
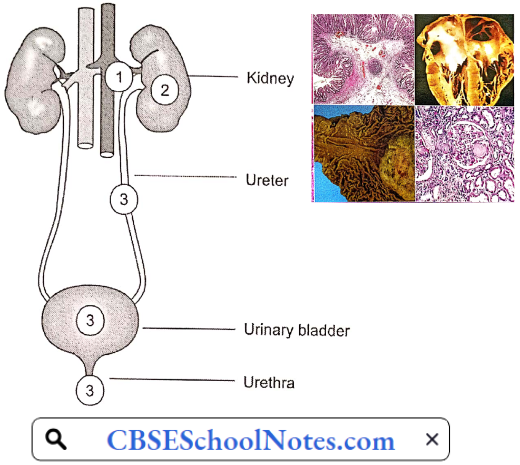
Disorders Of The Renal System
Kidney failure is defined as a condition when the kidneys are no longer able to remove the waste products from the body leading to their accumulation in the blood. This can cause unsafe levels of waste products to build up. This is known as kidney (or renal) failure. Unless it is treated, this can cause death. There are 2 main types of kidney (renal) failure: Acute (sudden) and chronic (over time).
Acute Renal Failure (ARF)
Acute renal failure is traditionally defined as an abrupt (within 48 hours) reduction in the rate of glomerular filtration, which manifests clinically as an abrupt and sustained increase in the serum levels of urea and creatinine with an associated disruption of salt and water homeostasis.
Read and Learn More Pathophysiology
The elevation of blood urea nitrogen (BUN) and serum creatinine levels is known as azotemia. Azotaemia is biochemical evidence of renal failure. (The normal range for blood urea is 20-40 mg/dl and the normal range for serum creatinine is 0.7-1.4 mg/dl.)
Symptoms Of Acute Renal Failure (ARF)
- Decrease in urine output (oliguria)
- Swelling of the hands, feet, and face (edema)
- Fatigue
- Nausea
- Confusion
- Seizures
- Coma
- Abnormal blood and urine tests
- High blood pressure
Pathogenesis Of ARF: Acute renal failure is classified as
- Pre-renal Azotaemia: It typically results from a severe decrease in renal blood flow due to severe blood loss leading to hypotension or severe dehydration. In this type of ARF, nephrons are normal. If blood volume is restored to normal, the patient makes a quick recovery.
- Renal Azotaemia: It occurs in response to cytotoxic, ischemic, or inflammatory insults to the kidney, with structural and functional damage to the nephrons. It is the most serious type of ARF. Recovery is slow.
- Post-renal Azotaemia: It includes disorders associated with obstruction of the urinary tract, for example, obstruction to the urethra by the enlarged prostate gland in males. Recovery is rapid after the removal of the obstruction.
With proper and timely treatment, most forms of ARI are reversible, since the kidney is a unique organ that can recover completely even after almost complete loss of renal function.
Prerenal Azotaemia
Prerenal Azotaemia Causes
- Hypovolemia: Hemorrhage, burns, dehydration, diuretics.
- Low Cardiac Output: Myocardial infarction, pulmonary embolism, CHF.
- Shock: Sepsis, anaphylaxis.
Prerenal azotemia represents the most common form (50 to 80%) of acute kidney failure and often leads to renal azotemia if it is not promptly corrected. All the conditions mentioned above cause renal hypoperfusion due to a decrease in the circulatory blood volume.
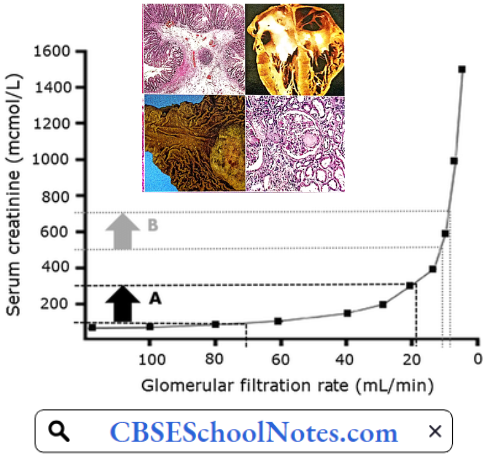
- A decrease in circulating blood volume activates high-pressure arterial baroreceptors leading to a reflex increase in sympathetic discharge, severe renal vasoconstriction, and a tendency to reduce GFR. When the renal hypoperfusion is severe, the renal compensatory mechanisms fail, resulting in a severe reduction in GFR and azotemia results.
