Bones Of Thorax And Abdomen
The following bones constitute the thorax:
- Sternum: Bone of anterior wall of thorax
- Twelve thoracic vertebrae: Bones of the posterior wall of the thorax. These are named after 1st thoracic vertebra to the twelfth thoracic vertebra from above downwards
- Twelve pairs of ribs: Bones of lateral walls of the thorax
The following bones constitute the abdomen and pelvis:
- Five lumbar vertebrae: Bones of the posterior abdominal wall. These are named from 1st lumbar vertebra to the fifth lumbar vertebra from above downwards.
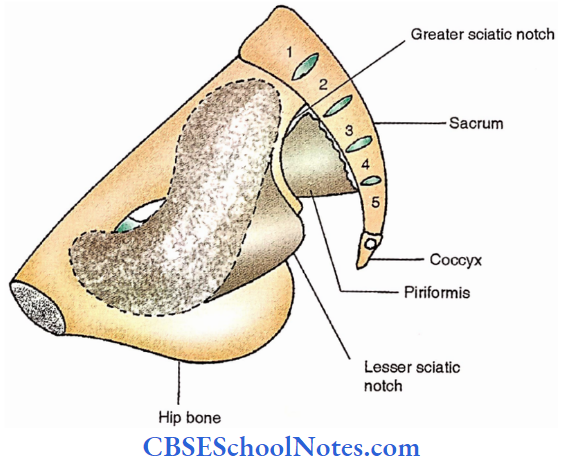
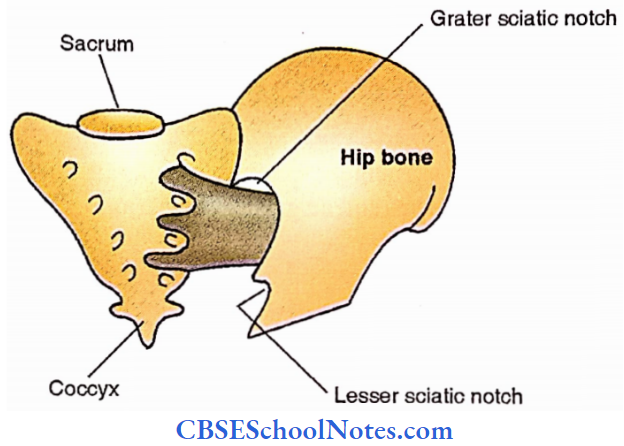
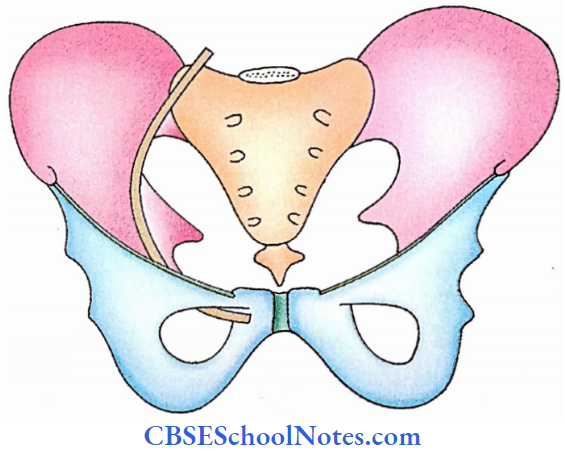
- Sacrum and coccyx: These together with hip bones form a bony pelvis or pelvic girdle and form the skeleton of the pelvis and gluteal region.
The total number of bones in the thorax and abdomen are as follows:
- Thorax -37
- Abdomen and pelvis- 9
Note: Two hip bones are common to both lower limbs and pelvis
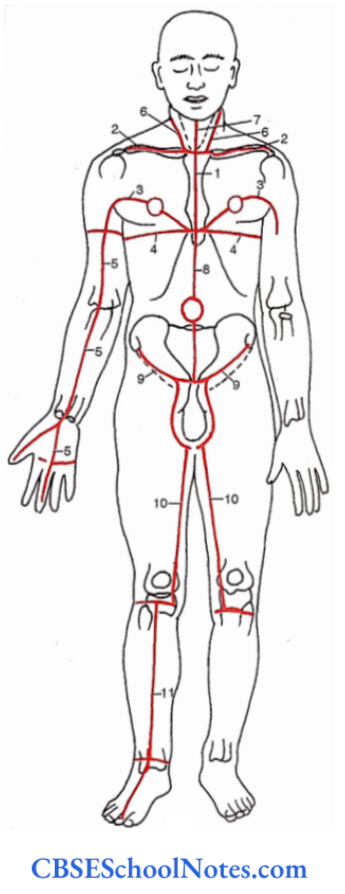
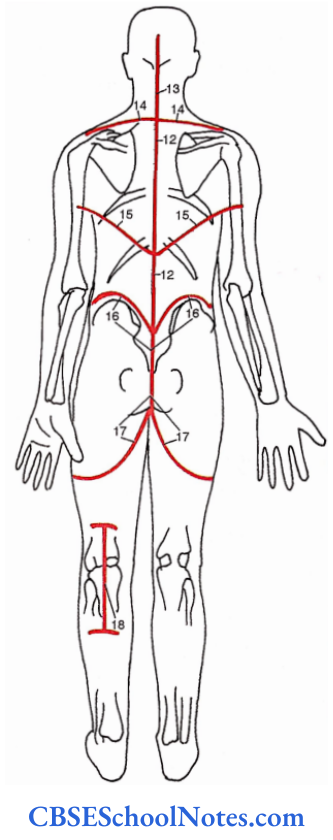
Reference diagrams to make incisions for dissection
Thoracic Cage Framework
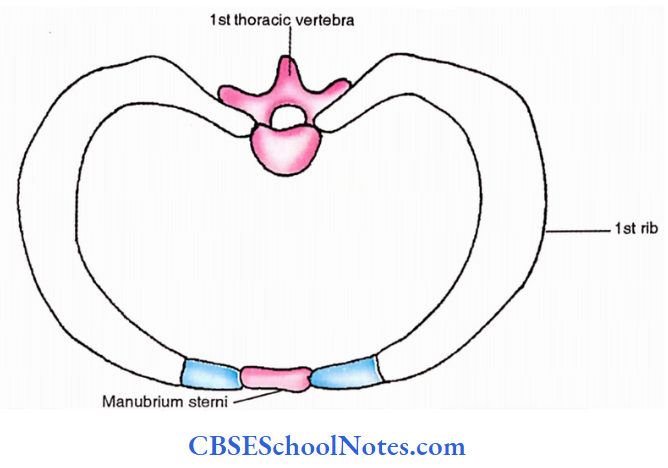
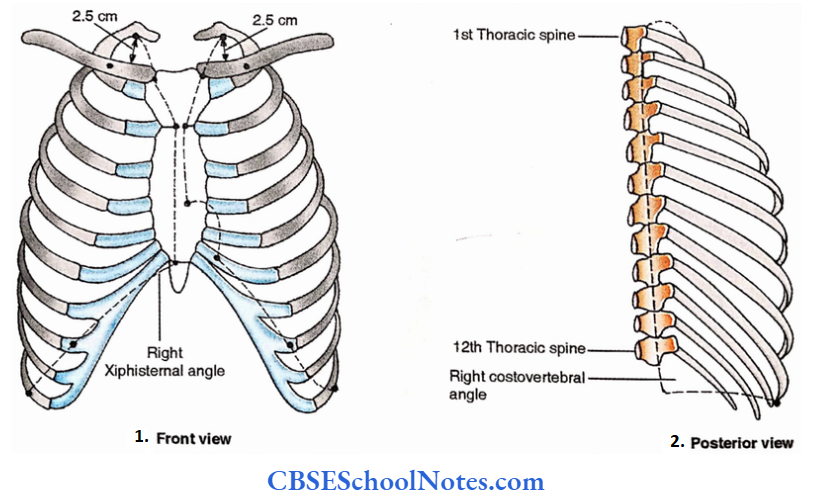
The thoracic cage is an osseoligamentous framework formed by 12 thoracic vertebrae posteriorly, sternum anteriorly and 12 pairs of ribs and costal cartilages on each side.
The posterior wall is longer as compared to the anterior wall making upper and lower openings of the thoracic cavity oblique.
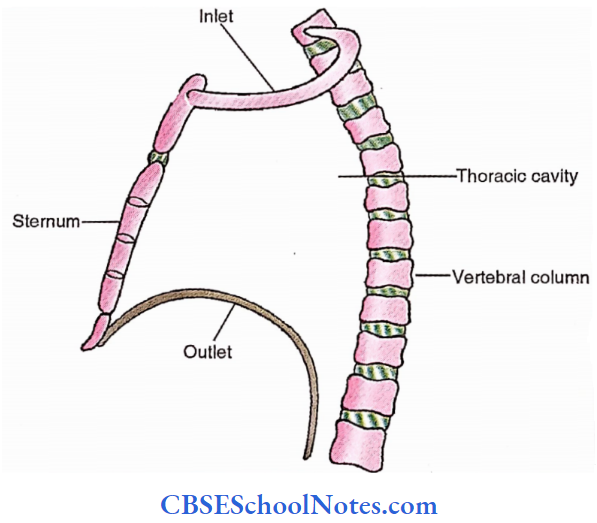
The upper opening (anatomists call it thoracic inlet and clinicians name it thoracic outlet) faces upwards and forwards.
It is bounded by the highest (1st) thoracic vertebra posteriorly, the superior border of manubrium stem anteriorly (sternum consists of 3 pieces from above downwards namely manubrium stem, body and xiphisternum) and the inner border of highest (1st) rib and its costal cartilage on each side.
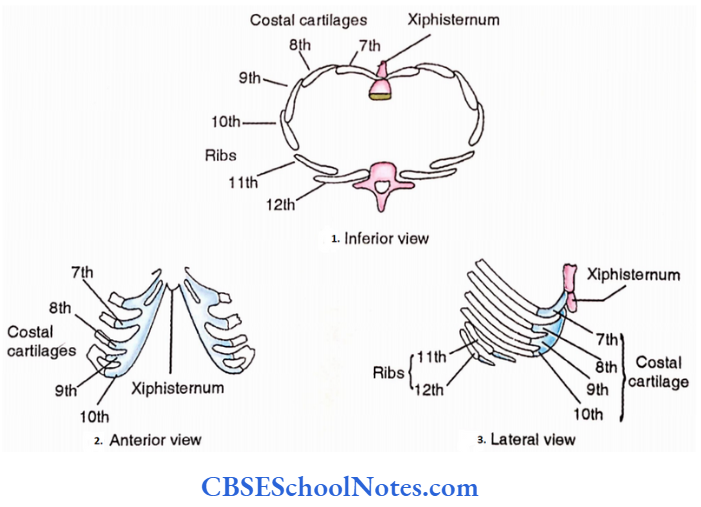
- The lower opening (thoracic outlet) faces forward and downwards. It is bounded anteriorly by the xiphisternal joint.
- Posteriorly by the last (12th) thoracic vertebra and the 12th pair of ribs and on each side by lower 6 (7th to 12th) costal cartilages. Boundaries formed by ribs and costal cartilages are also called coastal margins.
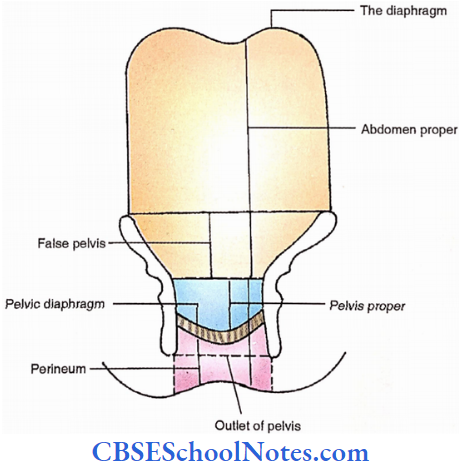
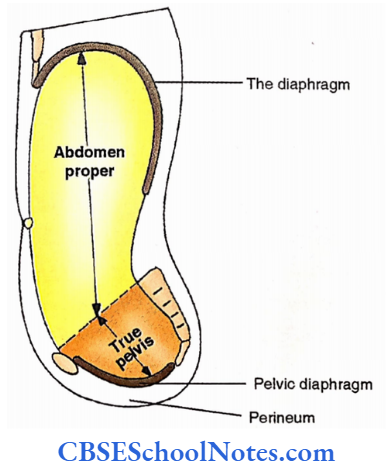
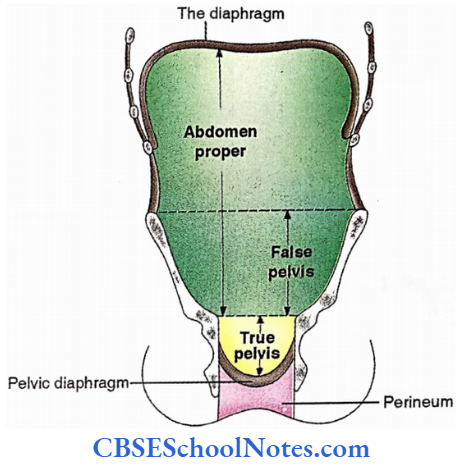
Which form a subcostal angle below the xiphoid process anteriorly. The lower opening is occupied by a musculotendinous partition between the thorax and abdomen called ‘the diaphragm’.
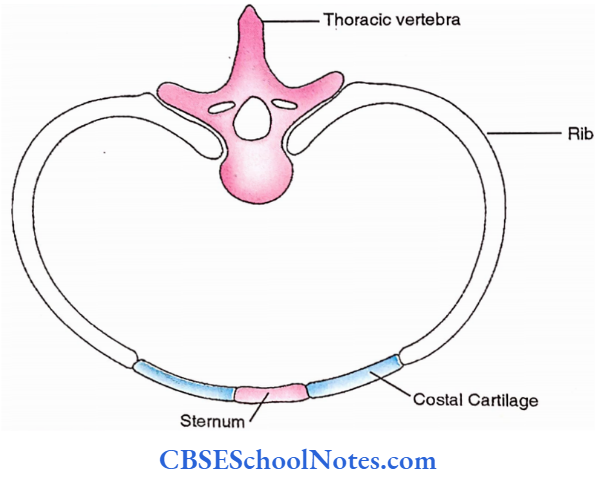
The thoracic cavity is not circular in outline, but compressed anteroposteriorly and due to the forward projection of thoracic vertebral bodies it becomes reniform (kidney-shaped) in shape.
- The 12 thoracic vertebrae follow the primary curvature (concavity forward i.e., the original foetal curvature) to provide adequate room for the vital thoracic organs.
- Ribs are curved bones whose posterior ends invariably articulate with the vertebrae and the anterior ends extend forwards variably. 1st rib fuses with the upper part of the lateral border of the manubrium stem (synostosis).
