
Chromosomal Anomalies
In order to initiate a normal process of embryonic development and subsequent growth in an individual, it is necessary to have a complete set of all the 46 chromosomes that are both structurally and functionally normal.
The genes that constitute the chromosomes function with precision and with a subtle balance only when the entire complement of the genome participates in a close interaction.
This delicate balance of the genes can be disturbed by several chromosomal abnormalities which are of the following types. Anomalies may be in the form of:
- Numerical anomalies
- Structural anomalies
- Existence of different cell lines (Mosaicism/Chimaeras).
Abnormalities of the chromosomes account for a significant proportion of morbidity and mortality in humans. These defects are responsible for more than 50% of all spontaneous abortions, up to 1% of all congenital disabilities and a number of malignancies.

Numerical Anomalies
There are situations where an individual may contain more (47, 48 … etc.) or less (45) number of total chromosomes in all its cells instead of the normal count of 46.
This increase or decrease in the chromosomal count can be accounted for by the presence of one or more than one chromosome to be present in one or more extra copies or the absence of one or more than one chromosomes in a cell.
These anomalies when described in terms of the particular chromosome/chromosomes involved in the defect are called ‘somas’.
For example a cell with a missing chromosome would contain a set of 45 chromosomes and condition is called as a monosomy (as one of the pairs of chromosomes would be single, without the other of the pair mono = one, soma = body) for that chromosome.
Read and Learn More Genetics in Dentistry Notes
As in the Turner’s syndrome (XO), the female has only one X chromosome of the pair (XO) instead of the usual XX. Thus it is a monosomy of the X chromosome.
Similarly in conditions in conditions where a cell has three copies of a chromosome instead of two (the pair), the condition is called a trisomy.
A commonly found trisomy is the Down’s syndrome (21st chromosome). Likewise an individual having four copies of the same chromosome it is designated as tetratomic for that chromosome. Somas may involve both the autosomes and the sex chromosomes.
A dissimilar kind of numerical abnormality of the chromosome number is called polyploidy. The condition is manifested by the increase in the number of chromosomes of a cell exactly in the multiple of its haploid number. A haploid is half of the normal set of chromosomes in the individual.
In humans the complete set of chromosomes called the diploid set. Hence, haploid set in humans comprise 23 chromosomes. Therefore the cells that have three haploid sets of chromosomes (69 chromosomes) instead of the normal two sets (46 chromosomes) are called triploid or just polyploidy.
Anomalies like ‘somas’ (related to individual chromosomes) or ‘ploidies’ (related to sets of chromosomes) involve abnormal chromosomal numbers and are called aneuploidies.
Mechanisms of Numerical Anomalies
During the events of spermatogenesis or oogenesis it may so happen that an egg or a sperm may receive more or less than its share of chromosomes or chromatids during the process.
These defective gametes may hand over aneuploid chromosomes into the zygote and the resultant embryo would manifest chromosomal numerical anomalies.
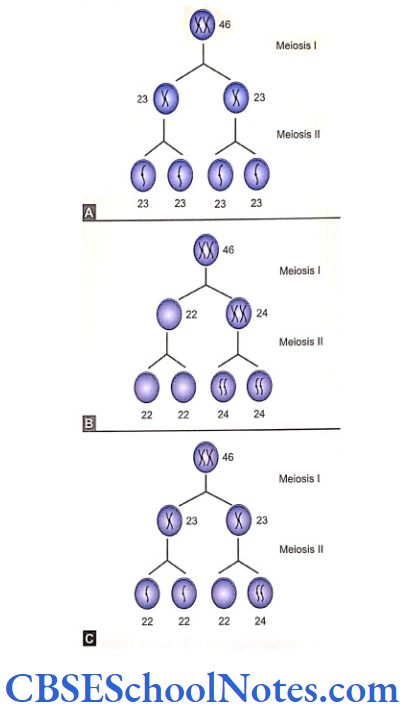
The failure of homologous pair of chromosomes to separate during meiosis I or meiosis II is called non-disjunction. Both these types of non disjunctions.
