Class 12 Physics Chapter 2 Electrostatic Potential And Capacitance Multiple Choice Questions
Question 1. The electric potential a; a point on the axis of a short electric dipole, at a distance x from the midpoint of the dipole is proportional to
- \(\frac{1}{x}\)
- \(\frac{1}{x^3/2}\)
- \(\frac{1}{y^3}\)
- \(\frac{1}{x^2}\)
Answer: 4. \(\frac{1}{x^2}\)
V = \(\frac{k p \cos θ}{r^2}\)
Read and Learn More Important Questions for Class 12 Physics with Answers
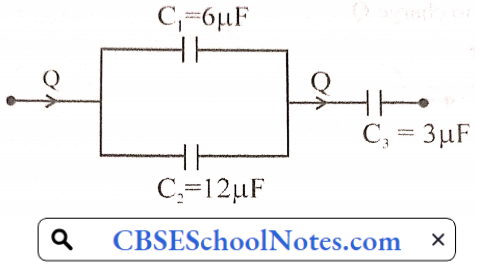
Question 2. In the given network all capacitors used are identical and each one is of capacitance C. Which of the following is the equivalent capacitance between the points A and B?
- 6 C
- 5/2 C
- 3/2 C
- 5/6 C
Answer: 3. 3/2 C

Question 3. A particle having a mass 1 g and an electric charge 10-8 C travels from point A having an electric potential of 600 V to point B having zero potential. What would be the change in its kinetic energy?
- \(-6 \times 10^{-6} \mathrm{erg}\)
- \(-6 \times 10^{-6} \mathrm{~J}\)
- \(6 \times 10^{-6} \mathrm{~J}\)
- \(6 \times 10^{-6} \mathrm{crg}\)
Answer: 3. \(6 \times 10^{-6} \mathrm{~J}\)
ΔK = \(\mathrm{W}=\mathrm{q}\left(\mathrm{V}_1-\mathrm{V}_2\right)\)
= \(10^{-8}(600-0)\)
= \(6 \times 10^{-6} \mathrm{~J}\)
Physics Class 12 Chapter 2 Important Questions PDF
Question 4. The energy of a charged capacitor is U, Now it is removed from a battery and then is connected to another identical uncharged capacitor in parallel. What will be the energy of each capacitor now,
- 3U/2
- U
- U/4
- U/2
Answer: 3. U/4

U, Q, C, V
U = \(\frac{Q^2}{2C}\)….(1)
Now,
In parallel, the charge will same equal to \(\frac{Q}{2}\) on each capacitor.
So, \(U^{\prime}=\frac{Q^2}{2 C}=\frac{\left(\begin{array}{c}\mathrm{Q} \\ 2\end{array}\right)^2}{2 \mathrm{C}}=\frac{\mathrm{Q}^2}{8 \mathrm{C}}\)…(2)
So, \(\frac{U^{\prime}}{U}=\frac{1}{8} \times 2=\frac{1}{4}\)
⇒ \(U^{\prime}=\frac{U}{4}\)
Question 5. The capacitance of a variable capacitor joined with the batten of 100 V is changed from 2μF to 10μF. What is the change in the energy stored in it?
- \(2 \times 10^{-2} \mathrm{~J}\)
- \(2.5 \times 10^{-2} \mathrm{~J}\)
- \(6.5 \times 10^{-2} \mathrm{~J}\)
- \(4 \times 10^{-2} \mathrm{~J}\)
Answer: 4. \(4 \times 10^{-2} \mathrm{~J}\)
U = \(\frac{1}{2} \mathrm{CV}^2\)
Δ U =\(\frac{1}{2} C_2 V^2-\frac{1}{2} C_1 V^2\)
= \(\frac{1}{2} \times 100 \times 100(10-2) \times 10^{-6}=4 \times 10^{-2} J\)
Question 6. The distance between electric charges Q C and 9 Q C is 4 m. What is the electric potential at a point of the line joining them where the electric field is zero?
- 4 kQ V
- 10 kQ V
- 2 kQ V
- 2.5 kQ V
Answer: 1. 4 kQ V
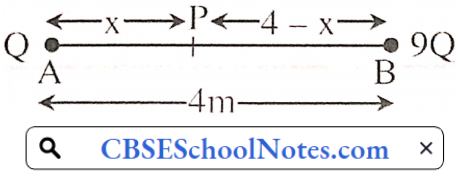
The electric field at P is zero \(\frac{k Q}{x^2}=\frac{k(9 Q)}{(4-x)^2}\)
⇒ \(9 x^2=(4-x)^2 \Rightarrow 3 x=4-x\)
x=1 m
So \(V=\frac{k Q}{(1)}+\frac{k(9 Q)}{3}=k Q+3 k Q=4 k Q\) volt
Question 7. For a capacitor, the distance between two plates is 5v and the electric field between them is E0. Now a dielectric slab having dielectric constant 3 and thickness v is placed between them in contact with one plate. In this condition, the potential difference between the two plates is
- \(15 \mathrm{E}_0 \mathrm{X}\)
- \(7 E_0 x\)
- \(\frac{13 E_0 x}{3}\)
- \(\frac{9 E_0 \mathrm{x}}{2}\)
Answer: 3. \(\frac{13 E_0 x}{3}\)
V = \(E_0(5 x-x)+E_m \times x\)
= \(E_0(4 x)+\frac{E_{01}}{3} x\left[E_m=\frac{E_0}{c_t}\right]\)
⇒ \(\frac{13 E_0 x}{3}\)
Physics Class 12 Chapter 2 Important Questions PDF
Question 8. A Point P is 40 m away from the 20 μC point charge and 20 m from the 4 μC point charge. The electric potential al P is V. (k = 9 x 109 Nm² C-2]
- 1300
- 6300
- 2700
- 4500
Answer: 2. 6300
V = \(\frac{k \times 20 \mu \mathrm{C}}{40}+\frac{k \times 4 \mu \mathrm{C}}{20} \Rightarrow \frac{28 \mathrm{k}}{40} \mu \mathrm{C} \)
= \(\frac{7}{10} \times 9 \times 10^9 \times 10^{-6}\)
V = \(6300 \text { volt }\)
Question 9. If a capacitor having a capacitance of 1200 μF is charged at a uniform rate of 100 μC/s, what is the time required to increase its potential by 20 volts?
