4 parts of boiling water & 100 parts of alcohol.
Test for Purity
Test for arsenic, heavy metals, lead, iron, barium sulphate, thiocyanate, loss on drying and non-volatile matter.
Assay
Weigh accurately about 0.2g, dissolve in 40ml of H2O, add 3 ml of Nitric acid, 5 ml of Nitrobenzene & 50 ml of 0.1N Silver nitrate, shake vigorously for 1 minute & titrate with 0.1N
ammonium thiocyanate using 2ml of solution of ferric ammonium sulphate as indicator.
Each ml of 0.1N silver nitrate is equivalent to 0.005349g of NH4Cl.
Uses:
- It is used as an expectorant.
- It is used as a diuretic & systemic acidifying agent.
- It is used to maintain the urine at acid pH in the treatment of some UIT disorders.
Review Questions
Very Short Answer Questions
Question. 1. Define Acidifying agents?
Answer. Acidifying agents are the inorganic chemical substances that either produce or increase acid in the g.i.t. tract.
Question 2. Write down the classification of Acidifying agents?
Answer. Acidifying agents can be broadly classified as :-
- Gastric acidifier
- Urinary acidifier
- Systemic acidifier
- Acids
Question 3. What is the difference between Urinary Acidifier and Systemic Acidifier?
Answer. Urinary Acidifiers are the drugs which are used to remove acidic urine from the body or to maintain the pH of the urine while Systemic Acidifiers are the drugs which are able to neutralise the alkaline body fluids especially blood.
Question 4. What do you understand by Systemic Acidifiers?
Answer. Systemic Acidifiers are the drugs which are able to neutralise the alkaline body fluids especially blood.
Question 5. By which other names Hydrochloric acid is also known?
Answer. Spirit of salt, Muriatic acid
Question 6. How would you prepare Hydrochloric acid?
Answer. Hydrochloric acid can be prepared by the action of cone. Sulphuric Acid on Sodium Chloride and passing the librated Hydrogen Chloride through water.
NaCl + H2SO4—————–>NaHSO4+ HCl
Question.7. What is Achlorhydria?
Answer. Achlorhydria is the absence or insufficient quantity of HC1 acid in the gastric secretion.
Question.8. What are the pharmaceutical uses of Hydrochloric Add?
Answer. Hydrochloric Acid is used as a pharmaceutical aid, as acidifying agent or acidifier.
Fill In The Blanks
1. Acidifying agents are the inorganic chemical compounds that either………… in the g.i.t. tract.
Answer: Produce or increase acid
2. Gastric acidifier are the drugs which are used to……………..the acidity of the stomach.
Answer: Increase
3……………….are the drugs which are used to remove acidic urine from the body or to maintain the pH of the urine.
Answer: Urinary acidifer
4……………….are the drugs which are able to neutralise the alkaline body fluids.
Answer: Systemic acidifier
5. Hydrochloric acid is also known as………………
Answer: Spirit of salt, Muriatic acid
6. Hydrochloric acid can be prepared by the action of…………………on…………………….
Answer: Cone, sulphuric acid, Sodium chloride
Antacids
Antacids are the substances which are used to neutralise the gastric acidity. Antacids occur due to excessive secretion of HC1 in stomach due to various reasons. They produce sympathomimetic relief from pain, heart burns or by neutralizing the excess of hydrochloric acid.
Peptic ulcers occur due to defective oesophageal sphincter as hiatal hernia. Gastric ulcers occur in lesser curvature and are found in first portion of duodenum.
The neutralizing capacity of an antacid is expressed in milliequivalents (mEq) of hydrochloric acid. Every antacid may have a total neutralizing capacity of atleast 5 mEq of HCl per
dosage unit.
Antacids raise the pH of the gastric contents to above 3.5.
Antacids may be classified as
- Systemic (absorable) antacids: These are soluble, readily absorable and capable of producing systemic electrolytic alterations and alkalosis. Example: Sodium Bicarboante.
- Non-systemic (Non-absorable) antacids: These are not absorbed to a significant extent and thus do not exert an appreciable systemic effects e.g. Aluminium salts, Magnesium
salts and Calcium Carbonate.
Ideal Characteristics of Antacids :
- The antacid should not be absorbable or cause systemic alkalosis.
- The antacid should not be a laxative or cause constipation.
- The antacid should exert its effect rapidly and over a long period of time.
- The antacid should probably inhibit pepsin.
- The antacid should have buffer in the pH range of 4-6.
- The reaction of the antacid with gastric hydrochloric acid should not cause a large evolution of the acid.
Sodium Bicarbonate
Molecular formula: NaHCO3 Molecular Weight: 84.01
Synonyms
Sodium Hydrogen Carbonate, Baking Soda, Mitha Soda.
It is highly water-soluble antacid with a very rapid onset of action but relatively short duration.
Preparations
On small scale, it is prepared by passing C02 gas through a solution of sodium hydroxide.
Solvay Process (Ammonia Soda Process)
Strong solution of Sodium Chloride containing a high concentration of ammonia is passed thorugh a carbonating tower where it is saturated with CO2 gas under pressure.
Ammonia and Carbon Dioxide react to form Ammonium Bicarbonate which further undergo decomposition to form Sodium Bicarbonate.
It is specific in the treatment of systemic acidosis.
Official test for identity.
- Gives the reaction characteristic of sodium and of bicarbonate.
- To a solution of the substance in C02 free water, phenophthalein solution is added. A pale link is produced.
Physical Properties
- It occurs as white crystalline or amorphous powder.
- It is having a saline taste.
- Its solution is alkaline in nature.
- Its freely soluble with water but practically insoluble in alcohol.
Assay
Weigh accurately about 0.6gm of sodium carbonate, previously dried, dissolved in 50 ml of water and titrate with 0.5 ml/HCl acid (Indicator : 3 drops of bromophenol blue TS).
Test for Purity
Test for alkalinity, aluminium, calcium, insoluble matter, arsenic, iron, lead, chloride, sulphate, ammonium compounds.