- Blood levels of urea or creatinine begin to rise only when GFR falls to less than 50% of normal. Any further delay in the treatment of hypovolemia results in such an intense renal vasoconstriction that the renal tubular epithelium undergoes ischemic necrosis (acute tubular necrosis, ATN).
Renal Azotaemia: One specific clinical disorder called acute tubular necrosis (ATN) accounts for most of the cases of intrinsic azotemia. It is produced by injury to renal parenchyma.
Pathogenesis Of Acute Tubular Necrosis: Acute tubular necrosis (ATN) is the term used to designate acute kidney injury resulting from damage to the tubules. The major causes of ATN are
- Ischaemic: Resulting from a severe or protracted decrease in renal perfusion (a complication of prerenal azotemia).
- Nephrotoxicity: Resulting from a variety of exogenous drugs that damage the kidneys.
- Hemoglobinuria: In case of incompatible blood transfusion, there is severe intravascular hemolysis leading to hemoglobinuria. The presence of hemoglobin in the kidney damages the renal tubules.
Pathology: Regardless of the pathogenesis, ATN is characterized by a common set of morphological changes. These morphologic changes usually appear in a segmental pattern with some segments of the nephron, such as the proximal tubule and thick ascending loop of Henle which are more susceptible than other parts of the nephron.
Tubular Epithelium: The tubular epithelium undergoes necrosis which can be seen by denudation of tubular epithelial cells. In some cases, the tubular basement membrane may rupture.
Tubular Lumen: The denuded and necrotic tubular epithelial cells ultimately fall into the tubular lumen and often plug the tubule in the form of proteinaceous casts. When ATN is initiated by hemolysis, heme pigment may be precipitated in the luminal debris.
ATN is a life-threatening but reversible disorder, if the underlying source of injury (i.e. renal ischemia or presence of toxin) is corrected. The tubular epithelium rapidly recovers and renal function is restored.
Post-renal Azotaemia: Approximately 5-10% of cases of acute azotemia are due to obstruction to the urinary tract. Since normal kidney function can be achieved by a single kidney, post-renal azotemia can occur if there is
- Obstruction of bladder neck (prostate pathology) or urethra.
- Bilateral ureteric obstruction, or
- Unilateral ureteric obstruction in a patient with only one functioning kidney.
The prostatic disease is the most common cause of post-renal azotemia. Continued formation of urine against the backdrop of obstruction to outflow causes an increase in intraluminal pressure upstream of the site of obstruction. Thus, there is a gradual distension of ureters, renal pelvis, and calyces (hydronephrosis).

- Ultimately, when the intraluminal pressure in the Bowman’s capsule becomes equal to hydrostatic pressure in the glomerular capillaries, filtration ceases. Cessation in glomerular filtration leads to azotemia, acidosis, fluid overload, and hyperkalemia.
- Post-renal azotemia is the most common cause of complete anuria because the basic cause is mechanical. In pre-renal and renal types of ARI, complete renal shutdown seldom occurs.
- With the relief of obstruction within 48 hours of onset, there is evidence that relatively complete recovery of GFR can be achieved within a week. Prolonged obstruction can lead to tubular atrophy and irreversible renal fibrosis.
Chronic Renal Failure
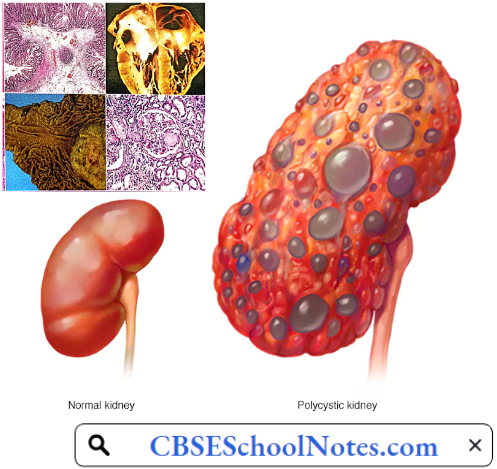
Chronic renal failure (CRF) refers to a decline in the glomerular filtration rate caused by a variety of diseases, such as diabetes, glomerulonephritis, and polycystic kidney disease. Patients with CRF have a high prevalence of hypertension.