- 500 s
- 6000 s
- 240 s
- 120 s
Answer: 3. 240 s
q = C V
V = \(\frac{q}{C}\)
⇒ \(\frac{\Delta V}{\Delta t}=\frac{1}{C} \frac{\Delta q}{\Delta t}\)
⇒ \(\frac{20}{t}=\frac{1}{1200 \mu F} \times 100 \frac{\mu C}{s}\)
t = \(\frac{1200 \times 20}{100}=240 \mathrm{sec}\)
Question 10. For uniform electric field \(\vec{E}=E_0(\hat{j})\), if the electric potential at y = 0 is zero, then the value of electric potential at y = +y will the
- -yE0
- yE0
- y²E0
- -y²E0
Answer: 1. -yE0
⇒ \(\int \mathrm{dV}=-\int \mathrm{Edr}\)
⇒ \(\int_0^1 \mathrm{dV}=-\mathrm{E}_0 \int_0^\gamma \mathrm{dy}\)
⇒ \(\mathrm{V}=-\mathrm{E}_0 \mathrm{y}\)
Physics Class 12 Chapter 2 Important Questions PDF
Question 11. Equipolcnlial Surface through a point is _____ to the electric field at that point.
- Normal
- Parallel
- At an angle of 45°
- At an angle of 30°
Answer: 1. Normal
Question 12. A particle having charge ‘q’ is accelerated with a potential difference ΔV it would gain energy of______
- q ΔV²
- q²ΔV
- qΔV
- q²ΔV²
Answer: 3. qΔV
Question 13. In a parallel plate capacitor, the area of each plate A 1 m² and the distance between two plates d = 1 mm. Then the capacitance of a capacitor C = ____ F.
- 8.85 x 10-12
- 8.85 x 10-9
- 8.85 x 10-6
- 8.85 x 10-15
Answer: 2. 8.85 x 10-9
C = \(\frac{\varepsilon_0 \mathrm{~A}}{\mathrm{~d}}\)
= \(\frac{8.85 \times 10^{-12} \times 1}{1 \times 10^{-3}}=8.85 \times 10^{-9} \mathrm{~F}\)
Physics Class 12 Chapter 2 Electrostatic Potential And Capacitance Assertion And Reason Type Questions And Answers
For question numbers 14 to 18 two statements are given-one labelled Assertion (A) and the other labelled Reason (R). Select the correct answer to these questions from the codes (1), (2), (3), and (4) as given below.
- Both A and R are true and R is the correct explanation of A
- Both A and R are true but R is NOT the correct explanation of A
- A is true but R is false
- A is false and R is also false
Question 1. Assertion: Electrons move away from a low potential to a high potential region.
Reason: Because electrons have a negative charge.
Answer: 1. Both A and R are true and R is the correct explanation of A
Question 2. Assertion: The capacity of a given conductor remains the same even if the charge is varied on it.
Reason: Capacitance depends upon nearly medium as well as the size and shape of the conductor.
Answer: 1. Both A and R are true and R is the correct explanation of A
Question 3. Assertion: A conductor having equal positive charge and volume, must also have the same potential.
Reason: Potential depends only on the charge and volume of the conductor.
Answer: 4. A is false and R is also false
Question 4. Assertion: A metallic shield in the form of a hollow shell may be built to block an electric field.
Reason: In a hollow spherical shell, the electric field inside it is zero at every point.
Answer: 1. Both A and R are true and R is the correct explanation of A
Question 5. Assertion: When charges are shared between any two bodies no charge is really lost, some loss of energy does occur.
Reason: Some energy disappears in the form of heat.
Answer: 1. Both A and R are true and R is the correct explanation of A
Physics Class 12 Chapter 2 Electrostatic Potential And Capacitance Short Answer Type Questions
Question 1. A 600 pF capacitor is charged by a 200V supply. It is then disconnected from the supply and connected to another uncharged 600 pF capacitor. How much electrostatic energy is lost in the process?
Answer:
Energy loss
ΔU = \(\frac{1}{2} \frac{C_1 C_2}{C_1+C_2}\left(V_1-V_2\right)^2\)
= \(\frac{1}{2} \frac{600 \times 600 \times 10^{-24}}{(600+600) \times 10^{12}}(200-0)^2\)
= \(\frac{1}{2} \times \frac{60(0 \times 600}{1200} \times 10^{-12} \times 4 \times 10^4\)
= \(6 \times 10^{-6} \mathrm{~J}\)
Question 2. A slab of material of dielectric constant K has the same area as the plates of a parallel-plate capacitor but has a thickness (3/4)d, where d is the separation of the plates. How is the capacitance changed when the slab is inserted between the plates?
Answer:
C = \(\frac{\varepsilon_0 A}{(d-1)+\frac{1}{K}}=\frac{\varepsilon_0 A}{\left(d-\frac{3}{4} d\right)+\frac{3 d}{4 K}}=\frac{\varepsilon_0 A}{d\left(1+\frac{3}{K}\right)}\)
Here \(\left(C_0=\frac{\varepsilon_0 A}{d}\right)\)
C = \(\frac{4 K C_0}{K+3}\)
Question 3. Four point charges Q, q. Q and q are placed at the corners of a square of side ‘a’ as shown in the figure.