- 2nd to 7th ribs end a short distance from the side of the sternum, the gap being filled by the costal cartilages (thus upper 7 ribs are vertebrosternal).
- The anterior ends of the 8th to 10th ribs are similarly replaced by the costal cartilages but instead of reaching the sternum they articulate with the costal cartilages just above (thus, the 8th to 10th ribs are vertebrochondral).
The lower two ribs are replaced by small costal cartilages at their anterior ends, which do not articulate with adjacent costal cartilages (thus, the 11th and 12th ribs are vertebral).

Between 12 pairs of ribs and costal cartilages are 11 pairs of intervals called the intercostal spaces. The obliquity of the spaces corresponds with the obliquity of the ribs.
Their width gradually reduces from above-downwards as those of coastal cartilages. The intercostal spaces are occupied by the intercostal muscles.
Joints Of Thorax
Sternal Joints
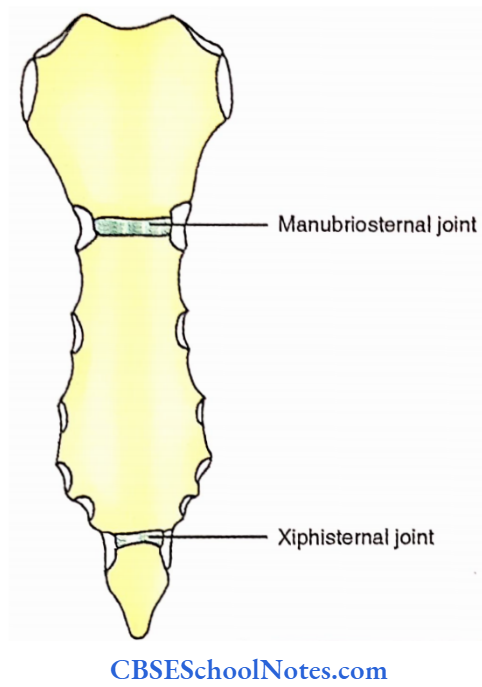
Three pieces of sternum (manubrium, body and xiphisternum) meet at two junctions, the manubriostemal and xiphisternal. Both the joints thus formed are secondary cartilaginous (symphyses) in nature.
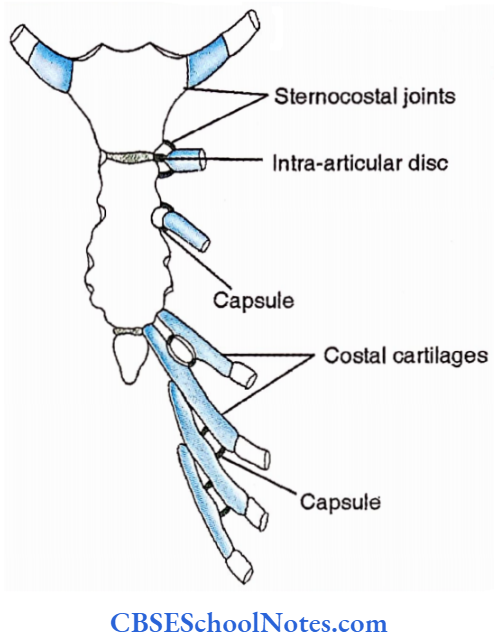
Sternocostal Joints
Only true ribs (upper seven, vertebrosternal) reach the sternum but indirectly through the costal cartilages to form sternocostal (truly speaking osteochondral) joints.
1st costal cartilage forms a primary cartilaginous joint with the side of the upper part of the manubrium. 2nd costal cartilage meets with the sternum at the manubriostemal joint (level of sternal angle) forming a synovial joint.
Its cavity is divisible into two by an intra-articular disc. 3rd to 6th costal cartilages meet with the side of the body of the sternum while the 7th reaches the side of the xiphisternal joint, each forming a single synovial joint cavity.
Interchondral Joints
Adjacent surfaces of6th to 9th costal cartilages form synovial interchondral joints. Each joint is supported by medial and lateral interchondral ligaments.
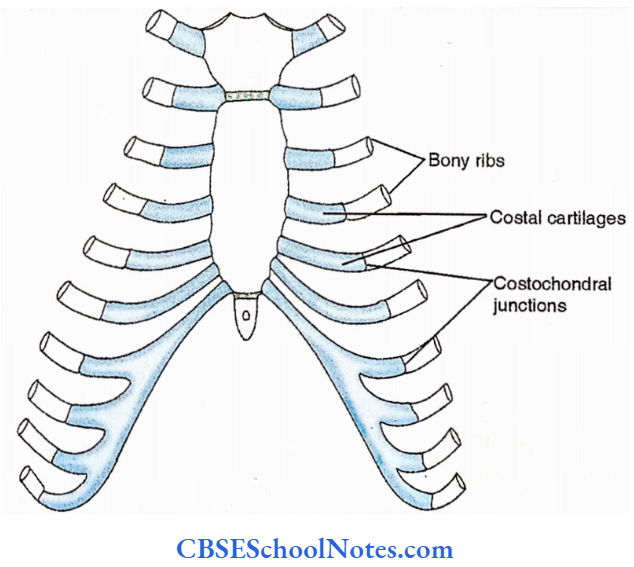
Costochondral Joints
These are primary cartilaginous joints between the concavities at the anterior ends of long ribs and convexities at the lateral ends of corresponding costal cartilages.
Costovertebral Joints
Joints Of The Heads Of The Ribs
The head of a typical rib articulates with the upper border of the corresponding vertebral body and the inferior border of the vertebral body above; i.e., levels with the intervertebral disc.
The synovial joint thus formed is strengthened by the radiate ligament that connects the front of the head of the rib with the adjacent vertebral border and intervertebral disc.
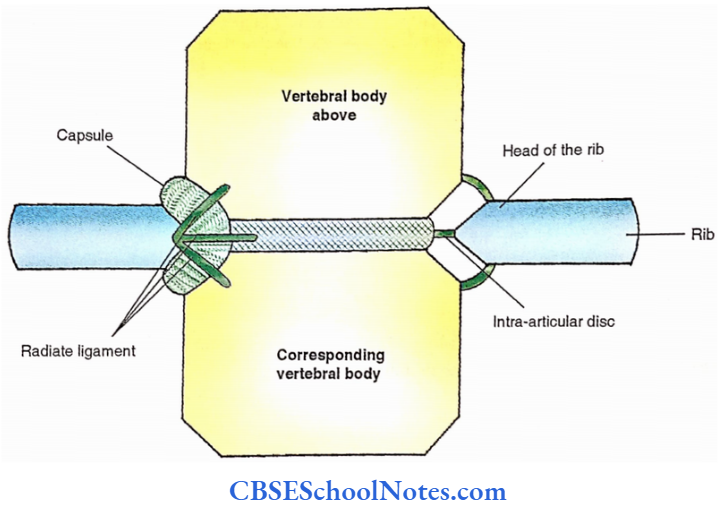
The cavity of the joint is divided into upper and lower compartments by an intra-articular ligament which connects the crest of the head with the intervertebral disc.
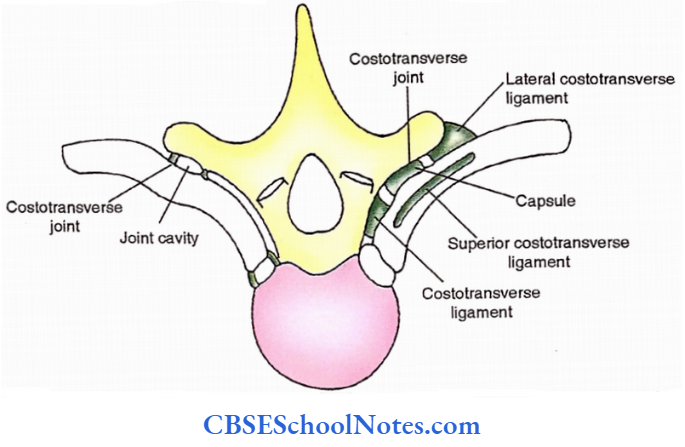
Costotransverse Joint
It is a synovial joint formed between the articular facet of the tubercle of the rib and the costal facet on the front of the lateral part of the transverse process of the corresponding vertebra. The joint is strengthened by three costotransverse ligaments.
The inferior costotransverse ligament connects the front of the corresponding transverse process medial to the joint.
A similar ligament lateral to the joint is called the lateral costotransverse ligament. The superior costotransverse ligament connects the superior border of the neck of the rib with the transverse process of the vertebra above.
Joints Of The Vertebral Column
Joints Of The Vertebral Bodies
Bodies of the adjacent vertebrae form secondary cartilaginous joints. Adjacent surfaces are covered with hyaline cartilages with intervening intervertebral discs.
- The latter has concentric fibrous laminae in the periphery (annulus fibrosus) and gelatinous mass in the centre (nucleus pulposus).
- Joints strengthened by vertical fibrous bands all along the vertebral column, anterior and posterior to the vertebral bodies called anterior and posterior longitudinal ligaments.
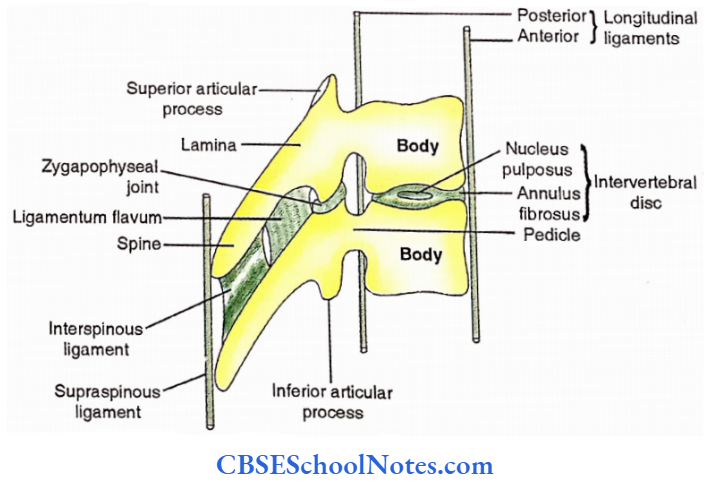
Joints Of The Vertebral Arches
Zygapophyseal Joints
These are plane synovial joints between the adjacent superior and inferior articular processes. articular surfaces are oblique and located along a horizontal arc therefore allowing rotational movements in the thoracic region.
Intervertebral Syndesmosis
Gaps between the adjacent laminae of the thoracic vertebrae are filled by the ligamentum flava. The spines of the adjacent vertebrae are held together by the interspinous ligaments.
The supraspinous ligament is an elongated band connecting the tips of the spines. Intertransverse ligaments connect the adjacent transverse processes.
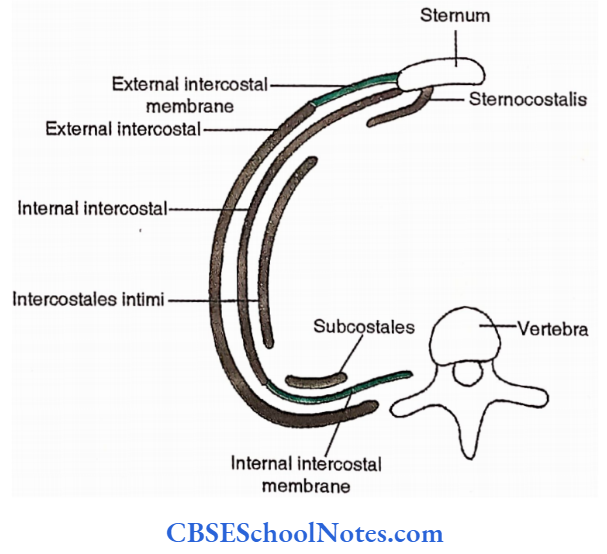
Intrinsic Muscles Of Thoracic Wall
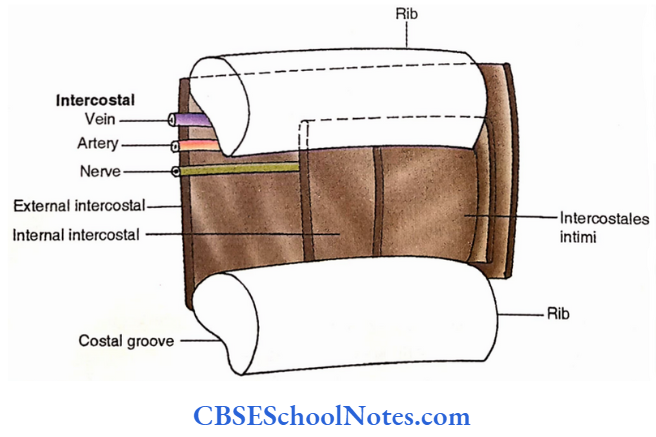
The muscles are arranged in three layers, external (external intercostal), middle (internal intercostal), and internal (stemocostal is, intercostales intimi and subcostales).
1st two are smaller and occupy the intercostal spaces while the innermost is larger and covers the inner surfaces of the ribs.
Intrinsic Muscles Of Thoracic Wall Attachments
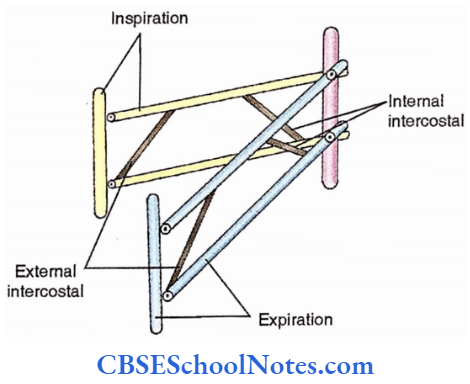
External intercostal muscles connect the adjacent border of the ribs. In the anterior part, its fibres downwards and forwards.
In an intercostal space, the external intercostal extends from the tubercle to the anterior end of the rib. The muscle is replaced by the external intercostal membrane between the costal cartilages.
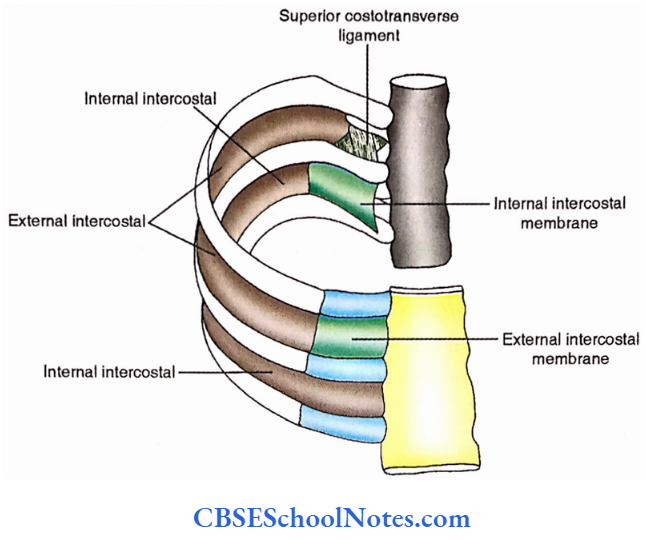
The internal intercostal muscle is attached to the upper border of the rib below and the costal groove of the rib above.