Consequences of Nondisjunction (trisomy and monosomy)
During the first meiotic division two chromosomes (with sister chromatids) of a pair may migrate to the same pole instead of two different poles of the dividing cell.
This causes both the chromosomes to aggregate in one of the daughter cells and the other cell receives none of the chromosomes.
Similarly during meiosis II a pair of sister chromatids may fail to segregate to go to two opposite poles of the dividing to segregate to go two opposite poles of the dividing cell and migrate to a single pole.
There is an equal distribution of chromosomes in both the situations described above (meiosis I and II) where the two chromosomes or the sister chromatids go to the same pole.
As seen in the figure, all the resultant gametes in the first situation are defective. Two of the gametes carry an extra number of a chromosome while the other two are devoid of the chromosome.
In the second situation two of the resultant gametes are normal whereas the other two resemble situation I.
All the defective gametes are aneuploids. Fertilization between the defective gametes with a normal one (23 chromosomes) well result in two types of zygotes.
The one formed with an extra chromosome (24 chromosomes) in the gamete would contain three chromosome of the type instead of two. This would thus result in a trisomy of the chromosome.
The other type of zygote formed by the union of a gamete devoid of a particular chromosome (22 chromosomes) with a normal one (23 chromosomes) will contain 45 chromosomes only.
This condition of absence of a chromosome of the pair is called monosomy of the said chromosome.
Developing zygotes where cells divide by mitosis may also exhibit nondisjunction. As a result a nondisjunction in the developing zygote gives rise to two or more different cell types having different number of chromosomes in them.
This phenomenon is known as mosaicism. The multiple of the haploid number of chromosomes (triploid, 69 or tetraploid, 92) are unknown in human except for some liver cells. Most of the polyploidies result in spontaneous abortion; a few may survive till birth.
Causes of Nondisjunction
Advancing maternal age and chromosomal abnormalities have been closely associated with each other. Disorders like trisomy 21 (Down’s syndrome), trisomy 13 and 18 have well-established association with advanced maternal age.
Meiosis I begins in primary oocytes before birth of a female and is completed at the time of an ovulation.
Thus a primary oocyte remains in an extended and suspended stage of activity from a period well before birth till any of the ovulatory cycle in the female (from menarche till menopause). Further, meiosis II is eventually completed only after fertilization of the secondary oocyte.
The state of this suspended meiotic activity, which is further delayed by a late motherhood, probably predisposes a gamete to non disjunctions because of abnormalities in spindle formation.
Though defective oocytes have been implicated in many cases of fetal chromosomal anomalies, non disunited sperms can also cause numerical anomalies.
The other causes implicated for nondisjunction are radiations from radioactive sources, delayed fertilization after ovulation, smoking, alcohol consumption, oral contraceptives, drugs, pesticides or some inherent genetic mechanism.
Numerical Abnormalities Of Autosomes
Trisomy’s related to the following chromosomes are commonly observed in the live-born children with congenital anomalies. Most other autosomal trisomy and monosomies are very severe and incompatible with life.
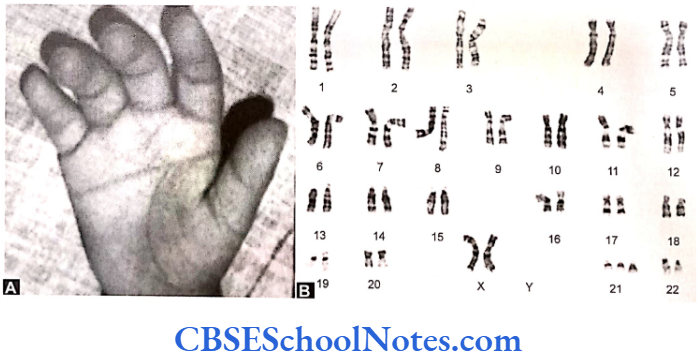
Trisomy 21 (Down’s Syndrome or Mongolism)
Characteristics of the Disease
Occurs in 1 out of 700 live-births. Incidence increases with the increasing maternal age. The risk at 45 years of age for its incidence is an high as 1 in 16. Males are more commonly affected than females.