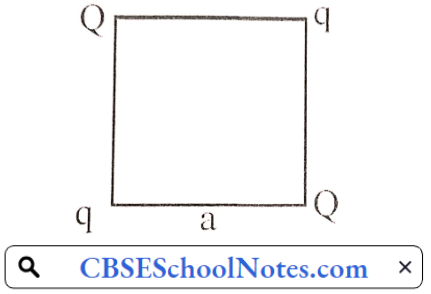
Find the potential energy of this system.
Answer:
The potential energy of the system
U = \(\frac{1}{4 \pi \varepsilon_0}\left[4 \frac{q Q}{a}+\frac{q^2}{a \sqrt{2}}+\frac{Q^2}{a \sqrt{2}}\right]\)
= \(\frac{1}{4 \pi \varepsilon_0 a}\left[4 q Q+\frac{q^2}{\sqrt{2}}+\frac{Q^2}{\sqrt{2}}\right]\)
Question 4. Two charges 3 x 10-8 C and -2 x 10-8 C are located 15 cm apart. At what point on the line joining the two charges is the electric potential zero? Take the potential at infinity to he zero.
Answer:
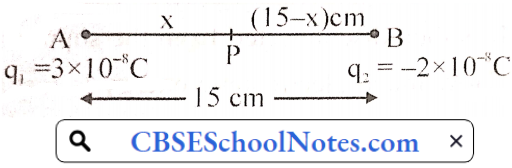
Let at point P potential is zero
Vp = V1 + V2= 0
⇒ \(V_F=\frac{k q_1}{x}+\frac{k q_2}{(15-x)}=0\)
⇒ \(V_f=k\left[\frac{3 \times 10^{-k}}{x}-\frac{2 \times 10^{-x}}{(15-x)}\right]=0\)
⇒ \(\frac{3 \times 10^{-x}}{x}=\frac{2 \times 10^{-x}}{(15-x)}\)
⇒ 45 – 3x = 2x
⇒ x = 9cm
Question 4. Three capacitors of capacitance C1, C2, and C3 are connected in series to a source of V volt. Show that the total energy stored in the combination of capacitors is equal to the sum of the energy stored in individual capacitors.
Answer:
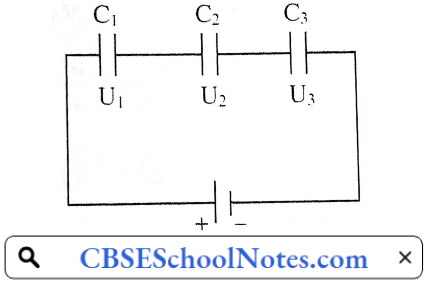
So. w.k.t. electric energy stored in the capacitor
U = \(\frac{\mathrm{Q}^2}{2 \mathrm{C}}\) (Series combination Q → constant)
⇒ \(\mathrm{U}_1=\frac{\mathrm{Q}^2}{2 \mathrm{C}_1} \cdot \mathrm{U}_2=\frac{\mathrm{Q}^2}{2 \mathrm{C}_2} \cdot \mathrm{U}_3=\frac{\mathrm{Q}^2}{2 \mathrm{C}_3}\)
So, Total energy \(\mathrm{U}_1+\mathrm{U}_2+\mathrm{U}_3=\frac{\mathrm{Q}^2}{2}\left(\frac{1}{\mathrm{C}_1}+\frac{1}{\mathrm{C}_2}+\frac{1}{\mathrm{C}_2}\right)\)
In Series Combination w.k.t. \(\frac{1}{C_{\text {eq}}}=\frac{1}{C_1}+\frac{1}{C_2}+\frac{1}{C_3}\)
So, \(U_1+U_2+U_3=\frac{Q^2}{2 C_{\text {eq}}}\)
⇒ \(\mathrm{U}_1+\mathrm{U}_2+\mathrm{U}_1=\mathrm{U}_{1 \text { Total }}\)
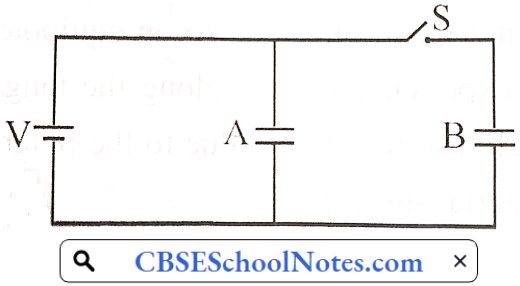
Question 5. Two identical parallel plate capacitors A and B are connected to a batter of V volts with switch S closed. The switch is now opened and the free space between the plates of the capacitors is filled with a dielectric of dielectric constant K. Land the ratio of the total electrostatic energy stored in both capacitors before and alter the introduction of the dielectric.
Answer:
When switch ‘S’ is closed, the initial energy (Ei) of the system, \(\mathrm{E}_{\mathrm{i}}=\frac{1}{2} \mathrm{CV}^2+\frac{1}{2} \mathrm{CV}^2=\mathrm{CV}^2\)
If \(\frac{1}{2} \mathrm{CV}^2=\mathrm{U} \text {. then } \mathrm{E}_{\mathrm{i}}=\mathrm{CV}^2=2 \mathrm{U}\)….(1)
When switch ‘S’ is opened then capacitor ‘A’ gets a constant supply of voltage (V) and on the other hand, charge ‘Q’ becomes constant in capacitor ‘B’.
∴ In the above situation, if the dielectric of strength ‘K’ is filled, we may write.
