
Endocrine Disorders
Diabetes Mellitus
Diabetes currently affects more than 62 million Indians, which is more than 7.2% of the adult population. Nearly 1 million Indians die due to diabetes every year. The high incidence is attributed to a combination of genetic susceptibility plus the adoption of a high-calorie diet, coupled with a low-activity lifestyle by India’s growing middle class.
Two Types Of Diabetes Mellitus (DM) Are Recognized
- Type 1 Diabetes Mellitus: Type 1 or insulin-dependent diabetes mellitus (IDDM) is juvenile-onset diabetes. In type I diabetes, there is an absolute deficiency of insulin. It is believed to be an autoimmune disease, which manifests in childhood. The patients are usually lean. Ketosis and acidosis are common complications of this type of diabetes. Plasma insulin levels are very low or undetectable.
- Type 2 Diabetes Mellitus: Type 2 diabetes manifests after the age of 40 years. Most of the patients with this type of diabetes are obese. Plasma insulin levels are often normal or even elevated. However, there seems to be a deficiency of insulin receptors in the tissues so at the tissue level, circulating insulin is ineffective. Ketotic acidosis is not very common in type 2 diabetes.
Read and Learn More Pathophysiology
Symptoms And Signs Of Diabetes Mellitus
- Polyuria
- Polydipsia
- Weight loss despite polyphagia
- Hyperglycemia
- Glycosuria
- Muscle weakness
- Frequent infections
- Ketosis
- Acidosis and
- Coma
Diabetes Mellitus Pathogenesis: At the metabolic level, fundamental defects in DM are
- Decreased glucose utilization
- Increased glucose production
- Increased lipolysis
- Increased protein catabolism
Diabetes mellitus starts without any symptoms. Gradually the condition worsens and when the blood sugar level is above 180 mg%, sugar appears in the urine. Only then does the patient become aware of the problem. In many cases, diabetic patients come to know about their disease only when they visit a physician for some other ailment and their blood glucose level is tested.
1. Hyperglycemia And Its Consequences: Hyperglycemia is one of the cardinal features of diabetes mellitus. It is due to
- Decreased peripheral utilization of glucose and
- Increased hepatic production of glucose (gluconeogenesis).
Mild transient hyperglycemia is harmless and occurs after every meal. However, when the blood glucose level is chronically elevated, numerous complications arise. When the blood glucose level exceeds the renal threshold, glucose appears in the urine (glycosuria).
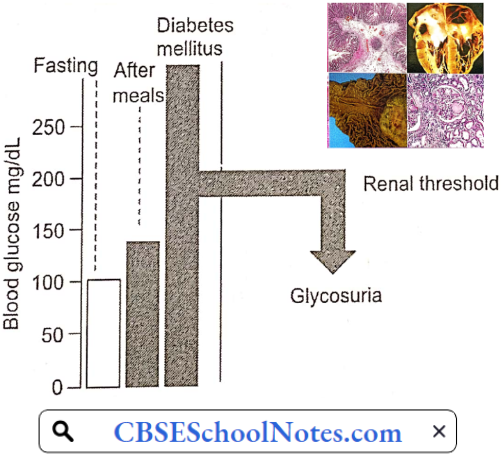
Renal excretion of osmotically active glucose molecules leads to the loss of large amounts of water in the urine (osmotic diuresis). The resultant dehydration activates the thirst mechanism leading to a large amount of water intake (polydipsia). The loss of glucose in the urine means loss of energy (calories) from the body.
An appreciable amount of Na+ and K+ are lost in the urine as side effects of osmotic diuresis. Deficient utilization of glucose in the hypothalamic ventromedial nuclei (satiety center) causes hyperphagia. In spite of excessive food intake, there is a loss of body weight liable to infections.
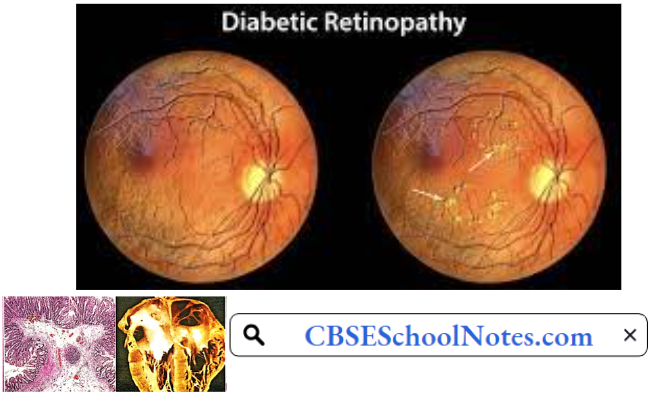
Chronically elevated blood glucose levels result in the attachment of glucose (glycosylation) to hemoglobin and tissue proteins. Tissue protein damage is responsible for long-term complications such as neuropathy, retinopathy, cataracts, nephropathy (kidney damage), and hypertension.