Uses
It is mainly used as an Electrolyte Replenisher. It is mainly used for its Acid Neutralizing properties. It is also find used as an antacid. It is used as local applicant for bums, insect bites etc.
Aluminium Hydroxide Gel
Chemical formula : Al(OH)3 Molecular Weight: 77.99
Synonym
Aluminium Hydroxide Powder, Aluminium Hydrated Powder
It can be recognized into two ways
- Aluminium Hydroxide Gel
- Dried Aluminium Hydroxide Gel
Aluminium Hydroxide Gel :
It is a white viscous suspension of Hydrated Aluminium Oxide with varying amounts of basic Aluminium Carbonate. It gets separated into the clear liquid on standing for sometime.
It exhibits suitable flavouring and antimicrobial agent. It has a pH between 5.5 and 8.0.
Preparation
When an Aluminium Salt such as Aluminium Chloride is treated with Ammonia or Sodium Carbonate, a white gelatinous precipitate of aluminium hydroxide is obtained.
After complete removal of CO2, the precipitate Aluminium Hydroxide is filtered, washed throughly with hot water untill it become free from sulphates ions. The precipitate may be
suspended in the purified water to strengthen aluminium hydroxide gel.
Dried Aluminium Hydroxide Gel
Synonyms
Aluminium Hydroxide powder.
Properties
It is not a typical gel but is a white, odorless, tasteless, amorphous powder. It is insoluble in water and alcohol but soluble in dilute mineral acids & solution of fixed Alkali Hydroxides.
It forms gel on prolonged contact with water. It absorbs certain acids and CO2 It has a pH between 5.5-8.0
One major drawback of gel is that of a loss of antacid properties on aging.
Test for purity
Tests for arsenic, ammonium salts, chloride, lead, sulphate, alkalinity neutralising capacity, viscosity. The presence of ammonium salt is determined by heating the substance with Sodium Hydroxide to yield Ammonia which is collected in standard acid and back titrated by the usual procedure.
The limit of Ammonia in Aluminium Hydroxide is determined to be 0.034%. An aqueous solution after addition of HQ acid complies with the limit test for Chlorides. Neutralising capacity is found by measuring pH suspension of the substance in a radium which is approximate N/20 in resp. of HQ acid.
Storage
It should not be stored at a temperature not exceeding 25°C and should be stored in air tight containers.
Calcium Carbonate
Chemical Formula: CaC03 Molecular Weight: 100.09
Synonyms
Precipitated Chalk, Precipitated Calcium Carbonate. It is found in nature as the lime stone, marble calcite, vaterite, aragonite and shell of sea animals.
Method of Preparation
It can be prepared by mixing the boiling solutions of Calcium Chloride and Sodium Carbonate and allowing the resulting precipitate to subside on cooling.
![]()
Properties
It occurs as a white, odorless, tasteless, microcrystalline powder. It is practically insoluble in air but solubility is increased by the presence of Carbon Dioxide and also by Ammonium
salts (except Ammonium Carbonate).
It is stable in air. It exists in two crystal form and both are of commerical importance, one Aragonite and other is Calcite.
Uses
It is used as fast-acting antacid, in calcium deficiency, dentrifices and in combination with magnesium containing antacids due to its constipative properties.
Magnesium Hydroxide
Synonyms: Milk of magnesia
Molecular formula: Mg(OH)2 Molecular weight: 58.31
Molecular weight: 58.31
Preparation
It is prepared by Combining a solution of many magnesium salts with basic water induces precipitation of solid Mg(OH)2:
![]()
On a commercial scale, Mg(OH)2 is prepared by treating seawater with lime Ca(OH)2.
![]()
Properties
It occurs as white, odourless powder. It is soluble in dilute acids and practically insoluble in ethanol and water.
Uses
It is used as a laxative to relieve constipation.
It is also used to treat gastrointestinal ailments such as heartburn, general upset stomach, or feelings of indigestion.
Review Questions
Very Short Answer Questions
Question. 1. Define Antacids?
Answer. Antacids are the drugs which are used to neutralize the gastric contents.
Question.2. How do antacids occur?
Answer. Antacids occur due to excessive secretion of hydrochloric acid in stomach.
Question.3. Classify Antacids?
Answer. Antacids can be classified into two categories :
- Systemic antacids
- Non-systemic antacids
Question.4. What is Systemic Antacid?
Answer. Systemic Antacid is readily absorable and capable of producing systemic electrolytic alterations and alkalosis. For example: Sodium bicarbonate
Question.5. What is Non-Systemic Antacid?
Answer. Non-systemic Acid is absorbed to a significant extent and thus do not exert an appreciable systemic effects.
For example : Aluminium salts such as Aluminium hydroxide gel, Calcium Carbonate.
Question.6. What do you understand by Neutralizing Capacity?
Answer. The Neutralizing Capacity of an antacid is expressed in milliequivalents (mEq) of hydrochloric acid.
Question.7. Enlist various inorganic compounds which are used as an Antacids?
Answer. Aluminium Hydroxide, Sodium Bicarbonatem Magnesium Oxide, Calcium Carbonate.
Question.8. What is the chemical formula for
- Sodium bicarbonate
- Calcium carbonate
Answer.
- NaHC02
- CaCO3
Question.9. By which other names Magnesium Oxide is known?
Answer. Magnesia.
Question.10. How would you prepare Magnesium Carbonate?
Answer. Magnesium Carbonate is prepared by mixing hot solution of Magnesium Sulphate and Sodium Carbonate. The precipitate is collected and washed with water and then
dried.
Question.11. What are the Pharmaceutical uses of Sodium Bicarbonate?
Answer. Sodium Bicarbonate is used as fast acting antacid in dentrifices. It is used as a local applicant for bums, insect bites etc.
Question.12. How would you prepare Sodium Bicarbonate?
Answer. Sodium Bicarbonate can be prepared by mixing the hot solution of Calcium Chloride and Sodium Carbonate and allowing the resulting precipitate to subside on cooling.