- Towards the posterior end, its fibres run downwards and backwards. In an intercostal space, it extends from the angle of the ribs to the anterior end of the intercostal space.
- The side of the sternum. Beyond the angle posteriorly, it is represented by the internal intercostal membrane.
The three components of the innermost layer i.e., stemocostal (also called the transverse thoracic), intercostales intima and the subcostales, occupy approximately the anterior 1/4th.
Middle 2/4th and the posterior 1/4th of the intercostal spaces respectively. Fibres of the stemocostal are attached to the posterior surface of the lower half of the sternum and extend upwards and laterally towards the 2nd to 6th pairs of the costal cartilages.

Intercostalis intimi connects the inner surfaces of the adjacent ribs while subcostales extend between the inner surfaces of distant ribs. The direction of fibres in both these muscles is the same as that of internal intercostals.
Intrinsic Muscles Of Thoracic Wall Dissection Steps
Remove the remains of the serratus anterior and pectoral muscles. Choose one intercostal space and cut through the external intercostal muscle and external intercostal membrane along the lower border of the space.
- Turn the muscle upward identify the internal intercostal muscle and note the direction of its fibres both anteriorly and posteriorly and concerning the external intercostal muscle.
- Expose and identify the lateral cutaneous branch of the intercostal nerve trunk deep into the internal intercostal muscle. Cut the internal intercostals, expose and follow the intercostal nerve forward and backwards with the accompanying intercostal vessels.
- Identify the innermost intercostal muscles and note their arrangement. Remove the intercostal muscles and membranes from the anterior part of the 1st and 2nd intercostal spaces and expose the internal thoracic artery lateral to the sternum.
- Trace this artery into the 6th intercostal space and note its terminal branches, namely superior epigastric and musculophrenic arteries.
Intrinsic Muscles Of Thoracic Wall Nerves
Intercostal nerves
Intrinsic Muscles Of Thoracic Wall Actions
External intercostals and the interchondral parts of the internal intercostals elevate the ribs i.e., help in inspiration, while rest depresses the ribs and helps in expiration.
The tone of the intercostal muscles prevents in-drawings and budging of the intercostal spaces during inspiration and expiration respectively.
Intrinsic Muscles Of Thoracic Wall Applied Anatomy
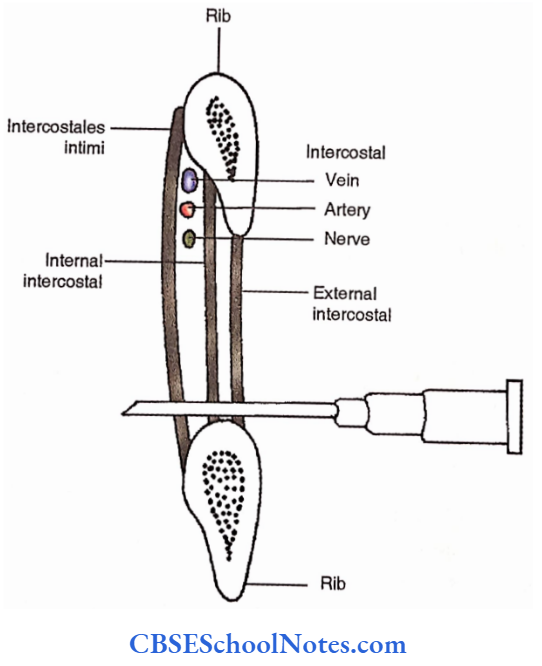
- The needle should be introduced near the upper border of the ribs to avoid injury to the main intercostal and vessels which run in the costal groove.
- Retraction of intercostal spaces is evident along with stridor, dyspnoea and cyanosis in cases of obstruction of major passages.
- Structural (fixed) scoliosis is always accompanied by rotation of vertebrae (i.e., there is some kyphosis). Asymmetrical paralysis of the intercostal muscles is one of the many causes of this condition.
Respiratory Movements
These are the movements of the ribs and diaphragm which are responsible for the act of respiration.
- The former is responsible for the increase in the anteroposterior and transverse diameters while the latter causes an increment of the vertical diameter during inspiration. All diameters are reduced during expiration.
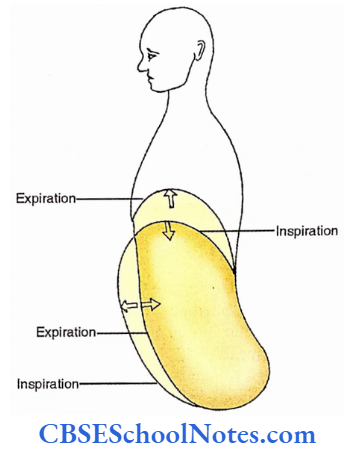
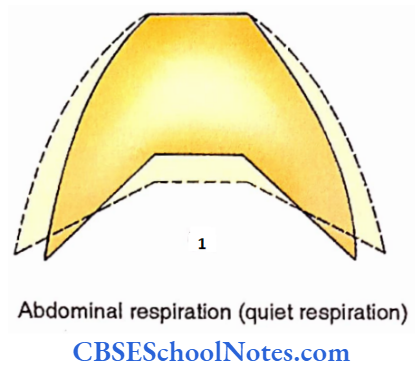
- Thoracic respiration involves movements of the thoracic cage. Movements of the diaphragm, as during quiet respiration result in ‘abdominal respiration.
- Normally, the anterior abdominal wall moves forwards and backwards during inspiration (depression of the diaphragm) and expiration (elevation of the diaphragm) respectively.
- Since the anterior ends of ribs lie at a lower level than the posterior ones, their elevation also 1 moves them forward, an action responsible for the increase in the anteroposterior diameter during inspiration.
Such movements elevate the sternum with angulation of 7° at the manubriostemal joint. This phenomenon is also called ‘pump handle movement.

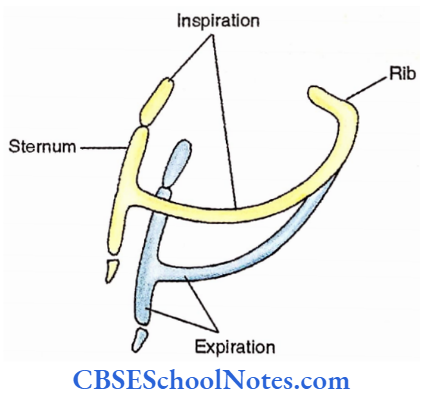
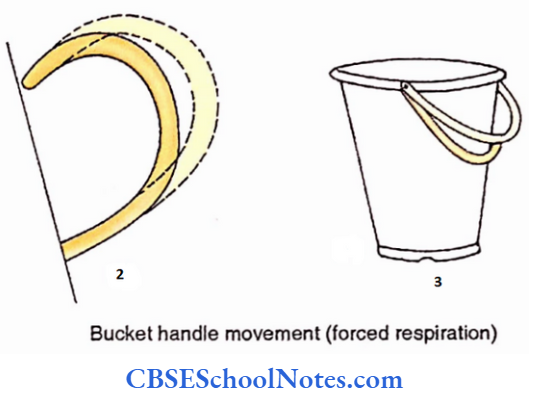
The lateral parts on the ribs are relatively lower than their ends. Therefore, these parts when elevated during inspiration also move laterally thereby increasing the thoracic transverse diameter.
This phenomenon is markedly noted in the lower ribs during forced inspiration and is often called “bucket handle movement”.
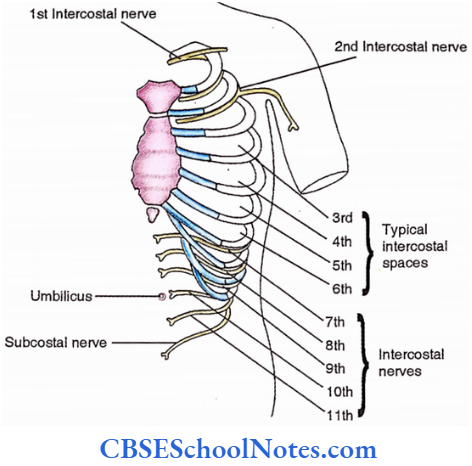
Intercostal Nerves
The ventral rami of the 1st to 11th thoracic nerves continue in the neurovascular plane (between internal intercostal and innermost intercostal thoracic muscles) as intercostal nerves.
Usually 3rd to 6th have similar features and are called ‘typical intercostal nerves’. The rest are atypical due to some differentiating features.
Atypical Intercostal Nerves
First Intercostal Nerve
It contributes to the lowest root of the brachial plexus.
Second Intercostal Nerve
Its lateral cutaneous branch (intercostobrachial nerve) supplies the floor of the axilla and the upper medial part of the arm.
Seventh To Eleventh Intercostal Nerves
These continue in the anterior abdominal wall after supplying the intercostal spaces and therefore are thoracolumbar.
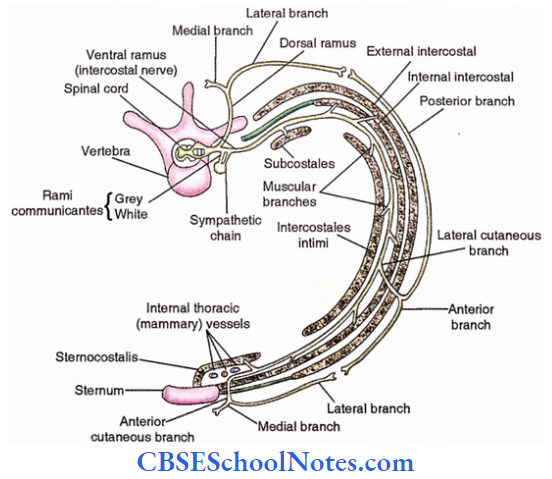
Typical Intercostal Nerve
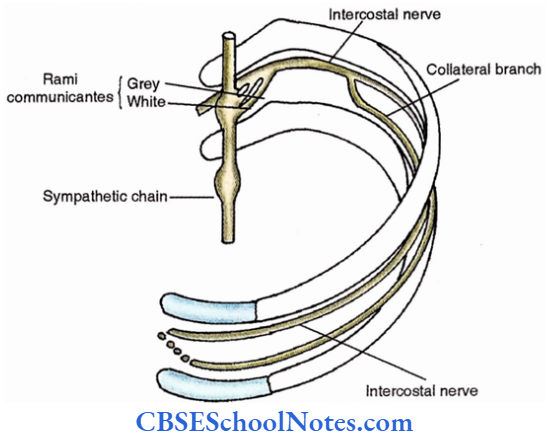
It runs in the neurovascular plane in the costal groove below the intercostal vessels (remember VAN: vein, artery and never) and provides the following branches
- Rami communicantes. Two small nerves connect the posterior part of the intercostal nerve with the adjacent ganglion of the sympathetic chain.
- Most often the lateral one is the white ramus communicans conveying preganglionic fibres to the ganglion and the medial one is the grey ramus communicans receiving postganglionic fibres from the ganglion.
- Muscular branches. Numerous branches supply the intrinsic muscles of the thorax
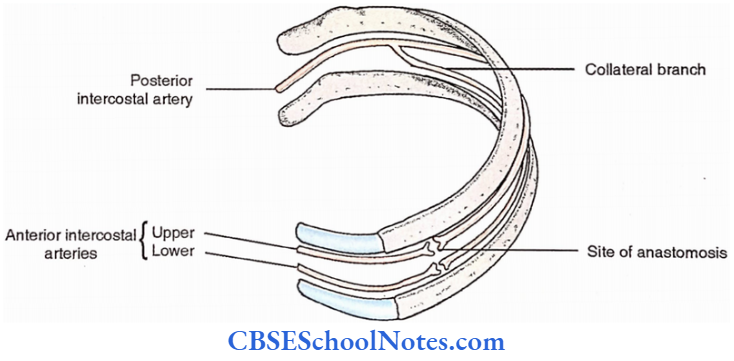
- Collateral branches. It usually appears at the angle of the rib and then runs in the lower part of the intercostal space along the upper border of the rib.
- Pleural branches. Conveying branches to the parietal pleura.
- Lateral cutaneous nerve. It pierces the muscles along the midaxillary line divides into the anterior and posterior branches and supplies the skin of the lateral thoracic region.
- Anterior cutaneous branch. It pierces the internal intercostal muscle and external intercostal membrane to appear by the side of the sternum and supply the skin of the front of the thorax.
Intercostal Nerves Applied Anatomy
- Herpes zoster: A viral disease of the spinal root ganglion which is the most important cause of intercostal neuralgia (severe cutaneous pain along the distribution of a nerve).
- Tube thoracostomy: The preferred site for insertion of the tube during thoracostomy is the 4th or 5th intercostal space at the anterior axillary line. The introduction of a tube at a further lower level might damage the diaphragm or enter the abdominal cavity causing injury to the liver, spleen or stomach.
- Intercostal nerve block. The nerve should be blocked before the emergence of lateral cutaneous nerve. The needle is directed towards the lower border of the rib and the tip is pushed towards the subcostal groove.
- Pain in the vertebral region may follow the course of the neurovascular bundle.
Internal Thoracic Mammary Vessels
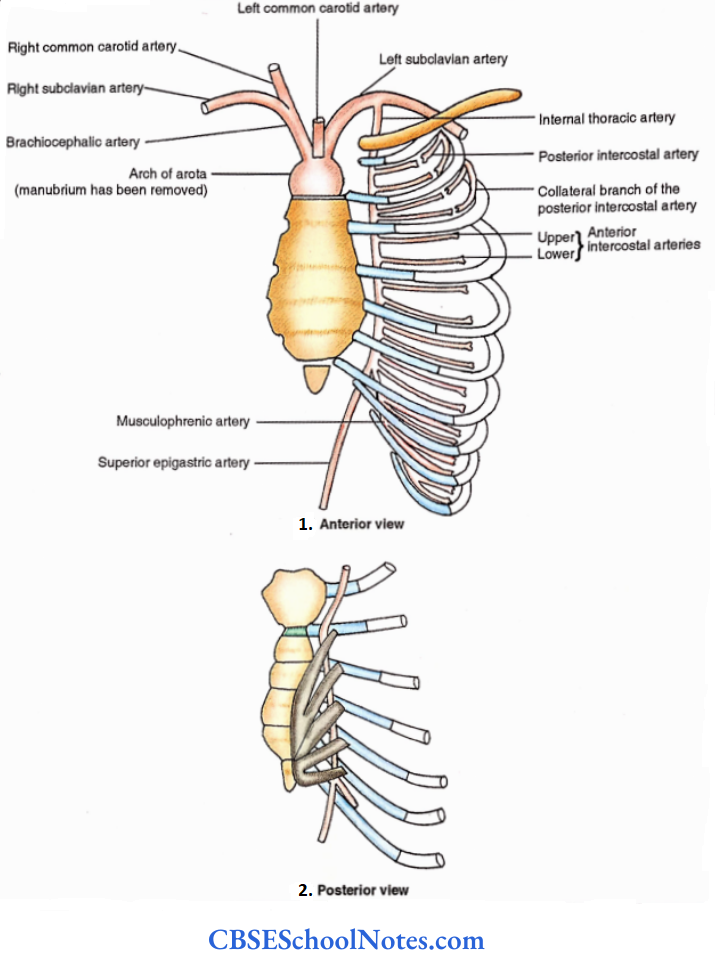
Internal Thoracic Artery
- Origin– Subclavian artery.