Whether hypertension is a cause or a result of CRF remains debatable. Chronic renal failure is a continuous process that begins when some nephrons begin to be lost and ends when the remnant nephrons can sustain life no longer.
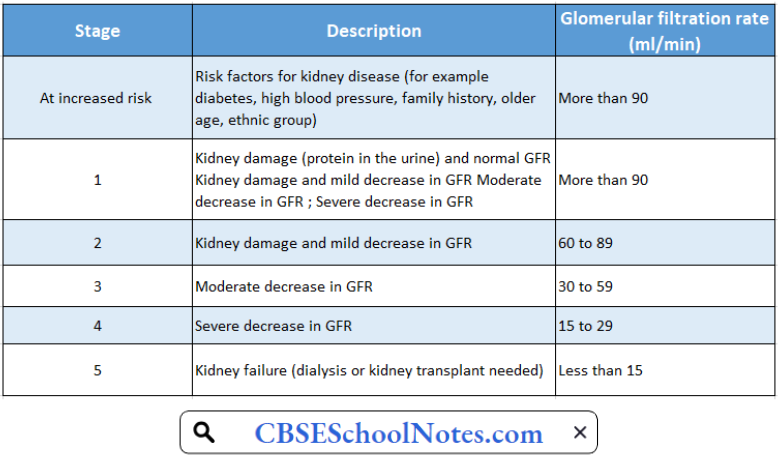
Chronic Renal Failure Classification: Staging of chronic kidney disease is a way of quantifying the severity of CKD. Chronic kidney disease has been classified into 5 stages. The end stage, when symptoms begin to appear, is known as uremia.
Stages Of Chronic Kidney Disease
Chronic Renal Failure Risk Factors: Factors that may increase the risk of chronic kidney disease include
- Diabetes
- High blood pressure
- Cardiovascular disease
- Smoking
Chronic Renal Failure Symptoms
- Nausea
- Vomiting
- Loss of appetite
- Fatigue and weakness
- Decreased mental sharpness
- Muscle twitches and cramps
- Swelling of feet and ankles
- Persistent itching
- Shortness of breath
- High blood pressure that is difficult to control
Aetiology
- Diabetes
- High blood pressure
- Glomerulonephritis, an inflammation of the kidney’s glomeruli
- Polycystic kidney disease
- Prolonged obstruction of the urinary tract, from conditions such as enlarged prostate, kidney stones, and some cancers
- Recurrent kidney infection, also called pyelonephritis
Pathology: The microscopic appearance of the “end-stage kidney” is similar regardless of cause, which is why a biopsy in a patient with chronic renal failure yields little useful information. The cortex is fibrotic, the glomeruli are sclerotic, there are scattered chronic inflammatory cell infiltrates, and the arteries are thickened. Tubules are often dilated and filled with pink casts.
Pathophysiology Of Uremia (End-Stage Renal Failure)
The most characteristic features of uremia are:
- Accumulation of nitrogenous waste products (urea, creatinine, uric acid, etc.) in the blood.
- Metabolic acidosis (due to failure of H+ excretion).
- Hyperkalaemia (due to failure of K+ excretion).
- Anemia (deficiency of erythropoietin).
- Uremic coma
The multiple organ failure in a uremic patient is due to the accumulation of some toxin(s) in the blood. However, the exact nature of the toxin(s) has not yet been identified. The final end product of carbohydrate and fat metabolisms is CO2 (and water), which can be easily excreted by the lungs.
The products of protein metabolism consist of a number of nitrogenous waste products which can be excreted only by the kidneys. Their accumulation in the blood consequent to renal failure is believed to be the cause of uremic toxicity.
- General Cellular Dysfunction: The most basic abnormality in uremia, at the cellular level, is partial inhibition of Na+– K+ pump, leading to a reduction in transmembrane potential, an increase in intracellular Na+, and a decrease in intracellular K+ concentrations. The most prominent result is an osmotically-induced overhydration of the cells.
- That is why salt and water retention is one of the important features of uremic syndrome. Overhydration of cerebral neurons is believed to be one of the factors contributing to the development of uremic encephalopathy.
