
- Acute And Chronic Inflammation Notes
- Bone Diseases: Types, Symptoms, And Treatments
- Cell injury and Cellular Adaptation Notes
- Diseases of the Kidney and the Urinary System
- Disorder Of Cardiovascular System Notes
- Disorders Of Respiratory System
- Endocrine Disorders: Causes, Signs, Types
- Gastrointestinal Diseases & Disorders
- Haematological Disorders Types, Symptoms
- Infectious Disease: Types, Causes & Treatments
- Nervous System Diseases: Types, Causes, Signs
Pathophysiology
Disorders Of Respiratory System
Disorders Of the Respiratory System
Obstructive Lung Disease
Obstructive lung diseases are the second (after cardiovascular diseases) leading cause of death in the adult population in India. Obstructive lung disease refers to a group of diseases that share a common feature—difficulty in expelling air from the lungs.
- Asthma
- Chronic bronchitis
- Emphysema
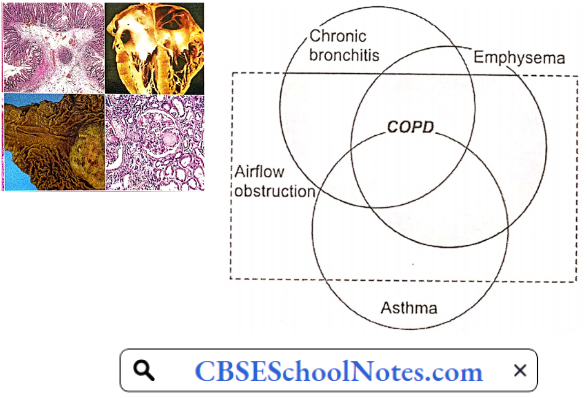
All three disorders have an increased airway resistance, but, are caused by a different mechanism in each case. However, often there is an overlap. In old cases of bronchial asthma, some element of emphysema develops. In chronic bronchitis, some elements of bronchospasm are commonly present.
Chronic bronchitis and emphysema are considered a spectrum of chronic obstructive pulmonary disease (COPD) with some patients showing dominantly bronchitis, while others show dominantly emphysema.
Read and Learn More Pathophysiology
In bronchial asthma, chronic bronchitis, and emphysema, the common factor is increased airway resistance. Pathogenesis and pathophysiology of obstructive lung disease can be explained only if the reader is familiar with the role of mucociliary clearance in respiratory mucosa and the physiology of airway resistance.
Mucociliary Clearance: From the trachea down to the terminal bronchioles, the respiratory mucosa is characterized by the presence of cilia, goblet cells, and submucosal mucous glands. The cilia are covered with a blanket of mucus, which traps any incoming particle greater than 5 p in size.
The ciliary movement of adjacent cells is so coordinated that it produces waves of ciliary motions from the distal to the proximal parts of the tracheobronchial tree. As a result, mucus blanket on the top of cilia laden with dust particles or bacteria is propelled upwards till it readies the oropharynx, where it is swallowed or expectorated.
Mucodliary clearance is a critical factor in the protection of the upper respiratory tract.
Airway Resistance
Resistance in the airways (RaW) is basically determined by the same factors that determine vascular resistance:
R = \(\frac{8 n L}{\pi r 4}\)
n = gas viscosity; L = airway length; r = radius
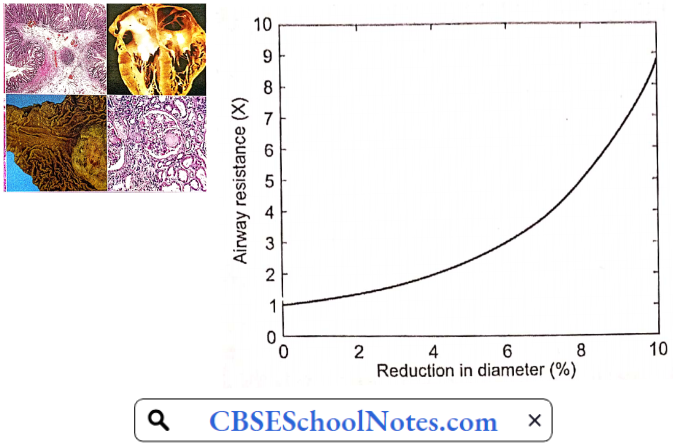
In the airways, the variable factor is the radius of the airways. A given reduction in the radius of bronchi results in a fourfold increase in airway resistance. Even a 4% reduction in airway diameter doubles the airway resistance.
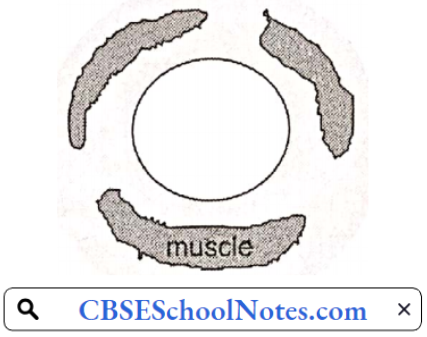
Lower Airway Resistance: The physiological control of airway resistance lies in the medium-sized bronchi (2-4 mm diameter). These airways contain, besides supporting cartilage, large amount of smooth muscle. Smooth muscle contraction can substantially increase airway resistance by reducing airway radius. The lumen of these bronchi can be altered by the following factors
- Bronchomotor muscle tone
- Radial traction by lung parenchyma
- Transmural pressure
- Luminal mucus
Bronchial Muscle Tone: Bronchial muscle tone is the chief factor that determines bronchial lumen size. It is chiefly regulated by parasympathetic neural discharge. In allergic asthma, a large number of local chemical mediators, such as histamine, prostaglandins, leukotrienes, kinins, etc. are released. All these mediators produce varying degrees of bronchial muscle spasm.
In chronic bronchitis also, there is some degree of bronchospasm. Circulating epinephrine can produce bronchodilation by acting on β2 receptors present on the bronchial smooth muscle. β2 agonists are used in the treatment of bronchial asthma.
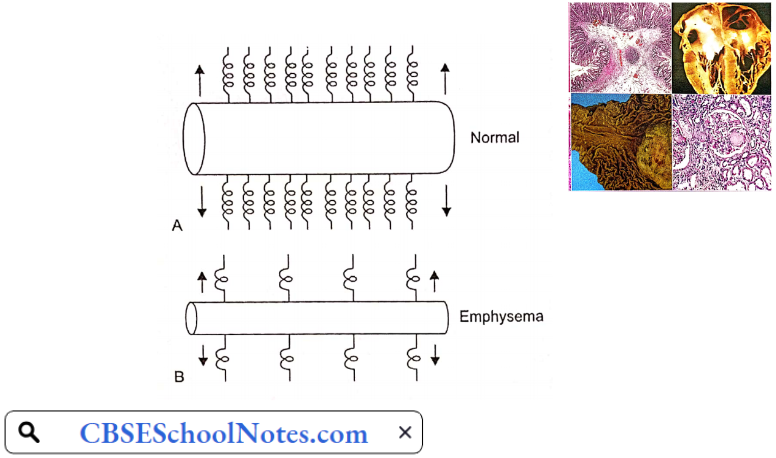
Radial Traction By Lung Parenchyma: Bronchi and bronchioles are surrounded by lung parenchyma, whose constant pull helps the patency of the airways. This supportive action is called radial traction. Parenchymal destructive diseases, such as emphysema, cause loss of radial traction. As a result, small airways collapse. That is the chief mechanism of bronchial narrowing in emphysema.
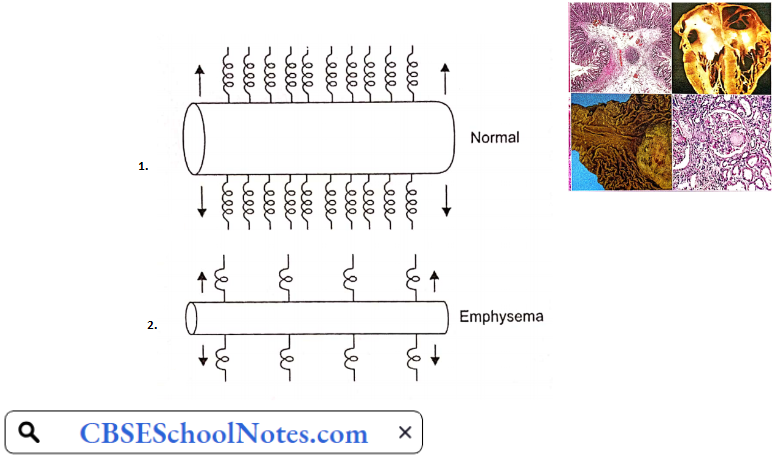
Transmural Pressure: During inspiration, intrapleural pressure is negative with respect to intrapulmonary pressure which helps to keep airways open. A similar situation exists during tidal expiration also. However, during forced expiration, intrapleural pressure becomes strongly positive, which tends to cause dynamic airway collapse.
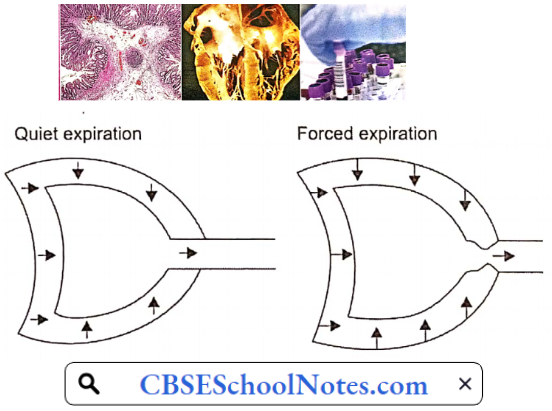
In emphysema, as explained later, expiration is brought about by the active contraction of expiratory muscles. The dynamic airway collapse causes expiratory flow limitations, i.e. beyond a point, increased expiratory effort does not produce further increase in air outflow. The problem is worsened in emphysema due to loss of radial traction, as well.
Mucus In Airways: The presence of mucus or other extraneous material in the airway lumen increases airway resistance. Cigarette smoking or respiratory infections enhance the secretion of submucosal mucous glands as well as mucosal goblet cells in the respiratory tract.
Bronchial Asthma
It is a disease characterized by recurrent attacks of breathlessness and wheezing, which vary in severity and frequency from person to person. Between the attacks, the patient’s breathing is normal. Worldwide, around 250,000 people die every year as a result of asthma.
Bronchial Asthma Symptoms
- Wheezing (a whistling sound arising from the lung during breathing)
- Tightness in the chest
- Shortness of breath
- Trouble sleeping caused by shortness of breath, coughing or wheezing
- Coughing or wheezing attacks that are worsened by a respiratory virus, such as a cold or the flu
Asthma Triggers: Exposure to various irritants and substances that trigger allergies (allergens) can trigger signs and symptoms of asthma. Asthma triggers are different from person to person and can include
- Airborne substances, such as pollen, dust mites, mold spores, pet dander, or particles of cockroach waste
- Respiratory infections, such as the common cold
- Physical activity (exercise-induced asthma)
- Cold air
- Air pollutants and irritants, such as smoke
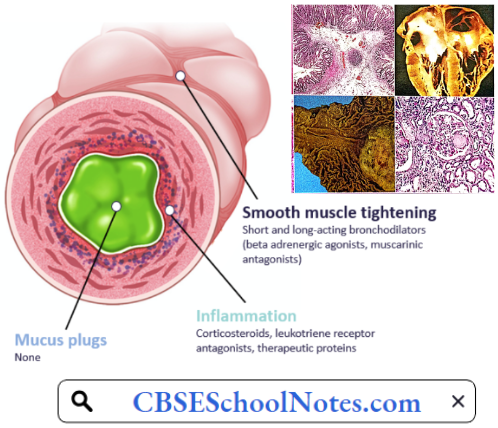
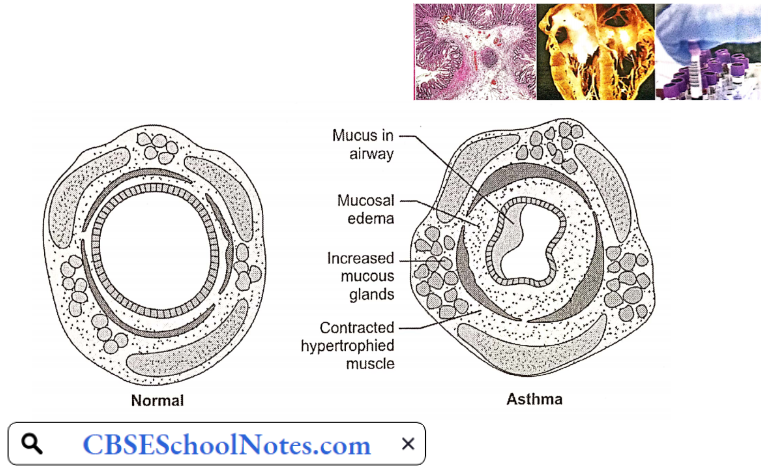
Pathogenesis: The pathology of bronchial asthma consists of reversible bronchial narrowing associated with a spasm of smooth muscle in the wall of the airways (bronchi). The airway hyper-responsiveness is a fundamental disorder. The airway smooth muscle shows an exaggerated response to a variety of triggers such as seasonal outdoor allergens (pollens) or allergens derived from house dust, mites present in carpets, beds, or domestic animals or cockroaches.
- There is a genetic predisposition to bronchial asthma. A substantial percentage of asthmatic patients have elevated IgE levels (a sign of allergic predisposition) and a history of additional allergic disorders.
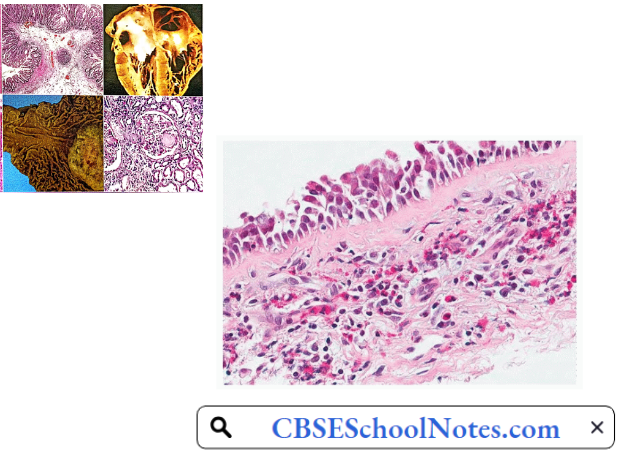
- Histological examination of small bronchi reveals epithelial damage, hypertrophy, and hyperplasia of bronchial smooth muscle, enlargement of mucous glands, increased number of goblet cells, and infiltration of the bronchial wall with eosinophils and lymphocytes.
- The inflamed tissues respond to any of the triggers by release of mediators such as histamine and bradykinin by the mast cells and eosinophils in the bronchial mucosa. These mediators produce bronchospasm and increased mucus secretion.
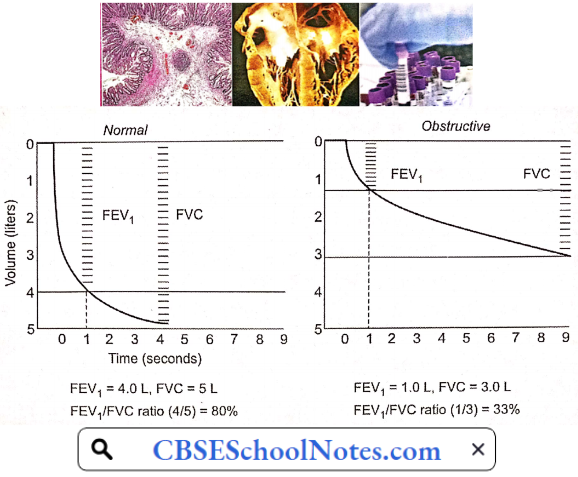
The combined effect of bronchoconstriction and increased mucus secretion produces a critical narrowing of airways and increased airway resistance, especially during the expiratory phase. During an asthmatic attack, though breathing difficulty is felt during inspiratory phases, it becomes worse during expiratory phases of respiratory cycles.
Confirmatory Pulmonary Function Tests
- Forced vital capacity (FVC) is decreased
- Forced expiratory volume 1st second/vital capacity ratio (FEV1/FVC ratio) is decreased.
- Peak expiratory flow rate (PEFR) decreased.
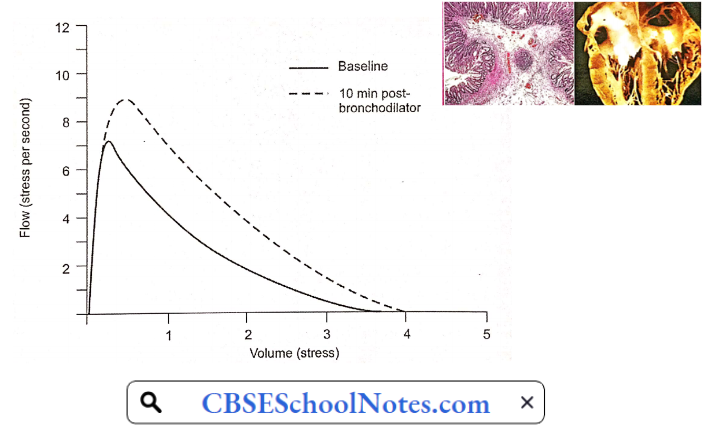
- Increase in FEV1/VC ratio and PEFR when tested after inhalation of a bronchodilator drug.
Bronchial Asthma Risk Factors
- Family history.
- Viral respiratory infections during infancy and childhood.
- Other Allergies: Having an allergic condition, such as eczema or allergic rhinitis is a risk factor for developing asthma.
- Smoking.
- Air pollution.
- Obesity.
Bronchial Asthma Complications
- Frequent attacks of bronchial asthma interfere with day-to-day life.
- Acute severe asthma may progress to a life-threatening condition known as status asthmaticus.
- COPD (emphysema) in later life.
Pathophysiological Basis Of Treatment: An attack of bronchial asthma terminated by administration of a bronchodilator drug.
Chronic Obstructive Pulmonary Disease (COPD)
COPD is defined as a chronic, slowly progressive disorder characterized by airflow obstruction which continues over several months. Bronchial asthma, though involves airflow obstruction, is excluded by this definition. COPD starts as chronic bronchitis, which over the years develops into emphysema.
Chronic Obstructive Pulmonary Disease Symptoms And Signs: Signs and symptoms of COPD may include
- Cough and copious sputum
- Shortness of breath, especially during physical activities
- Wheezing
- Chest tightness
- Blueness of the lips or fingernail beds (cyanosis) (later stages)
- Frequent respiratory infections
- Swelling in ankles, and feet (later stages)
Aetiology
- Cigarette Smoking: Cigarette smoking is considered to be the most important cause of COPD. Cigarette smoke contributes to the development of COPD through a number of mechanisms
- Inhibits ciliary clearance function in bronchial mucosa
- Inhibits function of alveolar macrophages
- Causes hypertrophy of goblet cells and mucous glands
- Provokes release of elastase from polymorphonuclear neutrophils
- Causes destruction of alveolar parenchyma by inhibiting antitrypsin
- Increases airway resistance by stimulating irritant receptors
- Air Pollutants: Almost 3 billion people worldwide use biomass and coal as their main source of energy for cooking, heating, and other household needs. In these communities, indoor air pollution is responsible for a greater fraction of COPD risk than smoking or outdoor air pollution.
- Biomass fuels used by women for cooking account for the high prevalence of COPD among nonsmoking women in parts of the Middle East, Africa, and Asia. Indoor air pollution resulting from the burning of wood and other biomass fuels is estimated to kill two million women and children each year.
- Frequent lower respiratory infections during childhood.
- Congenital alpha-1 antitrypsin deficiency.
- Occupational dust and chemicals (such as vapors, irritants, and fumes)
Pathophysiology
COPD with Predominant Bronchitis: In such patients, the major pathology is increased activity of hypertrophic and hyperplastic mucus-secreting apparatus (goblet cells and mucous glands) throughout large and small airways. Excessive production of thick and viscid mucus results in characteristic cough and copious purulent sputum.
- The airway obstruction is primarily due to these changes in tire terminal bronchioles. Besides intraluminal secretions, some degree of bronchospasm, or thickening of the airway wall by edema, inflammation, or fibrosis contributes to the increased airway resistance.
- A component of airway hyper-responsiveness may further aggravate bronchial obstruction resulting in what is called asthmatic bronchitis.
- In oxidatively pure chronic bronchitis, pulmonary parenchyma is mostly intact, and oxygen diffusion capacity is near normal. However, the patient shows a more marked decrease in arterial pO2 (45-50 mmHg) as well as moderately elevated pCO2 (50-60 mmHg) and marked polycythemia.
- The abnormalities in blood gases arise chiefly from uneven ventilation/perfusion in different parts of the lungs. Some bronchioles are obstructed by mucus/inflammation/edema causing a marked decrease in ventilation, but fairly well-maintained perfusion. The physiological shunts lead to hypoxia and polycythemia.
- Increased pulmonary vascular resistance is an important feature of chronic bronchitis. It mainly results from chronic hypoxia. Other contributory factors include increased polycythemia, increased pCO2, and acidosis.
Confirmatory Pulmonary Function Tests: Forced vital capacity (FVC) is decreased
- Forced expiratory volume 1st second/vital capacity ratio (FEV1/FVC ratio) is decreased.
- Peak expiratory flow rate (PEFR) decreased.
- There is no significant improvement in FEV1/ FVC ratio and PEFR when tested after inhalation of a bronchodilator drug.
- Total lung capacity (TLC) is normal.
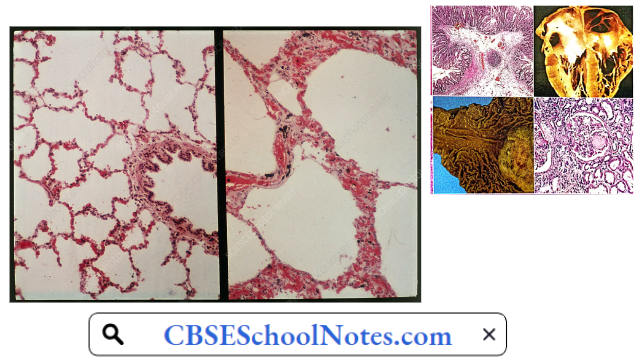
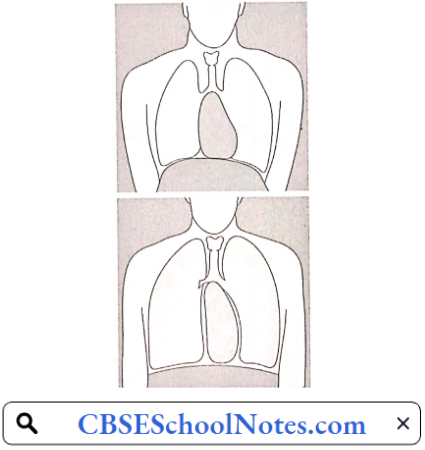
COPD With Prominent Emphysema: In such a patient, the primary problem is the degeneration of alveolar tissue. The destruction of air space walls reduces the surface area available for the exchange of oxygen and carbon dioxide during breathing.
- It also reduces the elasticity of the lung itself, which results in a loss of support for the airways that are embedded in the lung, leading to a decrease in the elastic recoil of the lungs.
- Therefore, the force that normally drives air out of the lungs during expiration decreases. Due to disruption of the alveolar septa, the support that keeps the small airways open due to transmural pressure is lost.
- Due to the loss of elastic fibers, compliance of the lungs increases, and the lungs are inflated to a larger volume for a given degree of increase in intrapulmonary pressure. The total lung capacity increases and the lungs remain permanently inflated. Residual volume and functional residual capacity are both increased.
- The chest becomes barrel-shaped. The diaphragm remains permanently flattened. As a result, diaphragm contraction cannot contribute to inspiratory effort. Inspiration is produced by the contraction of external intercostals only.
Due to the loss of elastic fibers, expiration is produced by the active contraction of expiratory muscles rather than by the passive recoil of elastic fibers. This results in dyspnoea and increased energy cost of work of breathing.
Confirmatory Pulmonary Function Tests
- Forced vital capacity (FVC) is decreased
- Forced expiratory volume 1st second/vital capacity ratio (FEV1/FVC ratio) is decreased.
- Peak expiratory flow rate (PEFR) decreased.
- There is no significant improvement in FEV1/ FVC ratio and PEFR when tested after inhalation of a bronchodilator drug.
- Total lung capacity (TLC) is increased.
Confirmatory Pulmonary Function Tests Complications
- Frequent respiratory infections
- Cyanosis
- Polycythaemia
- Congestive heart failure
- Respiratory failure
Pathophysiological Basis of Treatment
- Cessation of smoking
- Bronchodilators
- Antibiotics
- Oxygen therapy when the patient has cyanosis in the later stages of COPD
- Treatment of congestive heart failure (in later stages)
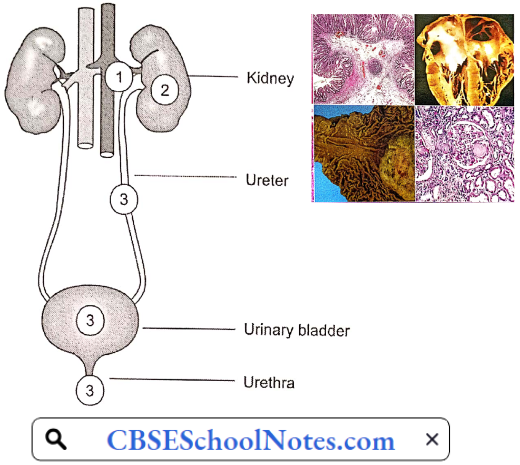
Diseases of the Kidney and the Urinary System
Disorders Of The Renal System
Kidney failure is defined as a condition when the kidneys are no longer able to remove the waste products from the body leading to their accumulation in the blood. This can cause unsafe levels of waste products to build up. This is known as kidney (or renal) failure. Unless it is treated, this can cause death. There are 2 main types of kidney (renal) failure: Acute (sudden) and chronic (over time).
Acute Renal Failure (ARF)
Acute renal failure is traditionally defined as an abrupt (within 48 hours) reduction in the rate of glomerular filtration, which manifests clinically as an abrupt and sustained increase in the serum levels of urea and creatinine with an associated disruption of salt and water homeostasis.
Read and Learn More Pathophysiology
The elevation of blood urea nitrogen (BUN) and serum creatinine levels is known as azotemia. Azotaemia is biochemical evidence of renal failure. (The normal range for blood urea is 20-40 mg/dl and the normal range for serum creatinine is 0.7-1.4 mg/dl.)
Symptoms Of Acute Renal Failure (ARF)
- Decrease in urine output (oliguria)
- Swelling of the hands, feet, and face (edema)
- Fatigue
- Nausea
- Confusion
- Seizures
- Coma
- Abnormal blood and urine tests
- High blood pressure
Pathogenesis Of ARF: Acute renal failure is classified as
- Pre-renal Azotaemia: It typically results from a severe decrease in renal blood flow due to severe blood loss leading to hypotension or severe dehydration. In this type of ARF, nephrons are normal. If blood volume is restored to normal, the patient makes a quick recovery.
- Renal Azotaemia: It occurs in response to cytotoxic, ischemic, or inflammatory insults to the kidney, with structural and functional damage to the nephrons. It is the most serious type of ARF. Recovery is slow.
- Post-renal Azotaemia: It includes disorders associated with obstruction of the urinary tract, for example, obstruction to the urethra by the enlarged prostate gland in males. Recovery is rapid after the removal of the obstruction.
With proper and timely treatment, most forms of ARI are reversible, since the kidney is a unique organ that can recover completely even after almost complete loss of renal function.
Prerenal Azotaemia
Prerenal Azotaemia Causes
- Hypovolemia: Hemorrhage, burns, dehydration, diuretics.
- Low Cardiac Output: Myocardial infarction, pulmonary embolism, CHF.
- Shock: Sepsis, anaphylaxis.
Prerenal azotemia represents the most common form (50 to 80%) of acute kidney failure and often leads to renal azotemia if it is not promptly corrected. All the conditions mentioned above cause renal hypoperfusion due to a decrease in the circulatory blood volume.
- A decrease in circulating blood volume activates high-pressure arterial baroreceptors leading to a reflex increase in sympathetic discharge, severe renal vasoconstriction, and a tendency to reduce GFR. When the renal hypoperfusion is severe, the renal compensatory mechanisms fail, resulting in a severe reduction in GFR and azotemia results.
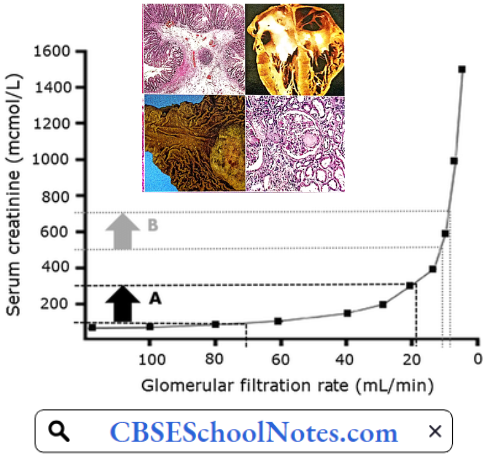
- Blood levels of urea or creatinine begin to rise only when GFR falls to less than 50% of normal. Any further delay in the treatment of hypovolemia results in such an intense renal vasoconstriction that the renal tubular epithelium undergoes ischemic necrosis (acute tubular necrosis, ATN).
Renal Azotaemia: One specific clinical disorder called acute tubular necrosis (ATN) accounts for most of the cases of intrinsic azotemia. It is produced by injury to renal parenchyma.
Pathogenesis Of Acute Tubular Necrosis: Acute tubular necrosis (ATN) is the term used to designate acute kidney injury resulting from damage to the tubules. The major causes of ATN are
- Ischaemic: Resulting from a severe or protracted decrease in renal perfusion (a complication of prerenal azotemia).
- Nephrotoxicity: Resulting from a variety of exogenous drugs that damage the kidneys.
- Hemoglobinuria: In case of incompatible blood transfusion, there is severe intravascular hemolysis leading to hemoglobinuria. The presence of hemoglobin in the kidney damages the renal tubules.
Pathology: Regardless of the pathogenesis, ATN is characterized by a common set of morphological changes. These morphologic changes usually appear in a segmental pattern with some segments of the nephron, such as the proximal tubule and thick ascending loop of Henle which are more susceptible than other parts of the nephron.
Tubular Epithelium: The tubular epithelium undergoes necrosis which can be seen by denudation of tubular epithelial cells. In some cases, the tubular basement membrane may rupture.
Tubular Lumen: The denuded and necrotic tubular epithelial cells ultimately fall into the tubular lumen and often plug the tubule in the form of proteinaceous casts. When ATN is initiated by hemolysis, heme pigment may be precipitated in the luminal debris.
ATN is a life-threatening but reversible disorder, if the underlying source of injury (i.e. renal ischemia or presence of toxin) is corrected. The tubular epithelium rapidly recovers and renal function is restored.
Post-renal Azotaemia: Approximately 5-10% of cases of acute azotemia are due to obstruction to the urinary tract. Since normal kidney function can be achieved by a single kidney, post-renal azotemia can occur if there is
- Obstruction of bladder neck (prostate pathology) or urethra.
- Bilateral ureteric obstruction, or
- Unilateral ureteric obstruction in a patient with only one functioning kidney.
The prostatic disease is the most common cause of post-renal azotemia. Continued formation of urine against the backdrop of obstruction to outflow causes an increase in intraluminal pressure upstream of the site of obstruction. Thus, there is a gradual distension of ureters, renal pelvis, and calyces (hydronephrosis).