- Course– The artery descends behind the costal cartilage by the side of the sternum.
- Termination– It terminates at the level of the 6th intercostal space into two terminal branches.
Branches
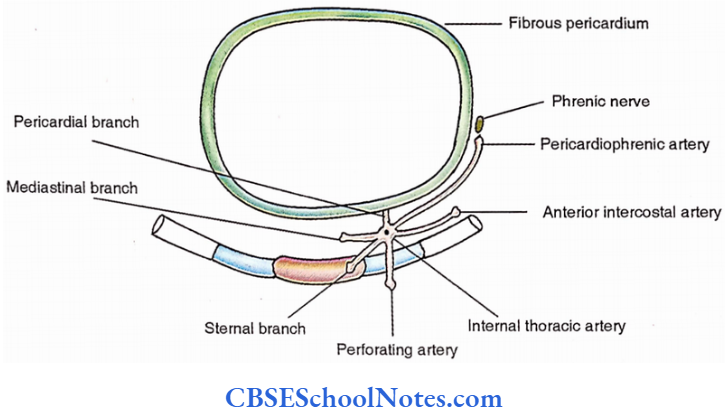
- Pericardiophrenic artery. It accompanies the phrenic nerve during its course over the fibrous pericardium.
- Pericardial branches. They supply the fibrous pericardium and parietal layer of the serous pericardium.
- Perforating arteries. These accompany the anterior cutaneous branches of the intercostal nerve I and appear by the side of the sternum.
- Mediastinal branches. These supply the structures in the anterior mediastinum including the thymus.
- Sternal branches. Supply the sternum and sternocostal muscle.
- Anterior intercostal arteries. A pair of anterior intercostal arteries, upper and lower, run laterally in each of the upper six intercostal spaces and anastomose with the posterior intercostal artery and its collateral respectively.
- Terminal branches
- Musculophrenic artery. It runs along the costal margin above the peripheral attachment of the diaphragm.
- Paired anterior intercostal arteries for the 7th to 9th intercostal spaces originate from this branch.
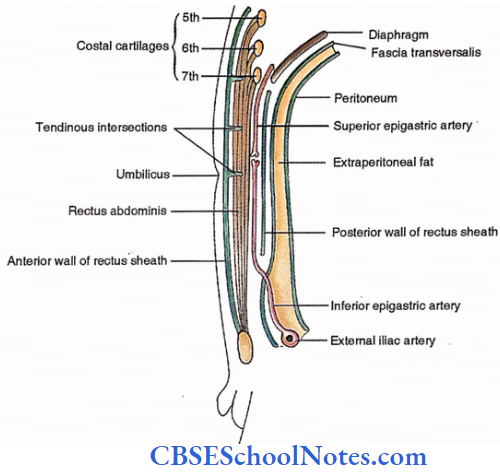
- Superior epigastric artery. This artery enters the rectus sheath and descends behind the rectus abdomen to supply the anterior abdominal wall.
Internal Thoracic Vein
It is formed at the level of 3rd costal cartilage by the union of venae comitantes of the internal thoracic artery. It ascends medial to the artery and ends in the brachiocephalic vein.
Intercostal Vessels
Intercostal Arteries
Posterior Intercostal Arteries
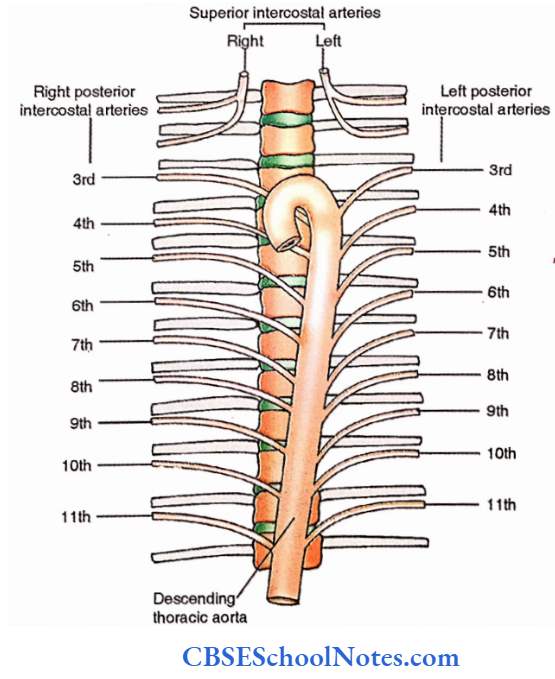
There are 11 pairs of posterior intercostal arteries, i.e., one in each space. Those for the upper two spaces originate from the superior intercostals artery, a branch of the costocervical trunk which itself arises from the subclavian artery.
3rd to 11th posterior intercostal arteries are the direct branches from the descending thoracic aorta.
Intercostal Arteries Applied Anatomy
- A needle should not be introduced into the thoracic wall medial to costal angle as it might risk the posterior intercostal artery due to its oblique course.
- In cases of coarctation of the aorta, dilated and tortuous intercostal arteries produce notches in the ribs, a phenomenon which can be easily appreciated in a chest radiograph.
Anterior Intercostal Arteries
There are two (upper and lower) intercostal arteries in the upper nine intercostal spaces. In the upper six spaces, these originate from the internal thoracic artery.
While those for the 7th to 9th spaces appear from the musculophrenic artery. There are no anterior intercostal arteries in the 10th and 11th intercostal spaces.
Intercostal Veins
Posterior Intercostal Veins
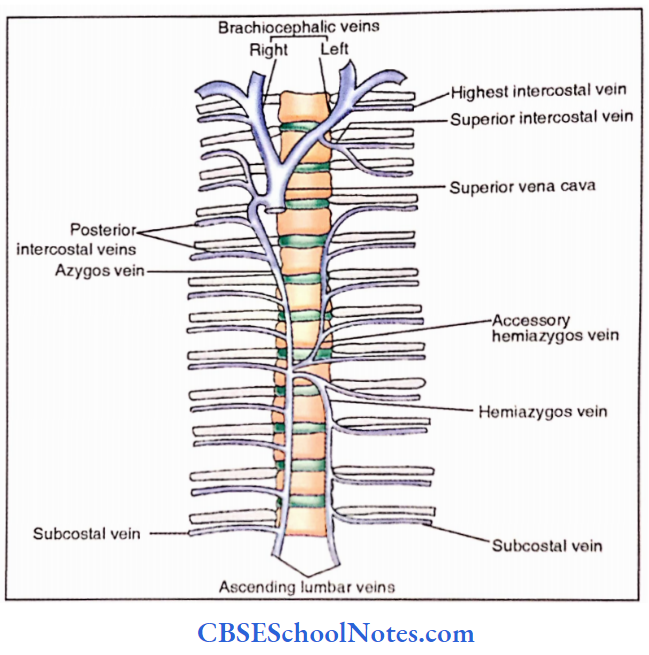
- There are 11 pairs of posterior intercostal veins, i.e., one in each intercostal space. The first (highest) intercostal vein of two sides drains into the corresponding brachiocephalic vein.
- 2nd and 3rd posterior intercostal veins unite to form superior intercostal veins which on the right and left sides drain into azygos and brachiocephalic veins respectively.
- Next 8 (i.e., from 4th to 11th) posterior intercostal veins drain into the azygos vein on the right side. On the left side.
- The posterior intercostal veins from 4th to 8th spaces join the accessory hemiazygos and those from 9th to 11th join the hemiazygos vein. Both accessory azygos and hemiazygos veins ultimately drain into the azygos vein.
Intercostal Veins Applied Anatomy
In the obstruction of the superior vena cava, the azygos veins provide an alternative route for the return of venous blood because these veins and their tributaries connect the two venae cavae.
Anterior Intercostals Veins
These accompany the corresponding arteries and end in the internal thoracic or musculophrenic veins.
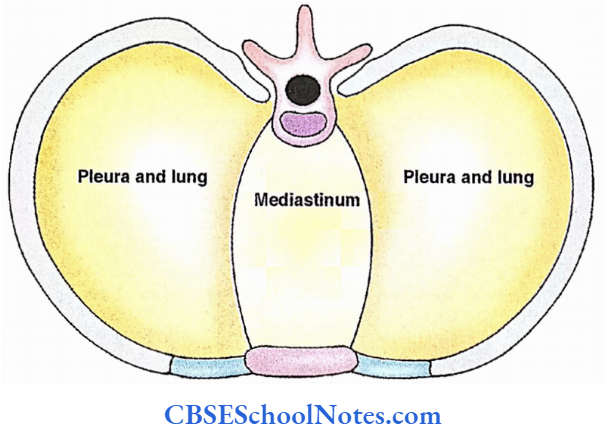
Subdivisions Of The Thoracic Cavity
The thoracic cavity is divisible into a midline part called the mediastinum and two lateral parts (right and left) occupied by the corresponding pleura and lung.
Pleura
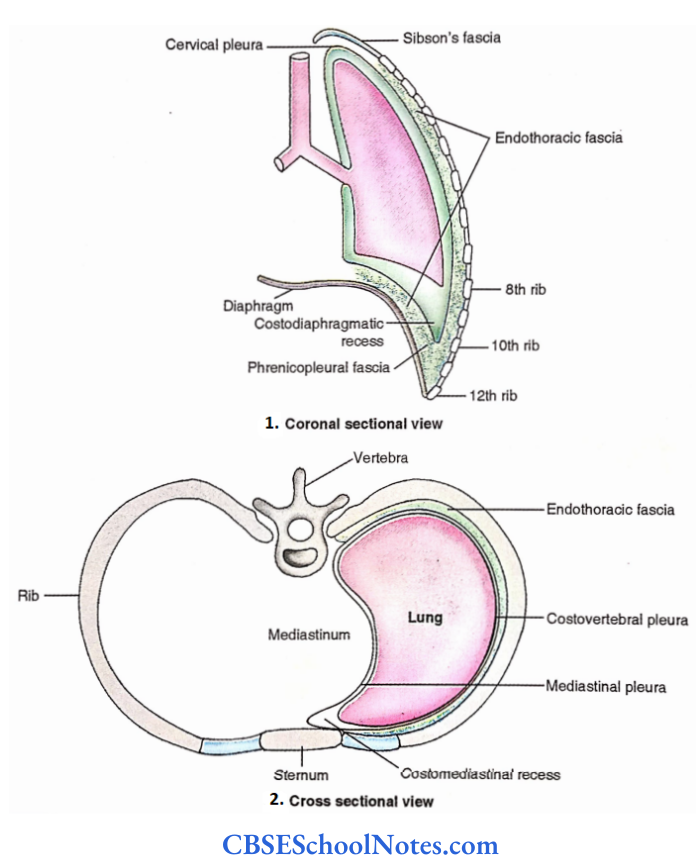
The pleura is a serous membrane (a fibrous membrane lined by simple squamous epithelium) around each lung. Since the pleural sac is invaginated by the corresponding lung from the medial side, the pleura on each side is divided into the following parts;
- Visceral (pulmonary)- It intimately covers the lung.
- Parietal pleura- It lines the walls surrounding each lung.
- Connecting pleura- It connects the visceral with the parietal pleura.
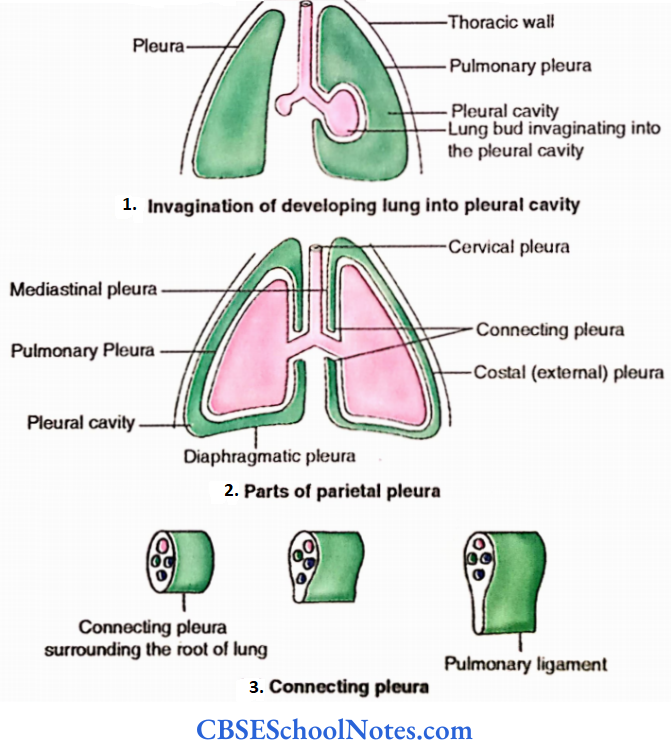
Parietal Pleura
The parietal pleura is subdivided into different parts according to their relations.
- Costovertebral pleura – It lines the thoracic cage, i.e., ribs, intercostal spaces, sternum and the vertebral column.
- The mediastinal pleura covers the midline septum (mediastinum) between the sternum anteriorly and the vertebral bodies posteriorly.
- Diaphragmatic pleura-It covers the dome of the diaphragm.
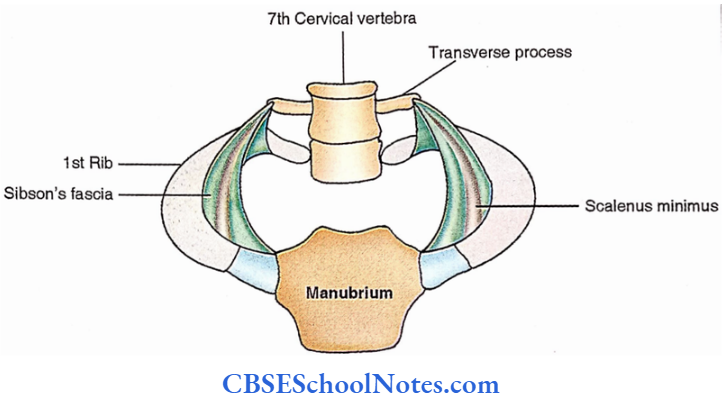
- Cervical pleura (cupola or dome)– It is the part of the pleura beyond the inner margin of the 1st rib. It lies under the suprapleural membrane (Sibson’s fascia) at the root of the neck.