The final energy of the system as \(\mathrm{E}_{\mathrm{f}}=\frac{1}{2}(\mathrm{KC}) \mathrm{V}^2+\frac{1}{2}\left(\frac{\mathrm{Q}^2}{\mathrm{KC}}\right)\)
or, \(\mathrm{E}_{\mathrm{f}}=\mathrm{KU}+\frac{\mathrm{U}}{\mathrm{K}}=\mathrm{U}\left(\frac{\mathrm{K}^2+1}{\mathrm{~K}}\right)\)
because \(\frac{1}{2} \mathrm{CV}^2=\frac{1}{2} \frac{\mathrm{Q}^2}{\mathrm{C}}=\mathrm{U}\)
Now, \(\frac{\mathrm{E}_{\mathrm{i}}}{\mathrm{E}_{\mathrm{f}}}=\frac{2 \mathrm{U}(\mathrm{K})}{\mathrm{U}\left(\mathrm{K}^2+1\right)}=\frac{2 \mathrm{~K}}{\mathrm{~K}^2+1}\)
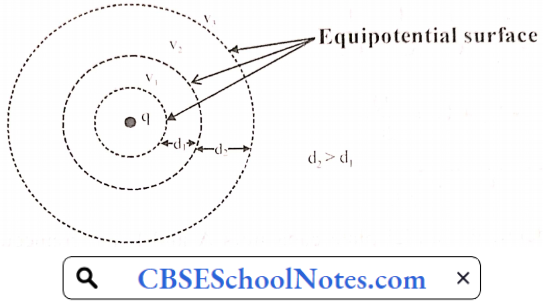
Question 6. Define an equipotential surface. Draw equipotential surfaces
- In the case of a single-point charge.
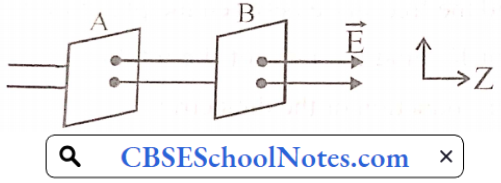
- In a constant electric field in Z-direction.
- Can an electric field exist tangential to an equipotential surface? Give reason.
Answer:
An equipotential surface is a surface that has equal potential at every point it. The net work done in moving a charge from one point to another on this surface is zero.
1. A point charge
2.
3. A number of electric fields cannot exist tangential to an equipotential surface. If it happens then a charged particle will experience a force along the tangential line and can move along it. Since a charged particle can move only due to the potential difference, this contradicts the concept of an equipotential surface.
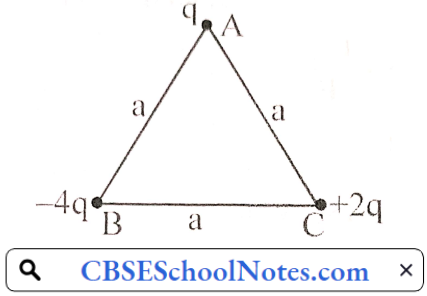
Question 7. Obtain an expression for the work done to dissociate the system of three charges placed at the vertices of an equilateral triangle of side ‘a’ as shown below.
Answer:
The total electrostatic potential energy of the system
U = \(U_{A B}+U_{B C^C}+U_{C A}=k\left[\frac{q(-4 q)}{a}+\frac{(-4 q)(2 q)}{a}+\frac{q(2 q)}{a}\right]=-k \times \frac{10 q^2}{a}\)
∴ Work done to dissociate the system W = -U
W = \(\frac{1}{4 \pi \varepsilon_0} \times \frac{10 q^2}{a}\)
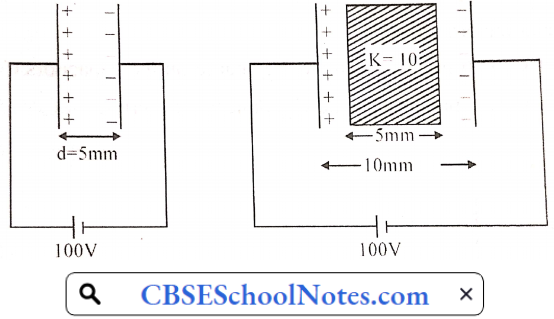
Question 8. A 200 μF parallel plate capacitor having a plate separation of 5 mm is charged by a 100 V dc source. It remains connected to the source. Using an insulated handle, the distance between the plates is doubled and a dielectric slab of thickness 5 mm and dielectric constant 10 is introduced between the plates. Find
- Capacitance,
- The electric field between the plates,
- The energy density of the capacitor will change?
Answer:
As we know for a capacitor C = \(\frac{\varepsilon_0 \mathrm{~A}}{d}\)
and for a capacitor partially filled with dielectric, capacity is C = \(\frac{\varepsilon_0 A}{(d-1)+\frac{1}{K}}\)
here, we may consider the term [(d – t) + \(\frac{1}{K}\)] as effective distance, which can be calculated for the present situation as,
⇒ \(\mathrm{d}_{\mathrm{eff}}=(2 \mathrm{~d}-\mathrm{t})+\frac{\mathrm{t}}{\mathrm{K}}=2 \times 5-5+\frac{5}{10}=5.5 \mathrm{~mm}\)
Thus,
1. Effective new capacitance = \(200 \mu \mathrm{F} \times \frac{5 \mathrm{~mm}}{5.5 \mathrm{~mm}}=\frac{2000}{11} \mu \mathrm{F}\)
= \(182 \mu \mathrm{F} \text { as } \rightarrow \frac{\mathrm{C}_{\text {eff }}}{\mathrm{C}}=\frac{\mathrm{d}}{\mathrm{d}_{\text {eff }}}=\frac{\mathrm{E}_{\text {eff }}}{\mathrm{E}}\)
2. Effective new electric field = \(\frac{100}{5.5 \times 10^{-3} \mathrm{~m}}=\frac{200000}{11} \simeq 18182 \mathrm{~V} / \mathrm{m}\)
3. \(\frac{\text { New energy Stored }}{\text { Original energy Stored }}=\frac{{ }_2^1 \mathrm{C}_{\mathrm{eff}} \mathrm{V}^2}{{ }_2^1 \mathrm{CV}^2}=\frac{\mathrm{C}_{\mathrm{eff}}}{\mathrm{C}}=\frac{10}{1 \mathrm{I}}\)
Thus, the new energy density will be (10/11)² of the original energy density = 100/121 times
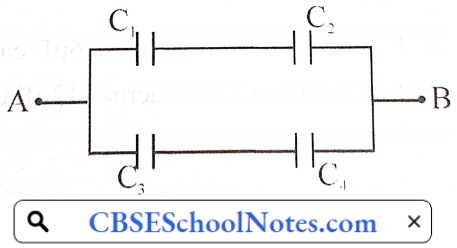
Question 9. In a network, four capacitors C1, C2, C3, and C4 are connected as shown
- Calculate the net capacitance in the circuit.