Question.13. How would you prepare Magnesium Oxide?
Answer. Magnesium Oxide can be prepared by heating gently Magnesium Carbonate on redness.

Question.14. What are the ideal characteristics of an Antacids?
Answer.
- Antacid should be absorable or cause systemic alkalosis.
- Antacid should probably inhibit pepsin.
- It should exert its effect rapidly and over a long period of time.
Fill In The Blanks
1. Antacids are the drugs which are able to……………..
Answer: Neutralize the gastric contents
2. Systemic antacid is…………….in nature while non-systemic antacid is ……………….
Answer:Absorbable, non-absorable
3. Example of systemic antacid is……………
Answer: Sodium Bicarbonate
4. Neutralizing capacity of an antacid is expressed in…………….
Answer: Milliequivalents of hydrochloric acid
5. Magnesium oxide can be prepared by heating………….on redness.
Answer: Magnesium Carbonate
6. Sodium bicarbonate is used as……………………
Answer: Dentrifice, in Calcium deficiency
7……………………..are the inorganic compounds which are used as Antacids.
Answer: Magnesium Carbonate
8. Magnesium oxide is also known as………………….
Answer: Magnesia
9. Magnesium carbonate is prepared by mixing ……………and……………….
Answer: Magnesium Sulphate, Sodium Carbonate
10………..is the aluminium containing salt as antacids.
Answer: Aluminium hydroxide gel.
Saline Cathartics
Cathartics waif he defined as those drugs which are used to bring about defecation i.e. emptying of the stomach.
Cathartics are used to
- To relieve from acute constipation.
- To ease in daefecation of patients suffering from harmful haemorrhoids or other rectal disorders.
- To clear bowels from stomach before surgery.
Laxatives are mild Carthatics while Purgatives are used for strong Carthatics. They act both by retaining fluids in the bowel. They should not be used on a regular basis because
they can cause water and electrolyte imbalance.
Stimulants, Bulk-forming, Emollients and Saline carthatics are the four types of laxatives. They may be administrated either by oral route (such as suspension or powder) or by rectal route (such as enema or suppository).
Inorganic compounds such as Sodium Potassium Tartarte and Magnesium Sulphate as widely used as Saline Carthatics
Classification
Laxatives can be conveniently classified into five categories :
Stimulant Laxatives: These act on the intestinal tract to increase its motor activity e.g. phenolphthalein, castor oil.
Saline Laxative: A number of magnesium salt as well as sulphate, phosphate and tartartes are used as saline laxative/carthatic. These cations and anions are not absorbed or slightly absorbed from the gastro intestinal tract.
Bulk-forming laxatives: These include natural and semisynthetic polysaccharides and cellular derivatives that are only partially digested. The undigested portion is hydrophilic & swells in presence of water to orm viscous gel.
Lubricant laxatives: These drugs (mineral oil & vegetable oil) lubricate the intestinal tract, soften the faecal contents & lubricate the passage of faeces.
Pecal softeners: Substance in this category are wetting agents e.g. docusate sodium which are non-absorbable & relatively non-toxic.
Mode of action: The saline carthatics act by increasing the osmotic load of GIT. These carthatics are salts of poorly soluble anions and cations. The body relieves hypertonidty off
the gut by secreting additional fluid into the intestinal tract.
This result is increased bulk in GIT. The resulting increasing bulk stimulates peristalsis. The saline carthatics are water soluble
and are taken with large amounts of water.
Magnesium Sulphate
Molecular Formula: MgS04.7H20 Molecular Weight: 246.5
Synonyms: Epsom salt, Magnesium sulphate
Method of Preparation
It is obtained by the action of dilute Sulphuric Acid on Magnesium Carbonate or Magnesium Oxide. The solution obtained is filtered off and then evaporated to crystallisation.
 Properties
Properties
It occurs as odourless, brillant, colourless crystals or white crystalline powder. It is having a bitter saline and cooling taste. It efflorescenes in warm dry air. It is soluble in water and
sparingly soluble in alcohol. When gently heated, it readily loses its water of hydration and is converted to monohydrate which quickly becomes anhydrous to 200°C.
Assay
This is a volumetric method and a complexometric assay. It is assayed by the titration of the substance against M/20 sodium edetate (disodium salt of ethylene diaminetetraacetic acid) using mordant black mixture, as indicator.
A mixture of strong ammonia and ammonium chloride is used as the buffer. The end point is the appearance of blue colour.
Storage
It should be stored in a well closed container because of its efflorescent nature.
Uses
It.acts as a saline laxative. It is also used in the treatment of magnesium deficiency, cholecystis (inflammation of gall bladder), hypertension and boils.
Sodium Orthophosphate
Molecular formula: Na2HPO4.12H20 Molecular Weight: 358.14
Synonyms: Phosphor soda
Method of Preparation
1. It is prepared by reaction of Orthophosphoric Acid with Sodium Hydroxide.
![]()
2. From bone ashes or mineral phosphorite, which is then treated with Sulphuric Acid.
Properties
It is colourless odorless, and crystalline powder. It is efflorescent. It is soluble in water and practically insoluble in alcohol.
Uses
It is used as a Pharmaceutical Aid and as a Saline Carthatic. It is used as a Buffering Agent.
Bentonite
Chemical Formula: Al2O3.4SiO2.H2O
Synonyms: Clay
It is a natural, colloidal, and an absorbent aluminium phyllosilicate consisting mostly of montmorillonite, Al2O3.4SiO2.H2O. It may also contain magnesium, calcium and iron. Volclay bentonite is its most common type composed of about 90% montmorillonite [Al2Si4O10(0H)2.nH20]. Other components such as feldspar [K20.Al2O3.6SiO2] and aluminosilicate containing Al2O3 , CaO, SiO2, MgO and soma K and Na.
Properties
It occurs as very fine odourless, cream coloured to greyish powder white. It is slightly earthy in taste. It is insoluble in water but soluble in organic solvents. It is stored in tightly closed containers
Uses
It is used as filler in pharmaceuticals, and due to its absorption/adsorption functions, it allows paste formation. It is also used as suspending agent.
Kaolin
Al2O3.2Si02.2H2O
Kaolin (China clay) is purified, natural, hydrated aluminium silicate of variable composition. It is derived from the decomposition of feld spar of granitic rocks. Kaolin consists of aluminium silicate with traces of compound of magnesium, calcium & iron.
Preparation
Kaolin is prepared when rock is mined, exacavated and the impurities are washed with water and then powdered. The rock is elutriated with water and large-sized particles separated. The turbid liquid is allowed to settle, heavy Kaolin containing the large particles & colloidal Kaolin containing particles of small size are separated & dried.
Properties
Kaolin has an earthy or clay-like taste. Its colour may be tinged grey, yellow brown, blue or red due to impurities. It is unctuous & soapy to touch. It is not affected by dil. HC1 or HNO3 acid but is decomposed by the prolonged boiling or treatment with cone. H2S04.
Heavy Kaolin
It is purified natural form of variable composition. Its particles are 20 pm in diameter, flat 7 irregularly arranged. With water plastic-like form is obtained which is less sticky. It is fine white or greyish-white earthy mass or powdder.
It is practically insoluble in water & in organic solvents. When the aqueous suspension is kept for sometime, the whole Kaolin settles below leaving clear supernatant liquid.
Light Kaolin
It is a native form, freed from most of its impurities by elutriation & dried. It contains a suitable dispensing agent. The particles are small, less than 2pm in diameter & have various
shape 4 size. Natural light Kaolin is a Kaolin which does not contain a dispensing agent.
Uses :
- Kaolins are adsorbent, anti-diarrhoeal and when given by mouth.
- Light Kaolin is used as a dusting powder food additive.
- They are employed in the sympathomatic treatment of diarrhoea & to coat irritated intestinal mucosa in case of diarrhoea.
Activated Charcoal
It is obtained from burning of organic material and as a residue during destructive distillation of various organic matter. The coarse material is crushed & powdered.
Alternatively, raw vegetable material may be treated with a solution of Zinc Chloride and Phosphoric acid and ignited to get the activated charcoal. The inorganic matter is removed by washing.
Properties
It is a fine black, odourless and tasteless powder having smooth touch & free from gritry particles. The fine powder provides more surface area for adsorbent properties.
Uses
It is a general typee of adsorbent which finds use in poisoningg. It also finds use in diarrhoea to absorb toxins.
Review Questions
Very Short Answer Questions
Question. 1. Define Cathartics.
Answer. Carthatics may be defined as those drugs which bring about defecation emptying of the stomach.
Question.2. Define Laxatives.
Answer. Laxatives are defined as those drugs which are used as mild carthatics.
Question.3. What is Purgative?
Answer. Purgative is defined as those drug which is used as a strong carthatic.
Question.4. Enlist various inorganic compounds which are widely used as Laxative or Purgative?
Answer. Manesium sulphate, sodium potassium tartarte.
Question.5. How do Laxative and Purgative act?
Answer. Laxative and Purgative act by retaining fluid in the bowel.
Question.6. How many types of laxatives are there?
Answer. There are four types of laxative
- Stimulant
- Bulk-forming
- Emollient
- Saline carthatics
Question.7. What is the chemical formula of Magnesium Sulphate?
Answer. MgSO4.7H2O
Question 8. What is the method of preparation of Magnesium Sulphate?
Answer. It is prepared by the action of dilute Sulphuric Acid on Magnesium Carbonate or Magnesium Oxide.The solution obtained is filtered off and then evaporatedto crystallise it.
Question.9. What are the side effects of Magnesium Sulphate when consumed in excessive amount?
Answer. Excessive use of Magnesium Sulphate causes hypermagnesaemia, gastro-intestinal irritation and watery diarrhoea.
Question.10. What is the molecular weight and molecular formula for Sodium Potassium Tartarte?
Answer. Chemical formula for Sodium Potassium Tartarte is C4H4KNa06.4H20 while molecular weight is 283.23.
Question.11. What are the other names for Sodium Potassium Tartrate?
Answer.
Potassium sodium tartarte.
Rochelle salt, Seignette’s salt
Question.12. How would you prepare Sodium Potassium Tartrate?
Answer. It is prepared by reaction of boiling solution of Potassium Bitartarte with Sodium Carbonate for sometime. The solution obtained is filtered, concentrated and crystallized.