Margins And Their Reflection
- Anterior margin (sternal reflection)-The line extends on both sides from the sternoclavicular joint to the middle of the sternal angle and then descends vertically on the sternum up to the level of the 4th costal cartilage.
- On the left side, the line makes a bold curvature beyond the sternal margin and descends to the 6th costal cartilage. On the right side, the line descends vertically to the xiphisternal joint.
- Inferior margin (costodiaphragmatic reflection)-The line of reflection extends laterally from the lower end of the anterior margin and meets with the midclavicular line at the 8th rib, and the midaxillary line at the 10th rib.
- Lateral to the upper border of erector spinae at the 12th rib and a point 2 cm lateral to the upper border of the 12th thoracic spine.
- Posterior margin (vertebral reflection) – It is a vertical line from the posterior end of the inferior margin to a point 2 cm lateral to the 2nd thoracic spine.
Pleural Recesses
The lungs do not extend as far anteriorly as well as inferiorly as the pleural reflections resulting in the formation of costomediastinal and costodiaphragmatic recesses respectively.
A recess therefore is a narrow space between the adjacent parietal pleurae. Recesses allow expansions of the lungs during inspiration.
Fasciae Holding The Parietal Pleurae
- Endothoracic fascia– It is loose areolar tissue which separates the parietal pleura from the rib cage, vertebrae and diaphragm.
- Suprapleural membrane (Sibson’sfascia)-This fascia diverges from the front of the 7th cervical transverse process to the inner border of the first rib. The cervical pleura is attached to it. It prevents the bulging of the apex of the lung with each inspiration.
- Phrenicopleural fascia– It is endothoracic fascia between the diaphragmatic pleura and muscles of the diaphragm.
Connecting Pleura
It is the site where the parietal pleura meets with the visceral pleura. Connecting pleura encircles the lung root. Below the root of the lung, the connecting pleura hangs down as an empty fold, the pulmonary ligament.
It provides a dead space into which the lung root descends during inspiration and also allows the expansion of pulmonary vessels, especially the inferior pulmonary vein.
Vessels And Nerves
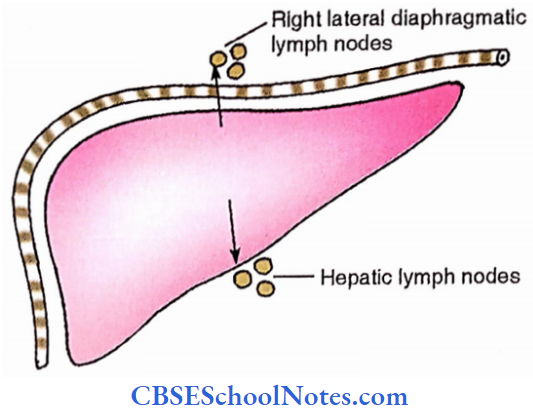
- Parietal pleura– It receives blood supply from the internal thoracic, musculophrenic, and intercostal vessels. Lymphatics drain into the parasternal, intercostal, posterior mediastinal and diaphragmatic lymph nodes.
- Mediastinal and the central parts of the diaphragmatic pleura are innervated by the phrenic nerve while the rest receives nerve supply from the intercostal nerves.
- Pulmonary pleura-It a part and parcel of the lung tissue and therefore its supply is like that of the lung. Its blood vessels are derived from the bronchial vessels.
Its lymphatics drain into the lymph nodes of the lung. It is innervated by the autonomic fibres and therefore insensitive to general stimuli.
Pleura Functions
The pleura acts as a bursa and therefore minimizes the friction between the lung and thoracic wall.
Negative pressure (-10 to -20 mm Hg) in the pleural cavity helps in the expansion of the lung during respiration and prevents its collapse.
Pleura Applied Anatomy
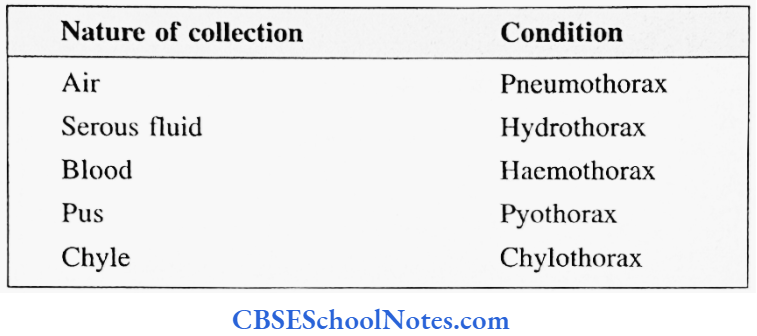
- Inflammation of pleura is called pleuritis or pleurisy.
- The pleural cavity being a potential space, is prone to the collection of air or fluid in pathological conditions:
The cervical pleura is at risk during incision in the region of the root of the neck due to the obliquity of the inlet of the thorax.
- At three sites the parietal pleura extends beyond the costal margins, i.e., the right xiphisternal angle and costovertebral angles of both sides. An abdominal incision at these sites may endanger the pleura.
- Costodiaphragmatic recesses are separated from the upper poles of the corresponding kidney at the costovertebral angles, a fact to be noted in incisions and wounds in this region.
- Aspiration needles and drainage tubes for removing fluid or air from the pleural cavity are passed through the chest wall close to the upper border of the rib to avoid injury to the intercostal nerve and vessels which run along the lower border.
- 4th intercostal space just in front of the midaxillary line is often chosen as there is no major structure here and the level avoids domes of the diaphragm.
- Referred pain from the pleura is a common observation. Pain is referred to the shoulder from phrenic nerve territory and to the abdomen from lower costal and peripheral diaphragmatic pleurae.
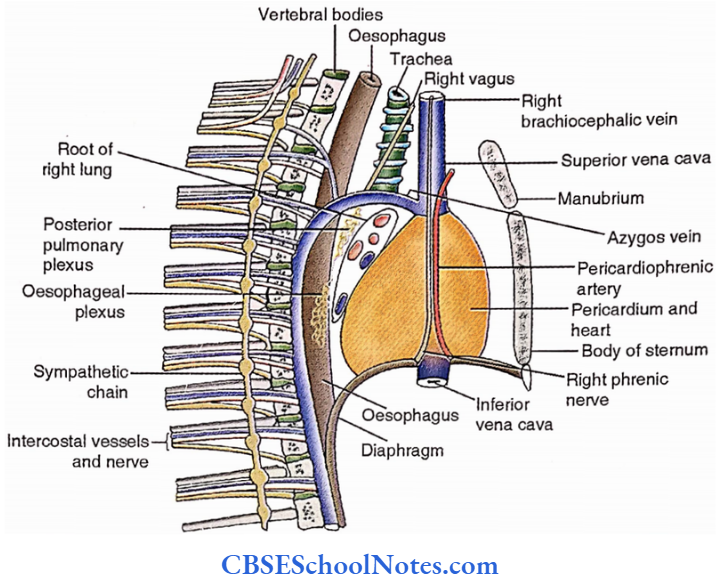
Right And Left Mediastinal Views
Features Of Right And Left Surfaces Of The Mediastinum
Right and left mediastinal views are mirror images of the impressions on the medial surfaces of right and left lungs respectively. Some of the relations are very specific for right and left views. These are as follows:
Right Mediastinal View
- Right atrium
- Inferior vena cava
- Superior vena cava
- Right brachiocephalic vein
- The upper four structures occupy the anterior part of the mediastinal view just behind the sternum.
- Azygos vein- It is a vertical vein over the vertebral bodies behind the heart. Reaching the level of sternal angle it arches forwards above the root of the right lung to enter the superior vena cava.
- Trachea- It lies in the upper part of the mediastinum in a plane posterior to the superior vena cava and right brachiocephalic vein.
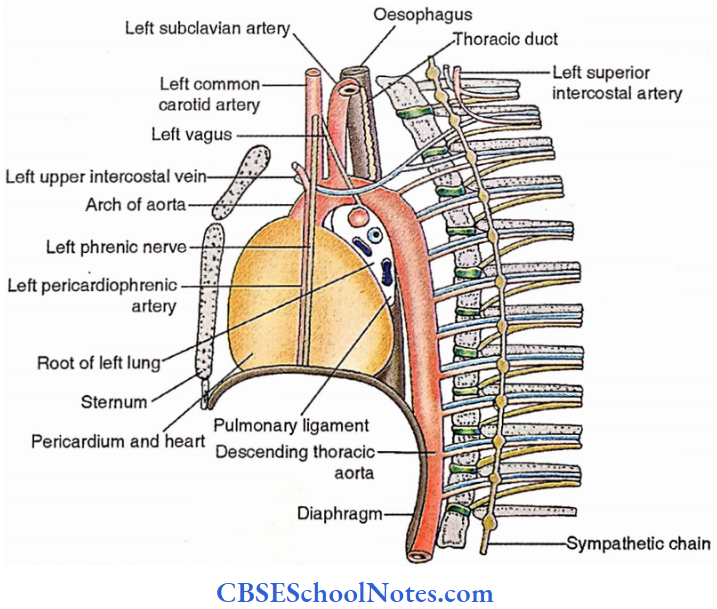
Left Mediastinal View
- Left ventricle- It lies in the anterior part of this view just behind the sternum.
- Arch of aorta- It arches over the root of the left lung.
- Descending thoracic aorta – It is a continuation of the arch of the aorta and lies just behind the heart.
- Left common carotid artery.
- Left subclavian artery.
- Above two arteries ascend from the arch of the aorta of which the former is more anterior. :
- Thoracic duct- It is a vertical lymphatic duct lying in the upper part of this view in a more posterior plane, even behind the subclavian artery.
Dissection Steps For Mediastinum And Heart In Situ
Define the boundaries and subdivisions of the mediastinum. Clean the pericardium and note the phrenic nerve and pericardiophrenic artery.
- Cut the fibrous pericardium on both sides in front of phrenic nerves vertically and join the lower ends of the incision by a transverse cut about 1 cm above the diaphragm.
- Define and note the attachments of the pericardium to the superior vena cava, aorta and pulmonary trunk. Now, maintaining small flaps on these structures cut through them.
- Identify the various pericardial sinuses and correlate them with their development. Remove the fibrous pericardium and study the heart in situ. Note its anatomical position. Identify coronary arteries and major cardiac veins.
The following additional features are alike on the two sides.
- Pericardium. Covers the heart and occupies a large area behind the body of the sternum.
- The root of the lung. Structures entering into or appearing from the lung constitute its root. It is located behind the upper part of the fibrous pericardium.
- It is covered by the connecting pleura which is loose and hanging below- called the pulmonary ligament.
- Sympathetic chain. It descends by the side of the vertebral column.
- Intercostal nerves and vessels. These occupy the intercostal spaces close to the lower border of the ribs.
- Phrenic nerve.
- Pericardiophrenic artery.
- The above two structures descend vertically over the fibrous pericardium.
- Vagus nerve. The right vagus crosses the trachea obliquely to reach the back of the root of the right lung.
- The left vagus crosses the left surface of the arch of the aorta to reach the posterior surface of the root of the left lung. (Phrenic-front and Vagus-behind).
- Oesophagus. It is prominently visible on the right side behind the trachea in the upper part and front of the azygos vein in the lower part.
- On the left side, it is crossed by the thoracic duct in the upper part. It is also visible between the lower part of the fibrous pericardium and the descending thoracic aorta.
Lungs
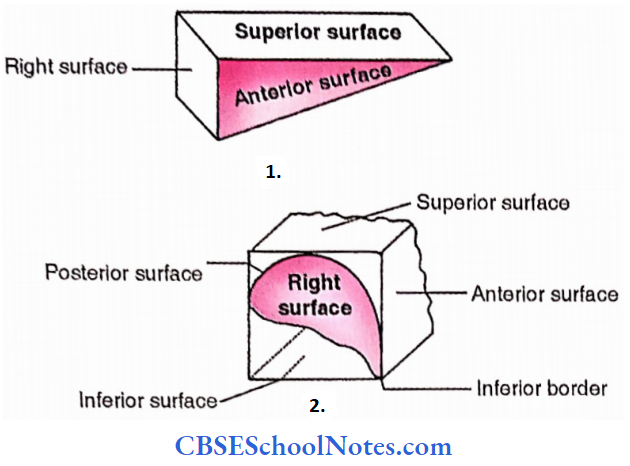
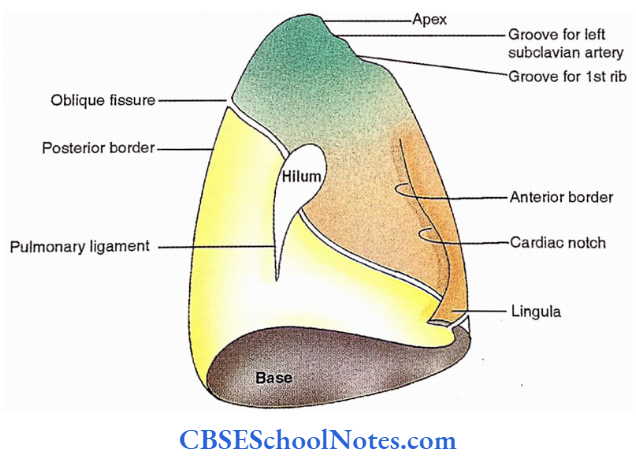
Lungs are essential organs of respiration. Each lung resembles the shape of a half cone and thus has a base, an apex, three borders and two surfaces.
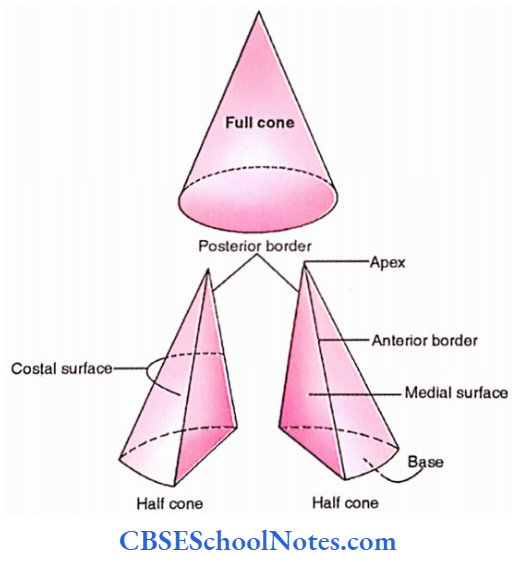
Base. It is deeply concave and faces downwards to rest over the corresponding dome of the diaphragm.