- If the charge on the capacitor C1 is 6 μC,
- Calculate the charge on the capacitors C3 and C4, and
- Net energy is stored in the capacitors C3 and C4 connected in series.
Answer:
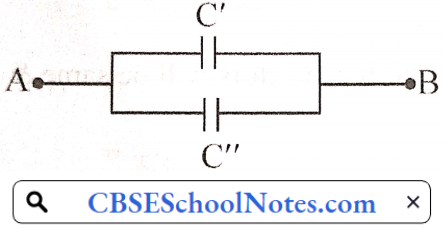
1. Equivalent capacitance of C1 and C2
C” = C1 + C2
C’ = 9μF
Equivalent capacitance of the circuit \(\frac{q_3^2}{2 C_3}+\frac{q_4^2}{2 C_4} \quad\left\{q_4=q_3\right\}\)
U = \(\frac{q_3^2}{2}\left[\frac{1}{C_3}+\frac{1}{C_4}\right]=\frac{18 \times 18}{2}\left[\frac{C_4+C_3}{C_3 \times C_4}\right]\)
U = \(\frac{18 \times 18}{2}\left[\frac{16}{12 \times 4}\right] \Rightarrow U=54 \mu \mathrm{J}\)
Question 10. Calculate the equivalent capacitance between points A and B in the circuit below. If a battery of 10 V is connected across A and B. calculate the charge drawn from the battery.
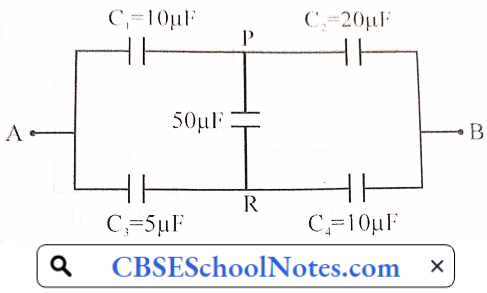
Answer:
The above circuit is a balanced Wheatstone bridge. So there is no flow of current in 50 uμF capacitor (between P and R). so this capacitor will not play any role in the circuit.
∴ modified circuit is ⇒
C1 ,C2 are in scries \(\frac{1}{C^{\prime}}=\frac{1}{10 \mu \mathrm{F}}+\frac{1}{20 \mu \mathrm{F}} \Rightarrow \mathrm{C}^{\prime}=\frac{20}{3} \mu \mathrm{F}\)
C3, C4 are in series
Now, \(C^{\prime \prime}=\frac{1}{5 \mu \mathrm{F}}+\frac{1}{10 \mu \mathrm{F}} \Rightarrow \mathrm{C}^{\prime \prime}=\frac{10}{3} \mu \mathrm{F}\)
Equivalent capacitance of the circuits C” + C”
⇒ \(C_{\mathrm{eq}}=\frac{20}{3}+\frac{10}{3}=10 \mu \mathrm{F}\)
Now, charge drawn from the battery
V = 10 volt (given)
Q = Ceq V ⇒ Q = 10 x 10 x 10-6= 10-4 C
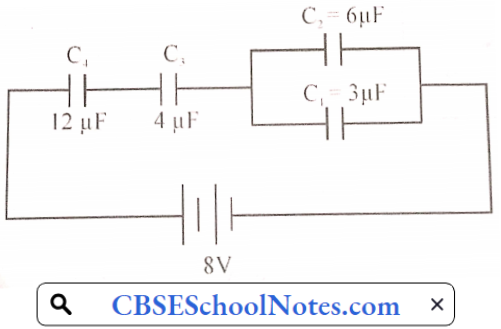
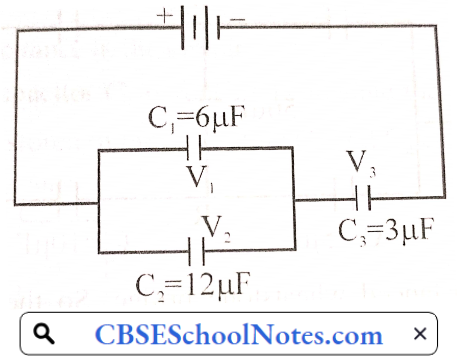
Question 11. In the following arrangement of capacitors, the energy stored in the 6 pF capacitor is E. Find the value of the following :
- Energy is stored in a 12 μF capacitor.
- Energy is stored in 3 μF capacitor.