Fill In The Blanks
1. ………..are used to bring about defecation.
Answer: Carthatics
2. Carthatics are used to………..
Answer: To relieve constipation
3. Laxatives are………… carthatics while Purgatives are………….. carthatics.
Answer: Mild, strong
4. Other names for Sodium Potassium Tartarte are…………..
Answer: Rochelle salt, Seignette’s salt
5 Chemical formula for Sodium Potassium Tartarte is……………..
Answer: C4H4KNa06.4H20
6. ……………… Inorganic compounds are used as saline carthatics.
Answer: Magnesium Sulphate;Sodium Potassium Tartarte
7. Excessive used of Magnesium Sulphate as saline Carthatics causes………………
Answer: G.i.t irritation and waking diarrhoea
8. Epsom salt is………………….
Answer: Magnesium sulphate
9……………………..is obtained by action of dilute Sulphuric Acid on Magnesium Carbonate.
Answer: Magnesium sulphate
10……………..is used as food additives in the preparation of meat & in cheese industry.
Answer: Sodium Potassium Tartarte
Expectorants And Emetics Notes
Expectorants And Emetics Introduction
Cough, a protective reflux (both voluntary and involuntary) helps to expel irritant matter from the respiratory tract. When a person coughs there is a short intake of breath and the larynx closes momentarily.
It is a vital part of the defence mechanism. It can be caused by infections, chemical irritants, asthma, lung tumour, breathing in dust particles. It is of two types
Productive Cough: A productive cough produces a phlegm or mucus (sputum). The mucus may have drained down the back of throat from the nose or from the lungs. A protective cough should not be supressed. It clears mucus from the lungs.
Irritative or Non-productive cough: A non-productive cough does not produce sputum. A dry, hacking cough may develop towards the end of a cold or after exposure to an irritant such as dust and smoke.
Expectorant
The latin word ‘Expectorate’ means ‘to drive from the chest’. Expectorants are drugs used to help in the removal i.e. explusion of secretions or exudate from the trachea, bronchii or lungs. Hence, they are used in the treatment of cough. They act upon the respiratory tract in two ways
By decreasing the viscosity of the bronchial secretion and facilitating their elimination;local irritants are expelled and ineffectual coughing is required.
By increasing the amount of respiratory tract fluid, a demulcent action is exerted on dry mucosal lining & relieving the unproductive cough.
Inorganic saline expectorants are:- Ammonium salts (Ammonium Chloride), iodide (Potassium/Sodium Iodide), citrates and Antimony Potassium Citrate.
Read and Learn More Pharmaceutical Inorganic Chemistry Notes
Potassium Iodide
Chemical Formula: KI Molecular Weight:166.01
Synonyms: Kalii Iodidum, Pot. Iod.
Method of Preparation
It is prepared by treating iron filling with iodine under water to get iodide which is then reacted with potassium carbonate.

Hydroiodic acid when treated with potassium bicarbonate results in the formation of potassium iodide.

Properties
It occurs as odourless, transparent or opaque crystals. It is white granular powder. It is slightly hygroscopic, taste is saline and slightly bitter.
It is very soluble in water and even more so in boiling water, freely soluble in glycerine and soluble in alcohol. On long exposure to air it becomes yellow due to liberation of iodine and small quantity of iodate may be formed.
Iodine readily dissolves in an aqueous solution of potassium iodide, forming a dark brown solution which contains potassium iodide.
Uses
It is used as an ingredient of expectorant mixture. It may be used for the prophylaxis and treatment of simple goitre. It is used as an antifungal agent in veterinary practise. Potassium
iodide solution is used as iodine supplement.
Ammonium Chloride
Chemical Formula: NH4Cl Molecular Weight: 53.49
Synonyms:
Ammonium Muriate, Sal Ammoniac, Salmiac, Amchlor, Ammon. Chlor.
Ammonium chloride occurs naturally in volcanic regions, forming on volcanic rocks near fume releasing vents.
Method of Preparation
It is a product of the Solvay Process used to produce Ammonium Chloride and Sodium Carbonate.

This method is used to minimize ammonia release in some industrial operations. Ammonium chloride is prepared by combining ammonia with either hydrogen chloride (gas)
or hydrochloric acid.
Properties
It is a white crystalline salt, highly soluble in water. Solutions of ammonium chloride are mildly acidic. It is somewhat hygroscopic. It is odourless and possesses cooling saline taste.
On heating, it sublimes without melting.
Ammonium chloride reacts with a strong base e.g. sodium hydroxide to release ammonia gas.

Ammonium chloride also reacts with alkali metal carbonates at elevated temperatures, giving ammonia and alkali metal chloride.

Storage
It should be stored in tightly closed containers because it is hygroscopic.
Assay
A modified Volhard’s method was used in I.P. 66. A solution of the substance acidified with nitric acid, is shaken with a measured yohjme of N/10 AgNP3, nitrobenzene being previously added.
Nitrobenzene is added to coagulate the precipitiate of AgCl, so that it will not interfere with the titrated later of excess of AgNO4 which is determined by titratio with N/10 ammonium thiocyanate, using ferrric ammonium sulphate as indicator.
The following is the reaction taking place at the end point when red ferric thiocyanate is formed.

Uses
Ammonium chloride is a nitrogen source in fertilizers e.g. chloro ammonium phosphate. It is used as an expectorant in cough medicine. Its expectorant action is caused by irritative action on the bronchial mucosa.
Ammonium chloride is used as a systemic acidifying agent in treatment of severe metabolic alkalosis. It is also used as an flavouring agent It is used in the textile and leather industry in dyeing, tanning, textile printing and to luster cotton. It is used in hair shampoos as a thickening agent.
Emetics
An emetic is a drug that produces vomiting. Vomiting is the involuntary, forceful expulsion of the content of one’s stomach and sometimes the nose. Emetics act either directly or by stimulation of the chemeoreceptor trigger zone in the floor of IV th ventricle in medulla or reflexly by irritant action on gastro-intestinal tract.
It is used medically where a substance has been ingested and must be expelled from the body immediately. Gastric secretions and likewise, vomiting are highly acidic. Salt water and mustard water have been used since ancient times as emetic Hydrogen peroxide is used as an emetic in veterinary practise Inorganic compounds e.g.
Copper sulphate, Sodium chloride, Zinc sulphate and Potassium antimony tartarte belong to the latter type. Emetics should be avoided in children and in the elderly pregnant women and in patients suffering from CNS depression, unconscious or in coma.
If the vomiting reflex continues for an extended period, dehydration, hypokalaemia and alkalosis may occur and replacement of fluid and electrolytes may be necessary. Emetics are also sometimes used in the preparation of cough syrups.
Copper Sulphate
Synonym: Blue vitriol
Chemical Formula: CuSO4.5H2O
Molecular Weight: 159.6
Preparation:
It is prepared by dissolving cupric oxide (or) cupric hydroxide (or) cupric carbonate in dilute H2SO4.
Properties
Its hydrated salt is blue in colour but anhydrous salt is colourless. It readily dissolves in water but is insoluble in alcohol.
Uses
It is used as a germicide and insecticide in agriculture. A mixture of copper sulphate and lime, commonly known as Bordeaux mixture, is used as fungicide. It is used in electroplating, calico printing and in electrical batteries.
Assay:
Weigh accurately 1 gm of copper sulphate (CuS04) in 50 ml of water, add 3 gm of potassium iodide, 5 ml of acetic acid and titrate the liberated iodine with 0.1 N Sodium thiosulfate (Na2S2O3) using solution of starch as indicator.
Sodium Potassium Tartrate
Synonyms: Rochelle salt
Chemical Formula: C4H4NaKO6
Molecular Weight: 210.158
Properties
It occurs as colourless crystals, saline in taste, soluble in hot water and insoluble in alcohol.
Uses:
It is used as laxative. It has also been used1in the process of silvering mirrors.
Expectorants And Emetics Very Short Answer Questions
Question.1 What do you understand by the term ‘Cough’?
Answer: Cough, a protective reflux (both voluntary and involuntary) helps to expel irritant matter from the respiratory tract.
Question.2 How many types of cough are there?
Answer: There are two types of cough :
1) Productive cough
2) Non-productive cough/Irritant cough
Question.3 Define Expectorants?
Answer: Expectorants are drugs used to help in the removal or explusion of secretions or exudate from the trachea, bronchii or lungs.
Question.4 Name any two inorganic compounds which are used as Expectorants?
Answer: 1) Ammonium salts such as Ammonium chloride
2) Iodide such as Potassium Iodide.
Question.5 How do expectorants act upon the respiratory tract?
Answer: Expectorants act upon the respiratory tract in two ways :
- By decreasing the viscosity of the bronchial secretion and facilitating their elimination; local irritants are expelled and ineffectual coughing is required.
- By increasing the amount of respiratory tract fluid, a demulcent action is exerted on dry mucosal lining and relieving the unproductive cough.
Question .6. What is the difference between emetic and vomiting?
Answer. An emetic is a drug that produces vomiting while vomiting is the involuntary; forceful expulsion of the contents of one stomach and sometimes the nose.
Question.7. Name two inorganic compounds which are used as emetics?
Answer. Copper sulphate, Zinc sulphate
Sodium chloride Potassium antimony tartrate
Question.8. What is the molecular formula of antimony potassium tartarte?
Answer. Molecular formula of antimony tartarte is C4H4O7SbK.1/2H2O.
Question.9. Which inorganic compound is used in the prevention and treatment of goitre?
Answer. Potassium iodide.
Question.10. What is the difference between productive cough and non-productive cough?
Answer. Productive cough produces a phlegm or mucus (sputum) while non-productive cough does produce sputum.
Question.11. How do emetics act?
Answer. Emetics act either directly or by stimulation of the chemeoreceptor trigger zone in the floor of IVth ventricle in medulla or refluxly by irritant action on gastro intestinal tract.
Question.12. What is the method of preparation of Ammonium Chloride?
Answer. Ammonium chloride is prepared by reacting ammonium with sodium chloride