Apex. It is conical and directed upwards towards the root of the neck.
Lungs Borders
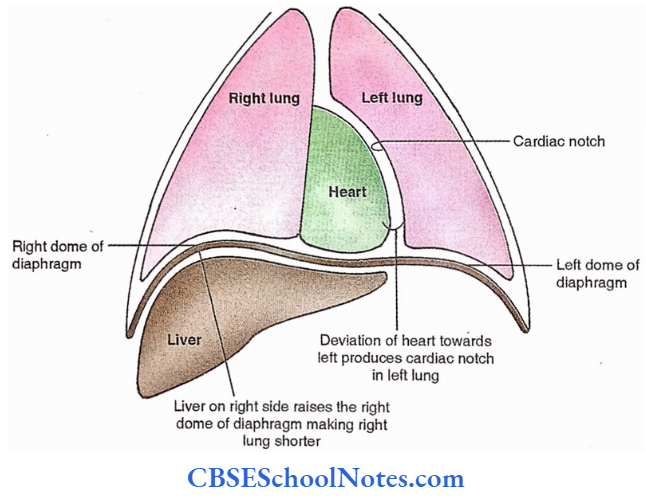
- Anterior border. It is a sharp border related to the anterior thoracic wall. Its lower part is marked by a deep concavity called a cardiac notch in the left lung.
- Posterior border. It is rounded and forms the junction of the costal and medial surfaces and corresponds to the heads of the ribs.
- Inferior border. It is a convex sharp border directed downwards to the costodiaphragmatic recess.
Lungs Surfaces
- Costal surface. This surface is related to the rib cage and the sternum.
- Medial surface. This surface is marked by the hilum, i.e., a depression where structures enter or come out of the lung. The medial surface is divisible into two parts.
- Vertebralpart. It is the posterior part of the medial surface and is related to the vertebral bodies and intervertebral discs.
- Mediastinal part. It is the large anterior part of the medial surface related to the mediastinum.

Side Determination Of Lung
The sides of the lungs are determined based on the following simple morphological features.
- Sharp anterior border faces forward.
- Deep concave base faces inferiorly
- The surface has hilum faces medially.
Fissures And Lobes
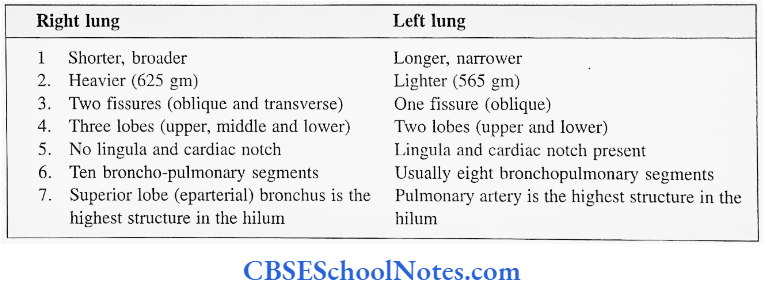
Right lung. Two fissures (oblique and transverse) divide the right lung into three lobes, superior, middle and inferior.
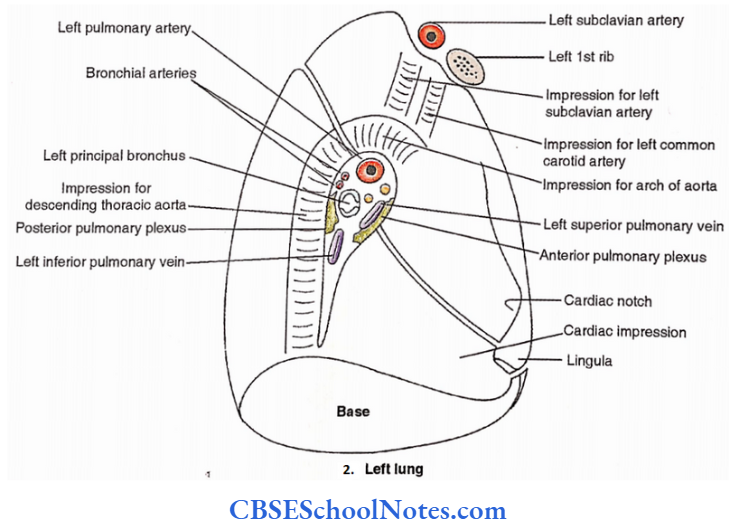
Left lung. There is only one fissure (oblique) in the left lung which divides it into two lobes, superior and inferior. The lower part of the superior lobe is also called the lingula which corresponds with the middle lobe of the right lung.
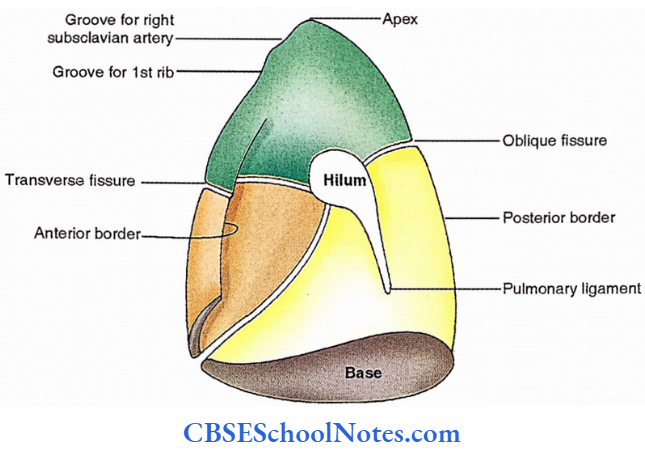
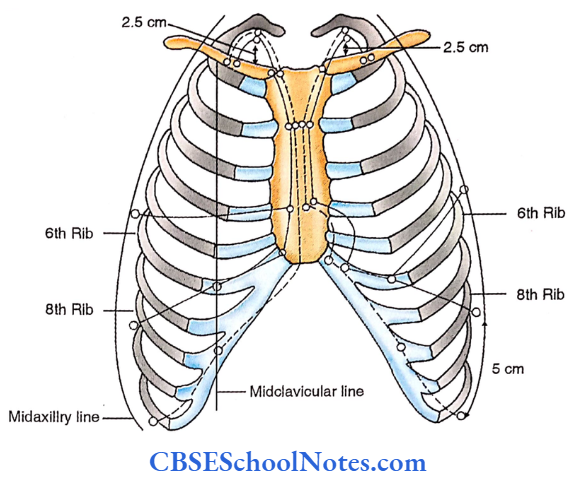
Surface Marking Of Lungs
Apex
It is marked by a line with bold convexity upwards formed by the union of three points, sternoclavicular joint, a point 2.5 cm above the medial l/3rd of clavicle and medial trisection of clavicle.
Anterior Border
Right lung. It is marked by a vertical line formed by the joining of the following three points.
- Right stemocalvicular joint.
- Midpoint of the sternal angle.
- 6th right costochondral junction.
Left lung. It is formed by the union of the following points.
- Left sternoclavicular joint.
- Midpoint of the sternal angle.
- 4th left chondrostemal junction.
- A point on the 6th costal cartilage, 2.5 cm from the left margin of the sternum.
This line becomes concave between points 3 and 4 to represent the cardiac notch.
Inferior border. It is formed by the union of the following four points.
- 1st point is different for the two lungs. For the right lung, it is present on the right 6th chondrostemal junction, while for the left it is located on the 6th costal cartilage 2.5 cm from the left margin of the sternum.
- Crossing of midclavicular line and 6th rib.
- Crossing of midaxillary line and 8th rib.
- At the level of the 10th thoracic spine, 2 cm from the midline.
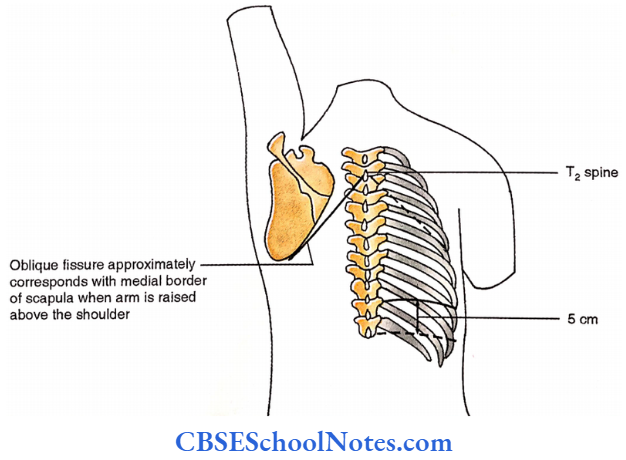
Posterior border. It is represented by a vertical line formed by the union of the following two points.
- 2 cm from the midline at the level of the T10 spine.
- 2 cm from the midline at the T2 spine.
Dissection Steps For The Removal Of Lung
Cut through the rib cage on both sides in the anterior axillary line. Reflect the flap upwards and identify the heart with the pericardium in situ, the lung with pleura in situ, the mediastinum, the internal thoracic artery and its terminal branches.
- Identify the morphological differences, fissures and lobes. Pull the lung laterally and look at the root of a lung on its medial aspect for the arrangement of structures at the hilum.
- The pulmonary ligament and various impressions, and structures related to it. Cut through the root close to the lungs remove the lung and study.
Oblique Fissure
Join the following points to mark the oblique fissure.
- 2 cm lateral to the 2nd thoracic spine.
- 3 cm lateral to the nipple.
- 6th costal cartilage, 7.5 cm from the middle plane.
The oblique fissure roughly corresponds with the medial border of the scapula if the corresponding side of the arm is raised above the head.
Transverse Fissure Of The Right Lung
It is represented by a horizontal line at the level of the 4th costal cartilage, extending from a point on the anterior median line to the midaxillary line.
Relations Of Lung
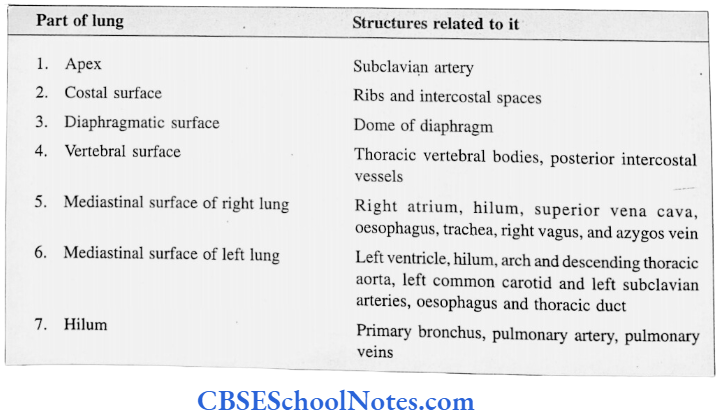

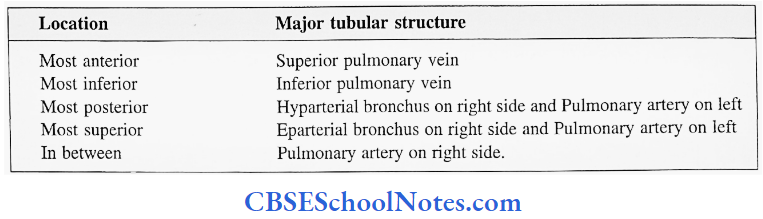
Hilum Of The Lung
It is a depressed site on the medial aspect of the lung joined by its root. Remember, the root is different from the hilum as the former is composed of structures which enter or leave the lung.
Major tubular structures can easily be identified based on their locations as shown below.
Bronchial arteries and hilar (broncho-pulmonary) lymph nodes are closely associated with bronchi.
Anterior and posterior pulmonary plexuses of autonomic nerves occupy respective sides of the lung root and are observed in the hilum.
Differences Between Two Lungs
Tracheobroncheal Tree
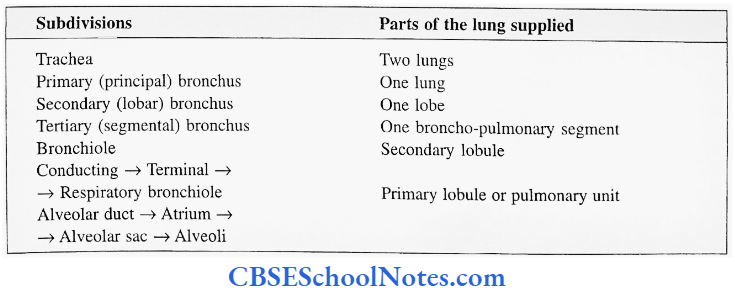
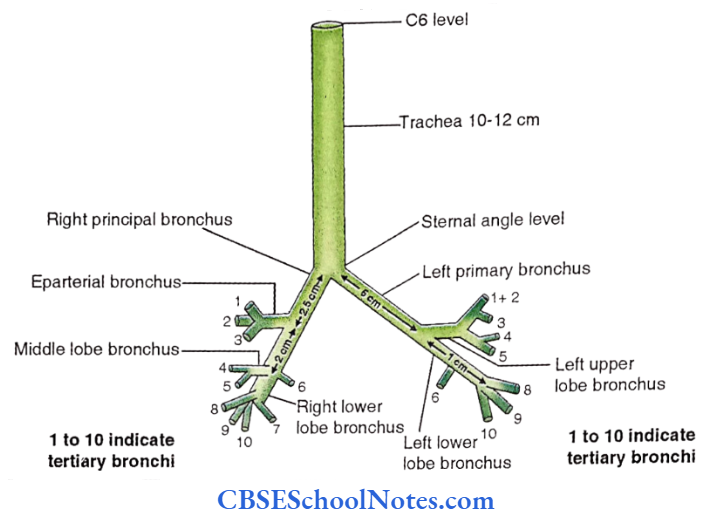
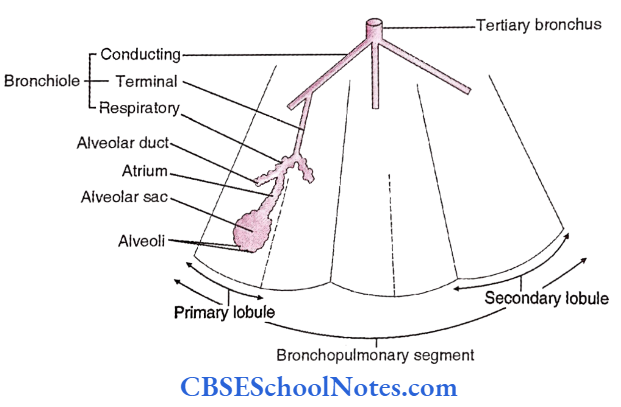
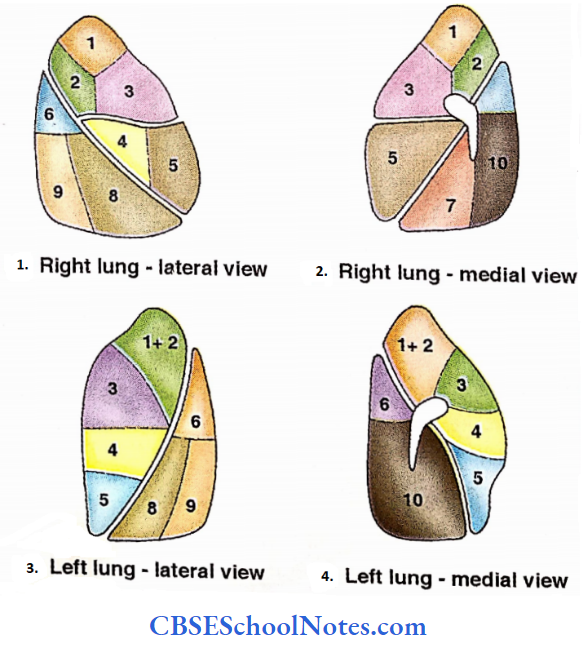
Bronchopulmonary Segments
It is defined as the developmental, structural and functional unit of the lung. It consists of a tertiary bronchus and the lung tissue supplied by it.