Children are mentally retarded with low I.Q. scores (range from 25-75) showing poor growth, short stature and reduced muscle tone. About 40% of children suffer from major heart defects.
Facial features typically are small head circumferences, epical this folds, protruding tongue, small ears and sloping palpebral fissures.
The hands are short and broad. There may be a single transverse palmar crease resulting from the fusion of the proximal and distal transverse palmar creases (Simian crease). The mean survival age is about 16 years though it varies from few weeks to decades. Most affected adults tend to develop Alzheimer’s disease in later life for specific metabolic defects.
Mechanisms that may cause Down’s Syndrome:
- Trisomy
- Translocation
- Mosaicism.
The trisomy of the 21st chromosome most commonly causes (95%) of Down’s syndrome. The karyotype in a trismic Down’s is either 47+XY or 47+XX> The source of the extra 21st chromosome is mostly from a nondisjunction in maternal meiosis I. Robesonian translocations (see below) may be the cause of Down’s syndrome in 3% cases.
The genotype in a Robertson Ian Down’s is 46+XX or 46+XY. Children with mosaicism contain two cell populations (one normal and the other trismic). These Down’s are due to early life disjunctions. Due to coexistence a set of normal cells in the individual, the person is less severely affected.
Counseling
Counseling may be prenatal or postnatal. Prenatal counselling can be advised in high risk. Pregnancies. Following the delivery of a Down’s child, the risk of begetting a Down’s child in subsequent pregnancies increases significantly in elderly ladies. Also the risk of getting a Down’s child is three folds in a previously affected lady when compared to a woman of the same age not affected with such a child.
In cases of translocations, the recurrence risk is 1 to 3% in case of the father bearing a translocation but risk increases substantially to 15% in case of a carrier mother.
Postnatal counselling is about the management of the child towards normal life and appropriate therapy.
Prenatal diagnosis: The prenatal diagnosis of Down’s syndrome can be done in cases with a prior history of such an event or on clinical suspicion. It can be done by amniocenteses for chromosomal analysis.
The triple test is an important diagnostic tool that estimates three specific biochemical markers (α-fetoprotein, estriol and chorionic gonadotrophin) present in the maternal serum at 16 weeks of gestation. In Down’s pregnancies the level of α-fetoprotein and estriol levels tend to be reduced as compared to the normal, while the level of human chorionic gonadotrophin is increased. Estimating the increasing levels of inhibin-A in the maternal serum also helps in diagnosis.
Trisomy 13: Patau’s Syndrome
Usually the pregnancies with his anomaly terminate spontaneously within days of conception. However, the incidence of Turner’s syndrome in all live-births is 1 in 5000. Most of the affected children die within a month while a few of them may survive for a few months.
Characteristics of the Disease
Children are severely retarded both physically and mentally and possess small skulls and eyes. The child may have cleft lip and cleft palate, extra finger or a malformed thumb. The CVS, CNS and excretory systems are susceptible to infections.
Trisomy of chromosome 13 is responsible for this syndrome that rarely develops also due to certain Mosaicism and Robertson Ian translocation patterns. The risk of recurrence is very small but the incidence increases with advanced maternal age
Numerical Abnormalities of the Sex Chromosomes
The sex chromosomes are commonly affected by the following numerical chromosomal anomalies:
- Trisomy’s like XXX or aneuploidies such as XXY, XYY
- Monosomy like 45, XO
- Mosaicism, 46, XY/46, XX or 46 XX/45 XO.
An extra X or Y chromosome usually has a relatively mild effect. This is because the Y chromosome contains relatively few functional X chromosome form Barr bodies. Developing zygotes tolerate sex chromosomal anomalies better than those of the autosomes.