- Ultimately, when the intraluminal pressure in the Bowman’s capsule becomes equal to hydrostatic pressure in the glomerular capillaries, filtration ceases. Cessation in glomerular filtration leads to azotemia, acidosis, fluid overload, and hyperkalemia.
- Post-renal azotemia is the most common cause of complete anuria because the basic cause is mechanical. In pre-renal and renal types of ARI, complete renal shutdown seldom occurs.
- With the relief of obstruction within 48 hours of onset, there is evidence that relatively complete recovery of GFR can be achieved within a week. Prolonged obstruction can lead to tubular atrophy and irreversible renal fibrosis.
Chronic Renal Failure
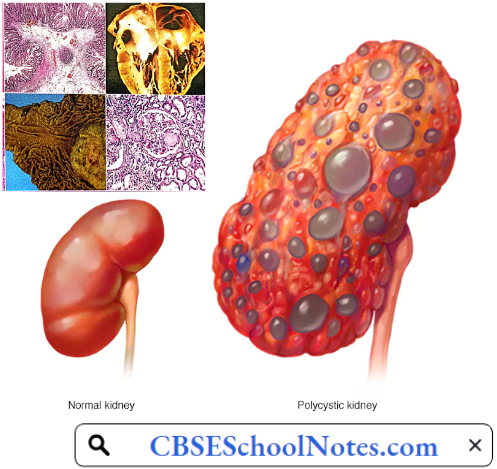
Chronic renal failure (CRF) refers to a decline in the glomerular filtration rate caused by a variety of diseases, such as diabetes, glomerulonephritis, and polycystic kidney disease. Patients with CRF have a high prevalence of hypertension.
Whether hypertension is a cause or a result of CRF remains debatable. Chronic renal failure is a continuous process that begins when some nephrons begin to be lost and ends when the remnant nephrons can sustain life no longer.
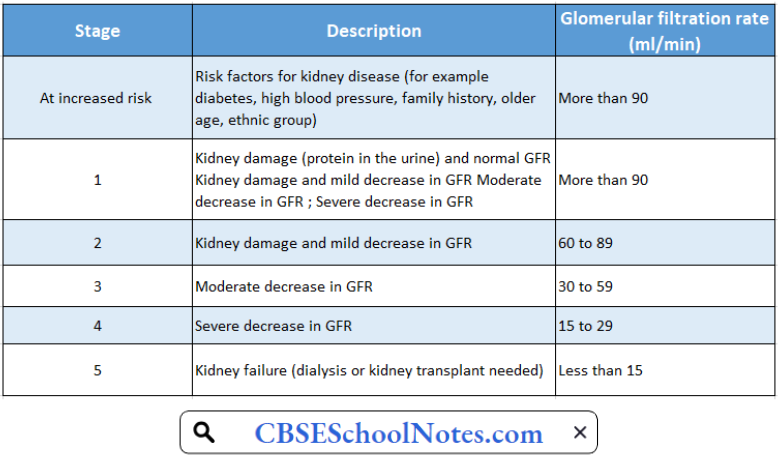
Chronic Renal Failure Classification: Staging of chronic kidney disease is a way of quantifying the severity of CKD. Chronic kidney disease has been classified into 5 stages. The end stage, when symptoms begin to appear, is known as uremia.
Stages Of Chronic Kidney Disease
Chronic Renal Failure Risk Factors: Factors that may increase the risk of chronic kidney disease include
- Diabetes
- High blood pressure
- Cardiovascular disease
- Smoking
Chronic Renal Failure Symptoms
- Nausea
- Vomiting
- Loss of appetite
- Fatigue and weakness
- Decreased mental sharpness
- Muscle twitches and cramps
- Swelling of feet and ankles
- Persistent itching
- Shortness of breath
- High blood pressure that is difficult to control
Aetiology
- Diabetes
- High blood pressure
- Glomerulonephritis, an inflammation of the kidney’s glomeruli
- Polycystic kidney disease
- Prolonged obstruction of the urinary tract, from conditions such as enlarged prostate, kidney stones, and some cancers
- Recurrent kidney infection, also called pyelonephritis
Pathology: The microscopic appearance of the “end-stage kidney” is similar regardless of cause, which is why a biopsy in a patient with chronic renal failure yields little useful information. The cortex is fibrotic, the glomeruli are sclerotic, there are scattered chronic inflammatory cell infiltrates, and the arteries are thickened. Tubules are often dilated and filled with pink casts.
Pathophysiology Of Uremia (End-Stage Renal Failure)
The most characteristic features of uremia are:
- Accumulation of nitrogenous waste products (urea, creatinine, uric acid, etc.) in the blood.
- Metabolic acidosis (due to failure of H+ excretion).
- Hyperkalaemia (due to failure of K+ excretion).
- Anemia (deficiency of erythropoietin).
- Uremic coma
The multiple organ failure in a uremic patient is due to the accumulation of some toxin(s) in the blood. However, the exact nature of the toxin(s) has not yet been identified. The final end product of carbohydrate and fat metabolisms is CO2 (and water), which can be easily excreted by the lungs.
The products of protein metabolism consist of a number of nitrogenous waste products which can be excreted only by the kidneys. Their accumulation in the blood consequent to renal failure is believed to be the cause of uremic toxicity.
- General Cellular Dysfunction: The most basic abnormality in uremia, at the cellular level, is partial inhibition of Na+– K+ pump, leading to a reduction in transmembrane potential, an increase in intracellular Na+, and a decrease in intracellular K+ concentrations. The most prominent result is an osmotically-induced overhydration of the cells.
- That is why salt and water retention is one of the important features of uremic syndrome. Overhydration of cerebral neurons is believed to be one of the factors contributing to the development of uremic encephalopathy.
- Additional factors decreasing intracellular K+ concentration include metabolic acidosis, poor dietary intake of K+, and excessive losses due to vomiting, diarrhea, or diuretics.
- Hypothermia: The sodium-potassium pump is the major consumer of ATP and hence the major cause of thermogenesis. Therefore, uremic patients have reduced energy metabolism, reduced BMR, subnormal body temperature, and an increased tendency to develop hypothermia.
- Anemia And Immune Dysfunction: Anemia is a regular feature of uremia. Normochromic normocytic anemia principally develops from decreased renal synthesis of erythropoietin, the hormone responsible for bone marrow stimulation for red blood cell production.
- Anemia associated with renal failure can be observed when the glomerular filtration rate (GFR) is less than 50 ml/min or when the serum creatinine is greater than 2 mg/dl. In the course of the disease, it becomes more severe as the GFR progressively decreases with the availability of less viable renal mass.
- Atrophy of lymphoid tissue leading to lymphopenia is common. The neutrophil count is usually normal. Uremic patients have impaired acute inflammatory response because of functional defects in neutrophils, monocytes, and lymphocytes. Therefore, uremic patients are more prone to infections. Clotting defects may also occur.
- Renal Osteodystrophy: In a uremic patient, a number of abnormalities Of the calcium, phosphate, and vitamin D metabolisms, such as hypocalcemia, hyperphosphatemia, increased PTH levels, and metabolic acidosis ultimately lead to renal bone disease (renal osteodystrophy).
- Renal osteodystrophy is characterized by areas of osteomalacia and osteoporosis and even osteosclerosis in various bones. These changes are seen more often in children or adults with slowly progressive chronic renal failure.
- Acidosis: Acidosis is another major metabolic abnormality associated with uremia. Metabolic acid-base regulation is controlled primarily by tubular cells of the kidney, while respiratory compensation is accomplished in the lungs. Failure to secrete hydrogen ions and impaired excretion of ammonium may initially contribute to metabolic acidosis.
- In uremia, metabolic acidosis may contribute to other clinical abnormalities, such as hyperventilation, anorexia, stupor, congestive heart failure, and muscle weakness. Uremic patients are likely to go into severe acidosis on exposure to exogenous acids, for example, high protein diet or endogenous acids such as lactic acid.
- Hyperkalemia: As renal function declines, the nephron is unable to excrete a normal potassium load, which can lead to hyperkalemia if dietary intake remains constant. In addition, other metabolic abnormalities, such as acidosis, may contribute to decreased potassium excretion and lead to hyperkalemia.
- The extracellular K+ concentration begins to rise progressively with the degree of azotemia. Serum K+ level of greater than 6.5 mEq/L is a clinical emergency.
- Cardiovascular Dysfunction: Left ventricular hypertrophy is a common disorder found in approximately 75% of patients of chronic renal failure who have not yet undergone dialysis. Left ventricular hypertrophy is associated with increased ventricular thickness, arterial stiffening, coronary atherosclerosis, and/or coronary artery calcification.
- Patients are at increased risk for cardiac arrhythmias due to underlying hyperkalemia and metabolic acidosis. Renal dysfunction may contribute to associated fluid retention, which may lead to uncontrolled hypertension and congestive heart failure.
- Fluid And Electrolyte Imbalance: In most cases of CRF, both total body sodium and water are increased and therefore the expansion of ECF volume may not be apparent. However, the patient is intolerant to both excessive salt intake and salt depletion. Excessive salt intake aggravates hypertension, congestive heart failure, ascites, or edema.
- Uremic patients also have impaired mechanisms for salt and water conservation. They are more prone to volume depletion in states of sodium loss (vomiting, diarrhea, fever) which may lead to orthostatic hypotension or circulatory shock. Volume depletion may produce further deterioration of renal function.
- Uremic Neuropathy: Uremic neuropathy is a distal sensorimotor polyneuropathy caused y uraemic toxins. The severity of neuropathy is correlated strongly with the severity of renal insufficiency. Paresthesias are the most common and usually the earliest symptom.
- Increased pain sensation is a prominent symptom. Weakness of lower extremities and atrophy follow the sensory symptoms. As disease progresses, symptoms move proximally and involve die upper extremities.
- Muscle cramps and restless legs syndrome were reported by 67% of uremic patients. Patients report that crawling, prickling, and itching sensations in their lower extremities are relieved partially by movement of the affected limb.
- Uremic Encephalopathy: Uremic encephalopathy (UE) is one of many manifestations of renal failure. Its exact cause is unknown. Accumulating metabolites of proteins and amino acids affect the entire neuraxis. No single abnormality can be precisely correlated with the clinical features of UE. Early symptoms include an inability to concentrate, drowsiness, and insomnia. Mild behavioral changes, loss of memory, and errors of judgment soon follow. Flapping tremors, chorea, stupor, seizures, and coma are seen in terminal stages.
- Malnutrition: Malnutrition usually occurs as renal failure progresses and is manifested by anorexia, weight loss, loss of muscle mass, low cholesterol levels, low BUN levels in the setting of an elevated creatinine level, and hypoalbuminemia.
- Co-morbid diseases, such as diabetes, congestive heart failure, or other diseases, that require reduced food intake or restrictions of certain foods may contribute to anorexia.
- Skin: The classic skin finding in persons with uremia is uraemic frost, which is a fine residue, thought to consist of excreted urea left on the skin after evaporation of water. Patients may become hyperpigmented as uremia worsens.
- Uremic pruritus remains one of the most frustrating, common, and potentially disabling symptoms in patients with end-stage renal disease. The exact cause is not yet clear.
Hemodialysis: Hemodialysis can be a life-saving measure in many types of acute renal failure produced by reversible pathological processes. Patients with chronic renal failure can also be kept alive for months or even years.
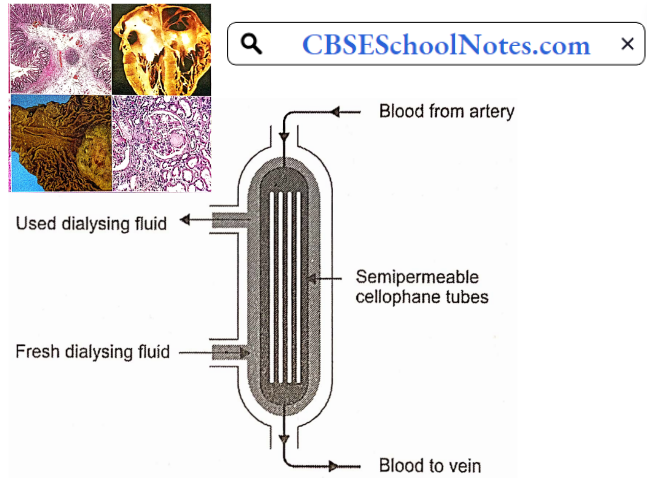
During hemodialysis, the patient’s radial artery is connected to a long and coiled cellophane tube immersed in a dialyzing fluid. The chemical composition of the dialyzing fluid is similar to that of plasma except that it is free of waste products, like urea, uric acid, etc.
Composition Of Dialyzing Fluid As Compared To That Of A Typical Uremic Plasma
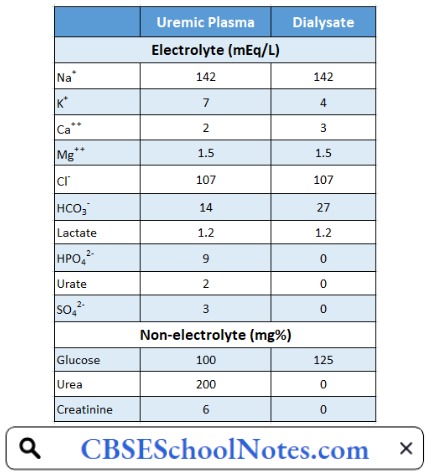
The patient’s blood passes through the dialyzing system and returns to a peripheral vein. The semipermeable cellophane membrane permits free diffusion of all the constituents of plasma except proteins. In this way, the dialysis of patient blood removes the toxic waste products and restores normal electrolyte concentration in the plasma. The dialyzing system is also known as the artificial kidney.
Hemodialysis is an expensive procedure and needs to be repeated almost every week. Therefore, it cannot be regarded as a remedy for irreversible renal failure caused by chronic renal diseases. With the recent advances in medical technology, such patients are treated by renal transplantation.
Haematological Disorders Types, Symptoms
Hematological Disorders
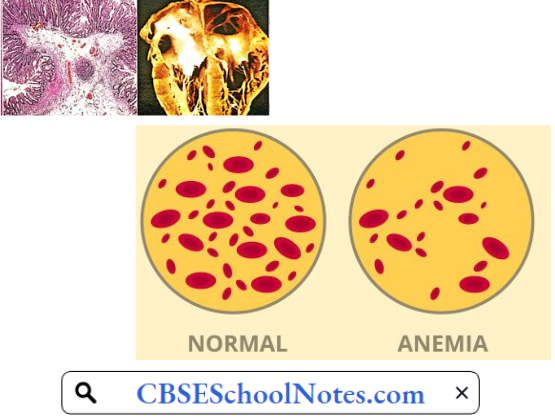
Anemia
Anemia is a global health problem. About 25% of the world’s population is anemic. Anemia is highly prevalent in India as well. In 2016, 51% of Indian women in the reproductive age group (15-49 years of age) and 57% of children under the age of 5 years were found to be anemic.
Surprisingly, 25% of Indian men were also found to be anemic. These statistics show that anemia is a national health problem in India.
Anemia Definition: Anemia is defined as a condition in which the hemoglobin concentration is below the normal range, for the age and sex of the individual. In adults, the lower limit of the normal range is taken as 13 g/dL in males and 12 g/dL in females (or hematocrit below 40% in males and 35% in females).
Read and Learn More Pathophysiology
Anemia Symptoms: Subnormal levels of hemoglobin decrease the oxygen-carrying capacity of the blood leading to a deficiency of oxygen in the tissues (hypoxia). The function of tissues with high oxygen demand such as the heart, brain, and exercising muscles is most affected. The symptoms of anemia include
- Pale skin
- Tiredness
- Palpitation
- Easy fatigability
- Generalized muscle weakness
- Lethargy
- Headache
- Light-headedness
- Cold hands and feet
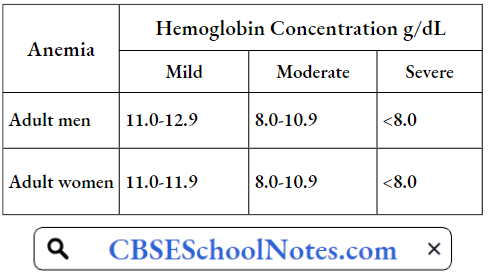
The severity of these symptoms increases with the severity of anemia. WHO has classified anemia as mild, moderate, and severe on the basis of hemoglobin concentration in the blood.
Classification Of Severity Of Anemia
When a patient is diagnosed as suffering from anemia, the treatment depends on its etiology (cause). However, before trying to find the cause, it is helpful to first classify anemia according to the red cell indices (laboratory classification) discussed below.
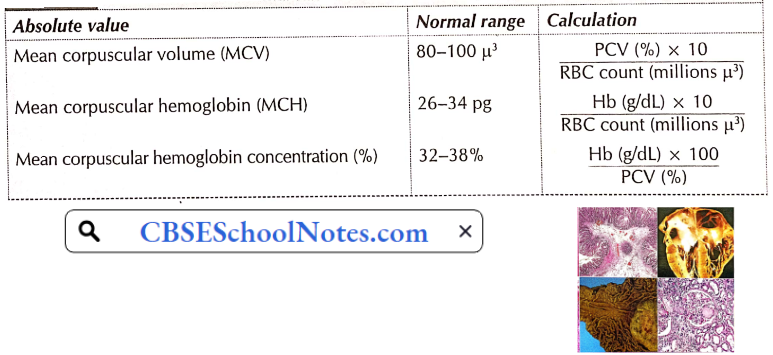
Red Cell Indices: From the RBC count, hemoglobin concentration, and hematocrit (PCV) value, certain indices (or absolute values) of the red cells of the person can be calculated. These absolute values are used in the laboratory diagnosis of anemia. The method of calculation and normal range of various red cell indices are shown in Table.
On The Basis Of Red Cell Indices, Anemia May Be Classified As
- Microcytic, normocytic or macrocytic, and
- Hypochromic or normochromic.
Once these indices are known, one can proceed to find out the cause.
Calculation And Normal Range Of Red Cell Indices
Aetiological Classification Of Anemias
- Deficiency anemia
- Hemorrhagic anemia
- Haemolytic anemia
- Aplastic anemia
Pathogenesis Of Anemia
1. Deficiency Anemia
Iron Deficiency Anemia: Iron deficiency is the most common cause of anemia in the world. Iron deficiency results in the efficient production of hemoglobin and the number of red blood cells. As explained below, it is more common in females than in males.
- It is important economically because it diminishes the capability of individuals who are affected to perform physical labor, and it diminishes both growth and learning in children. Anemic patients seem to be more prone to infections.
- Iron deficiency anemia is usually the end result of a long period of negative iron balance (iron intake is less than iron excretion). The daily requirement of iron in males is very little. Except for malnourished individuals, males are not prone to developing iron deficiency anemia.
- Therefore, in a male patient with such type of anemia, causes such as gastrointestinal blood loss, malabsorption or hookworm infestation should be looked for.
- Females in the reproductive age group are prone to develop iron deficiency because of loss of iron in menstruation, pregnancy, and lactation. Excessive menstrual losses or repeated pregnancies are the usual causes of iron deficiency anemia in women.
- Gastric surgery and achlorhydria are other causes of iron deficiency anemia which may occur both in males and females.
- Iron deficiency results in the production of a smaller number of red cells, which are not only deficient in hemoglobin (hypochromic) but also smaller in size (microcytic). Thus, in iron deficiency, the MCH is below 26 pg, MCHC below 32%, and MCV below 80 μ3
Severe iron deficiency not only interferes with erythropoiesis but also with cell division in many other tissues. Severe iron deficiency is associated with not only severe anemia but also with disorders of the tongue (atrophic glossitis), esophagus (dysphagia), and nails (koilonychia, spoon-like nails). Iron deficiency can be easily treated by oral administration of Fe2+ salts.