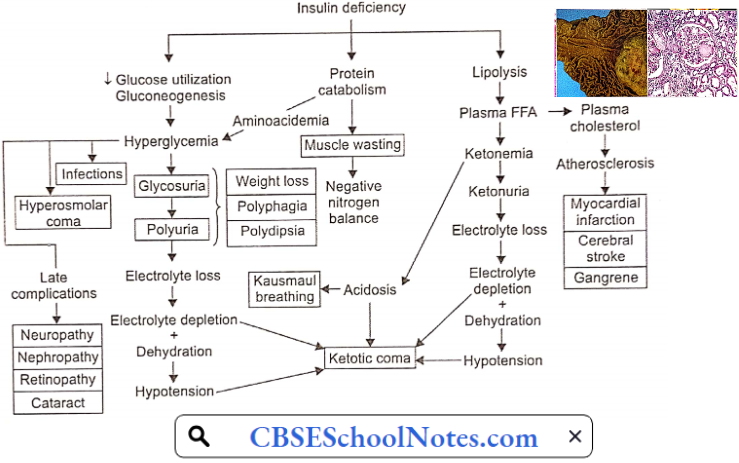
2. Ketosis And Its Consequences: A deficiency of insulin causes a great reduction in lipogenesis and accelerates the process of lipolysis. As a result, the plasma level of FFA is more than doubled.
- Free fatty acids provide energy to the glucose-starved insulin-sensitive tissues, like skeletal muscle. However, FFA mobilization also causes the formation of ketone bodies. The ketone body’s formation exceeds the rate of their utilization leading to ketosis and acidosis.
- Acidosis results in rapid, deep respiration (dyspnoea). The patient’s breath smells of acetone. The urine becomes highly acidic. When the capacity of the kidney to replace plasma cations accompanying the organic anions with H+ and NH4 is exceeded, Na+ and K+ are lost in the urine.
- The electrolyte and water loss leads to dehydration, hypovolaemia, and hypotension. Finally, acidosis and dehydration may depress the consciousness to the level of coma and death.
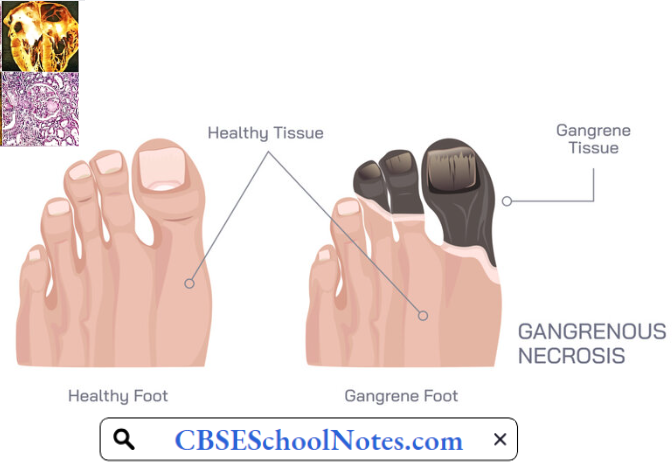
- Chronic hyperlipidemia leads to atherosclerosis which causes coronary artery disease cerebral stroke and gangrene in the lower limbs.
3. Protein Catabolism: In diabetes, protein anabolism is suppressed and catabolism is increased. Large amounts of amino acids are used for energy production. Amino acids also act as substrates for enhanced gluconeogenesis promoted by insulin deficiency. Consequently, the patient suffers from loss of weight, protein depletion, wasting, and negative nitrogen balance.