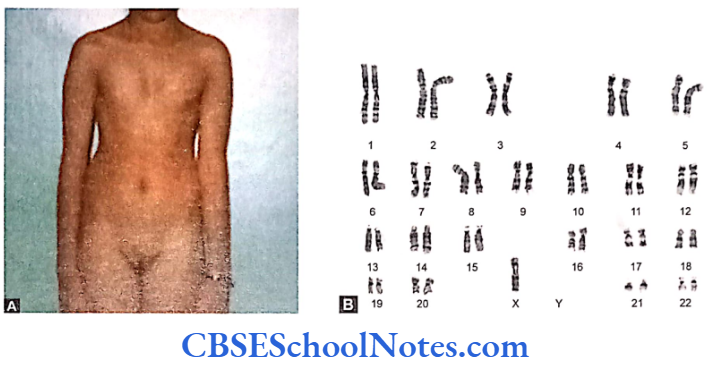
Turner Syndrome, 45, XO
This syndrome is actually a monosomy of the sex chromosome and is a common cause of spontaneous abortions. About 20% of spontaneously aborted fetuses have 45, XO genotype. Incidence in live-born infants varies from 1 in 5000 to 1 in 10,000. They survive to develop phenotypically into a female.
Characteristics of the Disease
The affected individuals are females possessing normal intelligence or might be slightly retarded. Usually show a webbed neck, low posterior hair line, cubitus valgus and broad chest with widely spaced nipples. They have a short stature.
Individuals are poor in arithmetical skills, reading maps and drawing diagrams.
Patients are mostly infertile which is due to a primary development failure of the ovaries. This also leads to the absence of mensuration. Breasts fail to develop and pubic hair is scanty as a lack of secondary sexual character, Individuals characteristically possess ill-developed or rudimentary gonads (ovaries) called the streak gonads. Ventricular septal defects or coarctation of aorta may exist. Sex-chromatin or Barr body examination is always negative as there is only one X-chromosome.
Genetic Characteristics and Counselling
The most frequent cause of Turner’s syndrome (45,XO) is the monosomy of the X chromosome. Mosaicism – 45, XO/46, XX, Isochromosome- – 46, X, i(Xq) and Ring chromosome – 46, X, r(X) may also account for certain percentage of the anomaly.
Estrogen replacement therapy (HRT) should be tried at adolescence for development of secondary sexual characteristics. Though affected females are sterile but can bear child with the help of “In vitro fertilization”. Genital tract reconstructions with surgery may be attempted to obtain a normal conjugal union.
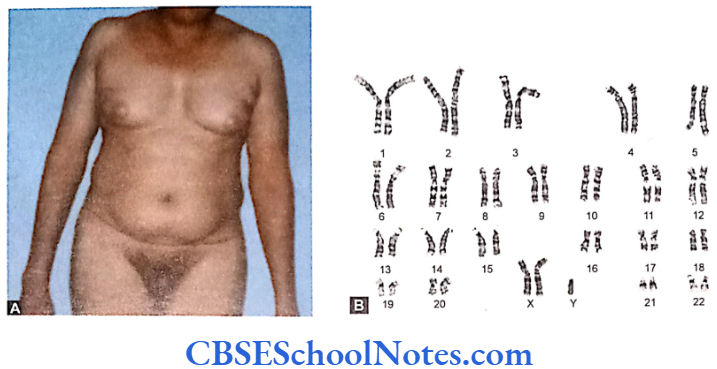
47, XXY: Klinefelter Syndrome
Characteristics of the Disease
Occurrence rate is about in 1 per 1000 newborn males. Affected individual is phenotypically a male. Syndrome usually remains undetected until adolescence. Patients are diagnosed when they attend infertility clinics for treatment of infertility. Appearance of an affected person is normal though he might be quite tall with a mile degree of mental retardation.
Puberty is usually delayed and individuals have very small pair of testes but a normal penis and scrotum. Secondary sexual characters don’t develop fully and the pubic and facial hair is scanty. Gynecomastia (enlarged breast) may be a prominent feature in some.
Genetic Characteristics and Counselling
Usual Klinefelter cases have karyotype of 47, XXY with some individuals showing a mosaic pattern. Mosaic (46XY/47, XXY) individuals show Barr body. Treatment with testosterone (HRT) at puberty may expedite the onset and development of secondary sexual characteristics.