Pernicious Anemia: In India, pernicious anemia is not common. Pernicious anemia is caused by a deficiency of vitamin B12 in the body. Although the vitamin B12 content of the diet of these patients is usually normal, the vitamin is not absorbed in the gut.
- Normally, a glycoprotein (mol. wt. 45,000), known as an intrinsic factor, secreted by the gastric mucosa, helps in the absorption of vitamin B12 in the ileum. Atrophy of gastric mucosa results in the absence of intrinsic factors, leading to malabsorption of vitamin B12.
- Recent evidence suggests that pernicious anemia is an autoimmune disease. The auto-antibodies destroy both the parietal and chief cells of the gastric mucosa (gastric atrophy). Deficiency of vitamin B12 produces a megaloblastic bone marrow reaction and a very severe degree of anemia.
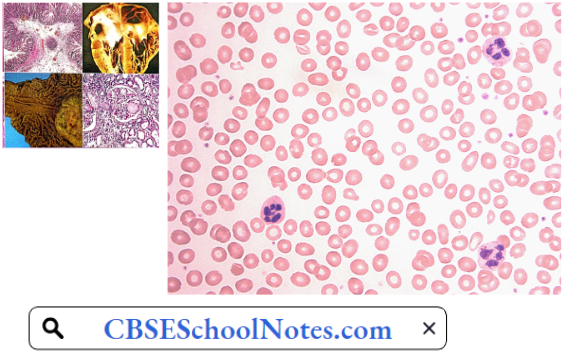
- In the peripheral blood, the red cells are larger in size (macrocytes, MCV greater than 100 μ3) but contain a normal concentration of hemoglobin (normochromic), i.e. vitamin B12 deficiency causes a macrocytic normochromic type of anemia.
The blood smear shows two characteristic features of red cells. Firstly, the cells show a wider variation in shape, i.e. all the red cells are not circular disks and vary in shape (poikilocytosis). Secondly, greater variation of cell size varies (4 pm to 12 pm, average 9.5 um (anisocytosis); normal variation 6.7 to 7.7 pm, average 7.5 pm).
Neural Symptoms In Pernicious Anemia: Vitamin B12 is essential for the synthesis of myelin. Therefore, vitamin B12 deficiency results in the destruction of thick myelinated fibers in the central and peripheral nervous system. Therefore, besides severe anemia, deficiency of vitamin B12 is associated with peripheral neuropathy and degeneration of posterior and lateral white columns of the spinal cord.
Pernicious Anemia Symptoms
- Lack of coordination
- Pain, numbness, and tingling in hands or feet
- Sensory loss
- Weakness of muscles
The disorder, if not treated, is invariably fatal. Pernicious anemia can be treated by regular administration of vitamin B12 by intramuscular route.
Folic Acid Deficiency Anemia: It occurs in individuals who do not take enough folic acid-rich food (green leafy vegetables, fresh fruits, meat). Folic acid deficiency is fairly common during pregnancy. It produces macrocytic normochromic type of anemia but there are no neurological problems. Folic acid deficiency anemia can be easily treated by oral administration of folic acid.
2. Hemorrhagic Anemia: This type of anemia usually results from mild chronic blood loss, for example, due to bleeding piles, excessive menstrual bleeding, or gastric ulcer. Blood loss leads to excessive loss of iron from the body.
Hence such patients usually show hypochromic microcytic (iron deficiency) type of anemia. Treatment of this type of anemia involves oral administration of iron salts as well as treatment of the underlying cause of chronic blood loss.
3. Hemolytic Anemia: The lifespan of normal red blood cells is approximately 120 days. Due to various congenital or acquired defects in the red blood cells, the life span of the red cells may be markedly reduced (as low as 30 days). The bone marrow tries to compensate for the increased rate of red cell destruction by the accelerated rate of erythropoiesis.
- When the rate of red cell regeneration cannot keep pace with the rate of red cell destruction, anemia develops. Moreover, an increased rate of red cell destruction overloads the excretory pathways of hemoglobin degradation products (bilirubin).
- Jaundice (hemolytic type) develops when the rate of bilirubin production exceeds the bilirubin excretory capacity of the liver.
- Hemolytic anemia is usually a normocytic normochromic type since there is no nutritional deficiency. Congenital hemolytic anemia is fairly common in India.
Hemolytic Anemia Causes
- Congenital Hemolytic Anemia
- Congenital (Hereditary) Spherocytosis: This disorder is caused by a congenital defect in the structural proteins in the cell membrane of red cells. Two important proteins, namely, spectrin and ankyrin, maintain the normal shape of red blood cells.
- A genetic defect in the synthesis of either of the two proteins results in a reduced surface area to volume ratio of the red cells. The cells tend to attain a spherical shape. The spherical shape makes the red cells less flexible. Spherocytes cannot bend or twist during passage through narrow capillaries and hence are damaged.
- The spleen seems to possess a special ability to detect and trap even mildly damaged red cells. Greater red cell destruction causes enlargement of the spleen. Thus, besides hemolytic anemia, splenomegaly is an important clinical feature of this disorder. The defect is inherited as an autosomal dominant trait.
- Congenital Disorders Of Hemoglobin: Hemolytic anemia may be due to a congenital defect in the globin chains of hemoglobin. These defects can mainly be divided into
- Hemoglobinopathies when there is an alteration in the amino acid sequences of a polypeptide chain of hemoglobin, for example, Hb S, Fib C, and Fib D.
- The thalassemia in which the amino acid sequence is not disturbed but synthesis of one of the two types of chains (α or β) is impaired.
- In hemoglobinopathies, the altered amino acid sequence results in an abnormality in the solubility of hemoglobin. Consequently, there is a striking abnormality in red cell morphology, which renders the red cell more prone to hemolysis, especially in the spleen.
- In thalassemia, suppression of either α or β chains results in deficient hemoglobin synthesis. Moreover, the absence of one type of polypeptide chain results in excessive production of the other type. This results in a disturbance in hemoglobin solubility and hence excessive hemolysis.
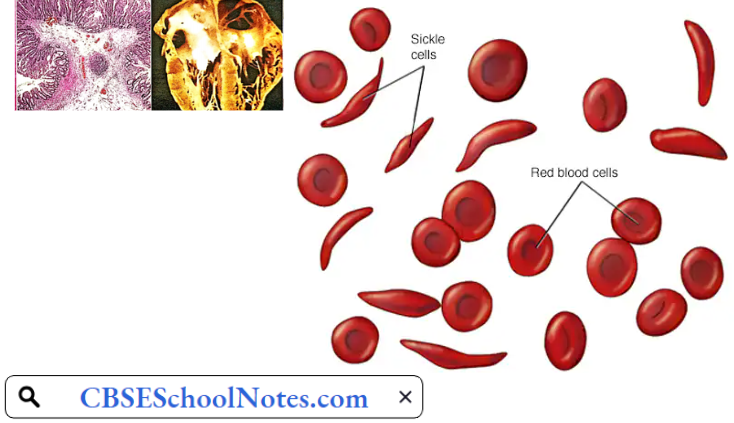
- Sickle Cell Anemia: This hemoglobinopathy is caused by the presence of amino acid valine instead of glutamic acid at position α of the β chains of hemoglobin. This variant is known as haemoglobin S (Hb S) because when deoxygenated, it polymerizes and distorts the red cell membrane into a sickle shape or a crescent shape.
- Hb S is highly prevalent in the black population of Africa but may be found in other countries also. Sickle cell anemia occurs in those individuals who are homozygous for Hb S gene. In such patients, the entire hemoglobin is Hb S type. In individuals who are heterozygous for Hb S gene, the red cells contain Hb S (50%) as well as normal Hb A (50%).
- Such individuals are said to have sickle cell trait. They act as carriers for the abnormal gene but do not suffer from hemolytic anemia.
- The sickle cells are not only abnormal in shape but also less elastic than normal biconcave red cells. The abnormal morphology makes the sickle cells more prone to hemolysis as well as gives a tendency to block the capillaries. The resultant tissue hypoxia causes further sickling of the red cells.
- Thalassemia: In thalassemia, the basic defect is the under-production of one type of the chains of globin component of hemoglobin. Two types of thalassemia are known: Thalassemia α and thalassemia β, depending on the name of the underproduced chains.
- In either case, the condition may be homozygous (thalassemia major) or heterozygous (thalassemia minor). Beta-thalassemia is common in the Mediterranean region, whereas thalassemia is seen in southeast Asia including India. Anemia is mild in patients with thalassemia minor, but very severe in those with thalassemia major.
- In the deficiency of one type of polypeptide chain, the red cells develop the tetramers of the other type, making red cells more prone to hemolysis.
- Congenital (Hereditary) Spherocytosis: This disorder is caused by a congenital defect in the structural proteins in the cell membrane of red cells. Two important proteins, namely, spectrin and ankyrin, maintain the normal shape of red blood cells.
- Acquired Haemolytic Anemia: Acquired hemolytic anemia results from the development of auto-antibodies against the red cells of the patient resulting in excessive destruction of the red cells. The auto-antibodies formed against red cell membrane antigens cause inappropriate destruction of red cells. Such type of anemia is not common in India.
4. Aplastic Anemia: Complete cessation of erythropoiesis is a rare but very serious and often fatal type of anemia. It arises as a complication of hypersensitivity reaction to certain drugs, for example, chloramphenicol, sulfonamides, etc. Excessive irradiation and cytotoxic drugs used in the treatment of malignant disorders also depress the bone marrow.
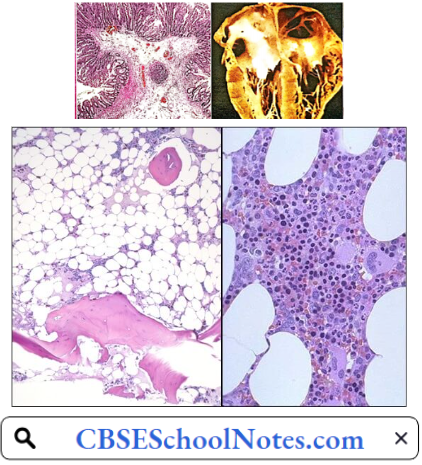
In most of such cases, besides very severe anemia, severe leucopenia, and thrombocytopenia is also present. Death may occur due to infection or severe blood loss. Bone marrow examination reveals the presence of adipose tissue where red bone marrow is normally present indicating cessation of hemopoiesis.
Complications Of Anemia: Left untreated, anemia can cause many health problems, such as
- Severe Fatigue: Severe anemia can make you so tired that you cannot complete everyday tasks.
- Pregnancy Complications: Pregnant women with folate deficiency anemia may be more likely to have complications, such as premature birth.
- Heart problems: Anemia can lead to a rapid or irregular heartbeat (arrhythmia). Severe anemia can lead to an enlarged heart or heart failure.
- Death: Some inherited anemias, such as sickle cell anemia, can lead to life-threatening complications.
Bleeding Disorders
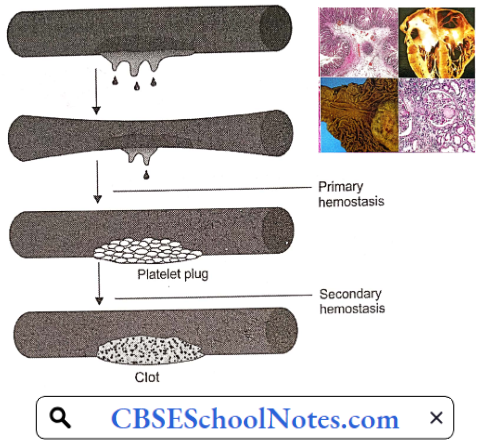
When a blood vessel is injured, hemostasis (stoppage of bleeding) occurs in two stages: Primary hemostasis results in the formation of a platelet plug which stops bleeding temporarily. The next step, secondary hemostasis results in the clotting of blood which stops bleeding permanently.
- Bleeding disorder may be due to a defect in either stage. Accordingly, bleeding disorders can be broadly classified into two categories
- Purpura results from a defect in primary hemostasis.
- Hemophilia results from a congenital defect in secondary hemostasis.
Purpura
Purpura Symptoms: This bleeding disorder is characterized by easy disability and spontaneous multiple hemorrhages under the skin and mucous membranes. At an early stage, the patient may present with numerous red spots of the size of a pinhead on the skin and mucous membranes (petechial hemorrhages). In more severe form, there are larger bleeding spots
- Easy or excessive bruising
- Superficial bleeding into the skin that appears as pinpoint-sized reddish-purple spots (petechiae)
- Bleeding from the gums or nose
- Blood in urine or stools
- Unusually heavy menstrual flow

Purpura Aetiology
- Thrombocytopenic purpuras—platelet counts are low.
- Nonthrombocytopenic purpuras—platelet levels are normal, suggesting another cause.
Purpura Pathogenesis: Idiopathic thrombocytopenic purpura (ITP), is an auto-immune disease resulting in greater destruction of platelets in the spleen. The platelet count in the blood is usually less than 50,000/μ3 Decreased platelet count results in a deficiency in the formation of platelet plugs. Hence blood vessels leak blood spontaneously or on mild trauma.
Risk Factors For Purpura Include:
- Infectious diseases, particularly among children and the elderly
- Poor nutrition when it leads to a lack of vitamin C
- Some forms of cancer, such as leukemia and myeloma
- Advanced age
- Poor blood vessel health
Hemophilia
Hemophilia Symptoms: In this disorder, bleeding occurs several hours after an injury. Such bleeding mostly occurs in deep tissues like muscles and joints. Characteristic clinical findings are hemarthrosis (bleeding into a joint) and muscle hematomas.
Hemophilia Aetiology: Hemophilia is a congenital bleeding disorder. Most commonly, there is a congenital deficiency of clotting factor 8. The condition is called hemophilia-A. In a few cases, clotting factor 9 is deficient (hemophilia-B). The disorder is transmitted as an X-chromosome-linked recessive trait. The only effective therapy is intravenous injections of the deficient clotting factor.
Hemophilia Pathogenesis: Factors 8 and 9 are involved in the intrinsic system of coagulation of blood. Deficiency of clotting factor 8 or 9 results in the formation of a weak blood clot in an injured blood vessel. Therefore, the blood vessel starts bleeding again after the effect of primary hemostasis wanes.
Hemophilia Complications
- Deep internal bleeding, for example, deep-muscle bleeding, leads to swelling, numbness or pain of a limb.
- Joint damage from hemarthrosis (hemophilic arthropathy), with severe pain, disfigurement, and even destruction of the joint.
- Intracranial hemorrhage is a serious medical emergency that can cause brain damage and death.
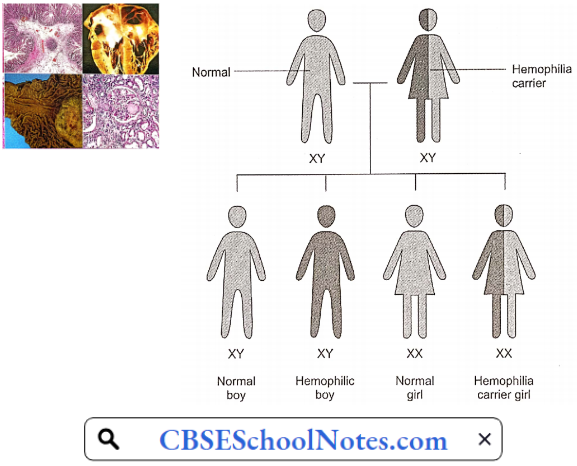
Genetics: The X and Y chromosomes are called sex chromosomes. The gene for hemophilia is carried on the X chromosome. Hemophilia is inherited in an X-chromosome-linked recessive manner. Females inherit two X chromosomes, one from their mother and one from their father (XX).
- Males inherit an X chromosome from their mother and a Y chromosome from their father (XY). That means if a son inherits an X chromosome carrying hemophilia from his mother, he will suffer from hemophilia. It also means that fathers cannot pass hemophilia on to their sons.
- But because daughters have two X chromosomes, even if they inherit the hemophilia gene from their mother, most likely they will inherit a healthy X chromosome from their father and not have hemophilia.
- A daughter who inherits an X chromosome that contains the gene for hemophilia is called a carrier. She can pass the gene on to her children. Hemophilia can occur in daughters but is rare.
For A Female Carrier, There Are Four Possible Outcomes For Each Pregnancy:
- A girl who is not a carrier
- A girl who is a carrier
- A boy without hemophilia
- A boy with hemophilia
Spontaneous mutations of genes account for about 30% of all cases of hemophilia, i.e. family history may be absent.
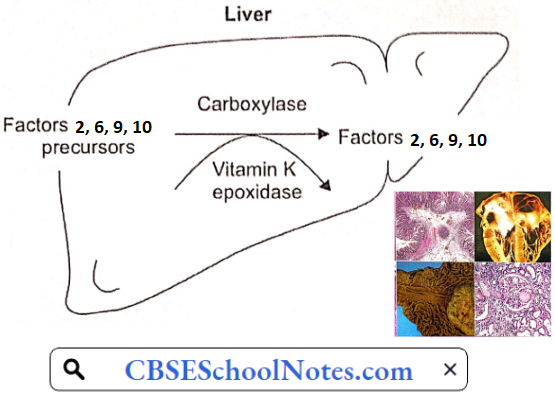
Acquired Defects of Secondary Hemostasis: These defects are far more common than congenital disorders of secondary hemostasis. Clotting factors prothrombin (clotting factor 2) and clotting factors 7, 9, and 10 are synthesized in the liver. Their synthetic reactions require vitamin K.
Severe liver disease or deficiency of vitamin K may cause deficiency of these clotting factors leading to severe and prolonged bleeding after a minor trauma. Intestinal bleeding is one of the serious complications of liver cirrhosis.
Causes Of Vitamin K Deficiency
- Some newborn babies are vitamin K deficient.
- Obstructive jaundice: Since bile-containing bile salts do not reach the small intestine, fats and fat-soluble vitamins including vitamin K are not absorbed in the gut.
- Prolonged administration of broad-spectrum antibiotics destroys bacteria in the large intestine. These bacteria are an important source of vitamin K.
- Overdose of oral anticoagulants (dicoumarol)
- Dietary deficiency of vitamin K is rare.
Endocrine Disorders: Causes, Signs, Types
Endocrine Disorders
Diabetes Mellitus
Diabetes currently affects more than 62 million Indians, which is more than 7.2% of the adult population. Nearly 1 million Indians die due to diabetes every year. The high incidence is attributed to a combination of genetic susceptibility plus the adoption of a high-calorie diet, coupled with a low-activity lifestyle by India’s growing middle class.
Two Types Of Diabetes Mellitus (DM) Are Recognized
- Type 1 Diabetes Mellitus: Type 1 or insulin-dependent diabetes mellitus (IDDM) is juvenile-onset diabetes. In type I diabetes, there is an absolute deficiency of insulin. It is believed to be an autoimmune disease, which manifests in childhood. The patients are usually lean. Ketosis and acidosis are common complications of this type of diabetes. Plasma insulin levels are very low or undetectable.
- Type 2 Diabetes Mellitus: Type 2 diabetes manifests after the age of 40 years. Most of the patients with this type of diabetes are obese. Plasma insulin levels are often normal or even elevated. However, there seems to be a deficiency of insulin receptors in the tissues so at the tissue level, circulating insulin is ineffective. Ketotic acidosis is not very common in type 2 diabetes.
Read and Learn More Pathophysiology
Symptoms And Signs Of Diabetes Mellitus
- Polyuria
- Polydipsia
- Weight loss despite polyphagia
- Hyperglycemia
- Glycosuria
- Muscle weakness
- Frequent infections
- Ketosis
- Acidosis and
- Coma
Diabetes Mellitus Pathogenesis: At the metabolic level, fundamental defects in DM are
- Decreased glucose utilization
- Increased glucose production
- Increased lipolysis
- Increased protein catabolism
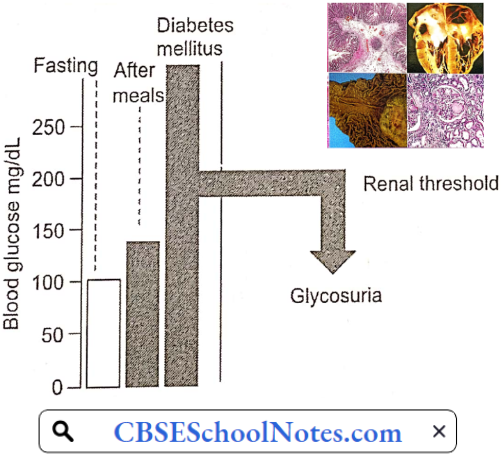
Diabetes mellitus starts without any symptoms. Gradually the condition worsens and when the blood sugar level is above 180 mg%, sugar appears in the urine. Only then does the patient become aware of the problem. In many cases, diabetic patients come to know about their disease only when they visit a physician for some other ailment and their blood glucose level is tested.
1. Hyperglycemia And Its Consequences: Hyperglycemia is one of the cardinal features of diabetes mellitus. It is due to
- Decreased peripheral utilization of glucose and
- Increased hepatic production of glucose (gluconeogenesis).
Mild transient hyperglycemia is harmless and occurs after every meal. However, when the blood glucose level is chronically elevated, numerous complications arise. When the blood glucose level exceeds the renal threshold, glucose appears in the urine (glycosuria).
Renal excretion of osmotically active glucose molecules leads to the loss of large amounts of water in the urine (osmotic diuresis). The resultant dehydration activates the thirst mechanism leading to a large amount of water intake (polydipsia). The loss of glucose in the urine means loss of energy (calories) from the body.
An appreciable amount of Na+ and K+ are lost in the urine as side effects of osmotic diuresis. Deficient utilization of glucose in the hypothalamic ventromedial nuclei (satiety center) causes hyperphagia. In spite of excessive food intake, there is a loss of body weight liable to infections.
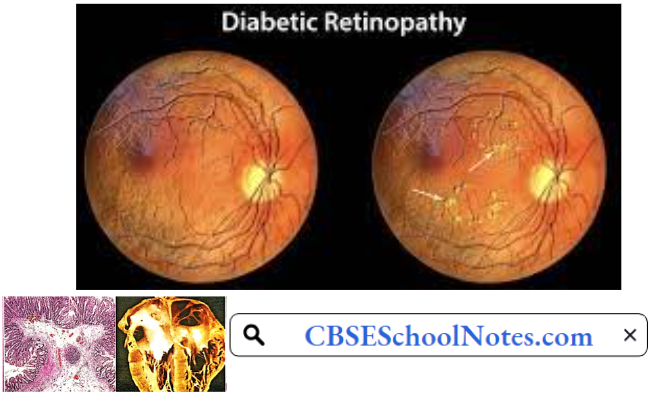
Chronically elevated blood glucose levels result in the attachment of glucose (glycosylation) to hemoglobin and tissue proteins. Tissue protein damage is responsible for long-term complications such as neuropathy, retinopathy, cataracts, nephropathy (kidney damage), and hypertension.
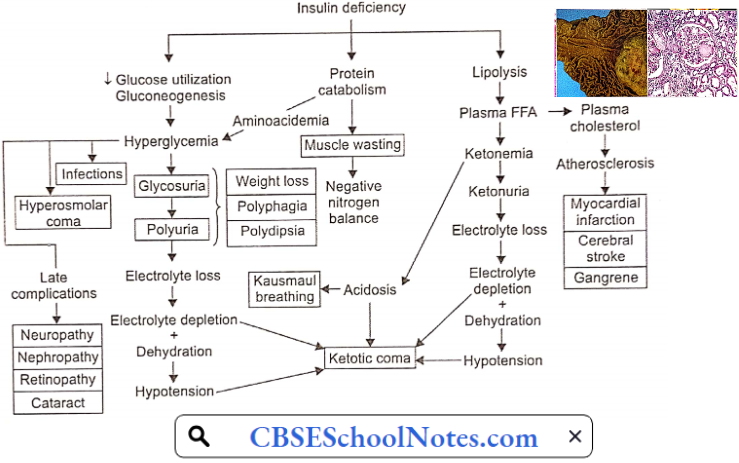
2. Ketosis And Its Consequences: A deficiency of insulin causes a great reduction in lipogenesis and accelerates the process of lipolysis. As a result, the plasma level of FFA is more than doubled.
- Free fatty acids provide energy to the glucose-starved insulin-sensitive tissues, like skeletal muscle. However, FFA mobilization also causes the formation of ketone bodies. The ketone body’s formation exceeds the rate of their utilization leading to ketosis and acidosis.
- Acidosis results in rapid, deep respiration (dyspnoea). The patient’s breath smells of acetone. The urine becomes highly acidic. When the capacity of the kidney to replace plasma cations accompanying the organic anions with H+ and NH4 is exceeded, Na+ and K+ are lost in the urine.
- The electrolyte and water loss leads to dehydration, hypovolaemia, and hypotension. Finally, acidosis and dehydration may depress the consciousness to the level of coma and death.
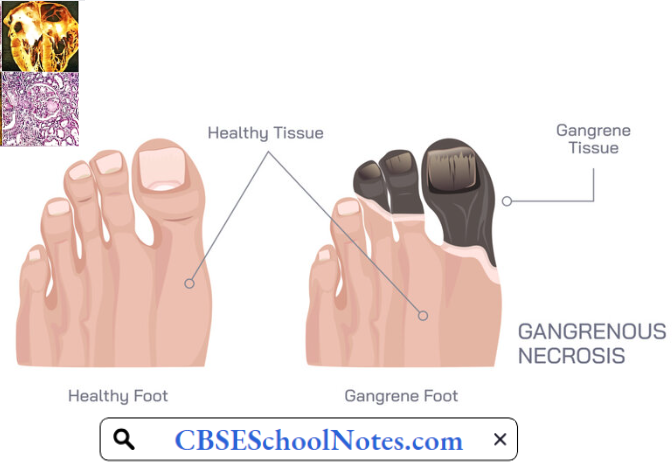
- Chronic hyperlipidemia leads to atherosclerosis which causes coronary artery disease cerebral stroke and gangrene in the lower limbs.
3. Protein Catabolism: In diabetes, protein anabolism is suppressed and catabolism is increased. Large amounts of amino acids are used for energy production. Amino acids also act as substrates for enhanced gluconeogenesis promoted by insulin deficiency. Consequently, the patient suffers from loss of weight, protein depletion, wasting, and negative nitrogen balance.
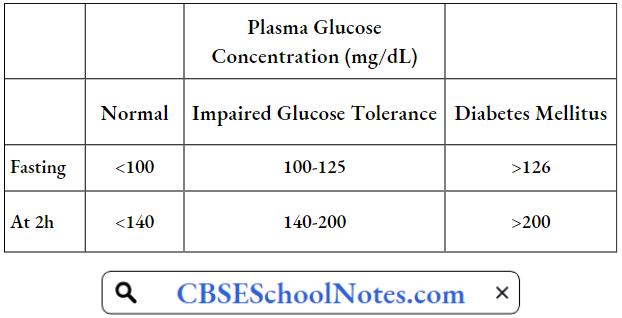
Glucose Tolerance Test (GTT): This is a test for the diagnosis of diabetes mellitus. After an overnight fast, a venous blood sample is taken. Then, the patient is given 75 g of glucose orally and four blood samples are collected half-hourly for estimation of plasma glucose levels. Plasma glucose levels are plotted against a time scale and the graph so obtained is known as the glucose tolerance curve.
The Results Are Interpreted As Follows:

Important Role Of Estimation Of Glycosylated Hemoglobin: In a normal subject, glucose molecules get a non-enzymic attachment to a small proportion (<7%) of hemoglobin-A to form glycosylated hemoglobin. In case of sustained hyperglycemia, such as in diabetes mellitus, a greater proportion (10-20%) of hemoglobin is glycosylated.
- The concentration of glycosylated hemoglobin has been found to reflect the average blood glucose level during the previous 6-8 weeks.
- Therefore, its measurement has become an important tool for the proper regulation of antidiabetic therapy, that is, to find out whether the given dose of the medication has been able to maintain blood glucose level within the physiological range during the previous 6-8 weeks. (The glucose tolerance test reflects the glucose level on the day of the test only.)
Long-term Complications Of Diabetes Mellitus
- Neuropathy, leading to numbness and muscle weakness
- Retinopathy, leading to blindness
- Cataract
- Nephropathy, leading to chronic renal failure
- Hypertension
- Coronary artery disease, and
- Strokes.
- Gangrene in lower limbs
Risk Factors For Type 1 Diabetes Include:
- Family History
- Genetics: The presence of certain genes indicates an increased risk of developing type 1 diabetes.
- Geography: The incidence of type 1 diabetes tends to increase as you travel away from the equator.
Risk Factors For Type 2 Diabetes Include:
- Overweight
- Inactivity
- Family History
- Age: The risk of type 2 diabetes increases as you get older, especially after age 45.
- Prediabetes: Prediabetes is a condition in which one’s blood sugar level is higher than normal, but not high enough to be classified as diabetes. Left untreated, prediabetes often progresses to type 2 diabetes.
- Gestational Diabetes: If one develops gestational diabetes, she has a greater risk of type 2 diabetes.
Disorders Of Thyroid Gland
Diseases of the thyroid gland are among the most abundant endocrine disorders worldwide second only to diabetes; India is no exception. Recent report shows that 300 million people in the world are suffering from thyroid disorders and among them about 42 million people reside in India.
Hypothyroidism is the most common thyroid disorder. Hyperthyroidism is less common. Thyroid disorders are more common in women than in men.
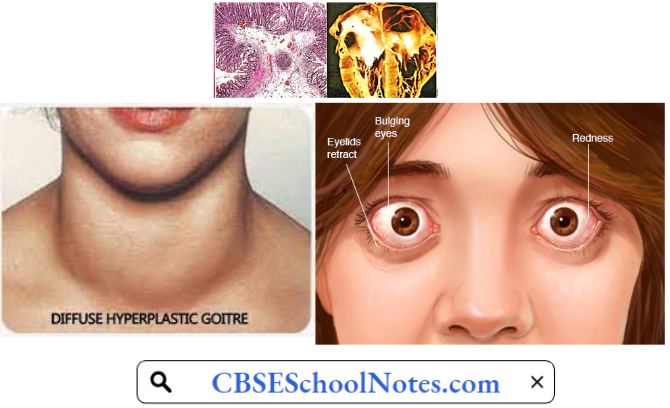
Hyperthyroidism: Hyperthyroidism results from excessive secretion of thyroid hormones. It is known as Graves’ disease or exophthalmic goiter. Less commonly, excessive thyroxine secretion is due to a thyroid adenoma (toxic thyroid adenoma).
Hyperthyroidism Aetiology: Graves disease is an autoimmune disorder characterized by the development of thyroid-stimulating immunoglobulin (TSI).
- TSI acts on thyroid stimulating hormone receptors (TSH-receptors) on the thyroid follicular cells to activate thyroid hormone synthesis and release as well as causes hypertrophy and increased vascularity of the thyroid gland.
- This results in the characteristic picture of Graves’ thyrotoxicosis, with a diffusely enlarged thyroid and excessive plasma thyroxine levels.
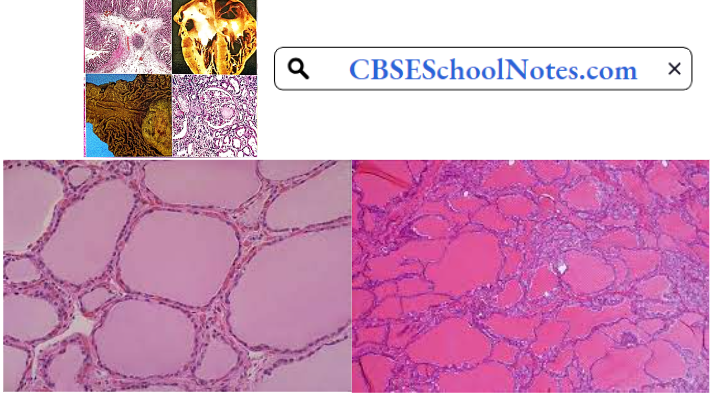
Hyperthyroidism Pathology: There is a diffuse thyroid enlargement of the thyroid gland (goiter). Microscopically, thyroid follicles are hypercellular and lined by tall columnar cells. In the follicles, colloids is scanty and show semi-lunar erosions near the follicular cells. Stroma shows lymphocytic infiltration.
Hyperthyroidism Symptoms And Signs: All the symptoms and signs reflect the effects of increased plasma thyroxine levels on various organs and tissues of the body
- Palpitation
- Tachycardia
- Nervousness
- Loss of weight
- Easy fatigability
- Restlessness
- Fine tremor
- Excessive appetite
- Diarrhea
- Excessive sweating
- Heat intolerance
- Muscle weakness
- Increased basal metabolic rate (BMR)
Some patients develop protrusion of eyeballs due to oedematous swelling of retrobulbar tissue (exophthalmos).
Hyperthyroidism Complications
- Tachycardia
- Atrial fibrillation
- Congestive heart failure
- Osteoporosis
- Ophthalmopathy
- Hyperthyroid crisis
Hyperthyroidism is commonly treated by the administration of anti-thyroid drugs, i.e. drugs that interfere with the synthesis of thyroxine.
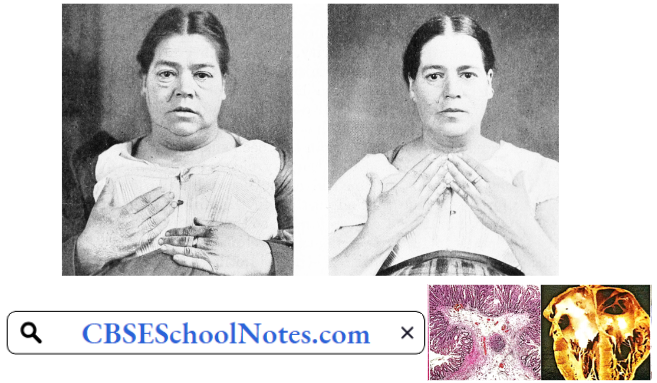
Hypothyroidism
1. Adult Hypothyroidism (Myxoedema): This is a common disorder, especially in middle-aged females.
Hypothyroidism Aetiology: The most common cause of hypothyroidism is an autoimmune disorder known as Hashimoto’s thyroiditis. Autoimmune disorders occur when our immune system produces antibodies that attack our own tissues.
Hypothyroidism Pathology: Microscopically, the thyroid shows atrophic follicles, fibrosis, and diffuse lymphocytic infiltration.