Question.13. Which expectorant is prepared by Solvay process?
Answer. Ammonium chloride.
Question.14. What is the other name of Kali Iodidum?
Answer. Kali iodidum is also known as Potassium Iodide.
Question.15. What is the structural formula of Antimony Potassium Tartrate?
Answer. Structural formula of Antimony potassium tartrate is
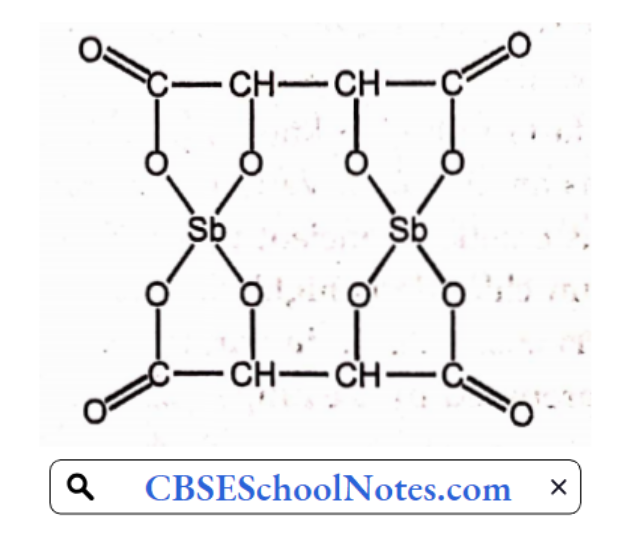
Question.16. What is the othei name of Antimony Potassium Tartrate?
Answer.
- Tartarised antimony
- Potassium antimonyl tartrate
Question.17. What are the Pharmaceutical uses of Potassium Iodide?
Answer: Potassium iodide is used as an ingredient of expectorant mixture. It is also used as an Iodine supplement.
Expectorants And Emetics Fill In The Blanks
1. Cough is a……………. reflux.
Answer: Protective
2. Emetics are used to produce…………………………..
Answer: Vomiting
3. Ammonium chloride is prepared by…………………
Answer: Solvay process
4. The latin word ‘expectorate’ means …………………….
Answer: To drive from the chest
5. Productive cough produces a…………………..
Answer: Mucus
6. Expectorants are used to help in the…………………
Answer: Removal of secretions
7. ………………….inorganic compound are used as saline expectorants.
Answer: Potassium iodide/ammonium chloride
8. Ammonium chloride is also known as ‘………………………
Answer: Ammonium Muriate/Amchlor
9. Antimony potassium tartarte is also known as…………………….
Answer: Emetic tartarte/Tartarised antimony
10………………….is used as an emetic in verterinary practise.
Answer: Hydrogen Peroxide
11………………….is used as emetic in ancient times.
Answer: Salt water/Mustard water
12. Solutions of ammonium chloride is highly…………..
Answer: Acidic
13. Ammonium chloride is………………in nature.
Answer: Hygroscopic
14. Potassium iodide is prepared by treating……… with………….under water.
Answer: Iron fillings with iodine
15. Ammonium chloride is used as………………in fertilizers.
Answer: Nitrogen source
Expectorants And Emetics Multiple Choice Questions
1. Productive cough produces.
- Mucus
- Vomiting
- Amalgam
- None of these
Answer: Mucus
2. Which cough does not produce mucus?
- Productive cough
- Both a) and c)
- Non-productive cough
- None of these
Answer: Non-productive cough
3. Which inorganic compound is used as Emetic?
- Ammonium chloride
- Potassium antimony tartarte
- Potassium iodide
- Potassium citrate
Answer: Potassium iodide
4. ‘KI’ stands for
- Potassium iodide
- Potassium iodate
- Potassium citrate
- None of these
Answer: Potassium iodide
5. Emetics act
- By stimulation of the chemeoreceptor trigger zone
- By increasing the amount of fluid
- By decreasing the viscosity of the bronchial secretion
- None of these
Answer: By stimulation of the chemeoreceptor trigger zone
6. If the vomiting reflex continues for an extended period,……….occurs.
- Dehydration
- Alkalosis
- Hypokalemia
- All of the above
Answer: All of the above
Antidotes in Poisoning
Antidotes Introduction
Poison may be defined as any substance that when introduced into or absorbed by a living organism causes illness or death.
Poisoning occurs in many ways
- by accidentally
- by use of recreational substances (such as cannabis, opiates etc.)
- by intentional behaviour
- by occupational exposure
So, as to counteract the effects of a poison, antidotes are used.
Antidotes
An antidote is an agent with specific action against the activity or effect of a poison.
OR
An antidote is an agent which counteracts as a poison.
Whether accidental or intentional, the poisoning requires only sympathomimetic and supportive therapy i.e. removal of poison from the body is first priority in case of poisoning.
It can be done by either gastric lavage or emesis induction (Gastric lavage is the process of cleaning the stomach) while (emesis induction can be done by the administration of substances like activated charcoal to reduce the absorption).
Classification Of Antidotes
The antidotes are classified into three types depending upon their mechanism of action.
Physiological antidotes: They act by producing the effects opposite to that of poison.
For example: Sodium nitrite which converts haemoglobin into methaemoglobin in order to bind cyanide, atropine & physostigmine.
Mechanical antidotes: These render the poison inert by mechanical action or prevent their absorption.
For example: Activated charcoal absorbs the poison to absorption across the intestinal wall, mercuric chloride, sulphanilamide.
Read and Learn More Pharmaceutical Inorganic Chemistry Notes
Chemical antidotes: They change the chemical nature of the poison.
For example:
- Sodium thiosulphate which changes toxic cyanide to non-toxic thiocyanate.
- Sodium sulphate is used to precipitate lead.
- Copper sulphate is used to precipitate phosphorous.
Universal antidote is a combination of physical and cheical antidote. It is an antidote which can be used in cases, where the nature of the poison swallowed is not definitely know. The universal antidote has following composition :
- Powdered animal charcoal
- Tannic acid ‘ • ‘
- Magnesium oxide
Antidotes Reasons Of Poisoning
Poisoning of the body is due to various reasons. It can be due to the presence of heavy metals such as lead, arsenic, mercury, and cadmium; insecticides or pesticides used in our
daily life and cyanide poisoning which occurs due to a variety of occupational sources.
Antidotes Lead Poisoning
Lead poisoning has been recognized as a major public health risk, particularly in developing countries. Though various occupational and public health measures have been under taken in order to control lead exposure.
Lead is regarded as a potent occupational toxin and its toxicological manifestations are well known. In case of severe lead poisoning, Sodium calcium edetate & dimercapol are
commonly used. Chelation therapy has so far been used.
Sodium Calcium Edetate leads from bone and the extra cellular space and then expels it out from the urine. Dimercapol is more effective than the sodium calcium edetate as chelating. It lead from the soft tissues such as brain.
Now a days, Succimer a water soluble analogue of dimercapol has been increasingly preferred. It is suitably administrated by mouth and is well tolerated.
It occurs by a number of ways such as inhalation or ingestion of soluble cyanide salts or cyanide releasing substances like seeds of peach, apricot, cyanamide, cyanogen chloride and
bitter almonds.
It has a characteristic odour of bitter almonds. The symptoms of cyanide poisoning are: Nausea, hypotension, dizziness, drowsiness, coma, convulsions and death.
Cyanide Poisoning
Cyanide poisoning takes place intentionally or accidentally to commit suicide. Two inorganic antidotes are used such as sodium nitrite and sodium thiosulphate to counteract its poisoning.
Nitrate generates ferrous ion of haemoglobin to the ferric ion of methahaemoglobin which has high affinity for cyanide radicals and form cyanomethaemoglobin. However, this
may again dissociate to release cyanide. Therefore, sodium thiosulphate is given to form sodium thiocyanate which is poorly dissociable and is excreted in the urine.