There are ten bronchopulmonary segments in the right lung. This number is less on the left side due to compression by the leftward deviated position of the heart which causes either fusion of adjacent segments or suppression of the same.
The number and names of these segments are very specific as shown below.

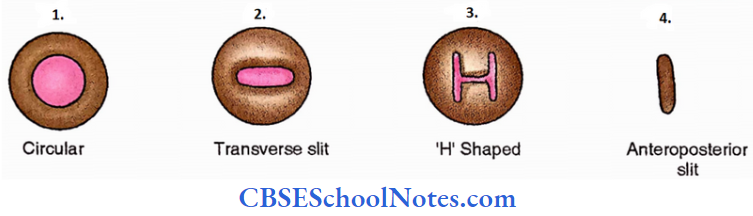
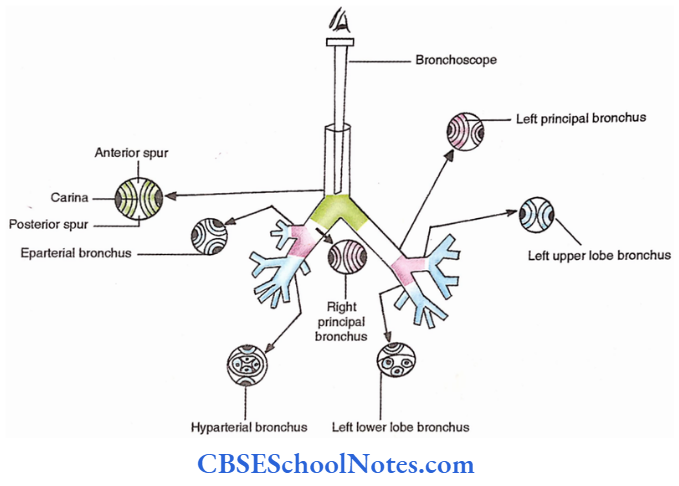
Bronchoscopy
Bronchoscopy is the direct visualization of the interior of the tracheobronchial tree up to the level of the bronchiole with the help of an instrument called the bronchoscope. The visual appearance of the respiratory passage at different levels is shown below.
Lungs Arteries
- Pulmonary arteries. One on each side forms a capillary plexus around the alveoli to facilitate gaseous exchange and supply nutrition (alveoli get oxygen from the atmosphere).
- Bronchial arteries. One on the right side (arising from the 3rd right posterior intercostal artery) and 11 two on the left side (arising from the descending thoracic aorta), supply nutrition as well as oxygen to the rest of the pulmonary tissue.
Lungs Veins
- Pulmonary veins. Two from each lung, a superior and an inferior pulmonary vein.
- Bronchial veins. These drain into the azygos vein on the right side and into the accessory hemiazygos vein on the left side.
Dissection Steps For Bronchopulmonary Segments
Identify the principal bronchus. Remove the substance of the lung piecemeal starting from the principal bronchus. Identify the lobar and segmental bronchi.
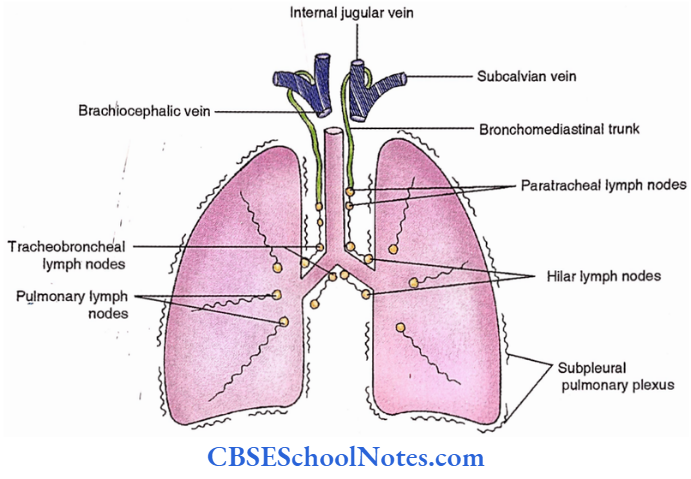
Lymphatic Drainage
Lymphatics. Superficial lymphatic vessels form superficial (subpleural) plexus. Deep lymphatics follow the pulmonary vessels.
Lymph nodes. Lymphatics are interrupted by the following lymph nodes
- Pulmonary lymph nodes- located in the interior of the lung.
- Hilar (bronchopulmonary) lymph nodes- located at the hilum of the lung.
- Tracheobronchial lymph nodes- located at the bifurcation of the trachea. These may be superior or inferior.
- Para tracheal lymph nodes – found in the trachea. Their efferents ultimately form corresponding bronchomediastinal lymph trunk which opens at the jugulo-subclavian junction.
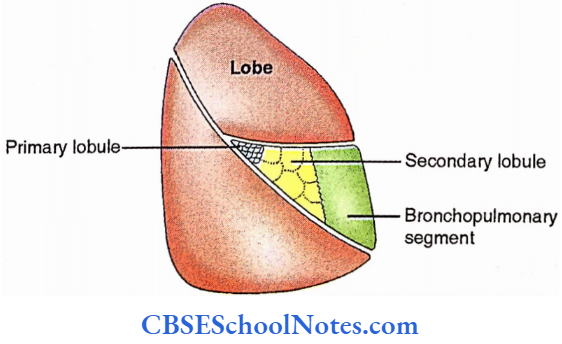
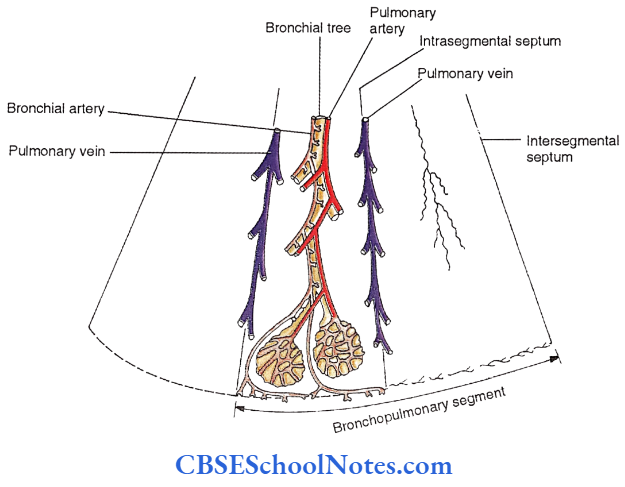
The vessels of the lung should always be considered in terms of bronchopulmonary segments which are isolated by the connective tissue intersegmental septa.
- Intrasegmental septa demarcate the lobule (primary and secondary) of the lung. It is interesting to note that the veins follow inter as well as intrasegmental septa and drain many adjacent segments.
- The bronchial tree, pulmonary artery and bronchial artery run in the centre of the lobule. Lymphatics follow both septa as well as the bronchial tree.
Lungs Innervation
The lung is supplied by the anterior and posterior pulmonary plexuses which are located on the front and back of the root of the lung respectively.
Both sympathetic and parasympathetic fibres innervate the lung. The former are derived from the 2nd to 5th thoracic spinal segments. Parasympathetic fibres come from the vagus nerve.
Functionally, stimulation of the sympathetic fibres causes bronchodilation and vasoconstriction while parasympathetic fibres result in bronchospasm, vasodilatation and increased secretion by the bronchial glands.
Lungs Applied Anatomy
Medicolegal importance. The presence of air in the lung observed during postmortem confirms the
live birth of the baby.
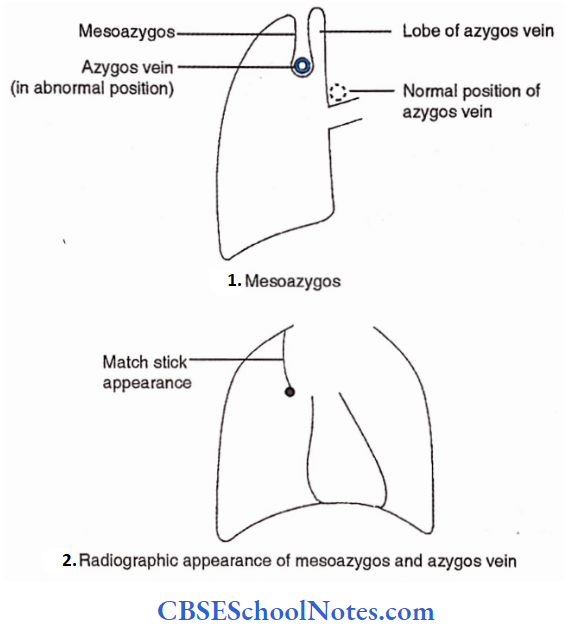
- The lobe of the Azygos vein. Rarely azygos vein descends through the apex of the right lung and occupies the depth of the parietal pleural fold (mesoazygos).
- This is responsible for the matchstick appearance in the chest radiograph (P-A view). The lung tissue medial to the mesoazygos is termed the lobe of the azygos vein.
- A stab wound above the clavicle might damage the apex of the lung.
- A foreign body in the trachea usually enters the right principal bronchus because of its relatively larger lumen and vertical position as compared to the left bronchus.
Surgical removal of the diseased lung or its part is a common procedure.
Bronchography. The tracheobronchial tree can be visualized by taking a radiograph of the chest after introducing radio-opaque dye (For example., diagnosis aqueous) into it.
- Pulmonary thromboembolism. This is a common postoperative complication in which a thrombus detached from the site of operation blocks the pulmonary artery. The patient usually undergoes respiratory distress which commonly proves fatal.
- Bronchogenic carcinoma. Its frequency is 30% of all common cancers occurring in men.
- The metastatic intracerebral abscess is sometimes a well-recognized complication of lung abscess.
- The two commonest signs of lung injuries are haemoptysis (sputum with blood) and subcutaneous emphysema (air under the skin).
- Aspiration pneumonia (inhaled vomitus). It is a common postoperative chest complication.
- Atelectasis (collapse of the lung). It is also a postoperative complication which may be segmental, lobar or massive.
Referred abdominal pain due to diaphragmatic inflammation caused by pleuropneumonia should always be differentiated from peritonitis as the rebound pain (pain in the abdomen when the pressure over the abdominal wall is suddenly released) is a specific sign of peritonitis.
Mediastinum
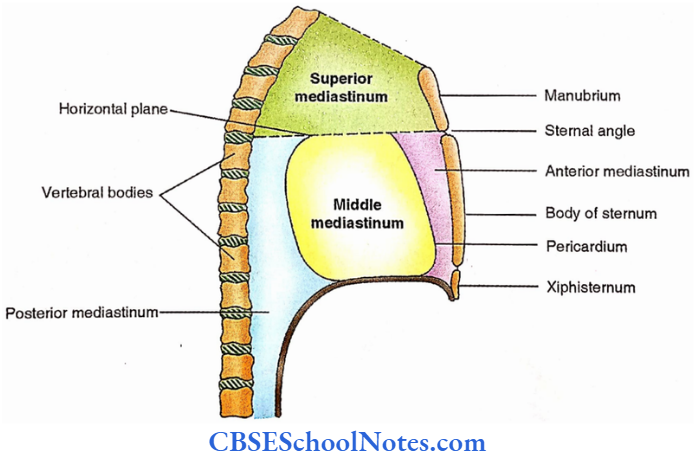
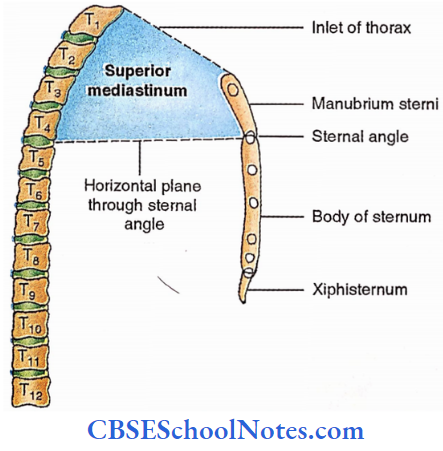
It is defined as the median septum in the thoracic cavity between the two pleural cavities.
The horizontal plane at the level of the sternal angle (which corresponds to the intervertebral disc between the 4th and 5th thoracic vertebrae) divides the septum into an upper part (superior mediastinum) and a lower part (inferior mediastinum).
The inferior mediastinum is further subdivided into the following three regions;
- Middle mediastinum. Partly occupied by the fibrous pericardium.
- Anterior mediastinum. Part anterior to the fibrous pericardium.
- Posterior mediastinum. Part behind the fibrous pericardium.
Anterior Mediastinum
Anterior Mediastinum Boundaries.
Anterior– Body of sternum.
Posterior– Fibrous pericardium.
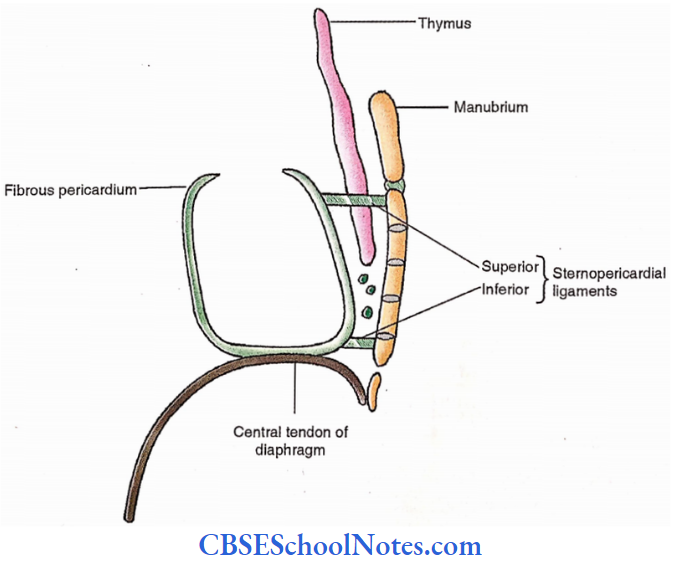
Anterior Mediastinum Contents.