Hypothyroidism Symptoms And signs: All the symptoms signs are the result of decreased plasma thyroxine levels on various tissues of the body.
- A puffy face is a characteristic finding. It is due to the accumulation of myxomatous gel in the subcutaneous tissue in the face.
- Slow heart rate
- Cold intolerance
- Increased body weight
- Muscle weakness
- Constipation
- Dry skin (lack of sweating)
- Decreased appetite
- Low BMR
- Somnolence
- High blood cholesterol
- Mental sluggishness
Hypothyroidism Complications
- Atherosclerosis
- Coronary artery disease
- Congestive heart failure
- Stroke
- Infertility
- Hypothermia
- Mental depression
- Myxoedema coma
Hypothyroidism is easily treated by oral administration of thyroxine.
2. Cretinism: This disorder results from a congenital deficiency of thyroxine. The child’s physical and mental growth is retarded leading to permanent mental deficit. The most common cause of cretinism is maternal iodine deficiency during pregnancy.
By the time the typical clinical picture develops in the infant, it is usually too late to reverse the mental retardation. The realization of this fact has led to the widespread use of iodized salt in India and many other countries.
3. Iodine-Deficiency Goitre: A dietary intake of at least 100-150 pg of iodide per day is required for normal thyroid function. Inadequate thyroid secretion occurs when iodide intake falls below 10 pg/ day. Due to the negative feedback mechanism, the secretion of TSH from the anterior pituitary is increased leading to hypertrophy of the thyroid gland.
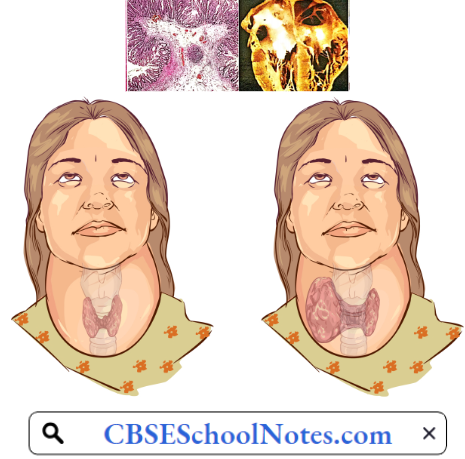
The enlarged hypertrophied thyroid gland so produced is known as iodine-deficiency goiter. Use of iodized salt can prevent the disorder.
Disorders Of Sex Hormones
Testosterone Deficiency: It is hard to know how many men among us have testosterone deficiency (TD), although data suggest that overall about 2.1% may have TD. As few as 1% of younger men may have TD, while as many as 50% of men over 80 years old may have TD.
Disorders Of Sex Hormone Symptoms
- Reduced sex drive
- Reduced erectile function
- Loss of body hair
- Less beard growth
- Loss of lean muscle mass
- Feeling very tired all the time (fatigue)
- Symptoms of depression
Disorders Of Sex Hormones Causes
- Klinefelter syndrome (rare congenital defect)
- Damage to testicles by accident
- Removal of testicles because of cancer
- Aging
- Obesity
- Metabolic syndrome (high blood pressure, high blood sugar, unhealthy cholesterol levels, and belly fat)
- Use of medications such as antidepressants and narcotic pain medications
Erectile Dysfunction (Impotence): Erectile dysfunction is defined as the inability to attain a penile erection of sufficient rigidity for vaginal penetration. The prevalence of impotence increases rapidly after the age of 50 years, especially in those with diabetes mellitus or atherosclerosis.
Impotence may be due to severe hypogonadism which causes erectile failure as well as loss of libido (sexual interest and initiative). However, in most cases, the erectile dysfunction can be attributed to atherosclerosis of the penile blood vessels or autonomic neuropathy involving nervi erigentes. In some cases, impotence may be psychological.
Infertility: The failure to conceive after one year of unprotected intercourse is called infertility. It affects about 10% of married couples. The problem may be in the husband or the wife or both. The congenital causes of male infertility are not common.
More common causes of male infertility are acquired defects of the testes which include viral orchitis (mumps virus) and testicular trauma. The patient’s semen usually shows low sperm count and/or decreased sperm motility.
Low Oestrogen Levels
Low Oestrogen Levels Cause
- Turner syndrome (a rare congenital defect)
- Premature ovarian failure
- Thyroid disorders
- Excessive exercise
- Being severely underweight
- Low-functioning pituitary gland
Low Oestrogen Levels Symptoms
- Irregular periods.
- Infertility: Low estrogen levels can prevent ovulation and make getting pregnant difficult, leading to infertility.
Female Infertility: The absence of ovulation during the reproductive age of the female may result from isolated gonadotropin deficiency or primary ovarian failure. Blockade of fallopian tubes by pelvic inflammation is a fairly common cause of female infertility in spite of normal ovulatory ovarian cycles.
Nervous System Diseases: Types, Causes, Signs
Disorders Of Nervous System
Stroke
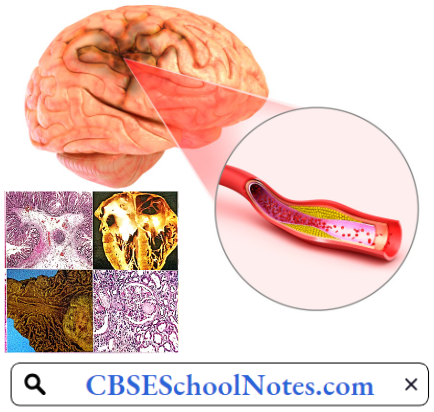
Stroke is one of the most devastating consequences of two common diseases, atherosclerosis and hypertension. It represents the second leading cause of death (after coronary artery disease) and a major cause of disability worldwide. Besides age, hypertension is the most important cardiovascular risk factor for developing both ischemic and hemorrhagic stroke.
Definition Stroke: The sudden death of some brain cells due to lack of oxygen when the blood flow to the brain is impaired by blockage or rupture of an artery to the brain is known as stroke.
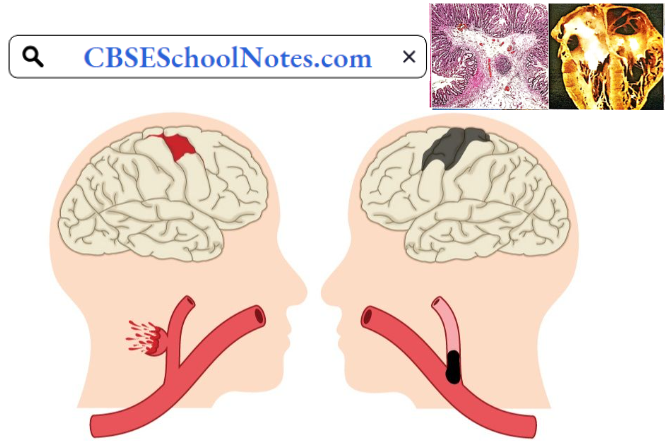
Stroke Causes: There are two types of stroke.
- Ischemic Stroke In a patient with atherosclerosis, a thrombus formation in one of the blood vessels supplying the brain blocks the blood flow to a part of the brain. That area undergoes ischemic necrosis and loss of function.
- In some patients, a blood clot in the heart or a blood vessel becomes loose (called an embolus), travels in the arterial system, and blocks a blood vessel in the brain, resulting in ischemia and necrosis. Ischemic stroke can also occur when a large atherosclerotic plaque clogs the brain’s blood vessels. About 80% of all strokes are ischaemic.
- Hemorrhagic Strokes occur when a blood vessel in the brain ruptures. The result is blood seeping into the brain tissue, causing damage to brain cells. The most common causes of hemorrhagic stroke are high blood pressure and cerebral artery aneurysms. An aneurysm is an abnormal focal dilation of an artery in the brain that results from a weakening of the muscular layer.
Read and Learn More Pathophysiology
Stroke Symptoms: The most common symptoms of a stroke are
- Weakness or numbness of the face, arm, or leg on one side of the body
- Loss of vision in one or both eyes
- Loss of speech, difficulty talking, or understanding what others are saying
- Sudden, severe headache
- Loss of balance or unstable walking
Stroke Signs
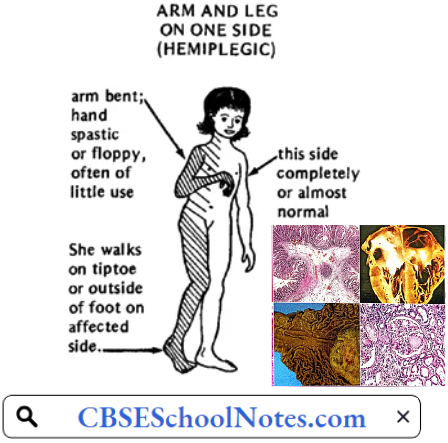
- Paralysis: The paralysis affects movements of the face, arm, and leg
- Muscle Tone: Hypertonia (spasticity) is most prominent in the antigravity muscles (flexors of the upper limb and extensors of the lower limb). When a passive flexion of a limb is attempted, initially the examiner feels a lot of resistance. But if the attempt is continued, the resistance suddenly disappears. This phenomenon is called spasticity or clasp-knife effect.
- Deep Reflexes: Knee jerks, ankle jerks, and biceps jerks are exaggerated.
- Superficial Reflexes: Abdominal and plantar reflexes are absent.
- Babinski’s sign is present.
- Sensory Deficit: In patients with more extensive lesions of the internal capsule, the sensory and visual fibers are also affected.
- Recovery: In many patients, a considerable degree of recovery occurs. Muscles of the lower limb and proximal muscles of the upper limb show better recovery of voluntary control than fine muscles of the hands and fingers.
Stroke Pathogenesis
- Ischemic Stroke: Ischemic stroke occurs because of a loss of blood supply to part of the brain. Cerebral ischemia initiates a series of changes called the ischemic cascade. Brain tissue ceases to function if deprived of oxygen for more than 60 to 90 seconds, and after approximately three hours will suffer irreversible injury leading to the death of the tissue, i.e. cerebral infarction.
- Atherosclerosis may disrupt the blood supply by
- Narrowing the lumen of blood vessels leads to a reduction of blood flow, or
- By causing the formation of blood clots within the vessel,
- Embolic infarction occurs when emboli formed elsewhere in the circulatory system, typically in the heart as a consequence of atrial fibrillation, or in the carotid arteries, break off, enter the cerebral circulation, and then lodge in and block brain blood vessels.
- Brain tissue is especially vulnerable to ischemia since it has little respiratory reserve and is completely dependent on aerobic metabolism, unlike most other organs. Since blood vessels in the brain are now blocked, the brain becomes low in energy, and thus it resorts to using anaerobic metabolism within the region of brain tissue affected by ischemia.
- Anaerobic metabolism of glucose can produce adenosine triphosphate (ATP) but releases a by-product called lactic acid. Lactic acid is an irritant that could potentially destroy cells since it is an acid and disrupts the normal acid-base balance in the brain.
- As oxygen or glucose becomes depleted in ischemic brain tissue, the production of ATP fails, leading to the failure of the energy-dependent sodium-potassium pump necessary for tissue cell survival. This sets off a series of interrelated events that result in cellular injury and death.
- Besides the failure of the sodium-potassium pump, another major cause of neuronal injury is the release of the excitatory neurotransmitter glutamate. Glutamate is normally stored within the neurons. During neuronal activity, glutamate is released into the cerebral extracellular fluid (ECF), but its extracellular concentration is immediately decreased by its re-uptake into the neurons.
- The re-uptake process is also dependent on an ATP-dependent sodium-potassium pump. In the deficiency of ATP, glutamate concentration in the cerebral ECF increases. Glutamate produces an influx of calcium into the neurons which activates enzymes that digest the cells’ proteins, lipids, and nuclear material.
- Calcium influx can also lead to the failure of mitochondria, which can lead further toward energy depletion and trigger cell death. Ischemia also induces the production of oxygen free radicals and other reactive oxygen species which are lethal to the neurons.
- Hemorrhagic Strokes: Hemorrhagic stroke constitutes about 10% of total strokes. Hypertension is the major cause of rupture of a cerebral blood vessel. The rupture of an aneurysm in the cerebral artery is another cause. Hemorrhagic strokes result in mechanical tissue injury by causing compression of tissue from an expanding hematoma.
- In addition, the pressure may lead to a loss of blood supply to affected tissue with resulting infarction. The third pathogenic mechanism is the direct toxic effect of blood in the cerebral ECF. Inflammation contributes to the secondary brain injury after hemorrhage.
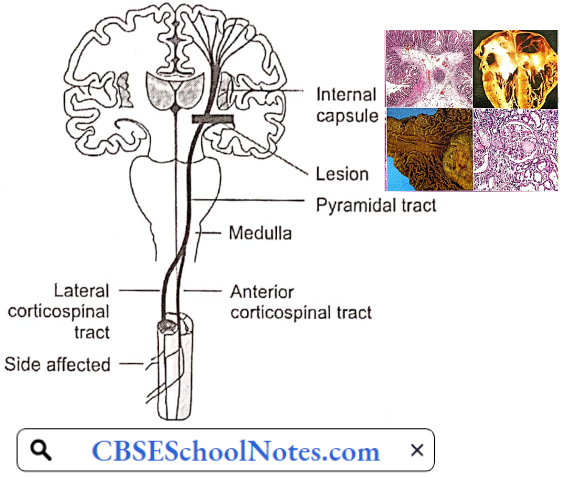
Stroke Pathophysiology: The changes in the brain described above occur most often in the middle cerebral artery, which supplies the region called the internal capsule. All tire descending motor fibres of the corticospinal tract as well as tire sensory fibers ascending to the sensory cortex pass through the internal capsule.
- Depending on the extent of the lesion in the internal capsule, stroke may result in only motor deficit or motor as well as sensory deficit.
- Moreover, because of the decussation of the corticospinal tract and sensory tract in the medulla, the internal capsule lesion produces motor and sensory effects on the contralateral side. It means, if the lesion is in the left internal capsule, motor and sensory deficits would occur on the right side of the body.
Stroke Risk factors
- High blood pressure
- Cigarette smoking
- High cholesterol
- Diabetes
- Age: People age 55 or older have a higher risk of stroke than younger people
- Sex: Men have a higher risk of stroke than women.
Stroke Complications
- Paralysis or loss of muscle movement may persist permanently
- Difficulty talking or swallowing may persist
- Memory loss or thinking difficulties.
- Emotional problems. The patient may develop depression.
- Pain.
- Bedsores
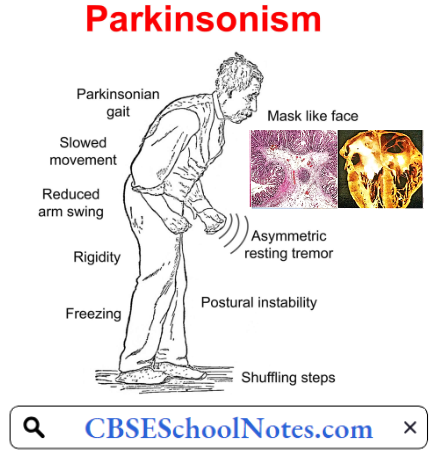
Parkinson’s Disease
Parkinson’s disease (PD) affects 1% of the population above 60 years of age. It is a long-term degenerative disorder of the central nervous system that mainly affects the motor system. PD usually begins around age 60, but it can start earlier. It is more common in men than in women.
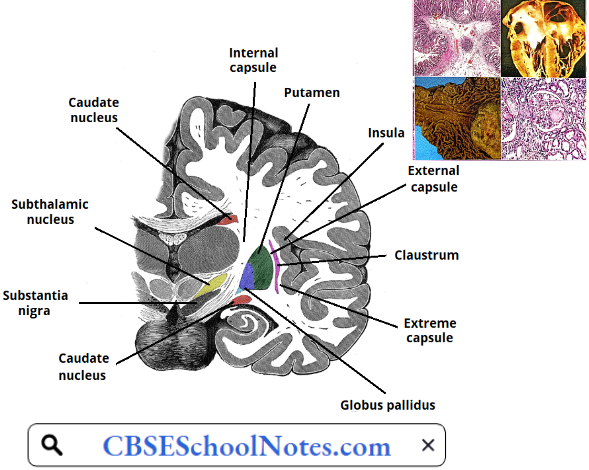
Parkinsons Disease Aetiology: PD is caused by degeneration of dopaminergic neurons in the substantia nigra, one of the basal ganglia. The cause of degeneration is not known.
Parkinson’s Disease Symptoms and Signs
1. Bradykinesia: This term is used to describe the inability to initiate movements. Poverty of movement is the most characteristic feature of Parkinson’s disease. The patient has a mask-like facial expression and an unblinking reptilian stare. There is absence of normal associated movements, for example, swinging of the arms during walking or change of facial expression related to the emotional content of the speech.
Even ordinary motor tasks are performed very slowly, taking much longer time than average normal. Bradykinesia /akinesia are not due to any paralysis. The sensory system is also normal. Still, there is great difficulty in initiating voluntary movements. Muscle power is not affected.
2. Lead Pipe Rigidity: Rigidity mostly involves the proximal muscles of the limbs. It affects both the protagonists and antagonists. During passive movement of a Jimb, the resistance is observed throughout the effort as if a lead pipe is being bent (i.e. there is no clasp-knife effect that is seen in patients with hemiplegia).
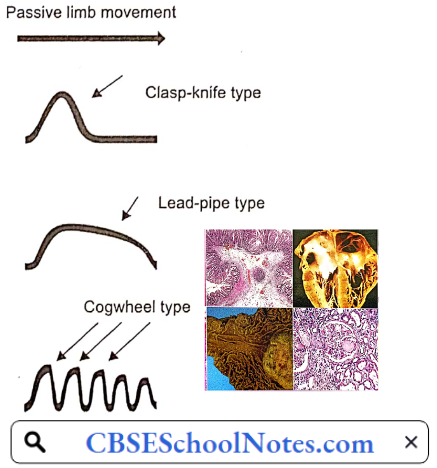
When the limbs of the person with PD are passively moved by the examiner, a “cogwheel rigidity” may be seen. Cogwheel-like rigidity is said to exist when a muscle is passively moved, it resists at first, but with enough force, it is partially moved until it resists again, and only with further force, will it be moved.
In advanced cases, the rigidity may increase to such an extent that the patient with arms adducted and flexed, knees flexed and the back bent has a statue-like appearance.
3. Tremor: Involuntary rhythmic oscillatory movements of the distal parts of the limb or tire head are called tremors. Tremors are produced by alternating contraction of tire protagonist and antagonist muscles.
It is a pronation-supination tremor that is described as ‘pill-rolling’, that is the index finger of the hand tends to get into contact with tire thumb, and they perform a circular movement together. Such a term was given due to the similarity of the movement in PD patients with the former pharmaceutical technique of manually making pills.
Parkinsonian tremor occurs at a frequency of 4-6 /s. Parkinsonian tremors are present at rest but disappear during sleep or voluntary activity, hence often called resting tremors. A patient showing severe tremors of the hand would hold a cup of tea and drink without difficulty. Parkinsonian tremors also disappear during sleep.
As mentioned above, Parkinson’s disease is due to degeneration of dopamine-producing neurons of the substantia nigra. As a result, there is a disturbance of the neural balance between the excitatory cholinergic and inhibitory dopaminergic activity of tire neostriatum.
4. Postural Disturbance: A forward-flexed posture
5. Postural Instability: In the late stages, postural instability is typical, which leads to impaired balance and frequent falls, that may lead to bone fractures.
6. Gait: Shuffling gait is characterized by short steps, with feet barely leaving the ground. Small obstacles tend to cause the patient to trip.
Parkinsons Disease Risk Factors: Risk factors for Parkinson’s disease include
- Age: Young adults rarely experience Parkinson’s disease. It ordinarily begins in middle or late life, and the risk increases with age. People usually develop the disease around age 60 or older.
- Heredity: Having a close relative with Parkinson’s disease increases the chances that you will develop the disease.
- Sex: Men are more likely to develop Parkinson’s disease than are women.
Parkinsons Disease Complications: Parkinson’s disease is often accompanied by these additional problems
- Dementia.
- Depression
- Swallowing problems
- Chewing and eating problems. Late-stage Parkinson’s disease affects the muscles in the mouth, making chewing difficult.
- Sleep disorders
- Bladder problems. Parkinson’s disease may cause bladder problems, including being unable to control urine or having difficulty urinating
- Constipation. Many people with Parkinson’s disease develop constipation.
Epilepsy
Epilepsy is a disorder of the brain characterized by repeated seizures. A seizure is defined as a sudden alteration of behavior due to a temporary change in the electrical functioning of the brain. Around 50 million people worldwide have epilepsy making it one of the most common neurological diseases globally.
Nearly 80% of people with epilepsy live in low- and middle-income countries. The prevalence in India is about 1% of the population.
Epilepsy Symptoms And Signs: Because epilepsy is caused by abnormal activity in the brain, seizures can affect any process your brain coordinates. Seizure signs and symptoms may include:
- Temporary confusion
- A staring spell
- Uncontrollable jerking movements of the arms and legs
- Loss of consciousness or awareness
- Psychic symptoms such as fear, anxiety
Epilepsy Pathogenesis: In epileptic seizures, a group of neurons begin firing in an abnormal, excessive, and synchronized manner, which can be detected by electroencephalography.
Epilepsy Causes: Epilepsy has no identifiable cause in about half the people with the condition. In the other half, the condition may be traced to various factors, including
- Genetic influence. Some types of epilepsy run in families. In these cases, it is likely that there is a genetic influence.
- Brain damage from prenatal or perinatal causes (for example, a loss of oxygen or trauma during birth, low birth weight);
- Congenital abnormalities or genetic conditions with associated brain malformations;
- A severe head injury;
- Stroke
- An infection of the brain such as meningitis, encephalitis
- A brain tumor.
Epilepsy Complications: Having a seizure at certain times can lead to circumstances that are dangerous to self or others.
- Falling leads to bone fractures
- Drowning while swimming
- Car accidents while driving
Psychiatric Disorders
Mental illness, also called mental health disorders, refers to a wide range of mental health conditions—disorders that affect your mood, thinking, and behavior. Examples of mental illness include depression, anxiety disorders, schizophrenia, dementia, etc. According to WHO, globally about 25% of the population suffers from some psychiatric disorder in their lifetime.
Psychiatric Disorders Depression: Depression is a common mental disorder and one of the main causes of disability worldwide. Globally, an estimated 264 million people are affected by depression. More women are affected than men.
- Depression is characterized by sadness, loss of interest or pleasure, feelings of guilt or low self-worth, disturbed sleep or appetite, tiredness, and poor concentration. People with depression may also have multiple physical complaints with no apparent physical cause.
- Depression can be long-lasting or recurrent, substantially impairing people’s ability to function at work or school and to cope with daily life. At its most severe, depression can lead to suicide.
Psychiatric Disorders Symptoms
- Feelings of sadness, tearfulness, emptiness, or hopelessness.
- Angry outbursts, irritability, or frustration.
- Loss of interest or pleasure in most or all normal activities, such as sex, hobbies, or sports.
- Sleep disturbances, including insomnia or sleeping too much.
- Tiredness and lack of energy, so even small tasks take extra effort.
- Reduced appetite and weight loss or increased cravings for food and weight gain.
- Anxiety, agitation, or restlessness.
- Slowed thinking, speaking, or body movements.
- Feelings of worthlessness or guilt, fixating on past failures or self-blame.
- Trouble thinking, concentrating, making decisions, and remembering things.
- Frequent or recurrent thoughts of death, suicidal thoughts, suicide attempts, or suicide.
- Unexplained physical problems, such as back pain or headaches.
Psychiatric Disorders Causes: It is not known exactly what causes depression. As with many mental disorders, a variety of factors may be involved, such as:
- Biological Differences: People with depression appear to have physical changes in their brains.
- Brain Chemistry: Neurotransmitters are naturally occurring brain chemicals that likely play a role in depression. A deficiency of a neurotransmitter may lead to depression. Treatment consists of increasing concentrations of certain neurotransmitters in the brain.
- Hormones: Changes in the body’s balance of hormones may be involved in causing or triggering depression. Hormone changes can result with pregnancy and during the weeks or months after delivery (postpartum) and from thyroid problems, menopause, or a number of other conditions.
- Inherited Traits: Depression is more common in people whose blood relatives also have this condition. Researchers are trying to find genes that may be involved in causing depression.
Psychiatric Disorders Complications: Examples of complications associated with depression include
- Excess weight or obesity, which can lead to heart disease and diabetes
- Family conflicts, relationship difficulties, and work or school problems
- Social isolation
- Suicidal feelings, suicide attempts, or suicide.
Schizophrenia: Schizophrenia is a severe mental disorder, affecting 20 million people worldwide. Symptoms of schizophrenia include
- Hallucinations—hearing or seeing things that do not exist outside of the mind
- Delusions—unusual beliefs not based on reality
- Muddled thoughts based on hallucinations or delusions
- Losing interest in everyday activities
- Not caring about your personal hygiene
- Wanting to avoid people, including friends
Schizophrenia Causes
- Genetics: One of the most significant risk factors for schizophrenia may be genes. This disorder tends to run in families. A person is likely to suffer from schizophrenia if a parent, sibling, or other close relative has suffered from this condition. Other factors, such as stressors, may be needed to “trigger” (listed below) the disorder in people who are at a higher risk.
- Brain Development: Studies of people with schizophrenia have shown there are subtle differences in the structure of their brains. These changes are not seen in everyone with schizophrenia and can occur in people who do not have a mental illness. However, they suggest schizophrenia may partly be a disorder of the brain.
- Chemical Changes In The Brain: There is a connection between neurotransmitters and schizophrenia because drugs that alter the levels of neurotransmitters in the brain are known to relieve some of the symptoms of schizophrenia. Research suggests schizophrenia may be caused by a change in the level of 2 neuro¬transmitters: Dopamine and serotonin. Some studies indicate an imbalance between the 2 may be the basis of the problem.
- Stress: The main psychological triggers of schizophrenia are stressful life events, such as:
- Bereavement
- Losing job
- Divorce
- Physical, sexual, or emotional abuse
These kinds of experiences, although stressful, do not cause schizophrenia. However, they can trigger its development in someone already vulnerable to it.
Schizophrenia Complications: Schizophrenia can be a dangerous disease if it is not treated properly. It can cause complications in many areas of life. Physical problems can occur if the symptoms of schizophrenia are not well controlled.
People with schizophrenia are at higher risk for complications such as depression or suicide. They may engage in self-destructive behaviors. People with schizophrenia may get involved in violent crime, either as the victim or as the person committing the crime.
Dementia: Worldwide, approximately 50 million people have dementia. Dementia is usually of a chronic or progressive nature in which there is deterioration in cognitive function (i.e. the ability to process thought) beyond what might be expected from normal aging.
- It affects memory, thinking, orientation, comprehension, calculation, learning capacity, language, and judgment. The impairment in cognitive function is commonly accompanied, and occasionally preceded, by deterioration in emotional control, social behavior, or motivation.
- In the later stages of dementia, the patient becomes totally dependent on relatives for all the daily tasks. Dementia is caused by a variety of diseases and injuries that affect the brain, such as Alzheimer’s disease or stroke.
Dementia Symptoms: Dementia symptoms vary depending on the cause, but common signs and symptoms include
- Cognitive Changes
- Memory loss, which is usually noticed by a spouse or someone else
- Difficulty communicating or finding words
- Difficulty with visual and spatial abilities, such as getting lost while driving
- Difficulty reasoning or problem-solving
- Difficulty with planning and organizing
- Difficulty with coordination and motor functions
- Confusion and disorientation
- Psychological Changes
- Personality changes
- Paranoia
- Depression
- Agitation
- Anxiety
- Hallucinations
- Inappropriate behavior
Dementia Causes: Alzheimer’s disease accounts for 60 to 80 percent of cases of dementia. Vascular dementia is the second most common cause of dementia.
- Dementia is often incorrectly referred to as “senility” or “senile dementia,” which reflects the formerly widespread but incorrect belief that serious mental decline is a normal part of aging.
- The two types of dementia are associated with particular types of brain cell damage in particular regions of the brain. For example, in Alzheimer’s disease, the brain cells of the brain region called the hippocampus are first to be damaged.
- The hippocampus region is the center of learning and memory in the brain, That is why memory loss is often one of the earliest symptoms of Alzheimer’s disease.
Risk Factors for Alzheimer’s Dementia
- Age: Advancing age is the greatest risk factor for developing Alzheimer’s disease. The majority of people diagnosed with Alzheimer’s disease are 65 or older. Although far less common, younger-onset Alzheimer’s (also known as early-onset Alzheimer’s) affects people younger than 65.
- Family Members With Alzheimer’s: A person is more likely to suffer from Alzheimer’s disease if a parent or sibling suffers from the disease.
- Genetics: Genes are estimated to play a role in as many as one-quarter of Alzheimer’s cases.
- Cardiovascular Disease: Factors that cause cardiovascular disease also may be linked to a higher risk of developing Alzheimer’s and other dementias. Such factors include smoking, obesity, diabetes, high cholesterol, and high blood pressure in midlife.
- Education And Alzheimer’s: Studies have linked fewer years of formal education with an increased risk of Alzheimer’s and other dementias.
- Traumatic Brain Injury: The risk of Alzheimer’s disease and other dementias increases after a moderate or severe traumatic brain injury, such as a blow to the head or injury of the skull that causes amnesia or loss of consciousness for more than 30 minutes.
Vascular Dementia: Vascular dementia is the second most common cause of dementia, after Alzheimer’s. Common conditions that may lead to vascular dementia include
- Stroke: Strokes that block a brain artery usually cause a range of symptoms that may include vascular dementia. But some strokes don’t cause any noticeable symptoms. These silent strokes still increase dementia risk. With both silent and apparent strokes, the risk of vascular dementia increases with the number of strokes that occur over time.
- Narrowed Or Chronically Damaged Brain Blood Vessels: Conditions that narrow or inflict long-term damage on your brain blood vessels also can lead to vascular dementia.
Symptoms of vascular dementia are similar to Alzheimer’s disease, although memory loss may not be as apparent in the early stages. Symptoms can sometimes develop suddenly and quickly get worse, but they can also develop gradually over many months or years.
Specific Symptoms Can Include:
- Stroke-like Symptoms: Including muscle weakness or temporary paralysis on one side of the body.
- Movement Problems: Difficulty walking or a change in the way a person walks
Dementia Risk Factors: In general, the risk factors for vascular dementia are the same as those for heart disease and stroke.
- Increasing age. Your risk of vascular dementia rises as you grow older. The disorder is rare before age 65, and the risk rises substantially by the 90s.
- History of heart attack, strokes or ministrokes
- Atherosclerosis
- Diabetes
- High cholesterol
- Smoking
- High blood pressure
- Obesity
Infectious Disease: Types, Causes & Treatments
Infectious Diseases
Over the previous centuries, global pandemics of infectious diseases, such as smallpox, cholera, and influenza, periodically threatened the survival of entire populations. By the mid-twentieth century, safe, effective, and affordable vaccines and the increasing availability of antibiotics had further reduced the toll of infectious diseases in high-income countries.
Not until the second half of the twentieth century did large-scale efforts begin to better control infectious diseases in low- and middle-income countries, where the infectious disease burden was greatest and highly varied. A survey in 1998 revealed that infectious diseases accounted for about 50% of the disease burden in India. Not much has changed in 2020.
Read and Learn More Pathophysiology
Meningitis: Bacterial meningitis is the most common and serious bacterial infection of the central nervous system (CNS), characterized by an acute purulent infection of the meninges around the brain and spinal cord (pia mater, arachnoid) and subarachnoid space.
Without prompt antibiotic treatment, bacterial meningitis is serious and can be fatal within days. Delayed treatment increases the risk of permanent brain damage or death Approximately 1.2 million cases are estimated to suffer from bacterial meningitis annually worldwide, resulting in 135,000 deaths.
The Meninges: The meninges comprise three membranes that, together with the cerebrospinal fluid, enclose and protect the brain and spinal cord. The pia mater is a very delicate impermeable membrane that firmly adheres to the surface of the brain. The arachnoid mater is a loosely fitting sac on top of the pia mater.
The subarachnoid space separates the arachnoid and pia mater membranes and is filled with cerebrospinal fluid. The outermost membrane, the dura mater, is a thick durable membrane, which is attached to both the arachnoid membrane and the skull.
Meningitis Symptoms And Signs: Early meningitis symptoms may mimic upper respiratory tract infection. Symptoms may develop over several hours or over a few days. Possible signs and symptoms in anyone older than the age of 2 include
- Sudden high fever
- Stiff neck
- Severe headache
- Headache with nausea or vomiting
- Confusion or difficulty concentrating
- Seizures
- Sleepiness or difficulty waking
- Photophobia (sensitivity to light)
- No appetite or thirst
- Skin rash (sometimes, such as in meningococcal meningitis).
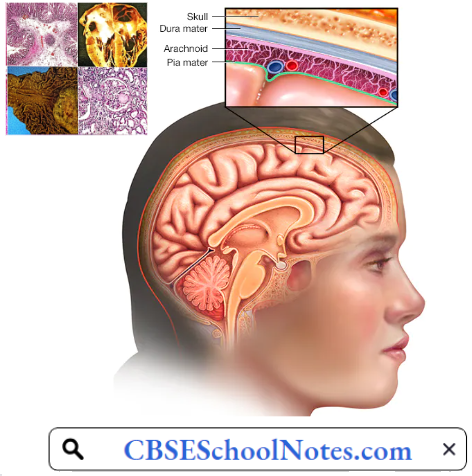
Meningitis Causes
- Bacterial Meningitis: Bacteria that enter the bloodstream and travel to the brain and spinal cord cause acute bacterial meningitis. Pneumococcus or meningococcus type of bacteria are causative organism.
- Viral Meningitis: The symptoms of viral meningitis are the same as in bacterial meningitis, but milder. Viral meningitis often clears on its own. In most cases, there is no specific treatment for viral meningitis. Most people who get mild viral meningitis usually recover completely in 7 to 10 days without treatment.
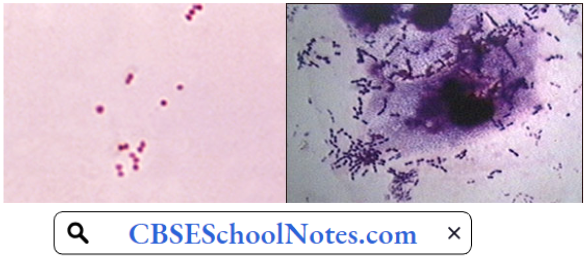
Since bacterial meningitis is a serious disorder, it is important to differentiate from viral meningitis. One of the tests for this differentiation is the physical appearance, chemical analysis, and microscopic examination of cerebrospinal fluid (CSF) obtained by lumbar puncture in the patient.
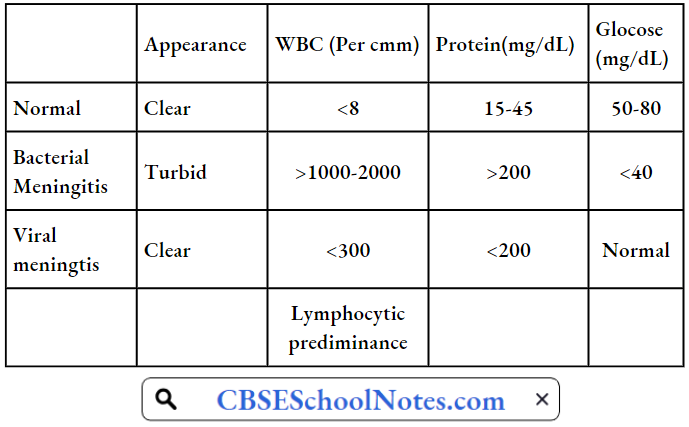