- Additional factors decreasing intracellular K+ concentration include metabolic acidosis, poor dietary intake of K+, and excessive losses due to vomiting, diarrhea, or diuretics.
- Hypothermia: The sodium-potassium pump is the major consumer of ATP and hence the major cause of thermogenesis. Therefore, uremic patients have reduced energy metabolism, reduced BMR, subnormal body temperature, and an increased tendency to develop hypothermia.
- Anemia And Immune Dysfunction: Anemia is a regular feature of uremia. Normochromic normocytic anemia principally develops from decreased renal synthesis of erythropoietin, the hormone responsible for bone marrow stimulation for red blood cell production.
- Anemia associated with renal failure can be observed when the glomerular filtration rate (GFR) is less than 50 ml/min or when the serum creatinine is greater than 2 mg/dl. In the course of the disease, it becomes more severe as the GFR progressively decreases with the availability of less viable renal mass.
- Atrophy of lymphoid tissue leading to lymphopenia is common. The neutrophil count is usually normal. Uremic patients have impaired acute inflammatory response because of functional defects in neutrophils, monocytes, and lymphocytes. Therefore, uremic patients are more prone to infections. Clotting defects may also occur.
- Renal Osteodystrophy: In a uremic patient, a number of abnormalities Of the calcium, phosphate, and vitamin D metabolisms, such as hypocalcemia, hyperphosphatemia, increased PTH levels, and metabolic acidosis ultimately lead to renal bone disease (renal osteodystrophy).
- Renal osteodystrophy is characterized by areas of osteomalacia and osteoporosis and even osteosclerosis in various bones. These changes are seen more often in children or adults with slowly progressive chronic renal failure.
- Acidosis: Acidosis is another major metabolic abnormality associated with uremia. Metabolic acid-base regulation is controlled primarily by tubular cells of the kidney, while respiratory compensation is accomplished in the lungs. Failure to secrete hydrogen ions and impaired excretion of ammonium may initially contribute to metabolic acidosis.
- In uremia, metabolic acidosis may contribute to other clinical abnormalities, such as hyperventilation, anorexia, stupor, congestive heart failure, and muscle weakness. Uremic patients are likely to go into severe acidosis on exposure to exogenous acids, for example, high protein diet or endogenous acids such as lactic acid.
- Hyperkalemia: As renal function declines, the nephron is unable to excrete a normal potassium load, which can lead to hyperkalemia if dietary intake remains constant. In addition, other metabolic abnormalities, such as acidosis, may contribute to decreased potassium excretion and lead to hyperkalemia.
- The extracellular K+ concentration begins to rise progressively with the degree of azotemia. Serum K+ level of greater than 6.5 mEq/L is a clinical emergency.
- Cardiovascular Dysfunction: Left ventricular hypertrophy is a common disorder found in approximately 75% of patients of chronic renal failure who have not yet undergone dialysis. Left ventricular hypertrophy is associated with increased ventricular thickness, arterial stiffening, coronary atherosclerosis, and/or coronary artery calcification.
- Patients are at increased risk for cardiac arrhythmias due to underlying hyperkalemia and metabolic acidosis. Renal dysfunction may contribute to associated fluid retention, which may lead to uncontrolled hypertension and congestive heart failure.
- Fluid And Electrolyte Imbalance: In most cases of CRF, both total body sodium and water are increased and therefore the expansion of ECF volume may not be apparent. However, the patient is intolerant to both excessive salt intake and salt depletion. Excessive salt intake aggravates hypertension, congestive heart failure, ascites, or edema.
- Uremic patients also have impaired mechanisms for salt and water conservation. They are more prone to volume depletion in states of sodium loss (vomiting, diarrhea, fever) which may lead to orthostatic hypotension or circulatory shock. Volume depletion may produce further deterioration of renal function.
- Uremic Neuropathy: Uremic neuropathy is a distal sensorimotor polyneuropathy caused y uraemic toxins. The severity of neuropathy is correlated strongly with the severity of renal insufficiency. Paresthesias are the most common and usually the earliest symptom.
- Increased pain sensation is a prominent symptom. Weakness of lower extremities and atrophy follow the sensory symptoms. As disease progresses, symptoms move proximally and involve die upper extremities.