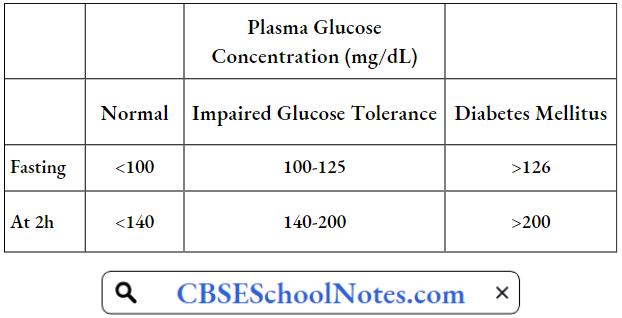
Glucose Tolerance Test (GTT): This is a test for the diagnosis of diabetes mellitus. After an overnight fast, a venous blood sample is taken. Then, the patient is given 75 g of glucose orally and four blood samples are collected half-hourly for estimation of plasma glucose levels. Plasma glucose levels are plotted against a time scale and the graph so obtained is known as the glucose tolerance curve.
The Results Are Interpreted As Follows:

Important Role Of Estimation Of Glycosylated Hemoglobin: In a normal subject, glucose molecules get a non-enzymic attachment to a small proportion (<7%) of hemoglobin-A to form glycosylated hemoglobin. In case of sustained hyperglycemia, such as in diabetes mellitus, a greater proportion (10-20%) of hemoglobin is glycosylated.
- The concentration of glycosylated hemoglobin has been found to reflect the average blood glucose level during the previous 6-8 weeks.
- Therefore, its measurement has become an important tool for the proper regulation of antidiabetic therapy, that is, to find out whether the given dose of the medication has been able to maintain blood glucose level within the physiological range during the previous 6-8 weeks. (The glucose tolerance test reflects the glucose level on the day of the test only.)
Long-term Complications Of Diabetes Mellitus
- Neuropathy, leading to numbness and muscle weakness
- Retinopathy, leading to blindness
- Cataract
- Nephropathy, leading to chronic renal failure
- Hypertension
- Coronary artery disease, and
- Strokes.
- Gangrene in lower limbs
Risk Factors For Type 1 Diabetes Include:
- Family History
- Genetics: The presence of certain genes indicates an increased risk of developing type 1 diabetes.
- Geography: The incidence of type 1 diabetes tends to increase as you travel away from the equator.
Risk Factors For Type 2 Diabetes Include:
- Overweight
- Inactivity
- Family History
- Age: The risk of type 2 diabetes increases as you get older, especially after age 45.
- Prediabetes: Prediabetes is a condition in which one’s blood sugar level is higher than normal, but not high enough to be classified as diabetes. Left untreated, prediabetes often progresses to type 2 diabetes.
- Gestational Diabetes: If one develops gestational diabetes, she has a greater risk of type 2 diabetes.
Disorders Of Thyroid Gland
Diseases of the thyroid gland are among the most abundant endocrine disorders worldwide second only to diabetes; India is no exception. Recent report shows that 300 million people in the world are suffering from thyroid disorders and among them about 42 million people reside in India.
Hypothyroidism is the most common thyroid disorder. Hyperthyroidism is less common. Thyroid disorders are more common in women than in men.
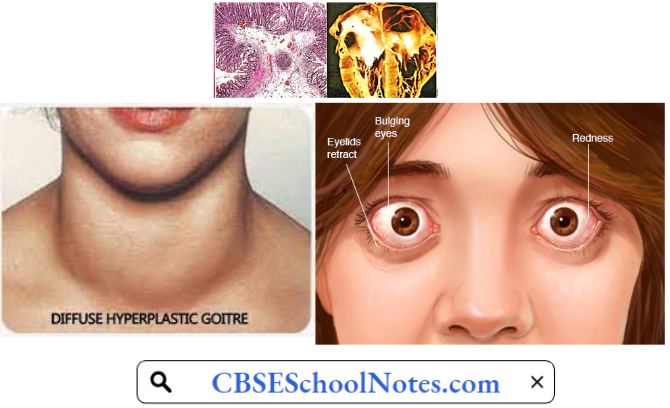
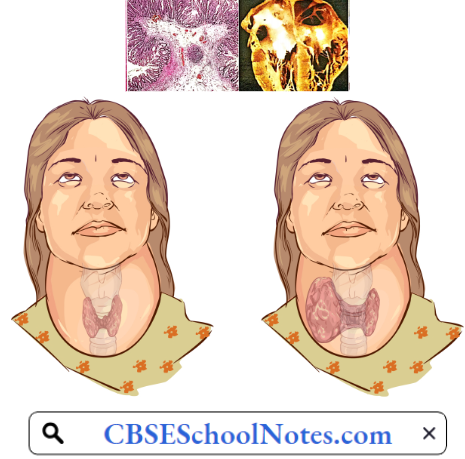
Hyperthyroidism: Hyperthyroidism results from excessive secretion of thyroid hormones. It is known as Graves’ disease or exophthalmic goiter. Less commonly, excessive thyroxine secretion is due to a thyroid adenoma (toxic thyroid adenoma).