- The CSF in bacterial meningitis is characterized by being turbid in appearance, decreased glucose concentration, increased protein concentration, and a large number of white blood cells, chiefly neutrophils.
- The CSF in viral meningitis is clear in appearance, with normal sugar concentration, only a mild increase in protein concentration, and a lesser number of white blood cells, chiefly lymphocytes.
Physical Appearance And Chemical Composition Of Csf In Bacterial And Viral Meningitis: In most cases, the disorder starts with a viral upper respiratory infection which breaks down the protective barrier provided by the mucous membrane of the nasal cavity.
- As a result, bacteria that normally reside on the nasal mucous membrane are able to enter the bloodstream. Once bacteria have entered the bloodstream, they enter the subarachnoid space in places where the blood-brain barrier is relatively weak, i.e. the choroid plexus.
- The cerebrospinal fluid present in the subarachnoid space is an ideal medium for the proliferation of bacteria because it has enough nutrients and very few phagocytic cells.
- Cells of the innate immune system of CNS (microglia and astrocytes) located in the choroid plexus and ependyma, detect bacteria and secrete cytokines and chemokines which attract circulating granulocytes into CSF.
- Granulocytes and macrophages contain powerful lysosomal enzymes used to kill the bacteria, but these cells have short lifespans. On senescence, these cells release proteolytic enzymes into cerebral interstitial space and damage the brain tissue and blood vessels (vasculitis).
- So the brain damage in bacterial meningitis is partly due to bacteria and partly by inflammatory response. The most dangerous complication of bacterial meningitis is increased intracranial pressure from cerebral edema.
- Cerebral edema results from greater permeability of the blood-brain barrier, increased cerebral hypoxia, and cellular toxicity. Increased intracranial pressure, in turn, causes decreased cerebral perfusion, ischemia, hypoxia, and neuronal necrosis.

Meningitis Complications: Meningitis complications can be severe. The longer the delay in the start of treatment, the greater is the brain damage and other complications, including
- Hearing loss.
- Ataxia.
- Cortical blindness.
- Mental retardation.
- Other cranial nerve dysfunction.
- Kidney failure
- Paralysis.
- Death.
- Muscular hypertonia.
Typhoid Fever: Typhoid, also called typhoid fever, occurs all over the world. In 2015, 12.5 million new cases worldwide were reported. The risk of death may be as high as 20% without treatment. In 2015, it resulted in about 149,000 deaths worldwide. The disease is endemic in India, Southeast Asia, Africa, and South America.
Typhoid Fever Symptoms And Signs
- In the first week, the body temperature rises slowly, and fever fluctuations are seen with malaise, headache, and cough.
- In the second week, high fever around 40°C (104°F). The abdomen is distended and painful in the right lower quadrant. The spleen and liver are enlarged (hepatosplenomegaly).
- In the third week of typhoid fever, a number of complications can occur
- Intestinal hemorrhage due to bleeding in congested Peyer’s patches;
- Intestinal perforation in the distal ileum is a very serious complication and is frequently fatal.
- Septicaemia or peritonitis.
Typhoid Fever Cause: Typhoid fever is caused by a virulent bacteria called Salmonella typhi. The bacteria that cause typhoid fever spread through contaminated food or water. The patient or the carrier passes bacteria in the feces.
You can contract the infection if you eat food handled by someone with typhoid fever who hasn’t washed his hands carefully after using the toilet. You can also become infected by drinking water contaminated with the bacteria.

Typhoid Fever Pathogenesis: Salmonella organisms penetrate the mucosa of the small intestine and proliferate in the mucosal epithelial cells. Next, the bacteria proliferate in the Payer’s patches (submucosal collection of lymphoid tissue) of the lower small intestine from where systemic dissemination occurs to the reticuloendothelial system of the liver and spleen.
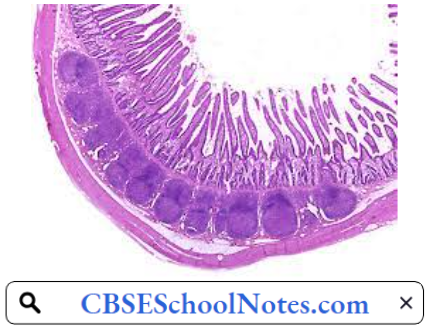
For a period varying from 1 to 3 weeks, the organism multiplies within these organs. Invasion of the mucosa causes the epithelial cells to synthesize and release various proinflammatory cytokines responsible for most of the symptoms of typhoid fever.

Ulceration over Payer’s patches accounts for complications such as bleeding, perforation, and peritonitis. Proliferation in the reticuloendothelial system leads to enlargement and congestion of the spleen and liver.
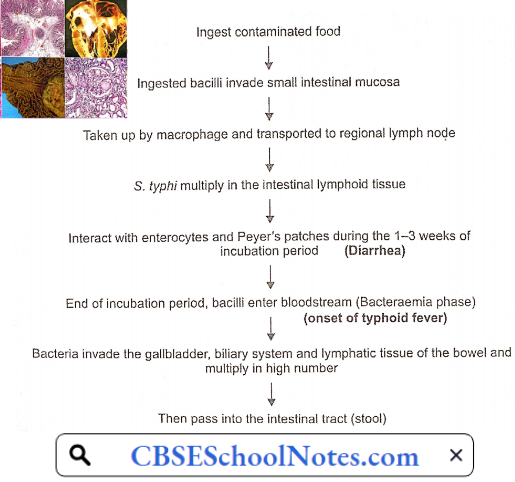
Typhoid Fever Complications
- Intestinal hemorrhage
- Intestinal perforation
- Septicaemia
Tuberculosis: In 2018, an estimated 10 million people fell ill with tuberculosis (TB) worldwide. A total of 1.5 million people died from TB in 2018. Worldwide, TB is one of the top 10 causes of death and the leading cause from a single infectious agent.
Tuberculosis generally affects the lungs, but can also affect other parts of the body. About 25T of TB patients of the world are Indians. In India, each year, approx. 220,000 deaths are reported due to tuberculosis.
Pulmonary Tuberculosis: Tuberculosis Symptoms And Signs
- Cough up sputum
- Cough up blood
- Consistent low-grade fever
- Night sweats
- Chest pains
- Unexplained weight loss
Tuberculosis Cause: Pulmonary TB is caused by the bacterium Mycobacterium tuberculosis. TB is contagious. This means the bacteria is easily spread from an infected person to someone else. You can get TB by breathing in air droplets from a cough or sneeze of an infected person. The resulting lung infection is called primary TB.
Tuberculosis Pathogenesis: The characteristic pathologic changes depend on the type of infection
- Primary Pulmonary TB (primary exposure) is characterized by the Ghon complex which consists of
- Subpleural focus of tubercular inflammation.
- Infected (inflamed) lymph nodes draining the primary subpleural lesion.
- Secondary Pulmonary TB (reactivation) is characterized by a focus of infection and granuloma formation usually in the apex of the lung. The small granulomas (tubercles) eventually coalesce to form larger areas of consolidation with central caseating necrosis. Regional lymph nodes contain caseating granulomas.
- Progressive Pulmonary TB: Primary or secondary TB may go on to heal as caseating granulomas are replaced by fibrosis and calcification. However, if the case does not heal spontaneously or with therapy, the disease progresses to form cavities or spread to other parts of the lung and other organs of the body through lymphatic channels and the bloodstream.
Primary Tuberculosis: The tubercle bacilli establish infection in the lungs after they are carried in droplets small enough (5 to 10 microns) to reach the alveolar spaces. If the defense system of the host fails to eliminate the infection, the bacilli proliferate inside alveolar macrophages and eventually kill the cells.
The infected macrophages produce cytokines and chemokines that attract other phagocytic cells, including monocytes, other alveolar macrophages, and neutrophils, which eventually form a nodular granulomatous structure called the tubercle.
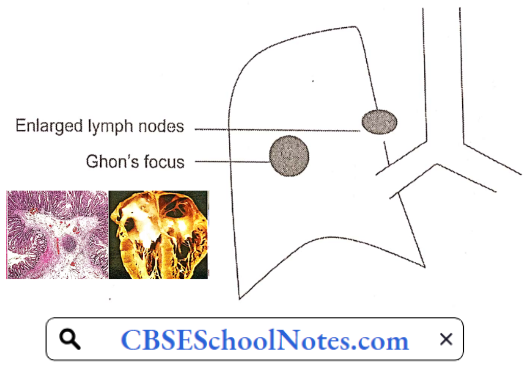
If the bacterial replication is not controlled, the tubercle enlarges and the bacilli enter local draining lymph nodes. This leads to lymphadenopathy, a characteristic clinical manifestation of primary tuberculosis. The lesion produced by the expansion of the tubercle into the lung parenchyma and lymph node involvement is called the Ghon complex.
Unchecked bacterial growth may lead to hematogenous spread of bacilli to produce disseminated TB in various vital organs of the body. Disseminated disease with lesions resembling millet seeds is termed miliary TB. In the absence of treatment, death ensues in 80% of cases.
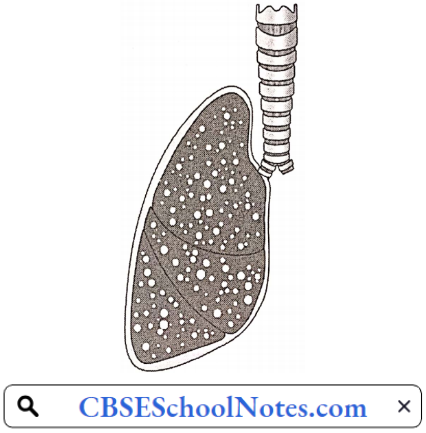
The remaining patients develop chronic disease or recover. Chronic disease is characterized by repeated episodes of healing by fibrotic changes around the lesions and tissue breakdown. Complete spontaneous eradication of the bacilli is rare.
Tuberculosis Reactivation Disease: Reactivation TB results from the proliferation of a previously dormant bacterium seeded at the time of the primary infection. Among individuals with latent infection and no underlying medical problems, reactivation disease occurs in 5 to 10 percent.
It is not clear what specific host factors maintain the infection in a latent state and what triggers the latent infection to become overt. The disease process in reactivation TB tends to be localized (in contrast to primary disease): There is little regional lymph node involvement and less caseation.
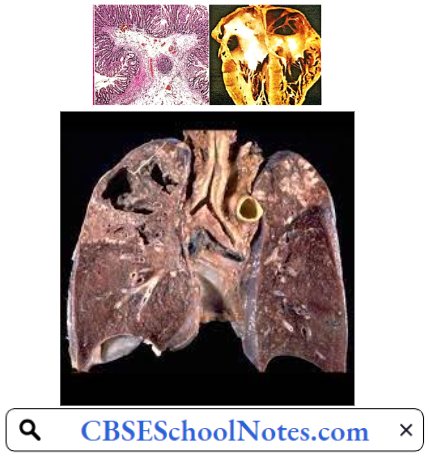
The lesion typically occurs at the lung apices, and disseminated disease is unusual unless the host is severely immunosuppressed. It is generally believed that successfully contained latent TB confers protection against subsequent TB exposure.
In many people, the infection waxes and wanes. Tissue destruction and necrosis are often balanced by healing and fibrosis. Affected tissue is replaced by scarring and cavities filled with caseous necrotic material. Tissue destruction and necrosis are often balanced by healing and fibrosis.
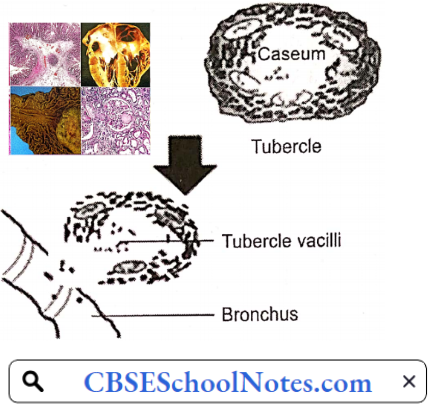
Affected tissue is replaced by scarring and cavities filled with caseous necrotic material. During active disease, some of these cavities are joined to the bronchi and this material can be coughed up. The sputum contains living bacteria and thus can spread the infection.
Tuberculosis Risk factors
- Contact with a patient of TB
- Live in crowded or unclean living conditions
- Have poor nutrition
Tuberculosis Complications
- Hemoptysis
- Pleurisy
- Pleural effusion
- Empyema
- Pneumothorax
Leprosy: Leprosy currently affects approximately a quarter of a million people throughout the world, with the majority of these cases being reported from India. India is currently running one of the largest leprosy eradication programs in the world.
- Despite this, 120,000 to 130,000 new cases of leprosy are reported every year in India. This is 58.8% of the global total of new cases. Leprosy colonies exist throughout India. These are typically made up of patients that have moved to the colony often from a significant distance away, along with their children and grandchildren. Leprosy is a curable disease.
- Leprosy, also known as Hansen’s disease, is a chronic infectious disease caused by Mycobacterium leprae. The disease mainly affects the skin, the peripheral nerves, mucosal surfaces of the upper respiratory tract, and the eyes. Leprosy is known to occur at all ages ranging from early infancy to very old age. Leprosy is curable and early treatment averts most disabilities.
Leprosy Transmission: The exact mechanism of transmission of leprosy is not known. At least until recently, the most widely held belief was that the disease was transmitted by contact between cases of leprosy and healthy persons. More recently the possibility of transmission by the respiratory route is gaining ground.
Leprosy Symptoms And Signs: The skin lesion is a characteristic feature of leprosy. The skin lesion can be single or multiple, usually less pigmented than the surrounding normal skin. Sometimes the lesion is reddish or copper-colored.
A variety of skin lesions may be seen but macules (flat), papules (raised), or nodules are common. Sensory loss is a typical feature of leprosy. The skin lesion may show loss of sensation to pin pick and/ or light touch. Thickened nerves, mainly peripheral nerve trunks, constitute another feature of leprosy.

A thickened nerve is often accompanied by other signs as a result of damage to the nerve. These may be loss of sensation in the skin and weakness of muscles supplied by the affected nerve.
Leprosy Pathogenesis: Leprosy bacilli multiply in macrophages in the skin and Schwann cells of the nerves. Two forms of leprosy are known
- One form is “the tuberculoid type which is a mild form. M. leprae multiplies at the site of entry, usually the skin, invading and colonizing Schwann cells. The microbe then induces T-helper lymphocytes, epithelioid cells, and giant cell infiltration of the skin, causing infected individuals to exhibit large flattened patches with raised and elevated red edges on their skin.
- These patches have dry, pale, hairless centers, accompanied by a loss of sensation on the skin, The loss of sensation may develop as a result of invasion of the peripheral sensory nerves.
- The second form of leprosy, the “lepromatous type”, causes serious disfigurement is more virulent, In this form, the microbes proliferate within the macrophages as well as within the epithelial tissues of the face and ear lobes. Extension penetration of this microbe may lead to severe body damage; for example, the loss of bones, fingers, anel toes, and nose.
Leprosy Risk Factor: Prolonged contact with a patient of leprosy.
Leprosy Complications
- The most severe complications result from peripheral neuropathy, which causes deterioration of the sense of touch and a corresponding inability to feel pain and temperature.
- Patients may unknowingly burn, cut, or otherwise harm themselves. Repealed damage may lead to a Kiss of digits.
- Muscle weakness can result in deformities (for example, clawing of the 4th and 5th fingers caused by ulnar nerve involvement, fool drop caused by peroneal nerve involvement).
- Papules and nodules can be particularly disfiguring on the face.
- Feet: Plantar ulcers with secondary infection are a major cause of morbidity, making walking painful.
- Nose: Damage to the nasal mucosa can result in chronic nasal congestion and nosebleeds and, if untreated, erosion and collapse of the nasal septum.
- Eyes: Iritis may lead to glaucoma, and corneal insensitivity may lead to scarring and blindness.
- Sexual Function: Men with lepromatous leprosy may have erectile dysfunction and infertility. The infection can reduce testosterone and sperm production by the testes.
- Kidneys: Amyloidosis and consequent renal failure occasionally occur in lepro- malous leprosy.
Urinary Tract Infection: Urinary tract infections (UTls) are some of the most common bacterial infections, affecting 150 million people each year worldwide. About 40% of women and 12% of men experience at least one symptomatic UT1 during their lifetime, and as many as 40% of affected women show recurrent UTI.
- A urinary tract infection (UTI) is an infection in any part of the urinary system—kidneys, ureters, bladder, and urethra. Most infections involve the lower urinary tract—the bladder and the urethra. Women are at greater risk of developing a UT1 than are men, since they have very short urethra.
- Urinary tract infections (UTIs) are the most common outpatient infections, with a lifetime incidence of 50-60% in adult women. Serious consequences can occur if a UTI spreads to the kidneys.
Urinary Symptoms And Signs: Each type of UTI may result in more specific signs and symptoms, depending on which part of your urinary tract is infected.
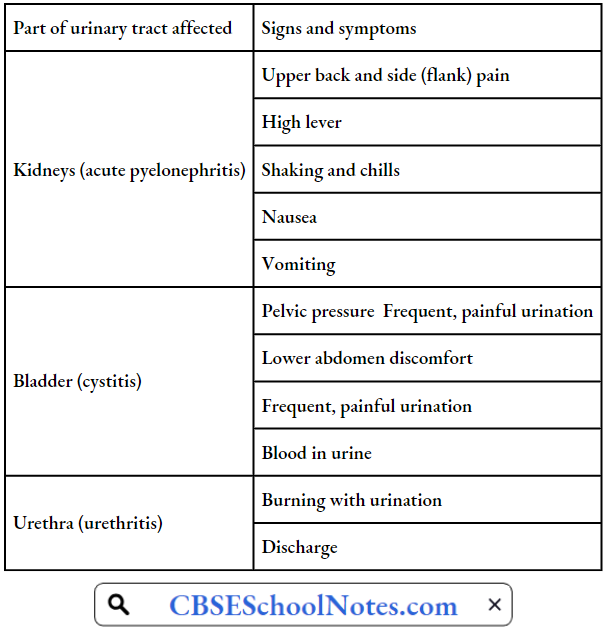
Microscopic examination of urine reveals a large number of white blood cells. Microbiological culture helps to identify the causative organism as well as its sensitivity to drugs.
Urinary Tract Infection Causes: Urinary tract infections typically occur when bacteria enter the urinary tract through the urethra and begin to multiply in the bladder. Although the urinary system is designed to keep out such microscopic invaders, these defences sometimes fail.
When that happens, bacteria may take hold and grow into a full-blown infection in the urinary tract. The most common UTIs occur mainly in women and affect the urinary bladder and urethra. Escherichia coli (E. coli) from the gut is the cause of 80-85% of community-acquired urinary tract infections.
Urinary Tract Infection Risk Factors: Risk factors specific to women for UTIs include
- Female Anatomy: A woman has a shorter urethra than a man does, which shortens the distance that bacteria must travel to reach the bladder.
- Sexual Activity.
- Menopause: After menopause, a decline in circulating estrogen causes changes in the urinary tract that make women more vulnerable to infection.
- Urinary tract abnormalities.
- Blockages in the urinary tract. Urinary obstruction by kidney stones or an enlarged prostate in males increases the risk of UTIs.
- Diabetes
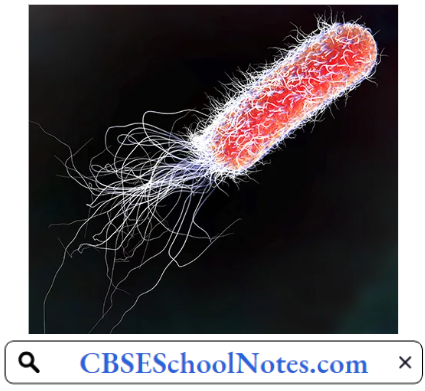
Urinary Tract Infection Complications: When treated promptly and properly lower urinary tract infections rarely lead to complications. But left untreated, a urinary tract infection can have serious consequences
- Recurrent infections, especially in women.
- Permanent kidney damage from an acute or chronic kidney infection (pyelonephritis) due to an untreated UTI.
- Sepsis, a potentially life-threatening complication of an infection, especially if the infection spreads to the kidneys.
Gonorrhea: Gonorrhea, is a sexually transmitted infection (STI). It is a global problem. The World Health Organization estimates that 62 million people are infected annually worldwide. In the United States, it is the second most commonly reported communicable disease and the second most prevalent sexually transmitted infection. In India, its exact prevalence is not known because of non-reporting by the patients.
Gonorrhea Symptoms And Signs: In many cases, gonorrhea infection causes no symptoms. Symptoms, however, can affect many sites in the body, but commonly appear in the genital tract.
- Signs And Symptoms Of Gonorrhoea Infection In Men Include:
- Painful urination
- Pus-like discharge from the tip of the penis
- Pain or swelling in one testicle
- Signs And Symptoms Of Gonorrhea Infection In Women Include:
- Increased vaginal discharge
- Painful urination
- Vaginal bleeding between periods, such as after vaginal intercourse
- Abdominal or pelvic pain
- Gonorrhea Can Also Affect These Parts Of The Body:
- Rectum: Signs and symptoms include anal itching, pus-like discharge from the rectum.
- Eyes: Gonorrhea that affects the eyes can cause eye pain and pus-like discharge from the eye.
- Throat: Signs and symptoms of a throat infection might include a sore throat and swollen lymph nodes in the neck.
- Joints: If one or more joints become infected by bacteria (septic arthritis), the affected joints might be warm, red, swollen, and extremely painful, especially during movement.
Gonorrhea Cause: Gonorrhoea, is caused by the bacterium Neisseria gonorrhoeae.