- Total energy drawn from the battery
Answer:
1. Let the EMF of the applied battery be V.
Energy stored in 6 μF capacitor = E (given)
Energy stored in a capacitor is given by
U = \(\frac{1}{2} \mathrm{CV}^2 \Rightarrow \mathrm{V}=\sqrt{\frac{2 \mathrm{U}}{\mathrm{C}}}\)
Here \(V_1=V_2\)
⇒ \(V_1 \Rightarrow \text { Potential difference across } 6 \mu \mathrm{F} \text { capacitor }\)
⇒ \(V_2 \Rightarrow \text { Potential difference across } 12 \mu \mathrm{F} \text { capacitor }\)
⇒ \(\sqrt{\frac{2 \mathrm{E}_1}{\mathrm{C}_1}}=\sqrt{\frac{2 \mathrm{E}_2}{\mathrm{C}_2}}\)
⇒ \(\mathrm{E}_1=\mathrm{E} \text { (given) }\)
⇒ \(\mathrm{E}_2=\frac{\mathrm{C}_2}{\mathrm{C}_1} \times \mathrm{E}_1 \Rightarrow \mathrm{E}_2=\frac{12}{6} \times \mathrm{E} \Rightarrow \mathrm{E}_2=2 \mathrm{E}\)
2. Energy stored in 12 μF capacitor (E2) = 2E
The total energy of a parallel combination of capacitors is the sum of the energy of both capacitors.
⇒ E + 2E = 3E
So, \(\frac{Q^2}{2 C_{c i}}=3 E \Rightarrow Q=\sqrt{2 C_{c i} \times 3 E}\)
The same charge (Q) flows through 3μF capacitor. So energy stored by a capacitor of 3 μF
⇒ \(\mathrm{E}_3=\frac{\mathrm{Q}^2}{2 \mathrm{C}_3}=\frac{2 \mathrm{C}_{\mathrm{ct} .} \times 3 \mathrm{E}}{2 \mathrm{C}_3} \Rightarrow \mathrm{E}_3=\frac{2 \times 18 \times 3 \mathrm{E}}{3 \times 2}\)
⇒ \(\mathrm{E}_3=18 \mathrm{E}\)
Total energy stored \(=\mathrm{E}_1+\mathrm{E}_2+\mathrm{E}_3\)
= E + 2E+ 18 E = 21 E
Thus, the energy is given by the battery = 2 x 21E = 42E
[As half part of the total energy given by the battery is stored in capacitors]
Question 12. Find the ratio of the potential differences that must be applied across the series and parallel combination of two capacitors C1 and C2 with their capacitances in the ratio 1: 2 so that the energy stored in the two eases becomes the same
Answer:
Let C1 =x and C2 = 2x
Equivalent capacitance in series combination \(C_{\mathrm{S}}=\frac{\mathrm{C}_1 \mathrm{C}_2}{\mathrm{C}_1+\mathrm{C}_2}=\frac{\mathrm{x} \times 2 \mathrm{x}}{\mathrm{x}+2 \mathrm{x}}=\frac{2 \mathrm{x}}{3}\)
∴ \(\mathrm{C}_{\mathrm{s}}=\frac{2 \mathrm{x}}{3}\)
Equivalent capacitance in parallel combination
CP = C1 + C2 = x + 2x = 3x
Now given that energy stored in series combination = Energy stored in parallel combination
⇒ \(\frac{1}{2} C_s V_1^2=\frac{1}{2} C_p V_2^2 \Rightarrow \frac{1}{2} \times\left(\frac{2 x}{3}\right) V_1^2=\frac{1}{2} \times 3 x \times V_2^2 \Rightarrow \frac{V_1}{V_2}=\frac{3}{\sqrt{2}}\)
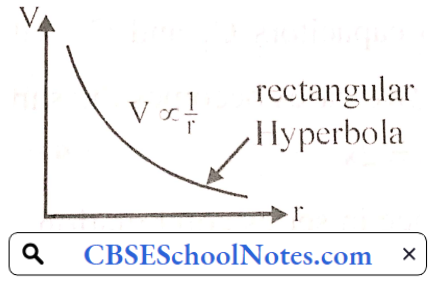
Question 13. Write the definition of electric potential. Calculate the electric potential due to a point charge Q at a distance r from it. Draw a graph between electric potential V and distance r for a point charge Q.
Answer:
Electric potential: The amount of work needed to bring a unit positive charge from infinity to a specific point inside the electric field of a positive charge is called electric potential at that point.
Potential due to point charge: Electrostatic force on + q0 at point A due to charge Q
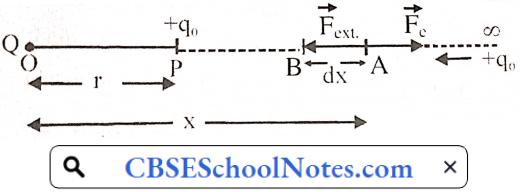
⇒ \(\mathrm{F}_{\mathrm{c}}=\frac{1}{4 \pi \varepsilon_0} \frac{\mathrm{Q} \mathrm{q}_0}{\mathrm{x}^2}\)
Work done in moving a charge +q0 in short displacement from A to B
dW = \(\mathrm{F}_c \mathrm{dx}=-\frac{\mathrm{Qq}_0}{4 \pi \varepsilon_0} \times \frac{1}{\mathrm{x}^2} \mathrm{dx}\)
Total work done in moving a charge q0 from ∞ to r
W = \(-\frac{\mathrm{Qq}_0}{4 \pi \varepsilon_0} \int_0^{\mathrm{r}} \frac{1}{\mathrm{x}^2} \mathrm{dx}\)
W = \(-\frac{\mathrm{Qq_{0 }}}{4 \pi \varepsilon_0}\left[-\frac{1}{\mathrm{x}}\right]^{\mathrm{r}}_{\mathrm{∞}}\)
W = \(\frac{\mathrm{Qq_{0 }}}{4 \pi \varepsilon_0}\left[\frac{1}{\mathrm{r}}-\frac{1}{\infty}\right]^{\mathrm{r}}_{\mathrm{∞}} \Rightarrow \mathrm{W}=\frac{\mathrm{Qq_{0 }}}{4 \pi \varepsilon_{0} \mathrm{r}}\)
From the definition of potential
V = \(\frac{W}{q_0} \Rightarrow V=\frac{1}{4 \pi \epsilon_0} \frac{Q}{r}\)
V = \(\frac{k Q}{r} \Rightarrow V \propto \frac{1}{r}\)
Physics Class 12 Chapter 2 Electrostatic Potential And Capacitance Long Answer Type Questions
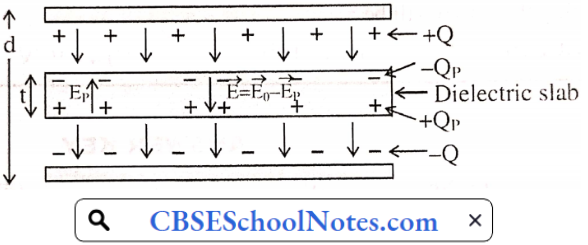
Question 1. A dielectric slab is a substance that does not allow the flow of charges through it but permits it to exert electrostatic forces on one another. When a dielectric slab is placed between the plates, the field E0 polarises the dielectric. This induces charge -QP on the upper surface and +QP on the lower surface of the dielectric. These induced charges set up a field EP inside the dielectric in the opposite direction of E0 as shown.