Sodium nitrite is used for this purpose because it has a very weak vasodilator action.
Sodium Nitrite
Chemical formula: NaNO2 Molecular Weight: 69.00
Synonym: Nitrous acid Sodium salt
Preparation
It can be prepared by strongly heating sodium nitrate.

It is more conventinely made by heating the sodium nitrate with metallic lead or carbon which reduces it at lower temperature.

Physical Properties
- It is odourless, colourless to slightly yellow crystals.
- Its taste is saline.
- It is water soluble and sparingly soluble in alcohol.
- It is hygroscopic.
- It is slowly oxidizes to nitrate in air.
Chemical Properties
1. Sodium Nitrite is easily decomposed by the acidification with dilute sulphuric acid.

2. It also act as a reducing and oxiding agent.

3. With aniline hydrochloride at 4°C, Nitrous acid forms diazonium chloride.

Uses
- It is used in treatment of cyanide poisoning in conjugation with sodium thiosulphate.
- Sodium nitrate is also used as a rust inhibitor preservative in foods such as cured meals for manufacturing dyes.
- It is used as a vasodilator.
Sodium Thiosulphate
Chemical formula: Na2S2O3.5H20 Molecular Weight: 248.2
Synonym: Sodium hyposulphate
Preparation
It can be prepared by boiling sodium sulphite with sulphur.
It can be obtained by mixing sulphide liquors sodium carbonate by passing S02 gas.
![]()
It is prepared by passing the sulphur dioxide gas into solution of sodium carbonate.

The sodium bisulphite so obtained further reacts with sodium carbonate to give the sulphite.

Physical Properties
- It occurs in the form of large, colourless crystals.
- It is odourless and is having an alkaline taste.
- It is soluble in water but insoluble in alcohol.
- It effloresces in warmy dry air above 33°C.
- When exposed to the moist air, it deliquesces lightly.
Chemical Properties
Sodium thiosulphate when acidified with hydrochloric acid, it decomposes to give sulphur dioxide, water and sulphur.
Thiosulphate act as reducing agent as shown by reaction with the ferric chloride solution.

It is also called as antichlor in bleaching due to its reaction with chlorine or hypochlorite

Assay
It is assayed by the iodemetric titration. Dissolve an accurately weighed amount of substance in water & titrate with 0.05M iodine solution using starch mucilage as indicator.