Gonorrhea Pathogenesis: Transmission of infection from one person to another normally occurs during periods of close physical contact which allow the organisms to pass from the site of infection in one host, to a susceptible mucosal surface in a new one.
- The infection is usually transmitted during intimate sexual contact, the most common site of infection being the mucosa of the genital tract. In addition, babies born to mothers harboring gonococci in their genital tract may become infected during passage down the birth canal and may develop gonococcal conjunctivitis.
- Neisseria gonorrhoeae is an obligate human pathogen that causes mucosal surface infections of male and female reproductive tracts, pharynx, rectum, and conjunctiva. Asymptomatic infections in the lower reproductive tract of women can lead to serious, long-term consequences if these infections ascend into the fallopian tube.
- The damage caused by gonococcal infection and the subsequent inflammatory response produce the condition known as pelvic inflammatory disease (PID). Infection can lead to tubal scarring, occlusion of the oviduct, and loss of critical ciliated cells.
- These defects interfere with the normal transport of the ovum from the ovary to the uterus. Consequently, there is an increased risk of ectopic pregnancy and infertility.
Gonorrhea Complications: Untreated gonorrhea can lead to major complications, such as
- Infertility in women.
- Infertility in men.
- Infection that spreads to tire joints and other areas of your body.
- Increased risk of HIV / AIDS.
- Complications in babies. Babies who contract gonorrhea from their mothers during birth can develop blindness.
Syphilis: Syphilis is a bacterial infection usually spread by sexual contact. The disease starts as a painless sore—typically on your genitals. Syphilis is caused by a bacterium called Treponema pallidum. Syphilis spreads from person to person via skin or mucous membranes. During the last 50 years, the prevalence of this disease seems to have decreased.
After the initial infection, the syphilis bacteria can remain inactive (dormant) in the body for decades before becoming active again. Early syphilis can be cured, sometimes with a single shot of penicillin. Without treatment, syphilis can severely damage the heart, brain, or other organs, and can be life-threatening. Syphilis can also be passed from mothers to unborn children.
Syphilis Symptoms And Signs
- Primary Syphilis: The first sign of syphilis is a small sore, called a chancre. The sore appears at the spot where the bacteria entered the body. The chancre usually develops about three weeks after exposure. Many people who have syphilis do not notice the chancre because it is usually painless. The chancre will heal on its own within three to six weeks.
- Secondary Syphilis: Within a few weeks of the original chancre healing, the patient experiences a rash that begins on the trunk but eventually covers the entire body. Some people also experience fever, a sore throat, and swollen lymph nodes. These signs and symptoms may disappear within a few weeks.
- Latent Syphilis: In this stage, there are no symptoms and it lasts for many years.
- Tertiary Syphilis: About 15% to 30% of people infected with syphilis who do not get treatment will develop complications known as late (tertiary) syphilis Tertiary Syphilis is the most serious stage of infection and is characterized by three major complications:
- Gummatous Syphilis causes the formation of soft, tumor-like lesions called gummas. These non-cancerous lesions can cause large ulcerative sores on the skin and mouth, and erode tissues of the heart, liver, muscles, bones, and other vital organs. Symptoms typically develop between three and 10 years after being infected.
- Cardiovascular syphilis can cause severe inflammation of the aorta and the development of an aortic aneurysm (the swelling and weakening of the aortic wall). It generally occurs 10 to 30 years after the initial infection.
- Neurosyphilis affects the central nervous system and usually develops within four to 25 years of an infection. There may be severe neurological disorders including meningitis, degeneration of the spinal cord (tabes dorsalis), seizures, personality changes, hallucinations, dementia, schizophrenia, and stroke.
While the syphilis infection can be treated during the tertiary stage, any damage caused to the heart, kidneys, and other organs may be permanent and lead to end-stage organ failure.
HIV/AIDS: Acquired immunodeficiency syndrome (AIDS) is a chronic potentially life-threatening condition caused by human immunodeficiency virus (HIV).
- The World Health Organization (WHO) estimates that in 2017, about 37 million people, including 1.8 million children (< 15 years), were living with HIV worldwide; of the total, about 25.7 million live in sub-Saharan Africa.
- More than two million Indians are suffering from HIV/AIDS. By damaging one’s immune system, it interferes with the body’s ability to various organs that cause disease.
HIV/AIDS: Symptoms And Signs: Symptoms and signs vary with the stage of the disease
- Primary Infection (acute HIV)
- Fever
- Headache
- Muscle aches
- Joint pains
- Rash
- Swollen lymph nodes in the neck
- Clinically Latent Infection (Chronic HIV): There are no symptoms or signs in this stage. This stage may last 10 years.
- Symptomatic HIV Infection
- Fever
- Weight loss
- Fatigue
- Diarrhea
- Swollen lymph nodes
Progression To AIDS: This stage occurs when the patient’s immune system has been severely damaged. Pathogens that normally cannot attack the human body are now able to enter the body and produce disease.
Such bacteria, viruses, and fungi are called opportunistic pathogens. The body loses the ability to detect and destroy malignant cells. Therefore, the patient is more prone to develop cancer. At this stage, symptoms and signs may include
- Night sweats
- Persistent fatigue
- Recurring fever
- Weight loss
- Chronic diarrhea
HIV/AIDS Pathogenesis: The human immunodeficiency virus (HIV) mainly infects the CD4 cells (helper T-cells) in the immune system. Over years of HIV infection, CD4 cell numbers usually drop gradually, but constantly, and the immune system is weakened. When the CD4 cell number falls below 200 mm3, symptoms of AIDS develop. At this stage complications listed below begin to appear. Due to opportunistic infections/tumors, severe muscle wasting can be observed in the patient.
HIV/AIDS Spread: HIV infection is transmitted by sexual intercourse. One can also get HIV infection by coming in contact with infected blood directly or through transfusion of infected blood or the use of contaminated syringes.
Complications Of AIDS
- Viral Infections, such as Cytomegalovirus (CMV), herpes simplex, molluscum, contagious, herpes zoster, human papillomavirus (HPV), etc
- Bacterial Infections, such as recurrent bacterial pneumonia, Mycobacterium tuberculosis, Pseudomonas, septicemia vasculitis, etc.
- Fungal Infections, such as Candida, Pneumocystis jirovecii, pneumonia, Cryptococcus neoformans
- Protozoal Infections
- Tumors, such as Kaposi’s sarcoma, primary cerebral lymphoma, high-grade non-Hodgkin lymphoma, carcinoma of the cervix, etc.
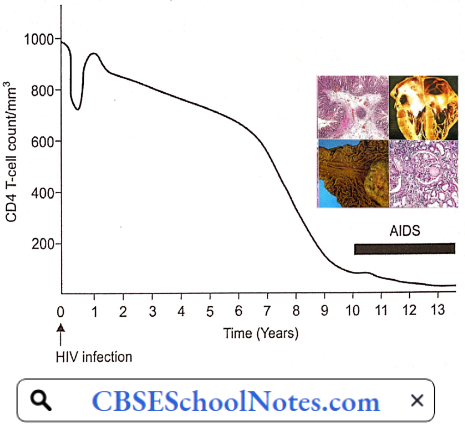
HIV/AIDS Risk Factors
- Unprotected sex with a person with HIV / AIDS
- Infected blood transfusion
- Sharing injection needles with a person with HIV/AIDS
Gastrointestinal Diseases & Disorders
Disorders Of the Gastrointestinal System
Peptic Ulcer
Peptic ulcer disease presents as a duodenal ulcer or gastric ulcer. During the last few decades, the incidence of peptic ulcer disease has decreased in India. In one study, the prevalence of duodenal ulcers was 12% in 1988, but it declined to 3 % in 2008. During the same period, gastric ulcer prevalence declined from 4.5% to 2.7%.
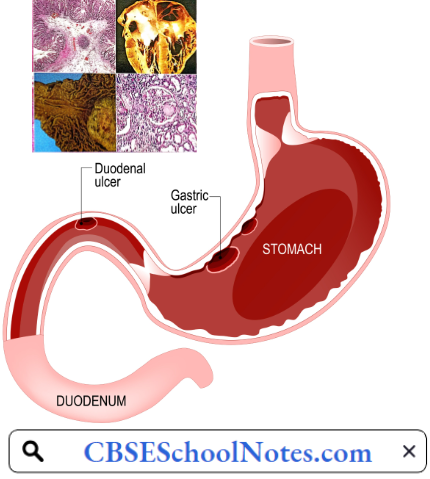
Peptic Ulcer Symptoms
- Burning stomach pain. The most common symptom of a duodenal ulcer is waking at night with upper abdominal pain that improves with eating. With a gastric ulcer, the pain may worsen with eating. The pain is often described as a burning or dull ache.
- The feeling of fullness, bloating, or belching
- Fatty food intolerance
- Heartburn
- Nausea
Read and Learn More Pathophysiology
Causes Of Peptic Ulcer
- H. pylori infection
- NSAIDs
- Alcohol
- Cigarette smoking
- Psychogenic stress
Peptic Ulcer Pathogenesis: It is a physiological marvel that gastric juice can easily digest the swallowed pieces of meat but normally, it has no corrosive action on the gastric mucosa itself. Several factors seem to be involved in the protection of gastric mucosa from autodigestion. These factors, collectively known as the gastric mucosal barrier, include:
- Mucus secreted by surface epithelial cells and mucus neck glands which forms a water insoluble visco-elastic gel with poor diffusion coefficient for H+.
- Bicarbonate is secreted by surface epithelial cells into the boundary zone between the epithelial cells and the mucus layer. The secretion of mucus and bicarbonate is believed to be mediated through prostaglandins.
- Tight Junctions between the adjacent cells of gastric surface epithelium.
- Rapid Turnover of surface epithelial cells, and rich blood supply.
- Prostaglandins: Endogenous prostaglandins stimulate the secretion of gastric mucus as well as gastric and duodenal mucosal bicarbonate. Prostaglandins also participate in the maintenance of gastric mucosal blood flow and integrity of the mucosal barrier and promote epithelial cell renewal in response to mucosal injury.
Under normal conditions, a physiologic balance exists between peptic acid secretion and gastro-duodenal mucosal defense. Mucosal injury may lead to peptic ulcer when the balance between the aggressive factors and the defensive mechanisms is disrupted.
- Aggressive factors, such as H. pylori, NSAIDs, alcohol, cigarette smoking, and psychogenic stress can alter the mucosal defense and allow back diffusion of hydrogen ions and subsequent epithelial cell injury.
- Mechanisms of injury differ distinctly between duodenal and gastric ulcers. Duodenal ulcer is essentially an H. pylori-related disease and is caused mainly by an increase in acid and pepsin load, and gastric metaplasia in the duodenal cap.
- Gastric ulcer is most commonly associated with NSAID ingestion, although H. pylori infection might also be present. Chronic, superficial, and atrophic gastritis predominate in patients with gastric ulcers when even normal acid levels can be associated with mucosal ulceration.
- Role Of Helicobacter Pylori: Helicobacter pylori is a bacillus responsible for one of the most common infections found in humans worldwide. H. pylori inhabit the mucus- adjacent to the gastric mucosa. Helicobacter pylori bacteria colonize the stomach and induce chronic gastritis.
- H. pylori is able to survive the highly acidic environment of the stomach because it protects itself by release of an enzyme urease, that splits blood urea and produces ammonia. The type of ulcer that develops depends on the location of chronic gastritis, which occurs at the site of H. pylori colonization.
- In those with duodenal ulcers, H. pylori colonizes the antrum. The inflammatory response to the bacteria causes destruction of somatostatin-producing D cells in the pylorus. Consequently, the G cells in the antrum secrete more of the hormone gastrin, which travels through the bloodstream to the fundus and body of the stomach.
- Gastrin stimulates the parietal cells to secrete more acid into the stomach lumen. Chronically increased gastrin levels eventually cause the number of parietal cells to also increase, further escalating the amount of acid secreted. The increased acid load damages the duodenum, and ulceration may eventually result.
- In contrast, in gastric ulcers, H. pylori colonizes the corpus of the stomach, where the acid-secreting parietal cells are located. However, chronic inflammation induced by the bacteria leads to a reduction of acid production, and eventually atrophy of the stomach lining. Gastric atrophy may lead to gastric ulcers and increase the risk of stomach cancer.
- Non-Steroidal Anti-Inflammatory Drugs: Non-steroidal anti-inflammatory drugs (NSAIDs) including low-dose aspirin are some of the most commonly used medicines. They are associated with gastrointestinal mucosal injury.
- Endoscopic studies have shown a prevalence rate of 14-25% of gastric and duodenal ulcers in NSAID users, NSAID acts as anti-inflammatory agents by inhibition of prostaglandin (PG) synthesis. As discussed earlier, prostaglandins are an important component of the gastric mucosal barrier. Inhibition of PG synthesis breaks the gastric mucosal barrier leading to peptic ulcers.
- Smoking: Cigarette smoking appears to be a risk factor for the development, maintenance, and recurrence of peptic ulcer disease. Smokers are about two times as likely to develop ulcer disease as non-smokers. Smoking predisposes to peptic ulcer by
- Acceleration of gastric emptying of liquids,
- Promotion of duodenal-gastric reflux,
- Reduction in mucosal blood flow, and
- Inhibition of mucosal prostaglandin production. Cigarette smoking not only causes ulcer formation but also increases the risk of ulcer complications such as ulcer bleeding, stomach obstruction, and perforation.
- Since cessation of smoking is associated with the prompt recovery of the respective functions, smokers will benefit immediately by stopping or reducing cigarette consumption.
- Cigarette smoking is also a leading cause of failure of medicinal treatment of peptic ulcers.
- Role Of Stress: The development of acute gastric ulcers as a result of severe stress after major surgery or extensive bums is well known. Reduced gastric blood flow coupled with raised plasma cortisol levels seem to be primarily responsible for such ulcers.
- Till the 1980s, psychological stress was considered the chief cause of the duodenal ulcers.
- The high-stung type “A” individuals were considered special candidates for the development of duodenal ulcers. In the 1990s, after the discovery of H. pylori, it began to be believed that psychogenic factors play no role in the development of chronic peptic ulcer disease.
- Over the years, it is now been appreciated that psychogenic stress acts as a co-factor with H. pylori in the production of hyperacidity leading to duodenal ulcers.
Peptic Ulcer Risk Factors
- Alcohol
- Spicy food
Alone, these factors do not cause ulcers, but they can make them worse and more difficult to heal.
Peptic Ulcer Complications: Left untreated, peptic ulcers can result in serious complications:
- Internal Bleeding: Bleeding can occur as slow blood loss that leads to anemia or as severe blood loss that may require hospitalization or a blood transfusion. Severe blood loss may cause black or bloody vomit or black or bloody stools. s
- Infection: Peptic ulcers can perforate the wall of the stomach putting at risk of a serious infection called peritonitis.
- Obstruction to the passage of food.
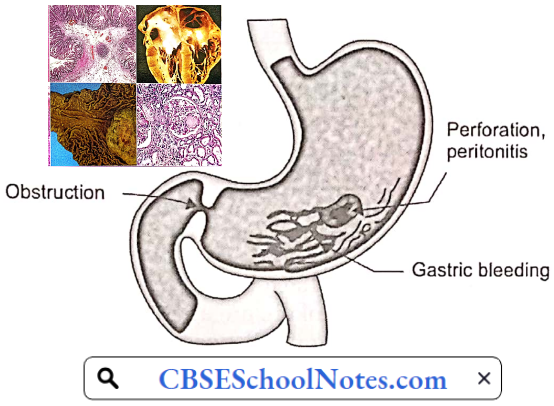
Hepatitis
Hepatitis is an inflammation of the liver. The condition can be self-limiting or can progress to fibrosis (scarring), cirrhosis, or liver cancer. Hepatitis viruses are the most common cause of hepatitis in the world but other infections, toxic substances (for example, alcohol, and certain drugs), and autoimmune diseases can also cause hepatitis.
Viral Hepatitis: Viral hepatitis is one of the major public health concerns around the world. Every year 1.4 million people die from viral hepatitis-related cirrhosis and liver cancer. Viral hepatitis is a cause for major healthcare burden in India as well.
There are 5 main hepatitis viruses, referred to as types A, B, C, D, and E. Viral hepatitis A, B, and E is an acute disorder. Types B and C lead to chronic hepatitis in hundreds of millions of people and, together, are the most common cause of liver cirrhosis and cancer.
- Hepatitis A virus (HAV) is present in the feces of infected persons and is most often transmitted through consumption of contaminated water or food. Most people in areas of the world with poor sanitation have been infected with this virus.
- Hepatitis B virus (HBV) is transmitted through exposure to infective blood, semen, and other body fluids. Transmission occurs through transfusions of HBV-contaminated blood and blood products, contaminated injections during medical procedures, and through injection drug use.
- HBV also poses a risk to healthcare workers who sustain accidental needle stick injuries while caring for infected HBV patients.
- Hepatitis C Virus (HCV) is mostly transmitted through exposure to infective blood. This may happen through transfusions of HCV-contaminated blood and blood products, contaminated injections during medical procedures, and through injection drug use. Sexual transmission is also possible but is much less common.
- Hepatitis D Virus (HDV) infections occur only in those who are infected with HBV. The dual infection of HDV and HBV can result in a more serious disease and worse outcome.
- Hepatitis E virus (HEV) is mostly transmitted through consumption of contaminated water or food. HEV is a common cause of hepatitis outbreaks in developing parts of the world and is increasingly recognized as an important cause of disease in developed countries.
Symptoms And Signs Of Hepatitis A
- Fatigue
- Sudden nausea and vomiting
- Abdominal pain or discomfort, especially on the upper right side beneath the lower ribs (site of the liver)
- Clay-colored stools
- Loss of appetite
- Low-grade fever
- Jaundice
- Dark urine
- Joint pain
- Intense itching
Pathology of Acute Hepatitis: The characteristic histopathological features of acute hepatitis include
- Ballooning degeneration
- Spotty necrosis
- Predominantly sinusoidal and lobular mononuclear cell infiltrate
- Kupffer cell hyperplasia
- Scattered apoptotic bodies
- Hepatocellular regeneration
Complications of Acute Hepatitis: Hepatic failure
Complications Of Chronic Hepatitis
- Hepatic failure
- Liver cirrhosis
- Hepatic cancer
Jaundice
Jaundice is a yellow discoloration of the skin, mucous membranes, and the whites of the eyes caused by increased amounts of bilirubin in the blood. Serum bilirubin level is normally below 1.0 mg/ dL, and levels over 2-3 mg/dL typically result in jaundice.
Bilirubin Metabolism
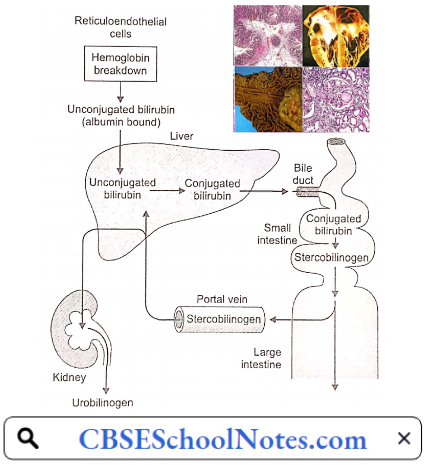
Destruction of senescent red blood cells in the tissue macrophages (in the spleen, liver, bone marrow, etc.) results in the catabolism of hemoglobin to haeme (and globin) and subsequently to bilirubin. Bilirubin released from the tissue macrophages is called unconjugated bilirubin.
- It is a lipid-soluble pigment transported in blood tightly bound to albumin. In the liver, the hepatocytes take up unconjugated bilirubin from the blood, convert it into water-soluble compounds called conjugated bilirubin (bilirubin mono- and di-glucuronide), and excrete it into bile canaliculi. The bile duct excretes conjugated bilirubin into the small intestine.
- Conjugated bilirubin cannot be absorbed in the intestines. In the large gut, bacterial degradation converts it to stercobilinogen (= urobilinogen), a water-soluble colorless product. Some of the urobilinogen is absorbed into the portal blood to reach the systemic circulation.
- Being water soluble, it is excreted into the urine by the kidneys. The remaining stercobilinogen is excreted in the feces. On exposure to air, stercobilinogen is oxidized to stercobilin which gives a brown color to the faeces.
- In obstructive jaundice, since bilirubin does not reach the intestines, stercobilinogen and urobilinogen excretion in the feces and urine is very low. That accounts for the pale chalky color of the stools of such patients.
Conjugated bilirubin is water-soluble; if present in the blood, it is excreted by the kidneys into the urine (bilirubinuria). Bilirubin imparts a dark brown color to the urine, an important clinical sign of conjugated hyperbilirubinemias (hepatic and post-hepatic jaundice). Classification of jaundice based on the pathophysiology of bilirubin metabolism is given below
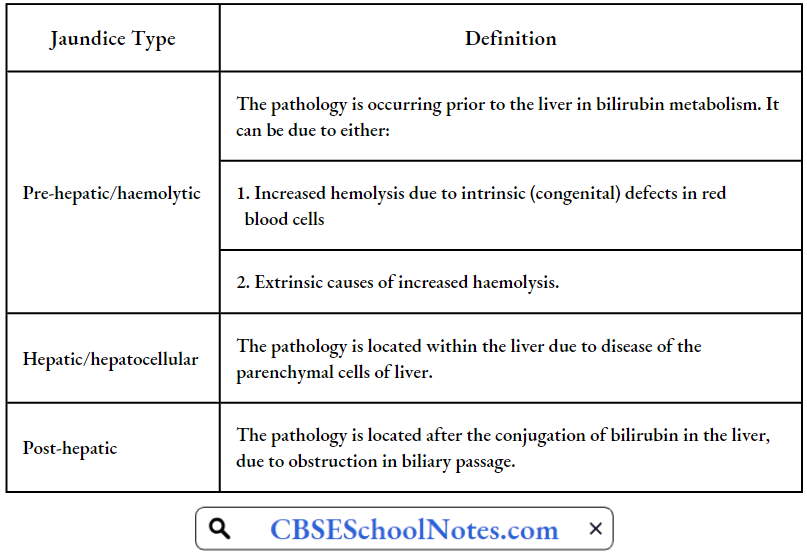
Pre-Hepatic Jaundice: Pre-hepatic jaundice is caused by an increased rate of hemolysis due to a congenital (sickle cell anemia, spherocytosis, thalassemia) or an acquired defect in the structure of red cells. The increased breakdown of red blood cells leads to an increase in the production of unconjugated bilirubin.
- The presence of excess of unconjugated bilirubin in blood causes its deposition into various tissues causing jaundice. Increased production of unconjugated bilirubin leads to increased production and increased excretion of stercobilinogen and urobilinogen in stools and urine respectively.
- Bilirubin is not found in the urine because unconjugated bilirubin is not water-soluble.
Pre-hepatic jaundice Laboratory Findings Include:
- Urine: Excess of urobilinogen, absent bilirubin.
- Serum: Increased unconjugated bilirubin.
Hepatic Jaundice: Hepatocellular (hepatic) jaundice results from an acute or chronic injury to hepatocytes (viral hepatitis, cirrhosis, alcoholic liver disease). Cell necrosis reduces the liver’s ability to take up, conjugate and excrete bilirubin. Therefore, the level of both unconjugated and conjugated types of bilirubin rises in the blood. The conjugated type of bilirubin, when present in the blood is excreted in the urine.
Hepatic Jaundice Laboratory Findings Include:
- Urine: Bilirubin present.
- Serum: contains excess of both conjugated and unconjugated bilirubin.
- Elevated levels of certain enzymes in the blood are indicative of hepatocellular injury.
Post-Hepatic Jaundice: Post-hepatic jaundice, also called obstructive jaundice, is caused by an interruption to the drainage of bile, containing conjugated bilirubin, in the biliary system.
- The most common causes are gallstones in the common bile duct, and cancer in the head of the pancreas, through which the bile duct passes. The back pressure on bile causes regurgitation of conjugated bilirubin and bile salts into blood circulation.
- In complete obstruction of the bile duct, bile does not reach the intestine, and stercobilinogen and urobilinogen are not found in the feces and urine, restively. Hence faeces have a pale chalky appearance.
Post-Hepatic Jaundice Laboratory Findings Include:
- Urine: Bilirubin present, urobilinogen absent
- Serum: contains excess of conjugated bilirubin.
Alcohol Liver Disease
Alcohol consumption is on the rise in India. Between 2010 and 2017, alcohol consumption in India increased by 38 per cent. In some parts of India, the prevalence of current alcohol use varies between 33% and 50%, with a higher prevalence among the lesser educated and the poor. In India, 15 people die every day from the effects of drinking alcohol.
Chronic Heavy Drinking May Lead To:
- Alcoholic fatty liver
- Alcoholic hepatitis
- Alcoholic cirrhosis (Laennec’s cirrhosis)
Between 10 and 20 percent of heavy drinkers will develop cirrhosis. Alcohol liver disease starts as an alcoholic fatty liver. It then progresses to alcoholic hepatitis, and then to alcoholic cirrhosis. Alcoholic liver cirrhosis is the most advanced form of liver disease that is related to drinking alcohol. Liver cirrhosis ends up as liver failure.
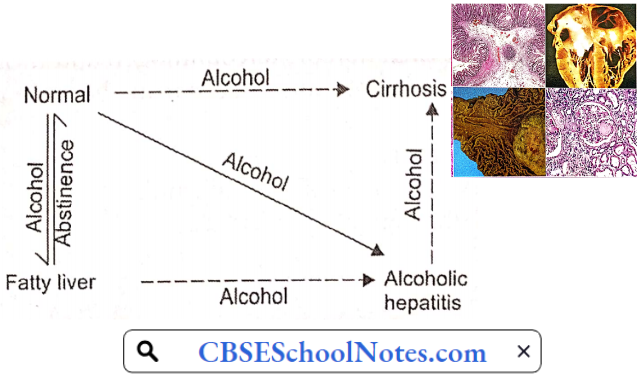
Alcohol Liver Disease Symptoms And Signs
- Alcoholic Fatty Liver
- Usually no symptoms
- Discomfort in the right upper abdomen (liver region)
- Fatigue
- Alcoholic Hepatitis
- Jaundice
- Fatigue
- Loss of appetite
- Low-grade fever
- Alcoholic Cirrhosis
- Fatigue
- Loss of appetite
- Nausea
- Ankles edema
- Nausea
- Vomiting
- Tenderness in the right upper abdomen
- Weight loss
- Jaundice
- Ascites
Pathogenesis Of Alcohol Liver Disease: In alcoholic liver disease, the total amount and duration of ethanol ingested rather than the type of alcoholic drink ingested determines the results. For example, 360 ml of beer (5% alcohol) and 45 ml of whisky contain the same amount of ethanol.
- Women appear to develop alcohol-induced liver injury at lesser levels of consumption than men. Malnutrition seems to augment the detrimental effects of alcohol. The cause of malnutrition in alcoholics is not merely economic. Even when economic problems is not present, alcoholism tends to produce malnutrition.
- In chronic alcoholics, alcohol itself may provide over 50% of total caloric requirements, which otherwise would have been provided by food containing proteins, vitamins, and minerals. The liver is the main site of alcohol metabolism.
- In the hepatocytes, alcohol is first oxidized to acetaldehyde, which is further oxidized to acetate. Both of these reactions increase the concentration of NADH which inhibits the operation of the citric acid cycle. Therefore, rather than undergoing further oxidation to CO2 and water, acetate is diverted to fatty acid synthesis.