1. In a parallel plate capacitor, the capacitance increases from 4μF to 80μF upon introducing a dielectric medium what is the dielectric constant of the medium?
- 10
- 20
- 50
- 100
Answer: 2. 20
2. A parallel plate capacitor with air between the plates has a capacitance of 8 pF. The separation between the plates is now reduced by half and the space between them is filled with a medium of dielectric constant 5. Calculate the value of capacitance of the capacitor in the second case.
- 8pF
- 10pF
- 80pF
- 100pF
Answer: 3. 80pF
3. A dielectric introduced between the plates of a parallel plate capacitor :
- Increases the electric field between the plates
- Decreases the capacity of the capacitor
- Increases the charge stored in the capacitor
- Increases the capacity of the capacitor
Answer: 4. Increases the capacity of the capacitor
4. A parallel plate capacitor of capacitance 1 pF has separation between the plates is d. When the distance of separation becomes 2d and wax of dielectric constant x is inserted in it the capacitance becomes 2 pF. What is the value of x?
- 2
- 4
- 6
- 8
Answer: 2. 4
Quetsion 2. The electrostatic potential of a charged body represents the degree of electrification of the body. It determines the flow of electric charge between two charged bodies placed in contact with each other. The charge always flows from a body of higher potential to another body at lower potential. The flow of charge stops as soon as the potential of the two bodies becomes equal. Now answer the following.
1. A uniform electric field of 100 N/C exists vertically upward direction. The decrease in electric potential as one goes up through a height of 5cm is :
- 20V
- 120V
- 5V
- Zero
Answer: 3. 5V
2. Work done to bring a unit positive charge unaccelerated from infinity to a point inside the electric field is called
- Electric Field
- Electric Potential
- Capacitance
- Electric Flux
Answer: 2. Electric Potential
3. Electric potential at a distance of 27 cm from a point charge 9 NC, is given by
- 200 V
- 100 V
- 300 V
- 50V
Answer: 3. 300 V
4. Two charges -6μC and 10μC arc placed at a distance 18 cm apart. The electric potential at the midpoint joining these two will be
- 4 x 105 V
- 4x 104 V
- 4x 103 V
- 4x 106 V
Answer: 1. 4 x 105 V
Physics Class 12 Chapter 2 Important Questions PDF
Question 2.
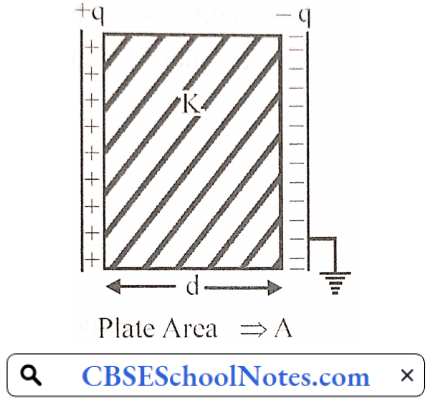
- Derivr an expression for the capacitance of a parallel plate capacitor filled with a medium of dielectric constant K.
- A charge q = 2 μC is placed at the center of a sphere of radius 20 cm. What is the amount of work done in moving 4 μC from one point to another point on its surface?
- Write a relation for polarisation \(\vec{P}\) of a dielectric material in the presence of an external electric field.
Answer:
Electrical capacitance: The ability of a conductor to store electrical energy (or charge) is called electric capacitance. The charge which is given to a conductor is directly proportional to its increasing potential
q ∝ V ⇒ q=C V
⇒ C = \(\frac{q}{V}\)
C ⇒ electrical capacity of a conductor.
The capacitance of parallel plate capacitor :
Electric Held intensity between two plates of the capacitor.
⇒ \(E_m=\frac{\sigma}{\varepsilon}\left\{\begin{array}{l}
\sigma=\frac{q}{A} \\
\varepsilon=\varepsilon_0 K
\end{array} \Rightarrow E_m=\frac{q}{\varepsilon_0 K A}\right.\)
The potential difference between the two plates of the capacitor
V = \(E_m \times d\)
V = \(\frac{q d}{\varepsilon_0 K A}\)
Capacitance C = \(\frac{q}{V} \Rightarrow C=\frac{q}{\left(\begin{array}{c}q d \\ \varepsilon_0 K A\end{array}\right)} \Rightarrow C=\frac{\varepsilon_0 K A}{d}\)
2. Sphere is equipotential surface: So. work done will be zero.
3. \(\vec{p}\)= ε0χ0\(\vec{E}\)
Question 3.