End point is indicated by the presence of blue colour.
Uses
- It is used in the treatment of Cyanide Poisoning. It is also used to treat parasitic skin diseases.
- It is used as antichlor in bleaching process in textile industry.
- It is widely used as stimulant analytical chemical.
Antidotes Short Answer Questions
Question. 1. Differentiate between Poison and Antidote?
Answer. Poison may be defined as any substance that when introduced into or absorbed by living organism causes illness or death while an antidote is an agent which counter
act as a poison.
Question.2. Which kind of therapy is required for Poisoning?
Answer. Poisoning requires sympathomimetic and supportive therapy.
Question.3. How poisoning can be removed immediately from the body?
Answer. Poisoning can be removed immediately from the body by gastric lavage or emesis induction.
Question.4. How poisoning can be occurred?
Answer. Poisoning can occur in many ways:-
- by accidentally
- by use of recreational substances
- by intentional behaviour
- by occupational exposure
Question.5. Classify antidotes.
Answer. Antidotes can be classified into three types
- Physiological antidotes
- Mechanical antidotes
- Chemical antidotes
Question.6. Write down the examples of Mechanical Antidote?
Answer.
- Activated charcoal
- Magnesium sulphate
- Copper sulphate
- Sodium monohydrogen phosphate
Question.7. Which drugs are used in the treatment of lead poisoning?
Answer. Sodium calcium edetate and Dimercapol
Question.8. Which therapy is used for lead poisoning?
Answer. Chelation therapy
Question.9. Which antidote is used in the treatment of cyanide poisoning?
Answer. Sodium nitrite, Sodium thiosulphate
Question.10. Differentiate between Physiological antidotes and Mechanical antidotes.
Answer.
- Physiological antidotes- They act by producing the effects opposite to that of poison.
- Mechanical antidotes : They prevent the absorption of poison into body
Antidotes Fill In The Blanks
1. ………….is used to counteract the poison.
Answer: Antidote
2. Cyanide poisoning kit contains . …,………. and ………….
Answer: Amyl nitrite, Sodium nitrite & Sodium thiosulphate
3. Cyanide poisoning has a characteristic odour of ……………….
Answer: Bitter almonds
4………………….therapy is used for lead poisoning.
Answer: Chelation
5. Chemical antidote act by changing the……………..of the poison.
Answer: Chemical nature
6. Activated charcoal is used to…………… the poison.
Answer: Absorb
7…………………is the example of physiological antidote.
Answer: Sodium nitrite
8…………….is the molecular formula of sodium thiosulphate.
Answer: Na2S2O3.5H2O
Antidotes Multiple Choice Questions
1. An important antidote in the treatment of cyanide poison is:
- Ethanol
- Atropine
- Sodium thiosulphate
- Desferrioxamine
Answer: Desferrioxamine
2. In case of poisoning, activated charcoal acts to reduce absorption of the substance by
- Increasing osmotic pressure of the intestinal contents
- Shortening transit time thorugh the gut
- Binding to the poison molecules
- Stimulating the chemoreceptor trigger zone in the medulla
Answer: Binding to the poison molecules
3. When a poison is inhaled what methods you will be thinking of to manage the case?
- Induction of emesis
- Carrying out a gastric lavage
- Thinking of an active elimination technique
- Administration of an antidote
- Both c) and d)
Answer: Both c) and d)
4. An antidote is used
- To counteract the poison
- To enhance the poison
- To cause illness e.g. death
- To prdouce consiousness
Answer: To counteract the poison
5. Which of the following antidotes is not used in cyanide poisoning?
- Hydroxy cobalamine
- Sodium nitrite
- Dimercapol
- Sodium calcium EDTA
Answer: Hydroxycobalamine And Sodium nitrite
6. Which kind of antidote reduces the poison across the intestinal wall?
- Mechanical antidote
- Physiological antidote
- Chemical antidote
- None of the above
Answer: Mechanical antidote
7. Physiological antidotes act by:-
- Absorption of the poison
- Changing the chemical nature of the poison
- Producing the effects opposite to that of poison
- By countering the effects of poison
Answer: Producing the effects opposite to that of poison
8.”Cyanide poisoning kit” contains following:-
- Sodium nitrite
- Amyl nitrite
- Sodium bicarbonate
- Sodium thiosulphate
Answer: Sodium bicarbonate
9. How does mechanical antidote act?
- By producing the effects opposite to that of poison
- By preventing the absorption of poison into the body
- By changing the chemical nature of the poison
- By changing the physical nature of the poison
Answer: By preventing the absorption of poison into the body
10. Which one of the following is an example of Physiological Antidote?
- Sodium nitrite
- Sodium thiocyanate
- Activated charcoal
- Copper sulphate
Answer: Sodium nitrite
11. Cyanide Poisoning has a characteristic odour of
- Bitter almonds
- Wheat
- Lemon
- Caraway
Answer: Bitter almonds
12. Sodium nitrite is given in conjuction with:-
- Sodium bicarbonate
- Sodium thiosulphate
- Sodium calcium edetate
- Dimercaprol
Answer: Sodium thiosulphate
Astringent: What is it, Uses, Benefits
Astringents Introduction
Topical astringents are used to firm Up (tone) the skin.
Astringents
A substance that controls or tightens tissue, thereby alleviating conditions such as diarrhoea, haemonhages and secretions is known as astringent.
Astringent is applied to skin, mucous membrane and does not destruct the tissue. It will cause constriction of capillaries and small blood vessels. Astringent acts as protein precipitant and arrest discharge by causing shrinkage of tissue.
Zinc Oxide and Calamine are astringents used in lotions, powders and ointments to relieve from itching and choping in various forms of dermatitis. Astringent helps to reduce oiliness e.g. excessive precipitation.
Astringents have bacteriostatic properties, though they are not generally used as antiseptics. The protein-precipitation brought about by astringent is ascribed to presence of metallic ions having large charge/ radium ratio of strong electrostatic fields.
The metal would form complex with various polar groups present on the protein or enzyme. This complexation of important functional group at active site of protein or an enzyme cause a drastic change in properties of the protein.
Astringent are used to treat diarrhoea, and also possess deodorant properties. Astringent promote healing process.
Read and Learn More Pharmaceutical Inorganic Chemistry Notes
Alum
Alum is both a specific and a class of chemical compound. The specific compound is the Hydrated Potassium Aluminium Sulfate (potassium alum) with the formula KA1(S04)2.12H2O.
More widely, alums are double sulphate salts, with the formula AM(SO4)2.12H2O, where A is a monovalent cation such as Potassium or Ammonium and M is a trivalent metal ion such
as Aluminium or Chromium (IE).
Alums are prepared by adding a hot, concentrated solution of either Potassium or Ammonium Sulphate to a hot solution of an equimolar proportion of Aluminium Sulphate and the alums get separate out.

Properties
Alum occurs as colourless, transparent, colourless crystals, white granules or powder. It has sweetish strongly astringent taste. Its crystals are sometimes opaque on the surface
due to formation of traces of basic salt.
It is freely soluble in water but slowly dissolves in glycerine and insoluble in alcohol. The aqueous solution is acidic to litmus.
On heating potash alum melts, it loses the water of crystallization below 200°C, forming a white residue of anhydrous aluminium sulphate and potassium sulphates. It is soluble in the water but insoluble in alcohol.
Assay
Complexometirc titration of aluminium is carried out 0.9gm is dissolved in the 20 ml of water. Each ml of 0.1N disodium edetate is equivalent to 47.44 mg of A1K.(SO4).12H2O
Official Test for Identity
- A solution of water gives the reactions characteristic of aluminium & sulphate.
- A small quantity of a solution in water is treated with sodium bicarbonate & filtered. The filterate gives the reactions of potassium.
Uses
Alum is used as an ingredient of some brands of toothpaste or powders. It is used in many subunits vaccines as a adjuvant to enhance the body’s response to immunogen. Vaccines
include hepatitis A, hepatitis B and DTAP.
It is used by pet owners to stem bleeding associated with animal injuries caused by improper nail clipping. It is used as a haemostatic agent, as mouth washes or gargles, as bladder irrigitations.
It is a powerful astringent. It is used in making lotions and douches. It has also been used as vaginal cleaning and deodrant preparations.
Zinc Sulphate
Chemical Formula: ZnSO4.7H2O Molecular Weight: 287.54
Synonym : white Vitriol
Preparation
It is prepared by boiling metallic Zinc with dilute Sulphuric Acid. A slight excess of zinc metal is used and the reaction is allowed to continue untill hydrogen gas evolves out.

The solution is filtered to separate unreacted Zinc, concentrated and crystallized.
It may also be prepared by the action of dilute Sulphuric acid on Zinc Oxide.

Chemical Properties
1) A white precipitate Zn(OH)2 is formed when zinc sulphate reacts with NaOH. The precipitate is solubilised in excess of NaOH.

Properties
It occurs as colourless, transparent crystals or crystalline powder. It is odourless. Its taste is astringent and metallic. It is very soluble in water and freely soluble in glycerin. It efflorescenes in dry air.
Assay
An aqueous solution of ZnSO2 has been acidic to litmus, due to hydrolysis of the salt and is having pH of about 5. The solution has been acid to solution of phenol red and not acid to solution of methyl orange.
Storage
Since it is efflorescent, it should be stored in tightly closed non-metallic containers.
Incompatibility
It is incompatible with alkali carbonates and hydroxides and with astringent infusions and decocations.
Uses
It is widely used as an astringent and in emetic (induces vomiting). A 0.25% aqueous solution is also used as an opthalmic astringents. It is used as reflex emetic especially in Narcotic
Poisoning (opium alkaloids poisoning). It has also been used internally as an emetic.
Astringents Short Answer Questions
Question. 1. Define Astringent.
Answer. Astringent is a substance that causes the contraction or shrinkage of tissue that dry up secretions.
Question.2. How do astringent act?
Answer. Astringent acts as protein precipitant.
Question.3. Name any two inorganic compounds that arc used as astringent?
Answer. Zinc Chloride, Alum, Zinc Sulphate.
Question.4. What Is the another name of Zinc Sulphate?
Answer. White Vitriol.
Question.5. What is the method of preparation of Zinc Sulphate?
Answer. Zinc Sulphate is prepared by the action of dilute sulphuric acid on zinc oxide.