Hyperthyroidism Aetiology: Graves disease is an autoimmune disorder characterized by the development of thyroid-stimulating immunoglobulin (TSI).
- TSI acts on thyroid stimulating hormone receptors (TSH-receptors) on the thyroid follicular cells to activate thyroid hormone synthesis and release as well as causes hypertrophy and increased vascularity of the thyroid gland.
- This results in the characteristic picture of Graves’ thyrotoxicosis, with a diffusely enlarged thyroid and excessive plasma thyroxine levels.
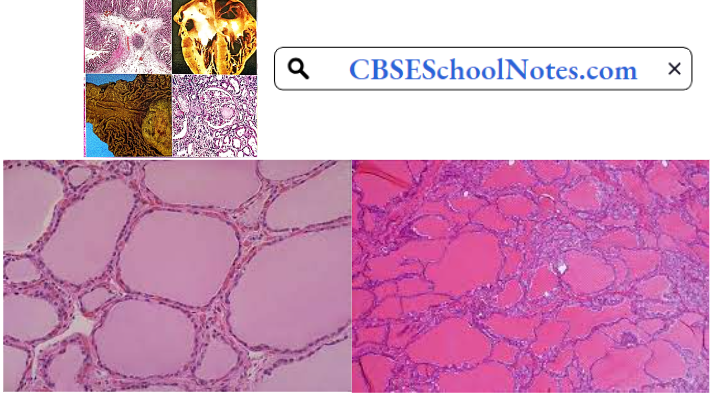
Hyperthyroidism Pathology: There is a diffuse thyroid enlargement of the thyroid gland (goiter). Microscopically, thyroid follicles are hypercellular and lined by tall columnar cells. In the follicles, colloids is scanty and show semi-lunar erosions near the follicular cells. Stroma shows lymphocytic infiltration.
Hyperthyroidism Symptoms And Signs: All the symptoms and signs reflect the effects of increased plasma thyroxine levels on various organs and tissues of the body
- Palpitation
- Tachycardia
- Nervousness
- Loss of weight
- Easy fatigability
- Restlessness
- Fine tremor
- Excessive appetite
- Diarrhea
- Excessive sweating
- Heat intolerance
- Muscle weakness
- Increased basal metabolic rate (BMR)
Some patients develop protrusion of eyeballs due to oedematous swelling of retrobulbar tissue (exophthalmos).
Hyperthyroidism Complications
- Tachycardia
- Atrial fibrillation
- Congestive heart failure
- Osteoporosis
- Ophthalmopathy
- Hyperthyroid crisis
Hyperthyroidism is commonly treated by the administration of anti-thyroid drugs, i.e. drugs that interfere with the synthesis of thyroxine.
Hypothyroidism
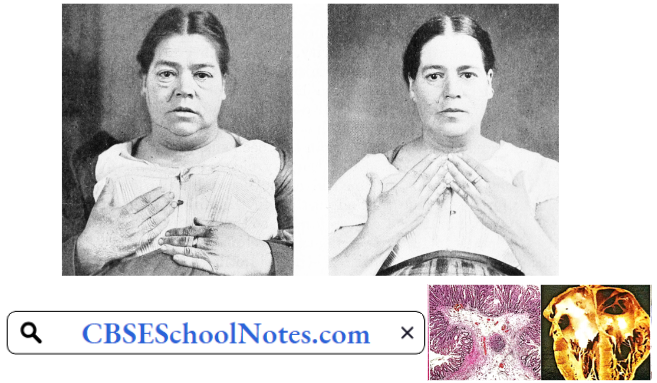
1. Adult Hypothyroidism (Myxoedema): This is a common disorder, especially in middle-aged females.
Hypothyroidism Aetiology: The most common cause of hypothyroidism is an autoimmune disorder known as Hashimoto’s thyroiditis. Autoimmune disorders occur when our immune system produces antibodies that attack our own tissues.