- Muscle cramps and restless legs syndrome were reported by 67% of uremic patients. Patients report that crawling, prickling, and itching sensations in their lower extremities are relieved partially by movement of the affected limb.
- Uremic Encephalopathy: Uremic encephalopathy (UE) is one of many manifestations of renal failure. Its exact cause is unknown. Accumulating metabolites of proteins and amino acids affect the entire neuraxis. No single abnormality can be precisely correlated with the clinical features of UE. Early symptoms include an inability to concentrate, drowsiness, and insomnia. Mild behavioral changes, loss of memory, and errors of judgment soon follow. Flapping tremors, chorea, stupor, seizures, and coma are seen in terminal stages.
- Malnutrition: Malnutrition usually occurs as renal failure progresses and is manifested by anorexia, weight loss, loss of muscle mass, low cholesterol levels, low BUN levels in the setting of an elevated creatinine level, and hypoalbuminemia.
- Co-morbid diseases, such as diabetes, congestive heart failure, or other diseases, that require reduced food intake or restrictions of certain foods may contribute to anorexia.
- Skin: The classic skin finding in persons with uremia is uraemic frost, which is a fine residue, thought to consist of excreted urea left on the skin after evaporation of water. Patients may become hyperpigmented as uremia worsens.
- Uremic pruritus remains one of the most frustrating, common, and potentially disabling symptoms in patients with end-stage renal disease. The exact cause is not yet clear.
Hemodialysis: Hemodialysis can be a life-saving measure in many types of acute renal failure produced by reversible pathological processes. Patients with chronic renal failure can also be kept alive for months or even years.
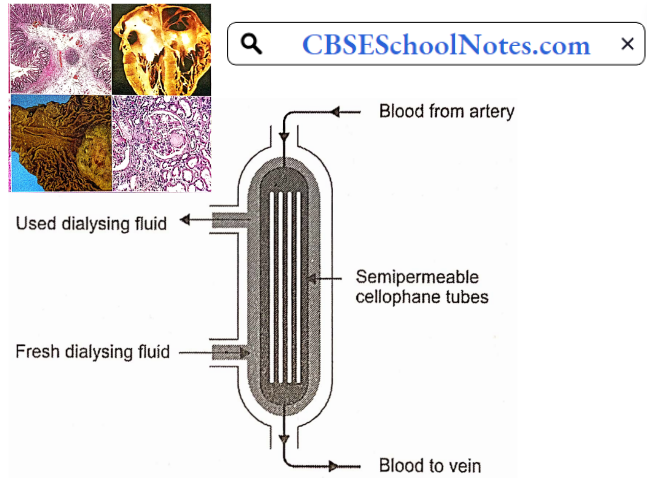
During hemodialysis, the patient’s radial artery is connected to a long and coiled cellophane tube immersed in a dialyzing fluid. The chemical composition of the dialyzing fluid is similar to that of plasma except that it is free of waste products, like urea, uric acid, etc.
Composition Of Dialyzing Fluid As Compared To That Of A Typical Uremic Plasma
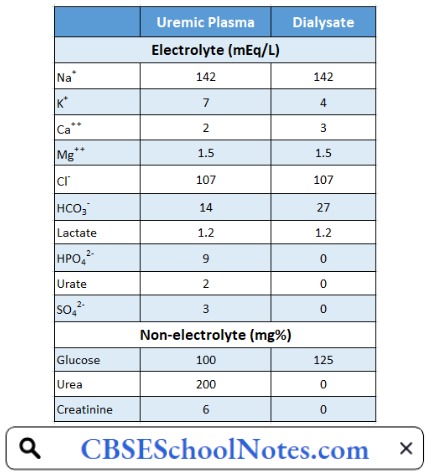
The patient’s blood passes through the dialyzing system and returns to a peripheral vein. The semipermeable cellophane membrane permits free diffusion of all the constituents of plasma except proteins. In this way, the dialysis of patient blood removes the toxic waste products and restores normal electrolyte concentration in the plasma. The dialyzing system is also known as the artificial kidney.
Hemodialysis is an expensive procedure and needs to be repeated almost every week. Therefore, it cannot be regarded as a remedy for irreversible renal failure caused by chronic renal diseases. With the recent advances in medical technology, such patients are treated by renal transplantation.