47, XXY Males
Characteristics of the Disease
The incidence is rated approximately at 1 per 1000 newborns. The males are phenotypically normal but usually tall built and almost always associated with slight mental retardation. Contrary to common belief they are not overtly criminals but may be hyperactive and restless individuals. These individuals may show emotional immaturity, impulsive behaviors or delinquent tendencies. Karyotype represents – 47, XXY. The additional Y chromosomes is usually due to nondisjunction in meiosis II during spermatogenesis in the father.
Structural Anomalies
Structural abnormalities of chromosomes commonly refer of defects in the form of a missing portion or a portion being represented twice or more in a chromosome. The abnormalities in structure of chromosomes are often secondary to events of chromosome breakage. Chromosomes are extremely fragile and they may at times, break spontaneously.
Chromosomal breakages may be induced by certain external agents like X-rays, chemicals, and viral infections. Fragmentation in chromosomes occurs usually at the ends that are away from the centromere (telomere). These small regions are lost during cell division and they are unable to move to the poles in daughter cells.
In fact chromosomal breakages are detected by specific mechanism and are not allowed to transmit to daughter cells in either mitosis or meiosis. Some of these anomalies, especially near the centromere, may remain undetected. Following are the important structural abnormalities.
- Deletion
- Inversion
- Ring chromosome
- Isochromosome
- Translocation.
Structural abnormalities cause loss of genes (as in deletion), gain of genes (as in duplication) or a change in the normal position of the genes (as in inversion and translocation) and result in genetic disorders.
Karyotype Symbols
p Short arm of chromosome
q Long arm of chromosome
ter Terminal portion
qter Terminal portion of long arm
pter Terminal portion of short arm
+ Before a chromosome number indicates that the chromosome is extra e.g. +21.
– A chromosome is missing. A plus or minus sign after the number of a chromosome indicates the addition or deletion respectively of a region in that chromosome.
Mos Mosaic
/ Separates karyotypes in mosaics, e.g. 47, XXX/45, X-chromosome
del Deletion
inv Inversion
r Ring chromosome
i Isochromosome
rep Reciprocal translocation
rob Robesonian translocation
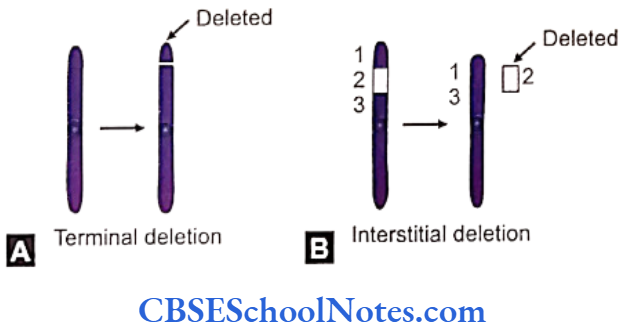
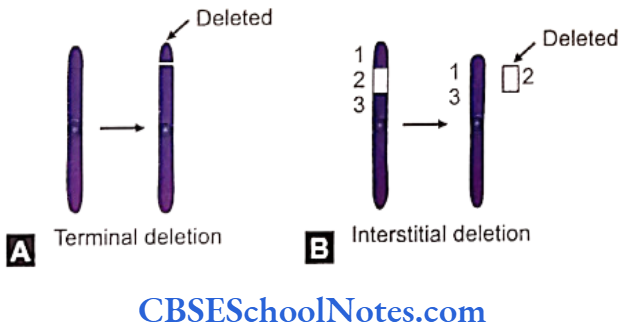
Chromosomal Deletion
Deletion denotes breakage that occurs in a part of the chromosome away from the centromere. The broken part is subsequently lost.
A part of a chromosome may get deleted near its terminal end by a single break. Sometimes a short intervening portion of a chromosome may break off by two separates breaks. There may be several genes within the broken off portion of the chromosome that eventually is deleted or lost. An individual cannot survive if a large piece of chromosome is deleted. A loss of more that 2% of genome will be lethal. Deletions are classified into two kinds.