Hypothyroidism Pathology: Microscopically, the thyroid shows atrophic follicles, fibrosis, and diffuse lymphocytic infiltration.

Hypothyroidism Symptoms And signs: All the symptoms signs are the result of decreased plasma thyroxine levels on various tissues of the body.
- A puffy face is a characteristic finding. It is due to the accumulation of myxomatous gel in the subcutaneous tissue in the face.
- Slow heart rate
- Cold intolerance
- Increased body weight
- Muscle weakness
- Constipation
- Dry skin (lack of sweating)
- Decreased appetite
- Low BMR
- Somnolence
- High blood cholesterol
- Mental sluggishness
Hypothyroidism Complications
- Atherosclerosis
- Coronary artery disease
- Congestive heart failure
- Stroke
- Infertility
- Hypothermia
- Mental depression
- Myxoedema coma
Hypothyroidism is easily treated by oral administration of thyroxine.
2. Cretinism: This disorder results from a congenital deficiency of thyroxine. The child’s physical and mental growth is retarded leading to permanent mental deficit. The most common cause of cretinism is maternal iodine deficiency during pregnancy.
By the time the typical clinical picture develops in the infant, it is usually too late to reverse the mental retardation. The realization of this fact has led to the widespread use of iodized salt in India and many other countries.
3. Iodine-Deficiency Goitre: A dietary intake of at least 100-150 pg of iodide per day is required for normal thyroid function. Inadequate thyroid secretion occurs when iodide intake falls below 10 pg/ day. Due to the negative feedback mechanism, the secretion of TSH from the anterior pituitary is increased leading to hypertrophy of the thyroid gland.
The enlarged hypertrophied thyroid gland so produced is known as iodine-deficiency goiter. Use of iodized salt can prevent the disorder.
Disorders Of Sex Hormones
Testosterone Deficiency: It is hard to know how many men among us have testosterone deficiency (TD), although data suggest that overall about 2.1% may have TD. As few as 1% of younger men may have TD, while as many as 50% of men over 80 years old may have TD.
Disorders Of Sex Hormone Symptoms
- Reduced sex drive
- Reduced erectile function
- Loss of body hair
- Less beard growth
- Loss of lean muscle mass
- Feeling very tired all the time (fatigue)
- Symptoms of depression
Disorders Of Sex Hormones Causes
- Klinefelter syndrome (rare congenital defect)
- Damage to testicles by accident
- Removal of testicles because of cancer
- Aging
- Obesity
- Metabolic syndrome (high blood pressure, high blood sugar, unhealthy cholesterol levels, and belly fat)
- Use of medications such as antidepressants and narcotic pain medications
Erectile Dysfunction (Impotence): Erectile dysfunction is defined as the inability to attain a penile erection of sufficient rigidity for vaginal penetration. The prevalence of impotence increases rapidly after the age of 50 years, especially in those with diabetes mellitus or atherosclerosis.
Impotence may be due to severe hypogonadism which causes erectile failure as well as loss of libido (sexual interest and initiative). However, in most cases, the erectile dysfunction can be attributed to atherosclerosis of the penile blood vessels or autonomic neuropathy involving nervi erigentes. In some cases, impotence may be psychological.
Infertility: The failure to conceive after one year of unprotected intercourse is called infertility. It affects about 10% of married couples. The problem may be in the husband or the wife or both. The congenital causes of male infertility are not common.
More common causes of male infertility are acquired defects of the testes which include viral orchitis (mumps virus) and testicular trauma. The patient’s semen usually shows low sperm count and/or decreased sperm motility.
Low Oestrogen Levels
Low Oestrogen Levels Cause
- Turner syndrome (a rare congenital defect)
- Premature ovarian failure
- Thyroid disorders
- Excessive exercise
- Being severely underweight
- Low-functioning pituitary gland
Low Oestrogen Levels Symptoms
- Irregular periods.
- Infertility: Low estrogen levels can prevent ovulation and make getting pregnant difficult, leading to infertility.
Female Infertility: The absence of ovulation during the reproductive age of the female may result from isolated gonadotropin deficiency or primary ovarian failure. Blockade of fallopian tubes by pelvic inflammation is a fairly common cause of female infertility in spite of normal ovulatory ovarian cycles.