Alcohol causes inhibition of fatty acid oxidation as well. Excessive concentration of acetaldehyde seems to inhibit biosynthesis and secretion of lipoproteins, the form in which fatty acids can be exported from the liver. Therefore, triglycerides accumulate in the hepatocytes, producing a “fatty liver”.
- Fatty liver may develop in any alcoholic after a bout of heavy drinking, but it is a reversible process. This condition presents clinically as a tender hepatomegaly with many non-specific symptoms such as malaise, weakness, anorexia, nausea, and abdominal discomfort.
- Elevated levels of hepatic enzymes may be the only laboratory finding. Jaundice is present in 15% of patients admitted to the hospital because of these symptoms of fatty infiltration of the liver.
- With total abstinence, the condition can return to normal within 2-4 weeks. However, continued alcohol consumption may result in more advanced forms of liver disease, either alcoholic hepatitis or cirrhosis.
Alcoholic Hepatitis: Some 10-15% of chronic alcoholics develop alcoholic hepatitis. Alcoholic hepatitis is characterized by hepatocyte ballooning, hepatocyte necrosis, and polymorphonuclear infiltration.
Deposition of collagen fibers around the central vein and in the perisinusoidal area sets the stage for progression to cirrhosis. A cardinal sign of alcoholic hepatitis is the rapid onset of jaundice. Other common features include fever and ascites.
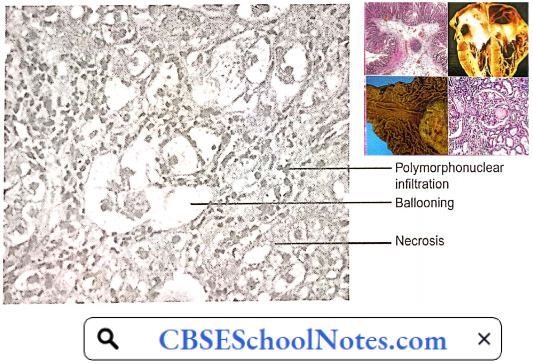
Encephalopathy may develop in those with severe hepatitis. Alcoholic hepatitis usually persists and progresses to cirrhosis if heavy alcohol use continues. If alcohol use ceases, alcoholic hepatitis resolves slowly over weeks to months, sometimes without permanent sequelae but often with residual cirrhosis.
Alcoholic Cirrhosis: The pathological hallmark of cirrhosis is the development of scar tissue that replaces normal hepatic parenchyma, blocking the portal flow of blood through the orga ]n and disturbing normal function.
- The fibrous tissue bands (septa) separate hepatocyte nodules; which eventually distort the entire liver architecture, and obstruct the normal hepatic blood flow leading to portal hypertension.
- Alcoholic liver cirrhosis is the most advanced form of liver disease that is related to drinking alcohol. Portal hypertension is responsible for most severe complications of cirrhosis such as edema feet, ascites, and bleeding from esophageal varices.

Complications Of Liver Cirrhosis
- Ascites
- Edema feet
- Bacterial peritonitis
- Bleeding from esophageal varices
- Hepatic encephalopathy
- Liver cancer
Inflammatory Bowel Disease
Inflammatory bowel disease (IBD) is an umbrella term used to describe disorders that involve chronic inflammation of your digestive tract. Types of IBD include
- Ulcerative Colitis: In ulcerative colitis, inflammation begins in the rectum and extends proximally in an uninterrupted fashion to the proximal colon, eventually involving the entire length of the large intestine. The small intestine is never involved.
- The rectum is always involved in ulcerative colitis, and no “skip areas” (i.e. normal areas of the bowel interspersed with diseased areas) are present. Ulcerative colitis primarily involves the mucosa and the submucosa, with the formation of crypt abscesses and mucosal.
- Crohn’s Disease: In Crohn’s disease, the most common location is the ileocecal region, followed by the terminal ileum Diseased segments frequently are separated by intervening normal bowel, leading to the term “skip areas.”
- Inflammation can be transmural (extending through the entire depth of the intestinal wall), often extending through to the serosa, resulting in sinus tracts or fistula formation.
Inflammatory Bowel Disease Signs And Symptoms that are common to both Crohn’s disease and ulcerative colitis include:
- Diarrhea
- Fever and fa li gue
- Abdominal pain and cramping
- Blood in your stool
- Reduced appetite
- Unintended weight loss
Inflammatory Bowel Disease Cause: The exact cause of inflammatory bowel disease remains unknown. One possible cause is an immune system malfunction.
- Age: Most people who develop IBD are diagnosed before they are 30 years old.
- Family History: You are at higher risk if you have a close relative—such as a parent, sibling, or child—with the disease.
- Cigarette Smoking: Cigarette smoking is the most important controllable risk factor for developing Crohn’s disease.
- Nonsteroidal Anti-Inflammatory Medications: These medications may increase the risk of developing IBD or worsen the disease in people who have IBD.
Inflammatory Bowel Disease Complications Colon Cancer: Having IBD increases your risk of colon cancer. General colon cancer screening guidelines for people without IBD call for a colonoscopy every 10 years beginning at age 50. Ask your doctor whether you need to have this test done sooner and more frequently.
- Skin, Eye, And Joint Inflammation: Certain disorders, including arthritis, skin lesions, and eye inflammation (uveitis), may occur during IBD flare-ups.
- Bowel Obstruction: Crohn’s disease affects the full thickness of the intestinal wall. Over time, parts of the bowel can thicken and narrow, which may block the flow of digestive contents. You may require surgery to remove the diseased portion of your bowel.
- Malnutrition: Diarrhea, abdominal pain, and cramping may make it difficult for you to eat or for your intestine to absorb enough nutrients to keep you nourished. It is also common to develop anemia due to low iron or vitamin B12 caused by the disease.
- Ulcers: Chronic inflammation can lead to open sores (ulcers) anywhere in your digestive tract, including your mouth and anus, and in the genital area (perineum).
Bone Diseases: Types, Symptoms, And Treatments
Disorders Of Bones and Joints
Rheumatoid Arthritis
Rheumatoid arthritis (RA) is characterized by inflammation and swelling of the synovial membrane of the joint, with subsequent destruction of articular structures. RA affects about 1% of the Indian population.
Rheumatoid Arthritis Aetiology: Rheumatoid arthritis is an autoimmune disorder of the synovial joints and other organs of the body.
Rheumatoid Arthritis Symptoms: Signs and symptoms of rheumatoid arthritis may include
- Tender, warm, swollen joints
- Joint stiffness that is usually worse in the mornings
- Fatigue
- Fever
- Loss of appetite
Read and Learn More Pathophysiology
Early rheumatoid arthritis tends to affect smaller joints first—particularly the joints that attach fingers to the hands and toes to the feet. As the disease progresses, symptoms often spread to the wrists, knees, ankles, elbows, hips, and shoulders.
In most cases, symptoms occur in the same joints on both sides of the body. Loss of movement and erosion of the joint surface lead to deformity and loss of function of the joint. About 40 percent of the people who have rheumatoid arthritis also experience signs and symptoms in other body systems, cardiovascular system in particular.
Rheumatoid Arthritis Pathophysiology: RA typically manifests with signs of inflammation of the synovial membrane. The affected joint is swollen, warm, painful, and stiff, particularly early in the morning on waking. The resulting inflammation thickens the synovial membrane, which can eventually destroy the cartilage and bone within the joint.
- As the pathology progresses, the inflammatory activity leads to tendon damage as well as erosion and destruction of the joint surface, which increases the range of movement and leads to deformity. Gradually the joint loses its shape and alignment.
- Destruction and fusion of bones of the wrist (carpal bones) is commonly observed. The skin, bones, and muscles adjacent to the joints atrophy from disuse and destruction.
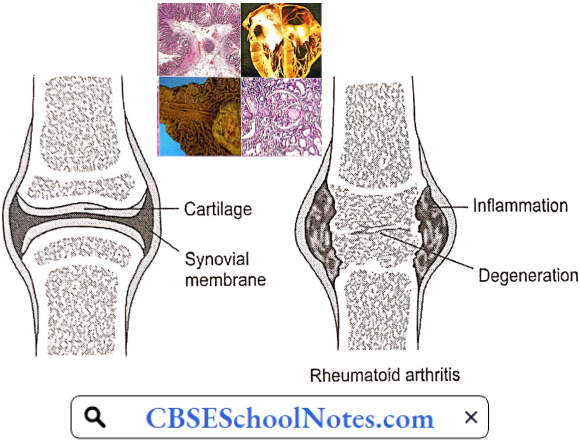
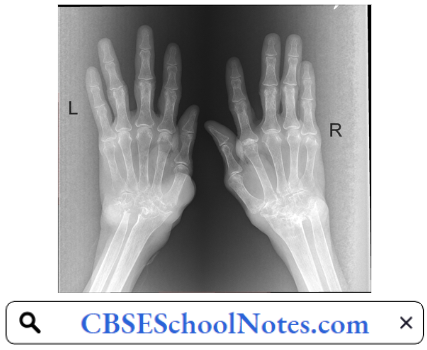
Rheumatoid Arthritis Risk Factors
- Sex: Women are more likely than men to develop rheumatoid arthritis.
- Age: Rheumatoid arthritis can occur at any age, but it most commonly begins in middle age.
- Family History: The risk of developing RA is greater, if there is a family history of the disease.
- Smoking: Cigarette smoking increases the risk of developing rheumatoid arthritis. Moreover, smoking also appears to be associated with greater disease severity.
Rheumatoid Arthritis Complications
- Osteoporosis, partly because of drugs used in the treatment of the disorder.
- Coronary artery disease
- Eye inflammation
- Stroke
- Anemia
- Lung fibrosis
- Depression
Osteoarthritis
Osteoarthritis is the most common chronic musculoskeletal disorder. Epidemiological studies estimate that it affects about 15% of the world’s population. In contrast to the inflammatory cause of rheumatoid arthritis, osteoarthritis is a degenerative disease.
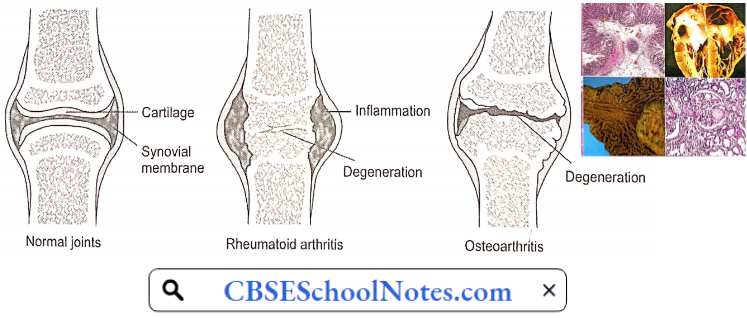
It occurs when the protective cartilage that cushions the ends of your bones wears down over time. The most common joints affected by osteoarthritis are the small joints of the hands and feet, the hip joint, and the knee joint.
Osteoarthritis Symptoms
- Pain or aching in the joint during activity, after a long activity, or at the end of the day.
- Joint stiffness usually occurs first thing in the morning or after resting.
- Limited range of motion that may go away after movement.
- Clicking or cracking sound when a joint bends.
- Swelling around a joint.
- Muscle weakness around the joint.
- Joint instability or buckling (knee gives out).
Osteoarthritis Aetiology: Osteoarthritis occurs when the cartilage that cushions the ends of bones in the joints gradually deteriorates. Cartilage is a firm, slippery tissue that enables nearly frictionless joint motion. Eventually, if the cartilage wears down completely, the bone will mb on bone.
Osteoarthritis Pathogenesis: Earlier, osteoarthritis has been considered to be a disease involving wear and tear of articular cartilage. Remnants of degenerated cartilage are found in the joint. Recent research has indicated that tire condition involves the entire joint.
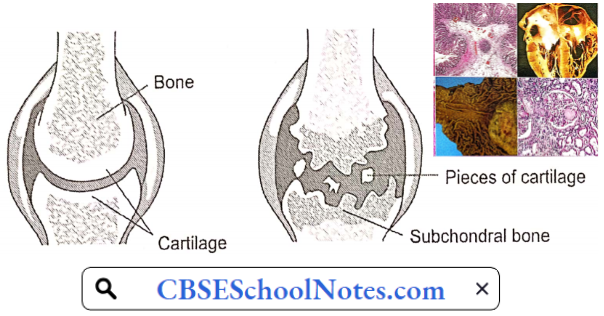
The loss of articular cartilage is the primary change, but a combination of cellular changes and biomechanical stresses causes several secondary changes, including subchondral bone remodeling, the formation of new bone at the joint margins called osteophytes and degenerative changes in the joint capsule, ligaments, and periarticular muscles.
Osteoarthritis Risk Factors: Factors that can increase the risk of osteoarthritis include
- Older Age: The risk of osteoarthritis increases with age.
- Sex: Women are more likely to develop osteoarthritis, though it is not clear why.
- Obesity: Carrying extra body weight contributes to osteoarthritis. The greater the body weight, the greater is the risk of osteoarthritis. Increased weight adds stress to weight¬bearing joints, such as hips and knees.
- Joint Injuries: Injuries, such as those that occur when playing sports or from an accident, can increase the risk of osteoarthritis.
- Repeated Stress On The Joint: If the job or a sport places repetitive stress on a joint, that joint might eventually develop osteoarthritis.
- Genetics: Some people inherit a tendency to develop osteoarthritis.
Osteoarthritis Complications
- Osteoarthritis is a degenerative disease that worsens over time, often resulting in chronic pain. Joint pain and stiffness can become severe enough to make daily tasks difficult.
- Depression and sleep disturbances can result from the pain and disability of osteoarthritis.
Osteoporosis
Osteoporosis is characterized by reduced bone mass and the disruption of normal bone architecture. The result is the fragility of bone that is easily fractured. Osteoporosis occurs in both men and women, but it sets in early and is more severe in women.
Around the world, 1 in 3 women and 1 in 5 men aged 50 years and over are at risk of an osteoporotic fracture. As explained below, Indians have lower bone mass as adults and hence are more prone to develop osteoporosis.

Osteoporosis seen in cases with immobilization or hormonal disorders such as Cushing syndrome or thyrotoxicosis is known as secondary osteoporosis. Senile osteoporosis in men and postmenopausal osteoporosis is far more common.
Osteoarthritis Symptoms: There typically are no symptoms in the early stages of bone loss. But once bones have been weakened by osteoporosis, signs and symptoms include:
- Back pain, caused by a fractured or collapsed vertebra
- Loss of height over time
- A stooped posture
- A bone that breaks much more easily than expected
Hip fractures often are caused by a fall and can result in disability and even an increased risk of death within the first year after the injury.
Osteoarthritis Aetiology And Risk Factors: The exact cause of senile/postmenopausal osteoporosis is not known. However, certain risk factors have been identified
- Peak Bone Mass: Peak bone mass has been identified as one of the most important factors in the pathogenesis of osteoporosis. Maximum bone mass is attained in both men and women at around the age of 30 years. A failure to attain optimal bone strength by this point is one factor that contributes to osteoporosis later in life.
- Bone is a living tissue. All the time some part of the bone is being resorbed and new bone is laid out. This process is known as bone remodeling. After the age of 30 years, the remodeling process involves slightly greater bone resorption than bone deposition.
- Thus, age-related bone loss gradually sets in. By the age of 60 years in men, and approximately a decade earlier in women, the loss of bone mass becomes significant. Osteoporosis sets in earlier in those with low peak bone mass.
- The racial difference in peak bone mass is reflected in the incidence of severe osteoporosis. In the American population, peak bone mass is significantly greater in blacks than whites. The incidence of fractured femoral neck (severe osteoporosis) is significantly greater in whites than blacks.
- Indians in general have low peak bone mass. Twin and family studies have shown that genetic factors play an important role in regulating bone mineral density and bone turnover.
- Gonadal Hormonal Deficiency: Ageing and loss of gonadal function are the 2 most important factors contributing to the development of osteoporosis. Estrogen or testosterone deficiency, regardless of age of occurrence, results in accelerated bone loss.
- The exact mechanisms of this bone loss is not clear. Whatever the mechanism, ultimately there is an increased bone resorption, which outpaces bone formation. Studies have shown that bone loss in women accelerates rapidly in the first years after menopause.
- Blood gonadal hormone levels decline with age both in males and females. However, the postmenopausal precipitous fall in blood estrogen levels observed in females does not occur in blood testosterone levels in males; blood testosterone levels in males decline more gradually.
- Dietary Calcium And Vitamin D: Dietary calcium and vitamin D intake during the first three decades of life is an important factor since it determines the value of peak bone mass.
- Exercise: At any age, immobilization with decreased weight bearing leads to rapid bone resorption. Physical activity, muscle strength, and body weight seem to be important determinants of bone strength. Osteoporotic subjects in general are less muscular and have lower body weight.
- Excessive Intake Of Acids: High acid intake, particularly in the form of a high protein diet may contribute to the development of osteoporosis; bone is involved in buffering the acid load. Acidosis may also increase the osteoclastic activity by a direct action.
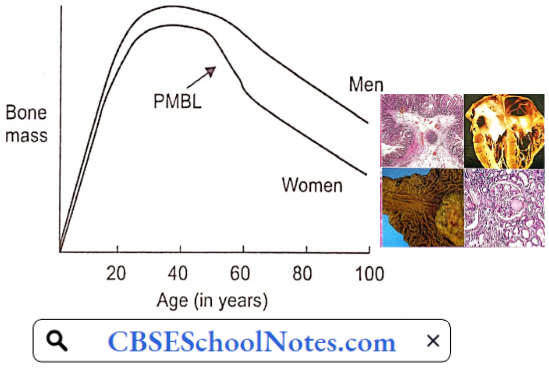
Osteoarthritis Complications: Bone fractures, particularly in the spine or hip, are the most serious complications of osteoporosis.
Gout
Gout is characterized by sudden, severe attacks of pain, swelling, redness, and tenderness in the joints, often the joint at the base of the big toe. In Western countries, gout occurs in 3-6% of men and 1-2% of women. In India, the prevalence of gout is much less, around 0.1%.
Gout Symptoms And Signs: The signs and symptoms of gout almost always occur suddenly, and often at night. They include
- Intense Joint Pain: Gout usually affects the large joint of the big toe, but it can occur in any joint. Other commonly affected joints include the ankles, knees, elbows, wrists, and fingers. The pain is likely to be most severe within the first four to 12 hours after it begins.
- Inflammation And Redness: The affected joint or joints become swollen, tender, warm, and red.
- Lingering Discomfort: After the most severe pain subsides, sore joint discomfort may last from a few days to a few weeks. Paler attacks are likely to last longer and affect more joints.
- Limited Range Of Motion: As gout progresses, movement in the joint becomes limit
Gout Causes: Clout occurs when urate crystals accumulate in a joint, causing inflammation and intense pain Urate crystals can form when a patient has a high serum uric acid level.
Gout Pathogenesis: Uric acid is normally produced in our body in the catabolism of purines. Purines are also found in certain foods, such as organ meats and seafood. Other foods also promote higher levels of uric acid, such as alcoholic beverages, especially beer, and drinks sweetened with fructose.
- Normally, uric acid remains dissolved in the blood and excreted by the kidneys into the urine. But sometimes serum uric acid rises due to either greater uric acid production in the body, or more often, decreased excretion by the kidneys.
- When this happens, uric acid can be deposited as sharp, needle-like urate crystals in a joint or surrounding tissue that cause pain, inflammation, and swelling.
- These crystals initiate the inflammatory process by being engulfed by synovial phagocytic cells leading to the release of lysosomal enzymes and the production of inflammatory chemokines. The chemotactic factors produced by monocytes and mast cells and the local vasodilatation stimulate neutrophilic chemotaxis.
- Also, endothelial cell activation further aggravates the inflammatory response and migration of neutrophils. The chemokines attract neutrophils into the synovial tissue and the synovial fluid.
The way to ultimately correct the underlying metabolic problem of hyperuricemia and the crystal deposition is to lower the serum urate level and dissolve the crystal deposits by medicines. This will stop both the acute attacks and the progressive joint damage.