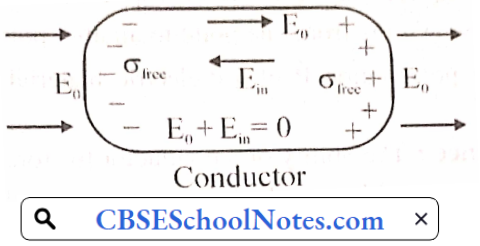
- Distinguish, with the help of a suitable diagram, the difference in the behavior of a conductor and a dielectric placed in an external electric field. Mow docs polarised dielectric modify the original external field.
- A capacitor of capacitance C is charged fully by connecting it to a battery of emf E. It is then disconnected from the battery. If the separation between the plates of the capacitor is now doubled, how will the following change?
- The charge is stored by the capacitor
- field strength between the plates.
- Energy stored by the capacitor
- Justify your answer with ease.
Answer:
1. When a conductor is placed in an external electric field, the free charges present inside the conductor redistribute themselves in such a manner that the electric field due to induced charges opposes the external field within the conductor. This happens until a sialic situation is achieved, i.e. when the two fields cancel each other and the net electrostatic field in the conductor becomes zero.
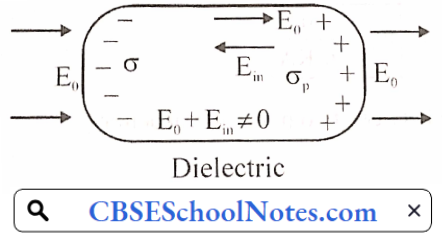
In contrast to conductors, dielectrics are non-conducting substances, i.e. they have no charge carriers. Thus, in a dielectric, free movement of charges is not possible. It turns out that the external field induces dipole moment by stretching molecules of the dielectric.
The collective effect of all the molecular dipole moments is the net charge on the surface of the dielectric which produces a field that opposes the external field. However, the opposing field is so induced, that does not exactly cancel the external field. It only reduces it. The extent of the effect depends on the nature of the dielectric.
Both polar and non-polar dielectrics develop net dipole moments in the presence of an external field. The dipole moment per unit volume is called polarisation and is denoted by P for linear isotropic dielectrics
2. After disconnecting the battery and doubling the separation between the two plates of the capacitor
(1) Charge on capacitor remains same (due to charge conservation)
i.e., \(C V=C^{\prime} V^{\prime} \Rightarrow C V=\left(\frac{C}{2}\right) V^{\prime} \Rightarrow V^{\prime}=2 V\)
Voltage will be doubled
(2) Field strength between the plates.
E’ = \(\frac{V^{\prime}}{d^{\prime}}=\frac{2 V}{2 d} \Rightarrow E^{\prime}=\frac{V}{d}=E\)
The electric field between the plates remains the same.
(3) Energy stored in capacitor when connected to battery \(\mathrm{U}_1=\mathrm{q}^2 / 2 \mathrm{C}\)
Now energy is stored in the capacitor after disconnection from the battery
⇒ \(U_2=\frac{q^2}{2 C^{\prime}}=\frac{q^2}{2 \times C / 2}=q^2 / C\)
∴ Energy stored in the capacitor gets doubled to its initial value.
Physics Class 12 Chapter 2 Important Questions PDF
Question 4.
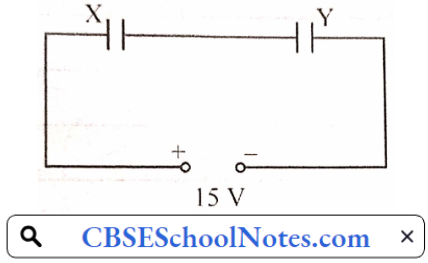
- Two parallel plate capacitors X and Y have the same area of plates and the same separation between them. X has air between the plates while Y contains a dielectric medium of εr=4.
- Calculate the capacitance of each capacitor if the equivalent capacitance of the combination is 4 μF
- Calculate the potential difference between the plates of X and Y.
- Estimate the ratio of electrostatic energy stored in X and Y.
- Two metallic spheres of radii R and 2R are charged so that both of these have the same surface charge density σ. If they are connected to each other with a conducting wire, in which direction will the charge flow and why?
Answer:
1. (1) Let us assume that capacitance of X capacitor = C μF
∴ Capacitance of Y capacitor = 4C μF (As C = KC) equivalent capacitance of system = 4μF (given)
So, \(\frac{1}{4 C}+\frac{1}{C}=\frac{1}{4} \Rightarrow C=5 \mu \mathrm{F}\)
The capacitance of Y capacitor → 4C = 20pF
(2) We assume the potential of capacitor X is V1 and V2 for capacitor Y
∴ \(\mathrm{Q}_{\mathrm{X}}=\mathrm{Q}_{\mathrm{Y}}\) [Both capacitor are in series]
⇒ \(C_X V_X=C_Y V_Y\)
⇒ \(\frac{1}{4}=\frac{V_Y}{V_X} \Rightarrow V_Y=\frac{V_X}{4}\)….(1)
Also given that Vx + VY = 15V…(2)
By solving the above eq (1) and (2),
we get V1 = 12V VY = 3V
(3) Ratio of energy stored \(\frac{E_X}{E_Y}=\frac{C_X V_X^2}{C_Y V_Y^2}=\frac{C_X}{C_Y} \times\left(\frac{V_X}{V_Y}\right)^2=\frac{1}{4} \times\left(\frac{4}{1}\right)^2 \Rightarrow \frac{E_X}{E_Y}=\frac{4}{1}\)
2. Potential on the surface of a charged metallic sphere is given by
V = kq/r
V= k.4π² σ/r
So V ∝ r
It means that a sphere having a large radius will be at a higher potential and charge always flows from a higher potential to a lower potential. So charge will flow from the metallic sphere of radius 2R to the sphere of radius R.