Microscopic or Chromosomal Deletion
This can be visualized microscopically by using usual karyotyping methods in cases of sufficiently large deletions, e.g. deletion of the short arm of chromosome 5 (cri-du-chat syndrome) and of the short arm of chromosome 4 (Wolf-Hirschhorn syndrome) are some of the well known examples.
CRI-DU-CHAT Syndrome
Characteristics of the Disease
The incidence is about 1 in 50,000 births. This syndrome bear underdeveloped larynx which make them produce the characteristic cat like cry. Other features include microcephaly with physical and mental retardations. Infants suffering from Wolf-Hirschhorn (4p-) are severally mentally retarded an may also show the stunted physical growth.
Submicroscopic Microdeletions
These defects cannot be visualized by usual karyotype methods and hence needs molecular techniques for their detection, e.g. FISH.
Following a few of the common microdeletion syndromes.
Syndromes Affected chromosome
Prader-Willi 15
Angelman 15
Wilms tumor 11
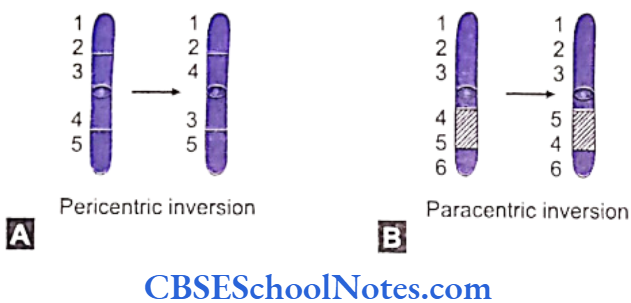
Chromosomal Inversion
The abnormality involves only a single chromosome which braks at two points. The broken segment rearranges itself back into the chromosome by inverting its position. Inversions may be of two different types, i.e. pericentric (involving the centromere) and paracentric (not involving the centromere).
Inversion abnormalities do not result in clinical problems in individuals as inversions usually do not cause a loss in chromosomal material; the breaks generally occur at noncoding sites. However, if the disruption or break is caused at the site of an important functional gene, it may result in a abnormality in a person.
A person with a chromosomal inversion in his or her germ cells furnishes abnormal gametes. It is a fact that genes undergo recombination and rearrangements during ‘crossing over’ phases in meiosis I. Inversions existing in chromosomes undergoing recombination produce unequal distribution of genes and hence defective gametes. Fertilization with these gametes commonly results in spontaneous abortions.
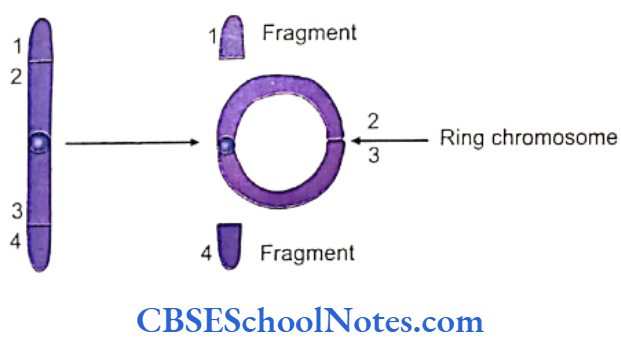
Ring Chromosomes
Rarely chromosomes form a closed circle (ring) structure. Formation of ring chromosomes start with breaks near the tips (ends) of each arm of a chromosome. These broken and sticky ends then fuse with each other. The two distal fragments are lost during cell division.
DNA replicates in these chromosomes before cell division. But migration of the sister chromatids is abnormal due to the anomalous configuration of the chromosome. This results in the loss of the entire chromosome from the cell. As such individuals with ring chromosomes tend to develop a mosaic cell population.