Gout Risk Factors: Factors that increase the uric acid level in the body include
- Diet: Eating a diet rich in meat and seafood and drinking beverages sweetened with fruit sugar (fructose) increases levels of uric acid. Alcohol consumption, especially beer, also increases the risk of gout.
- Obesity: If one is overweight, the body produces more uric acid.
- Medical Conditions: Certain diseases increase the risk of gout. These include hypertension, diabetes, metabolic syndrome, and heart and kidney diseases.
- Certain Medications: The use of thiazide diuretics—commonly used to treat hypertension—and low-dose aspirin also can increase uric acid levels.
- Family History Of Gout
- Age And Sex: Gout occurs more often in men, primarily because women tend to have lower uric acid levels. After menopause, however, women’s uric acid levels approach those of men. Men are also more likely to develop gout earlier—usually between the ages of 30 and 50, whereas women generally develop signs and symptoms after menopause.
Gout Complications: People with gout can develop more severe conditions, such as
- Joint Destruction: If left untreated, gout can cause erosion and destruction of a joint.
- Urate Tophi: Untreated gout may cause deposits of urate crystals to form under the skin in nodules called tophi. Tophi can develop in several areas such as your fingers, hands, feet, elbows, or Achilles tendons.
- Kidney Stones: Urate crystals may collect in the urinary tract of people with gout, causing kidney stones.
Disorder Of Cardiovascular System Notes
Disorder Of the Cardiovascular System
Hypertension
Hypertension: Hypertension is a serious medical condition that significantly increases the risks of heart, brain, kidney, and other diseases. According to WHO, in 2015, worldwide 25% of males and 20% of females were suffering from hypertension.
Of these, only 20% of patients had BP under control. In India about 33% urban and 25% rural population is hypertensive. More worrying is the report that only one-tenth of rural and one-fifth of urban Indian hypertensive population have their BP under control. Hypertension is directly responsible for 57% of all stroke deaths and 24% of all coronary heart disease deaths in India.
Hypertension Definition: Hypertension is defined as arterial blood pressure greater than 140 mmHg and/or diastolic pressure greater than 90 mmHg. A systolic pressure of 120-140 mmHg or diastolic pressure of 80-90 mmHg is known as prehypertension.
Read and Learn More Pathophysiology
In a vast majority of cases of hypertension, no definite cause can be detected. Such patients are said to suffer from “essential hypertension.” In a small percentage of patients with hypertension, a definite cause can be found, such as kidney disease or/and endocrine disorder. Such cases are said to suffer from secondary hypertension.
Hypertension Symptoms: In most of the cases of high blood pressure, there are no symptoms till the complications occur. When blood pressure is very high, severe headaches may be reported.
Aetiology And Pathogenesis Of Essential Hypertension: Blood pressure = Cardiac output x Peripheral resistance = CO x PR
Regardless of the origin of hypertension, the actual increase in arterial blood pressure is caused by either an increase in peripheral vascular resistance (PR) or an increase in cardiac output (CO). The former is determined by the vascular tone (i.e. state of constriction) of systemic resistance vessels, whereas the latter is determined by heart rate and stroke volume.
In later stages of hypertension, only peripheral resistance is found to be increased; CO is normal. However, as discussed below, in the early stages of hypertension, many individuals have increased sympathetic activity leading to increased CO.
- Genetic Predisposition: Epidemiological studies have shown the importance of genetic predisposition in the development of essential hypertension. If a family history of hypertension is present, the subject has a 3-4 fold greater chance of developing hypertension, at an age earlier than the general population.
- Although genetics appears to contribute to essential hypertension, the exact mechanism has not been established. Genetic factors interact with environmental factors such as high salt intake, male sex, smoking, obesity, stress and physical inactivity, etc.
- Sympathetic Overactivity: There is evidence for a widespread autonomic abnormality in the early phases of hypertension. Overwhelming and excessive sympathetic activity is consistently present in some patients since their childhood.
- In the early stages of hypertension, blood pressure is elevated when recorded in a doctor’s clinic, but found to be normal when recorded at home. Such cases are said to suffer from “white coat hypertension”. Earlier, it was believed that persons with “white coat hypertension” do not develop established hypertension. There is no support for such an assertion; in fact, such patients are at a high risk of future accelerated hypertension.
- The hallmark of sympathetic over-activity in these patients is the so-called hyperkinetic state that is best characterized by borderline elevation of blood pressure, a fast heart rate, and an increased cardiac output even at rest.
- Both the hyperkinetic state and sympathetic overactivity are less readily recognizable later in the course of hypertension. A large proportion of previously hyperkinetic patients later develop established hypertension.
- It is not clear how from a fast heart rate /high cardiac output form of borderline hypertension is transformed later into the normal cardiac output/high vascular resistance profile that is characteristic of established hypertension.
- Role Of Sodium Intake: Essential hypertension is seen primarily in societies with an average sodium intake above 100 mEq/ day (2.3 g sodium); it is rare in societies with average sodium intakes of less than 50 mEq/day (1.2 g sodium). These epidemiological observations led to the suggestion that the development of hypertension requires a threshold level of sodium intake. This factor effect appears to be independent of other risk factors for hypertension, such as obesity.
- Vascular Hyper-reactivity: Hypertensive patients manifest greater vasoconstrictive response to infused norepinephrine or immersion of one hand in ice-cold water (cold pressor test) than normal individuals.
- Greater vasoconstrictive response to norepinephrine has also been demonstrated in normotensive offspring of hypertensive patients as compared to controls with no family history of hypertension. It suggests that vascular hyperreactivity may be genetic in origin.
- Renin-Angiotensin-Aldosterone-System (RAAS): In patients with essential hypertension, about 15% have mildly elevated plasma renin activity. In another 60% of hypertensives, plasma renin activity is “within the normal range’ but it may be inappropriate in the presence of elevated blood pressure.
- Less than 25% patients of with essential hypertension have subnormal plasma renin activity. Moreover, favorable therapeutic response to RAAS blockers suggests that a renin-dependent mechanism may be involved in tire pathogenesis in about 70% of cases of essential hypertension.
- The fundamental cause of elevated renin activity in such cases is not yet clear. It could be due to chronic sympathetic overactivity. This possibility is supported by the reports that administration of β-blockers in cases with essential hypertension leads to a decrease in plasma renin activity paralleled by a decrease in arterial blood pressure.
- Endothelial dysfunction: Due to its position between the bloodstream and vascular smooth muscle, endothelial dysfunction could either be a consequence or a causative factor in essential hypertension. In recent years, considerable evidence has suggested that changes in vascular endothelial function may cause an increase in vascular tone.
- For example, in hypertensive patients, the vascular endothelium produces less nitric oxide (intrinsic vasodilator). Moreover, the vascular smooth muscle is less sensitive to the actions of this powerful vasodilator. There may also be an increase in endothelin (a vasoconstrictor) production by the endothelial cells, which can enhance vasoconstrictor tone.
Complications Of Untreated Essential Hypertension
- Atherosclerosis: Many of the complications of hypertension are related to the effects of sustained elevations of blood pressure on vasculature and heart. Atherosclerosis is commonly associated with and is accelerated by long-standing hypertension.
- Most of the adverse outcomes in hypertension are associated with thrombosis rather than bleeding. Atherosclerosis predisposes the hypertensive patient to coronary thrombosis and cerebral stroke. Cerebral strokes are more often due to thrombosis rather than hemorrhage in the cerebral vessels.
- The excess morbidity and mortality related to hypertension are progressive over the whole range of systolic and diastolic blood pressures and are not limited to high values only. However, target-organ damage varies markedly between individuals with similar levels of hypertension. Atherosclerosis may also result in aortic aneurysm or peripheral arterial disease.
- Hypertensive Cardiomyopathy: A sustained increase in blood pressure (afterload) results in hypertrophy and subsequent dilatation of the left ventricle. Electrocardiographic evidence of left ventricular hypertrophy is found in up to 15% of persons with chronic hypertension. Left ventricular hypertrophy may cause or facilitate many cardiac complications of hypertension, including myocardial ischemia, congestive heart failure, and ventricular arrhythmias.
- Cerebrovascular Complications: Hypertension is an important risk factor for cerebral stroke. Approximately 85% of strokes are due to thrombosis and the remainder are due to hemorrhage in cerebral blood vessels.
- The term hypertensive encephalopathy is used to describe a group of symptoms and signs that sometimes follow a sudden and sustained rise in blood pressure. The symptoms are characterized by a severe headache, restlessness, impaired judgment, and memory, confusion, somnolence, and stupor. If the condition is not treated, these neurological symptoms may worsen and ultimately turn into a coma.
- Cerebral encephalopathy seems to result from a failure of autoregulation of cerebral blood flow. The autoregulation seems to fail when hypertension becomes excessive.
- Retinopathy: The primary response of the retinal arterioles to systemic hypertension is vasoconstriction. However, sustained hypertension leads to disruption of the blood—retinal barrier, increased vascular permeability, and secondary arteriolosclerosis. Loss of vision may occur.
- Renal Complications: Renal failure is one of the important complications of chronic hypertension. Sustained elevation of blood pressure damages renal microvasculature. Renal damage itself is a cause of hypertension (see secondary hypertension below), starting a vicious cycle.
- Sexual Dysfunction: Sexual dysfunction is more common and more severe in men with hypertension than it is in the general population. Hypertension is itself the major cause of erectile dysfunction. Experimental studies indicate that essential hypertension results in structural and functional changes in penile vasculature.
- Cavernous vessels are affected by chronic elevation of arterial blood pressure in the same fashion as other blood vessels. Marked hypertrophy in the smooth muscle of cavernous vessels, increased smooth muscle layer in cavernous space, and increased extracellular matrix (collagen) explain the pathophysiological mechanism of erectile dysfunction in essential hypertension.
Pathophysiological Basis Of Treatment Of Essential Hypertension
Non-Pharmacological Measures
- Reduction or elimination of factors such as stress, smoking, obesity
- Regular aerobic exercise
- Restriction of dietary calories, salt, cholesterol, and saturated fats
Pharmacological Measures: A variety of drugs are being used in the treatment of essential hypertension. They reduce cardiac output, peripheral resistance, or both.
Secondary Hypertension: Secondary hypertension is defined as hypertension that is caused by an underlying well-defined primary cause. It is much less common than essential hypertension, affecting only 5% of hypertensive patients. Some of the causes of secondary hypertension are treatable.
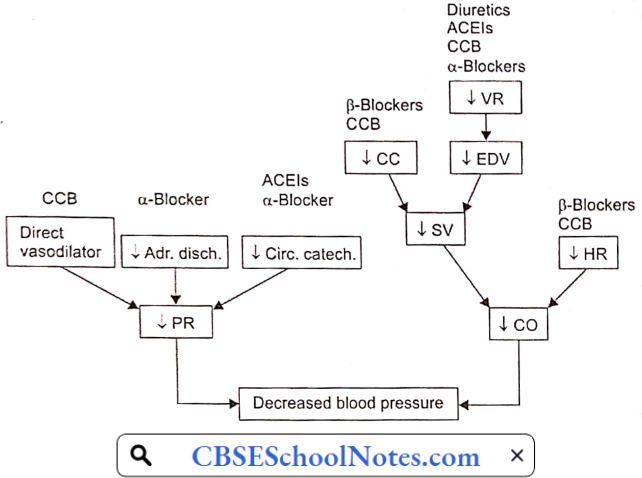
Secondary Hypertension Symptoms: Like primary hypertension, secondary hypertension usually has no specific signs or symptoms, even if blood pressure has reached dangerously high levels.
Secondary Hypertension Causes
- Chronic kidney disease (chronic glomerulonephritis)
- Renal artery stenosis
- Cushing syndrome (increased secretion of cortisol by a tumor of the adrenal cortex).
- Aldosteronism (increased secretion of aldosterone by a tumor of the adrenal cortex).
- Pheochromocytoma (increased secretion of norepinephrine and epinephrine by a tumor of the adrenal medulla).
- Coarctation of the aorta: There is congenital narrowing (coarctation) in the thoracic aorta. Hypertension is recorded in the upper part of the body only.
Atherosclerosis
Arteriosclerosis is the thickening, hardening, and loss of elasticity of the walls of arteries. This process gradually restricts the blood flow to one’s organs and tissues and can lead to severe organ damage. Atherosclerosis, which is a specific form of arteriosclerosis, is caused by the build-up of fatty acid-cholesterol plaques in the artery walls.
Atherosclerosis: Atherosclerosis develops primarily in large elastic arteries, for example, the aorta and carotid arteries, or large or medium-sized muscular arteries such as coronary, cerebral, renal, and popliteal arteries.
Atherosclerosis can lead to serious complications such as coronary artery disease, cerebral stroke, and peripheral arterial disease (gangrene of feet or legs). Risk factors associated with atherosclerosis, include:
- Elevated blood cholesterol and triglyceride levels
- High blood pressure
- Obesity
- Smoking
- Physical inactivity
- Diabetes mellitus
Atherosclerosis Symptoms: Atherosclerosis develops gradually. Mild atherosclerosis usually does not have any symptoms. Symptoms develop only when the narrowing of the artery is so severe that an adequate amount of blood does not reach the tissues or organs. At that time symptoms depend on the artery affected.
- Coronary Artery: Symptoms of angina or myocardial infarction
- Cerebral Artery: Symptoms of cerebral stroke.
- Renal Artery: Development of hypertension or symptoms of renal failure.
- Popliteal Artery: Pain in the legs while walking (claudication)
Pathogenesis Of Atherosclerosis: Aetiological factors named above induce hypercholesterolemia, which disturbs vascular homeostasis, including a decrease in nitrous oxide bioactivity, an increase in superoxide production, an increase in adhesion molecules, and attenuation of endothelium-dependent vasodilatation.
The earliest pathologic lesion of atherosclerosis is the fatty streak. The fatty streak is the result of focal accumulation of serum lipoproteins within the intima of the vessel wall. Gradually, the fatty streak progresses to form a fibrous plaque.
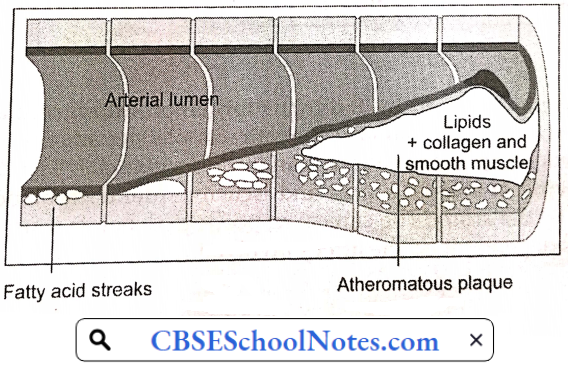
Circulating monocytes infiltrate the intima of the vessel wall. The combination of diabetes and hypertension appears to have an additive effect on monocyte adhesion. These tissue macrophages act as scavenger cells, taking up LDL cholesterol and forming the characteristic foam cells of early atherosclerosis.
These activated macrophages produce numerous factors that are injurious to the endothelium. Atherosclerotic plaque is the result of progressive lipid accumulation along with migration and proliferation of smooth muscle cells. Growth of the fibrous plaque results in progressive luminal narrowing.
Microscopy reveals lipid-laden macrophages, T-lymphocytes, and smooth muscle cells in varying proportions. Atheromatous plaques convert the smooth lining of the tunica intima of the blood vessels to a roughened surface prone to thrombosis.
Moreover, developing atherosclerotic plaques are prone to necrosis. Loss of the overlying endothelium or rupture of the protective fibrous cap may result in exposure of the thrombogenic contents of the core of the plaque to the circulating blood.
This exposure constitutes an advanced or complicated lesion. A plaque rupture may result in thrombus formation leading to partial or complete occlusion of the blood vessel.
Complications Of Atherosclerosis
Thrombosis: Rupture of plaque is followed by thrombus formation (intravascular clotting). The rough endothelial lining of a blood vessel attracts platelet adhesion and activation. Activated platelets result in the formation of an intravascular clot.
The thrombus results in critical narrowing of the arterial lumen and ischemia (deficient blood supply) in the tissues supplied by the artery. The clinical response to ischemia caused by obstructive atherosclerosis is dependent on the artery involved:
Coronary Artery Disease
Cardiovascular diseases are the number 1 cause of death globally. An estimated 17.9 million people died from CVDs in 2016, representing 31% of all global deaths. Of these deaths, 85% are due to heart attack and stroke.
In India, studies have reported an increasing prevalence of coronary artery disease over the last 60 years, from 1% to 9-10% in urban populations and <1% to 4-6% in rural populations.
Myocardial Oxygen Supply
- The myocardial oxygen supply depends on:
- The oxygen content of the arterial blood, and
The rate of coronary blood flow. The oxygen content of arterial blood may be decreased because of decreased hemoglobin concentration or because of poor systemic blood oxygenation (hypoxic hypoxia). Thus, angina may be a presenting feature of a patient with severe anemia or lung disease.
- In the absence of anemia or lung disease, oxygen supply to the heart is determined by the rate of coronary blood flow.
- In most other organs, because of the greater pressure head, blood flow is greater during systole than in diastole of the heart. However, in the case of the myocardium, the reverse is true. The coronary arteries that run on the surface of the heart are called epicardial coronary arteries.
- Branches of epicardial arteries that run into and supply blood to the myocardium are called subendocardial coronary vessels. During systole, myocardial contraction has a strangulating effect on the blood vessels passing through the cardiac muscle fibers. Because of this, blood flow in the subendocardial vessels stops.
- As a result, most myocardial perfusion occurs during diastole when the subendocardial coronary vessels are patent because of the absence of extramural pressure.
- Although coronary vessels are supplied with sympathetic and parasympathetic nerve fibers, coronary vascular resistance is chiefly determined by intrinsic metabolic factors rather than neural control.
- Local vasodilator metabolites such as adenosine (chiefly) and other products of anoxic metabolism (lactate, H+, certain prostaglandins) regulate coronary blood flow by a direct action on vascular smooth muscle. During exercise, greater release of local vasodilator metabolites assures greater blood flow in the coronary arteries.
- Atherosclerotic narrowing of coronary arteries produces its effects mainly by hypo-perfusion (decreased blood supply) of the myocardium. The effect may range from angina to myocardial infarction.
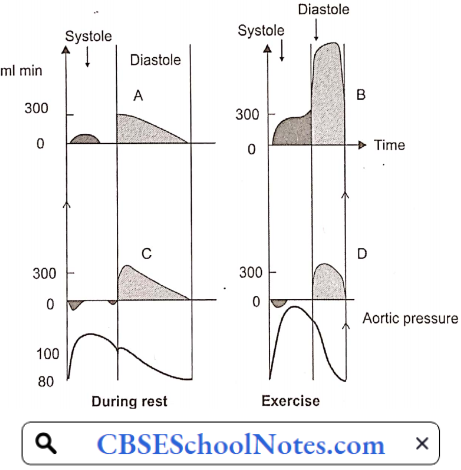
Angina Pectoris: In normal individuals during exercise, by the local metabolite control, coronary arteriolar resistance decreases in proportion to the increase in O2 demand of the myocardium. Thus, coronary blood flow increases in proportion to the oxygen demand of the myocardium.
- When atherosclerotic narrowing is greater than 60-70%, coronary blood flow cannot increase during exercise in spite of the presence of vasodilator metabolites. Therefore, myocardial ischemia results; which is commonly intermittent (only during exertion).
- Anginal pain is characterized by the fact that it occurs only at times of increased myocardial oxygen demand such as exertion or emotional excitement, but subsides by rest. Such a condition is known as angina. In angina, pain may be localized to the substernum or referred to the left arm, neck, or jaw.
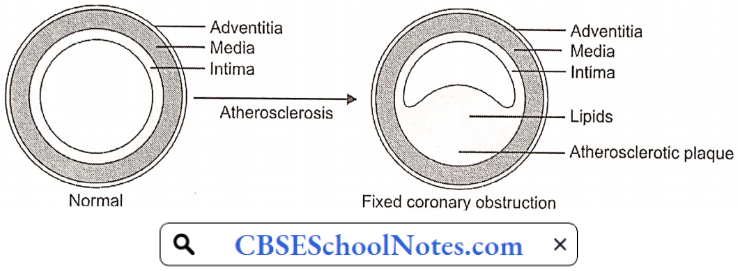
Angina Pectoris Symptoms: Angina symptoms include
- Pain or discomfort can spread to the chest, jaw, shoulders, arms (mostly the left arm), and back.
- Chest tightness, burning, heaviness, feeling of squeezing or not being able to breathe.
- Angina will sometimes cause dizziness, paleness, and weakness.
The Mechanisms Of Cardiac Pain: It is presumed that pain of angina pectoris results from the release of anoxic metabolites (adenosine, bradykinin) by the myocardium. These metabolites excite the sensory ends of the sympathetic and vagal afferent fibers supplying the heart.
Within the spinal cord, cardiac sympathetic afferent impulses may converge with impulses from somatic thoracic structures, which may be the basis for referred cardiac pain, for example, to the left arm.
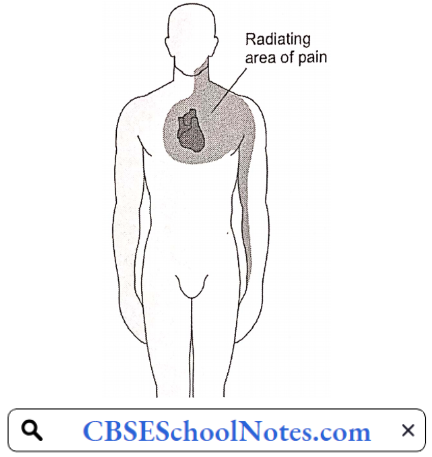
Pathophysiologic Basis Of Treatment Of Angina: For the immediate relief of angina pain, the patient is advised to take a sublingual tablet of nitroglycerin.
- Nitroglycerin is converted to a powerful vasodilator nitric oxide (NO) in the body. It may produce some dilation of coronary arteries, but the major action is venous vasodilation. Vasodilation causes the pooling of blood within the venous system, reducing preload to the heart.
- This causes a decrease in cardiac work, and cardiac oxygen demand and hence relieves angina pain.
Myocardial Infarction
When the myocardial ischemia progresses to a degree that irreversible necrosis of a part of the myocardium occurs, an acute myocardial infarction (MI) is said to have occurred. An acute MI almost always results from an acute thrombotic obstruction of an atherosclerotic coronary artery.
Myocardial Infarction Symptoms
- Chest pain or discomfort, possibly described as pressure, squeezing, burning, or fullness
- Pain in the left arm, neck, jaw, shoulder, or back accompanying chest pain
- Nausea
- Fatigue
- Shortness of breath
- Sweating
- Dizziness
In acute MI, the pain has the same characteristics as angina, but it is far more severe, lasts longer, may radiate more widely, and is not relieved by rest or nitroglycerin. Pain may be due to the accumulation of anoxic metabolites as well as products of tissue necrosis. The pain is accompanied by greater psychogenic effects, i.e. feeling of impending death.
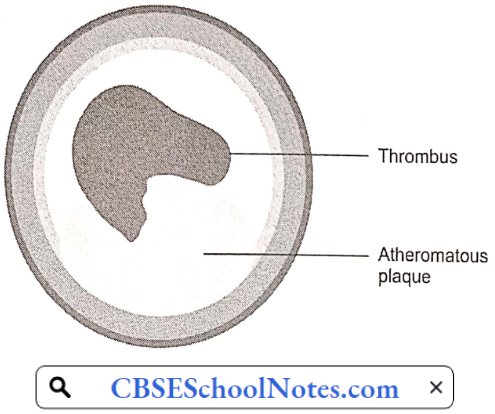
Myocardial Infarction Pathogenesis: Acute myocardial infarction (MI) indicates irreversible myocardial injury resulting in necrosis of a significant portion of myocardium (generally >1 cm). Myocardial infarction is usually due to thrombotic occlusion of a coronary vessel caused by rupture of a vulnerable plaque.
Ischemia induces profound metabolic and ionic perturbations in the affected myocardium. Prolonged myocardial ischemia results in ischemic necrosis of the myocardium. The adult mammalian heart has negligible regenerative capacity, thus the infarcted myocardium heals through the formation of a scar.
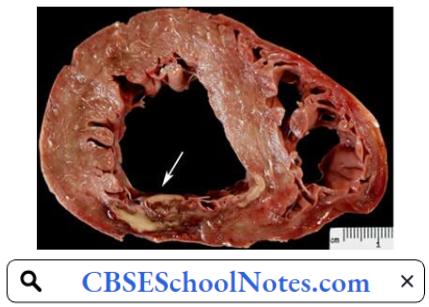
Infarct healing is intertwined with the geometric remodeling of the chamber, characterized by dilation, hypertrophy of viable segments, and progressive dysfunction. Cell membrane damage in acute MI leads to the release of certain intracellular enzymes. An increase in their plasma levels is used as diagnostic evidence of myocardial infarction.
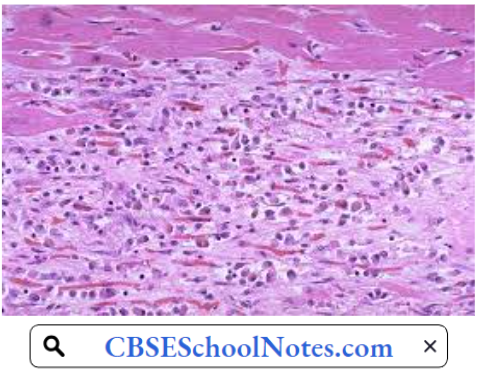
Myocardial Infarction Risk Factors
- Age: Men age 45 or older and women age 55 or older are more likely to have a heart attack than are younger men and women.
- Tobacco: This includes smoking and long-term exposure to second-hand smoke.
- High Blood Pressure: Over time, high blood pressure can damage coronary arteries.
- High Blood Cholesterol Or Triglyceride Levels: A high level of low-density lipoprotein (LDL) cholesterol (the ‘bad’ cholesterol) is most likely to narrow arteries. A high level of triglycerides, a type of blood fat related to your diet, also increases your risk of heart attack.
- Obesity: Obesity is associated with high blood cholesterol levels, high triglyceride levels, high blood pressure, and diabetes.
- Diabetes.
- Family history of heart attack
- Lack of physical activity
- Stress.
Myocardial Infarction Diagnosis
- Electrocardiogram: An electrocardiogram (ECG) is a recording of the electrical activity of the heart. Abnormalities in electrical activity usually occur with heart attacks and can identify the areas of the heart muscle that are deprived of oxygen and/or areas of muscle that have died.
- In a patient with typical symptoms of heart attack (such as crushing chest pain) and characteristic changes of heart attack on the ECG, a secure diagnosis of heart attack can be made quickly in the emergency room and treatment can be started immediately.
- Blood Tests: Cardiac enzymes are proteins that are released into the blood by dying heart muscles. These cardiac enzymes are creatine kinase (CK-MB), and troponin, and their levels can be measured in blood.
- These cardiac enzymes typically are elevated in the blood several hours after the onset of a heart attack. Currently, troponin levels are considered the preferred lab tests to use to help diagnose a heart attack, as they are indicators of cardiac muscle injury or death.
A series of blood tests for tire enzymes performed over a 24-hour period are useful not only in confirming the diagnosis of heart attack, but the changes in their levels over time also correlate with the amount of heart muscle that has died.
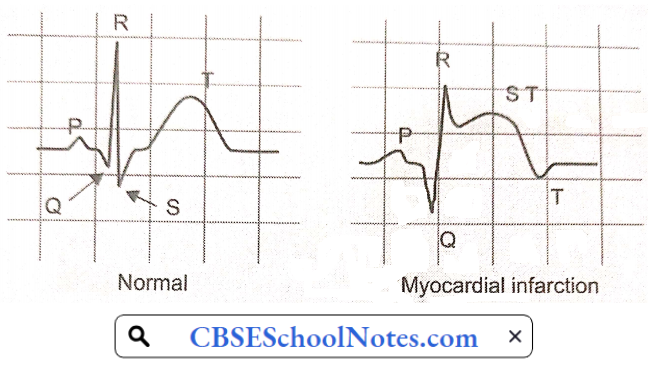
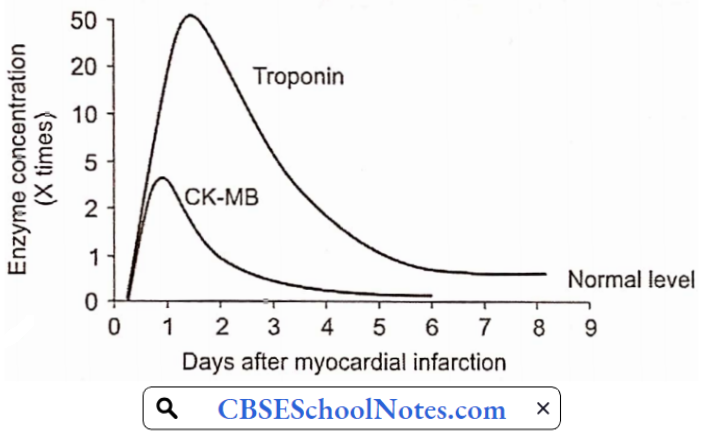
Complications Of MI: More important complications include
- Cardiogenic shock
- Cardiac arrhythmias (ventricular tachycardia or ventricular fibrillation are life-threatening complications).
- Congestive heart failure
Pathophysiologic Basis Of Treatment: Treatment aims at immediate restoration of blood flow in the artery blocked by a blood clot followed by measures to prevent thrombosis again
- Angioplasty And Stent: Special tubing with an attached deflated balloon is threaded up to the coronary arteries. A stent is a wire mesh tube used to prop open an artery during angioplasty.
- Long-term antiplatelet therapy
Congestive Heart Failure
Congestive heart failure (CHF), or heart failure is defined as an inability of the heart to pump blood at a rate appropriate for the metabolic requirements of the tissues;
- Aetiology: Important causes include:
- Hypertension: Due to high blood pressure, expulsion of blood requires more forceful ventricular contraction during each systole. Over time, the left ventricle initially undergoes hypertrophy and later it dilates leading to heart failure.
- Coronary Artery Disease: Myocardial infarction weakens the myocardium.
- Valvular Disease: Disorders of aortic or mitral valve cause extra burden on the heart. Initially, the heart undergoes hypertrophy and later dilatation.
Congestive Heart Failure Symptoms And Signs
- Exercise intolerance
- Fatigue
- Dyspnoea on effort
- Cyanosis
- Ankle edema
- Distended neck veins
- Liver enlargement (hepatomegaly)
- Spleen enlargement (splenomegaly)
- Oedema feet
- Ascites (fluid in the peritoneal cavity, abdomen)

Pathophysiology Of CHF: When the heart is unable to pump out a sufficient amount of blood, a number of natural compensatory mechanisms are activated so as to improve the cardiac output and maintain normal perfusion of the vital organs. These mechanisms include:
- Frank-Starling mechanism
- Increased adrenergic discharge
- Regional redistribution of cardiac output
- Hormonal mechanisms
As you have learned in physiology lectures, cardiac output can be increased by an increase in end-diastolic volume (EDV) (Starling mechanism) as well as an increase in sympathetic discharge to the heart. Both of these mechanisms are utilized to bring the failing heart to produce normal cardiac output.
The other two compensatory mechanisms help in these primary mechanisms are:
- Frank-Starling Mechanism: By working at greater EDV (Y), the heart can pump out a normal amount of blood. EDV is increased by the fourth compensatory mechanism mentioned above.
- Increased Adrenergic Discharge: In the failing heart, depressed cardiac output is sensed by high-pressure baroreceptors located in the carotid sinus and aortic arch, leading to a reflex increase in adrenergic discharge to the heart and blood vessels.
- In the heart, increased adrenergic discharge improves the cardiac output by increasing the heart rate as well as stroke volume. In the blood vessels, it causes a redistribution of cardiac output described next.
- Redistribution Of Cardiac Output: The redistribution of cardiac output serves as an important compensatory mechanism when cardiac output is reduced. Blood flow is redistributed so that the delivery of oxygen to vital organs, such as the brain and myocardium, is maintained at normal or near-normal levels, while flow to less critical areas, such as the cutaneous and muscular beds and viscera, is reduced. Vasoconstriction mediated by the adrenergic nervous system is largely responsible for this redistribution.
- Hormonal Mechanisms: Decreased cardiac output activates the renin-angiotensin II mechanism. Angiotensin II produces arteriolar constriction and increases thirst (increased water intake). It also increases aldosterone secretion, thereby producing salt and water retention in the kidney. As a result of both these factors, blood volume and thereby EDV is increased.
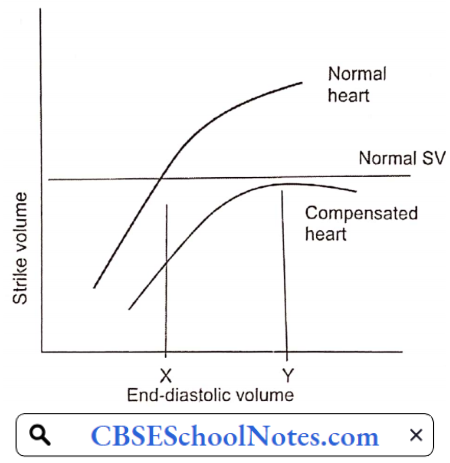
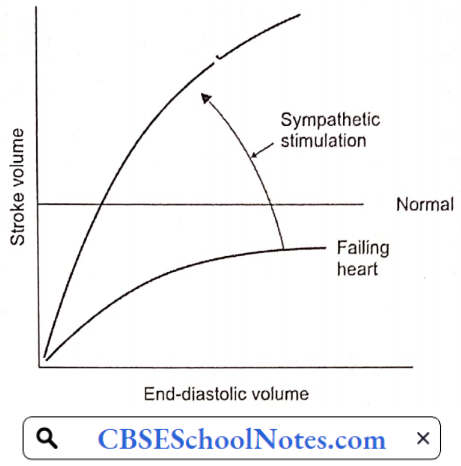
Congestive Heart Failure Decompensation: As the cardiac function gradually deteriorates, the compensatory mechanisms discussed above cannot maintain normal cardiac output. Moreover, excessive increase in EDV increases left and right atrial pressures resulting in congestion in the lungs and in systemic veins. At this point, congestive heart failure is said to have set in.
Pathophysiological Basis of Treatment
- Strengthening The Force Of Contraction Of The Heart: Digitalis.
- Reducing Salt And Water Retention: Diuretics
- Reducing Sympathetic Over-Activity: Beta-blockers