Question.6. What are the pharmaceutical uses of Zinc Sulphate?
Answer. Zinc Sulphate is used as an astringent and in emesis. A 0.25% aqueous solution is also used as an opthalmic astringents.
Question.7. Write down the incompatibilities of zinc sulphate?
Answer. Zinc Sulphate is incompatible with alkali carbonates and hydroxides.
Question.8. What are the properties of Zinc Sulphate?
Answer.
- It occurs as colourless, transparent crystals or crystalline powder.
- It is very soluble in water and freely soluble in glycerine.
Question.9. Write down any two pharmaceutical uses of Alum?
Answer.
- Alum is used as an ingredient of some tooth paste or powders.
- It is a powerful astringent.
- It is widely used in vaginal cleansing and deodrant preparation.
Question.10. What is the taste of Alum?
Answer. It has sweetish strongly astringent taste.
Astringents Fill In The Blanks
1. An astringent is a drug which shrinks by……………………from their surfaces.
Answer: Protein precipitation
2. Commercially………..is prepared by heating metallic zinc to bright redness in the presence of preheated air.
Answer: ZnSO4
3. ………………..is used in narcotic poisoning which is also an inorganic astringent.
Answer: ZnSO4 (Zinc sulphate)
4. Astringent act as………………..
Answer: Protein precipitate
5. Astringent cause…………………of tissue.
Answer: Shrinkage or contraction
6. Alum is prepared by adding a hot cone, solution of………………. to a hot solution of…………… and it get separate out.
Answer: Ammonium sulphate, aluminium sulphate
7. ………………………..is used as astringent.
Answer: Zinc sulphate, Alum
8. Topical astringents are used to………………………..
Answer: Firm up the skin
9. Chemical formula of Alum is………………………while of Zinc Sulphate is………………
Answer: AM(SO4)2.12H2O, ZnSO4
10. ZnS04 is externally used as…………………..
Answer: Astringent
Astringents Multiple Choice Questions
1. What is the effect of astringents on tissues?
- Contraction
- Both a) and b)
- Shrinkage
- None of these
Answer: Both a) and b)
2. How do astringents act?
- Lipid precipitant
- Bacterial inhibition
- Protein precipitant
- Enzymatic catalysis
Answer: Bacterial inhibition And Protein precipitant
3. What is the chemical formula of Alum?
- KA1(SO4)2.12H2O
- K2SO4.12H2O
- KSO4.2H2O
- K(SO4)2.12H2O
Answer: KA1(SO4)2.12H2O
4. Zinc sulphate is also known as
- White vitriol
- Red vitriol
- Blue vitriol
- Yellow vitriol
Answer: White vitriol
5. Which inorganic astringent is used in the treatment of nacrotic poisoning?
- Alum
- Zinc Sulphate
- Aluminium chloride
- Zirconium Sulphate
Answer: Zinc Sulphate
6. Zinc sulphate is prepared by the action of………. on Zinc Oxide.
- Conc. HCl
- Conc. HNO3
- Conc. H2SO4
- None of these
Answer: Conc. H2SO4
Haematinics
Haematinics are substances required in the formation of blood in process of hematopoiesis and are used for treatment of anaemias. The main hematinics are B12 & folate.
These drugs increase the number of red blood cells and the amount of hemoglobin to normal level and above when they are below normal.
Anaemia occurs when the balance between production and reduction of red blood cells is disturbed
- Due to blood loss
- Impaired red cell formation due to
- Deficiency of essential factors: Iron, folic acid vitamin B12.
- Bone marrow depression, erythropoietin deficiency
- Increased destruction of RBCs (Haemolyticanaemia)
Ferrous Sulphate
Synonyms: Green vitriol
Molecular formula: FeSO4.7H2O
Molecular weight: 278
It contains not less than 98% and not more than 105% of FeSO4.7H2O
Preparation
When iron is treated with dilute H2SO4, iron dissolve and form ferrous sulphate and hydrogen gas is liberated.
Read and Learn More Pharmaceutical Inorganic Chemistry Notes

Ferrous sulphate Is obtained commercially by exposing the moist Iron pyrites to air when slow oxidation takes place.

Properties
Physical properties:
It occurs as transparent, pale bluish green crystalline powder; odourless; metallic in soluble in boiling water, freely soluble in water but practically insoluble in alcohol.
Chemical properties:
When it is treated with ceric ammonium sulphate [(NH4)4Ce(SO4)42 H20] in acidic medium, it reduces ceric ion.

Assay:
Ferrous sulphate solution may bring about discolouration of the teeth in contract. The assay is based on oxidation-reduction (redox) titration. An acidified solution of substance is titrated with ceric.
Ammonium sulphate in presence of sulphuric acid using ferrous sulphate solution as an indicator. Weigh accurately 1 gm of ferrous sulphate (FeSO4) and dissolve in 20 ml of diluted sulphuric acid in 30ml. of water. Titrate the contents of the flask with 0.1 N potassium permanganate (KMnO4) until a permanent pink colour is obtained.
Uses:
It is used as hematinic in the treatment of iron deficiency anaemia. It is also used to dye fabrics and in tanning leather.
- White nitric oxide, ferrous sulphate forms black colourednitroso ferrous sulphate FeSO2.NO.
- On heating it decomposes into ferric oxide sulphur dioxide &nelpherotrixodide.

Ferrous Gluconate
Molecular formula:-C12H22FeO14.2H2O
Molecular weight: 482.2
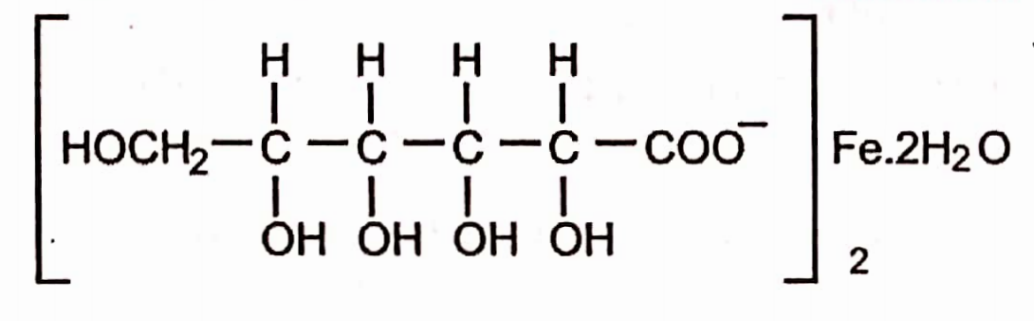
Preparation
1 . It is obtained by dissolving ferrous carbonate in calculated amount of gluconic acid. First of all gluconic acid is prepared by the oxidation of glucose.

Gluconic acid is treated with BaCl2 solution which is then treated with FeS04 solution. BaS04 precipitates out & is removed by filtration.
Properties
- It occurs as a fine, yellowish gray & pale greenish yellow powder or granules with slight burnt sugar.
- It is freely but slowly soluble in water.
Assay
The assay is based on the oxidation-reduction titration. To a weighed amount (l,5gm) dissolved in water and 2N sulphuric acid, zinc powder is added & kept for 20 minutes, filtered and the filter is washed with the water.
To the combined liberate and washing ferrous sulphate solution is added & titrated with 0.1N ceric ammonium sulphate until the colour is change from orange to green. A blank determination is performed.
Use
1 . It is used for the preparation of ferrous Gluconate tablets.
Haematinics Very Short Answer Questions
Question. 1. What are haematinics?
Answer. Haematinics are substances required in the formation of blood. These drugs are used for the treatment of anaemia. These drugs increase the number of red blood cells and
the amount of haemoglobin is raised to normal level and above when they are below normal.
Haematinics Fill In The Blanks
1. Total body iron in an adult person is…………..
Answer:2.5 gm to 5 gms
2. Vitamin K] is also known as………….. is used in prevention of haemorrhagic disease of new borne.
Answer: Phytonadione