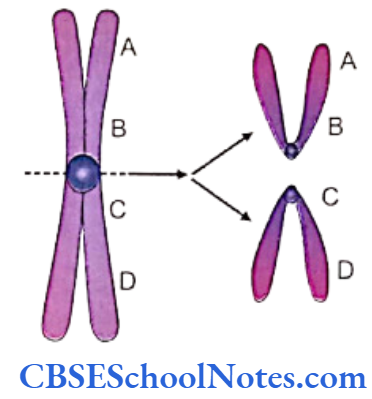
Isochromosomes
Isochromosomes result as a consequence of incorrect splitting of chromosomes at their centromeres during cell division. This faulty splitting results in the formation of two isochromosomes. Each defective splitting produces two types of chromosomes.
Each of them contain two arms that are identical to each other. One of the chromosomes has two short arms whereas the other possesses two long arms.
Cells having, for example an isochromosome with two short arms, will contain an extra short arm as well as the set of genes located on the short arm (in fact the total dose of those shorts arm and its genes would exist in triplicate or in thrice dose in the cell; the normal chromosome providing the third short arm and the homologous genes.
This cell is devoid of one long arm that is lost and migrates to the other daughter cell with the formation of the long arm isochromosome.
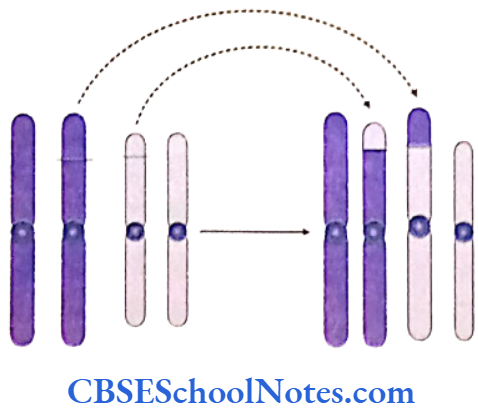
Chromosomal Translocation
The exchange of genetic material between chromosomes is called translocation. Micro and macro segments of chromosomes are found to germ fragmented and exchanged between homologous as well as between heterologous chromosomes. Translocation can be wither balanced or unbalanced.
A translocation is balanced when the event does not result in any loss of genetic material. The entire complement of genes gets appropriately expressed in an individual. Unbalanced translocations accompany loss of genes. People with balanced translocations are normal, but may have affected children if translocations involved their germ cells.
Two types of Translocations usually observed:
Reciprocal Translocations
Incidence: Approximately in 500 people.
This translocation occurs between tow nonhomologous chromosomes after breakage and exchange of the fragments.
Reciprocal translocations are usually balanced rearrangements that more often than not have no detectable phenotypic effects in the individual. The reciprocal translocation between chromosome 11 and 22 (between groups D and G) are relatively common.
Gametogenesis is defective as the chromosomes with translocations are unable to align properly to form the bivalents during meiosis 1. As a consequence asymmetrical distribution of chromosomes results in abnormal gametes.
Robertson Ian Translocation
Incidence: About 1 in 1000 people.
Acrocentric (groups D and G) may break at their centromeres giving rise to a long arm and a short arm with satellite body. The long arm from one group may fuse with the long arm of the other group (D/G). This fusion may also occur between long arms within the same group, e.g. 21/22 or 21/21. The short arms thus generated by the breaks fuse together and are lost.
This is functionally a balanced translocation though the total chromosome number is reduced to 45 (loss of the fused short arms and satellites that don’t carry significant genetic material).
A 21/21 translocated individual is normal with a total of 45 chromosomes in all his somatic as well as germ cells. During meiosis, however, one group of gametes receive the translocated 21/21 chromosome and the other group gets none of the 21st chromosome. On fertilization with normal gametes, the 21/21 containing gamete begets a Down’s child and the gamete with no 21st chromosome produces a monosomy (45XX/XY, -21) child that is incompatible with life.
On the other hand, individuals bearing a D/G translocation involving the 21st chromosome (45 XX/XY), produce 4 types of gametes. On fertilization with a normal gamete the 4 varieties of gametes may probably yield a normal child (46 XX/XY), one normal child that receives that translocated 21st chromosome (45XX/XY), one Down’s affected child resulting from inheriting two normal chromosomes 21 (one each from the mother and the father and the additional one from the translocated chromosome involving the 21st chromosome from the normal gamete and none from the translocated germ cell.
Individuals having translocation involving the D and G (21st chromosome) groups may conceive a Down’s child for every four pregnancies. 21/21 translocations will have an absolute risk of 100% for Down’s syndrome progenies.
Almost about 4% cases of all Down’s syndromes are due to Robertson Ian translocations. The others are accounted for by nondisjunction’s at gametogenesis.
Existence Of Different Cell Lines (Mosaicism/Chi merism)
Chromosomal Mosaic or Mosaicism
Majority of we people have identical chromosomal constitution in all our cells and tissues. Chromosomal mosaicism is a condition where two genetically different cell populations coexist in the same individual. The difference is generally observed in the number of chromosomes in the cells. Mosaicism may affect both the autosomes and the sex chromosomes.
Whatever the differences though, the types of different cell lines in a mosaic pattern are derived form a single zygote as the source of the cells. In mosaics a group of cells may be normal (46,XX/XY) whereas others may have extra or less number of chromosomes. Mosaicism involving sex chromosomes may denote a full range of anomalies, e.g. true hermaphrodites (46 XX/46 XY), a variant of Turners (46 XX/X0), etc.
Causes of Mosaicism
The most usual cause of chromosomal mosaicism is a nondisjunction occurring in an early embryonic mitotic division.
Mosaicism not only occurs at the chromosomal level but also at the level of the gene. If a gene mutates at a very early stage of embryonic cell division, the fetus possesses two different cell lines, i.e. some cells with the normal gene and others with the mutant gene. Mosaics may result from isochromosome splitting and delay in chromosomal migration called the ‘Anaphase lag’ also resulting in unequal distribution of the chromosomes.
Chimera
In undifferentiated and early life cells from two or more embryos of different mouse are mixed together and introduced into the uterus of a foster mother, the resultant mass of cells can give rise to a normal mouse at term. However, this mouse would constitute different cell population in its body.
The cells have identical number of chromosomes yet each different cell line would be unique is its parent source. This individual is called a chimera. Thus a chimera is an individual with two or more than one zygote or life source.
Chi merism may be induced by the fusion of two zygotes obtained by fertilization of two different ova from two different sperms. Chi merism may evolve with sharing of placenta between dizygotic twins, sequestration of very minute maternal tissue into the fetus from the fetoplacental unit. Chimeras exhibiting different sex chromosomes may represent a distinct bisexual karyotype with 46, XY/46, XX genotype (true hermaphrodites; see also mosaicism).
Chromosomal Abnormalities Summary
- Numerical Anomalies
- Abnormalities in chromosome numbers may arise due to an increase (47,48,etc.) or decrease (4%) in the total number of chromosomes instead of normal complement of 46.
- Anomalies in chromosome numbers usually occur during gametogenesis when homologous pair of chromosomes fail to separate from each other during meiosis I. This phenomenon is called non-disjunction.
- The most commonly observed numerical chromosomal abnormalities are.
- Down’s syndrome (trisomy 21)
- Patau’s syndrome (trisomy 13)
- Edward’s syndrome (trisomy 18)
- Turner syndrome (45,X)
- Klinefelter syndrome (47, XXY)
- XXX females
- XYY males.
- Structural Anomalies
- Aberration in chromosomal structure may result either from missing (deletion) or getting represented twice (duplication) of a piece of chromosome.
- Structural abnormalities occur due to abnormal rearrangement of the chromosome.
Following are the most commonly observed structural abnormalities:- Deletion
- Inversion
- Ring chromosome
- Isochromosome
- Translocation.
- Mosaicism
- An individual with two or more different cell populations is called a chimera.
- The chromosomal constitutions of the cell lines vary in autosomal or the sex chromosomal number.
- Chromosomal mosaicism is due to a nondisjunction occurring during an early embryonic mitotic division, isochromosome splitting, anaphase lag, ring chromosome, etc. that cause unequal chromosomal distribution.
- Chimera
- An individual having two or more genetically distinct cell populations derived from more than one zygote or life source is called a chimera.