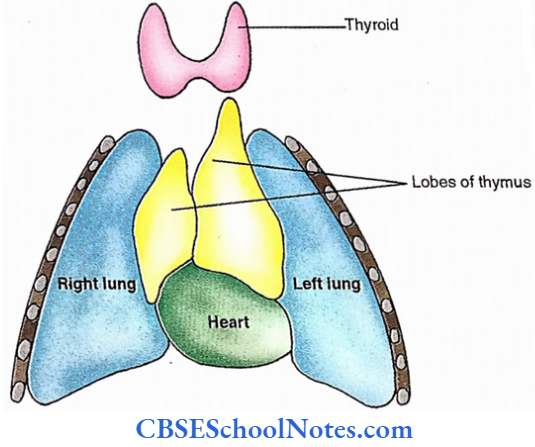
- Thymus
- Lymph nodes
- Loose areolar tissue
- Pericardial branches of the internal thoracic artery
- Sternopericardial ligaments.
These ligaments are usually two in number (superior and inferior) connecting the sternum with the fibrous pericardium.
Anterior Mediastinum Thymus
It is a primary central lymphatic organ as well as an endocrine gland. It develops from the 3rd pharyngeal pouch. Though single, it is comprised of two asymmetric lobes called the thymic bodies.
It occupies the lower neck and upper thorax (up to 4th costal cartilage). At puberty, it is most prominent and weighs about 30 grams.
It is only 10 g at birth and middle age. It is the site of the production of T lymphocytes as well as factors and hormones.
Pericardium
The pericardium is the covering of the heart. Its outer component is tough and inelastic and called the fibrous pericardium. The inner component, called serous pericardium is comprised of two parts.
The one which lines the inner surface of the fibrous pericardium is called the parietal layer and the other which covers the heart is termed the visceral layer.
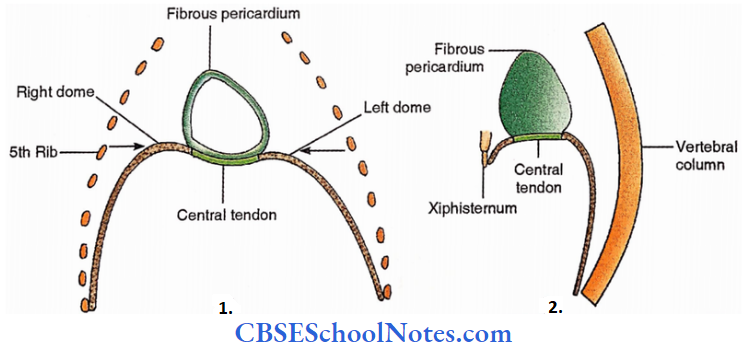
Fibrous Pericardium
It is derived from the septum transversum and extends from the 2nd to the 6th costal cartilage. It is said to have;
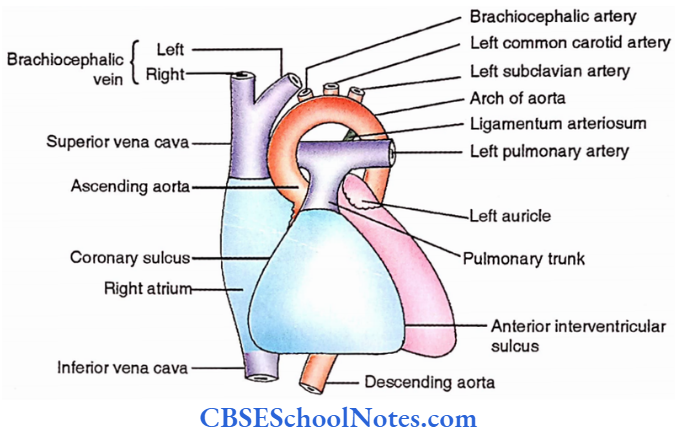
- Base. It faces inferiorly and is pierced by the inferior vena cava.
- Apex. It is directed upwards and is pierced by the ascending aorta, pulmonary trunk and the superior vena cava.
- Four surfaces
- Anterior surface. Related to the anterior mediastinum.
- Posterior surface. Related to the posterior mediastinum and is pierced by four pulmonary veins.
- Right lateral surface. Related to right lung and pleura.
- Left lateral surface. Related to left lung and pleura.
The fibrous pericardium is fixed to the central tendon of the diaphragm, adventitia of great vessels (except the inferior vena cava which is free from it) and the sternum (by the sternopericardial ligaments).
The fibrous pericardium protects the heart and provides a slippery surface for the movements of both the heart and lungs.
Serous Pericardium
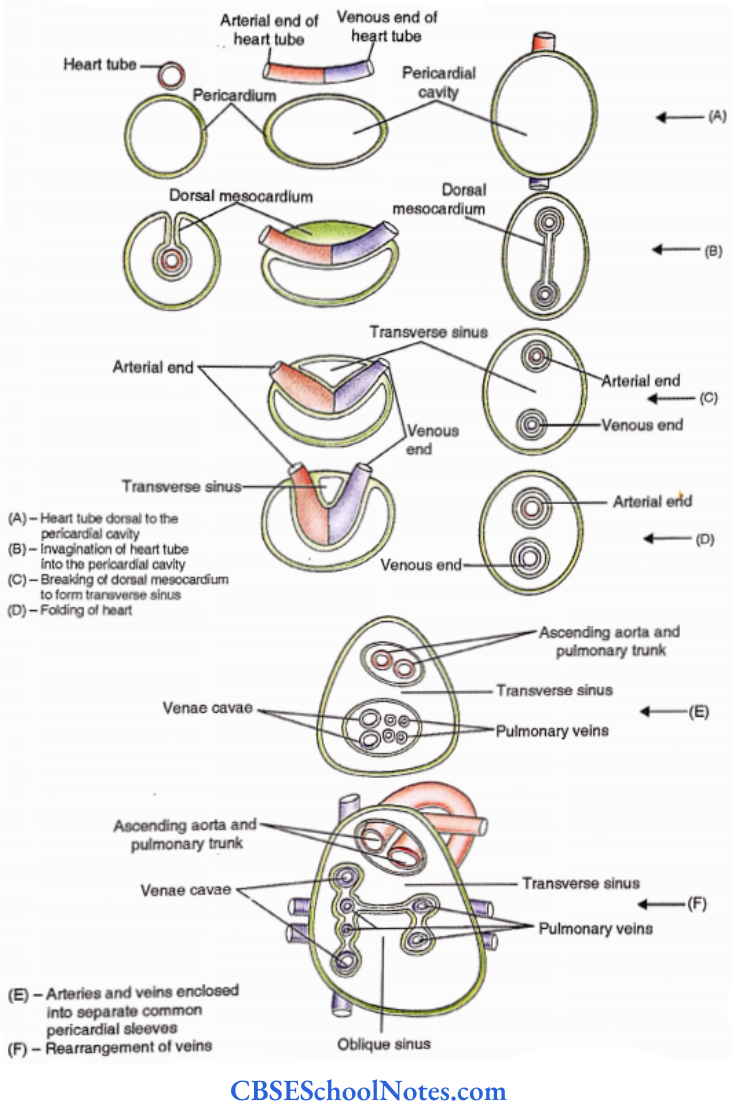
- Truly speaking, it is a bursa around the heart to allow its free movement. The pericardial cavity may be divided into three parts
- Main ‘general’ cavity.
- Transverse sinus. It is located between the pulmonary trunk and the ascending aorta anteriorly and the superior vena cava and left atrium posteriorly.
- Oblique sinus. It is a cul-de-sac behind the left atrium whose opening is directed downwards and towards the left between the inferior vena cava and the left inferior pulmonary vein. It allows atrial pulsation.
The heart invaginates into the pericardial cavity from its posterior aspect. Steps involved in the formation of the pericardial sinus are shown.

Pericardial Vessels And Nerves
- The fibrous pericardium and the parietal layer of the serous pericardium receive arterial supply from the internal thoracic artery through its pericardial, musculophrenic, and pericardiophrenic branches and also from branches of descending thoracic aorta.
- Pericardial veins drain into the azygos system. Their nerve supply comes from the branches of the phrenic nerve.
- The visceral layer of serous pericardium is supplied by the coronary arteries and drained by the coronary sinus. It receives autonomic innervation from the vagus and the sympathetic trunk similar to the heart.
Pericardium Applied Anatomy
- Pericarditis. It is inflammation of the pericardium. It leads to chest pain. It produces characteristic ‘pericardial rub’, a high-pitched sound heard on auscultation, due to the friction between two inflamed pericardial layers.
- A chronic condition in which due to excessive fibrosis, the dilatation of the heart is restricted, is called ‘constrictive pericarditis’.
- Pneumopericardium. Entry of air into the pericardial cavity is sometimes a complication of pneumothorax.
- Pericardial effusion. It is a collection of clear fluid in the pericardial cavity. When too much, it restricts the cardiac dilatation, a condition called the ‘cardiac tamponade’.
- Haemopericardium. The blood can enter the pericardial cavity either due to a stab wound of the heart or perforation of the infarcted and fibrosed thin wall of the heart.
- Pericardiocentesis. It is the procedure to drain excess fluid in the pericardial cavity.
- The needle is preferably introduced in the left 5th or 6th intercostal space adjacent to the sternum or left xiphicostal angle. These sites are devoid of pleura.
- Transverse pericardial sinus is surgically very important as it helps in temporary ligation of the ascending aorta and the pulmonary trunk for cardiopulmonary bypass.
- This is needed in coronary bypass surgery.
- Exposure of the superior and inferior vena cava. Both the venae cavae are preferably exposed from inside the pericardial cavity, i.e., by opening it.
Heart
Heart Surface Features
The heart is a hollow conical muscular organ.
Heart Measurement
Base to apex – 12 cm
Maximum transverse diameter – 8 cm
Anteroposterior – 6 cm
Heart Weight
Male – 300 g
Female – 250 g
Heart Surfaces And Borders
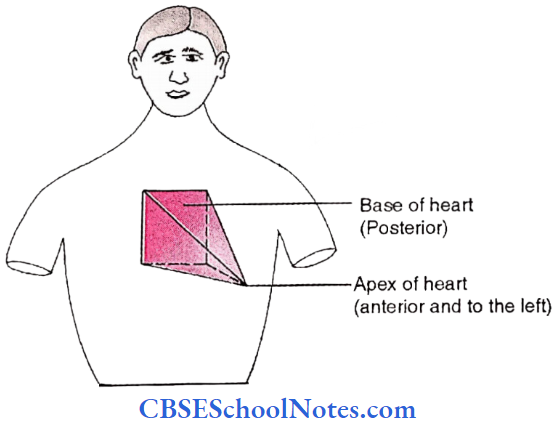
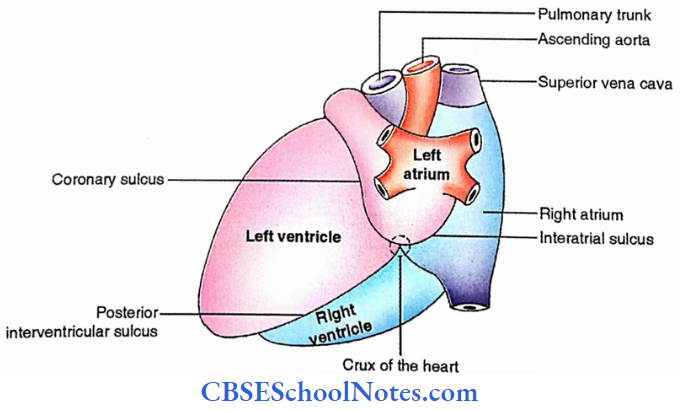
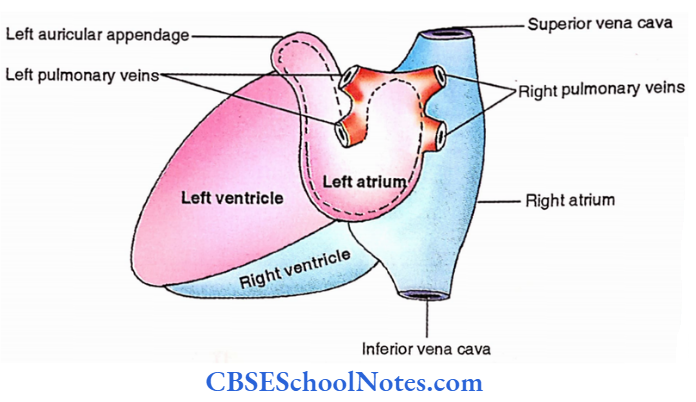
Base. It is posterior. It is formed mainly by the left atrium.
Apex. It is directed forward and towards the left (opposite the base). It is formed by the left ventricle.
Borders. It has four borders.
- Superior border (clinicians consider it as the base). It is formed by atria.
- Inferior border. Formed by ventricles.
- Right border. Formed by the right atrium.
- Left border. Formed by the left ventricle.
Surfaces
- Sternocostal surface. It faces forward. It is formed from right to left by right atrium, right ventricle (2/3rd) and left ventricle (l/3rd).
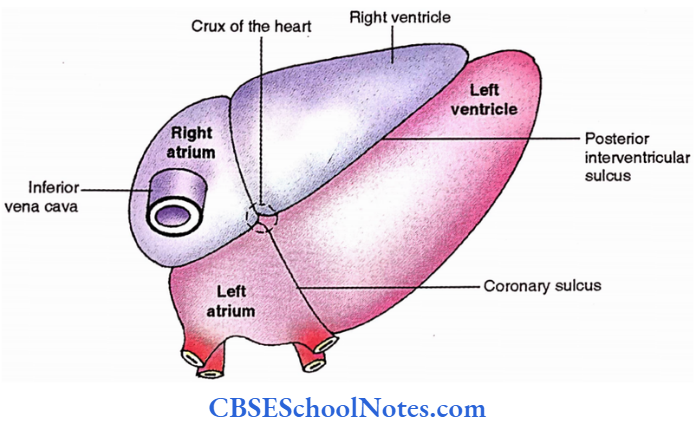
- Diaphragmatic surface. It faces inferiorly. It is formed mainly by the left and right
ventricle contributing 2/3rd and l/3rd of this surface respectively. - Right and left surfaces. These are also called the pulmonary surfaces.
Grooves and sulci
- Interatrial groove. It is located between right and left atria.
- Atrioventricular sulcus. It is the junction between the atria and the ventricles. This is also called the coronary sulcus.
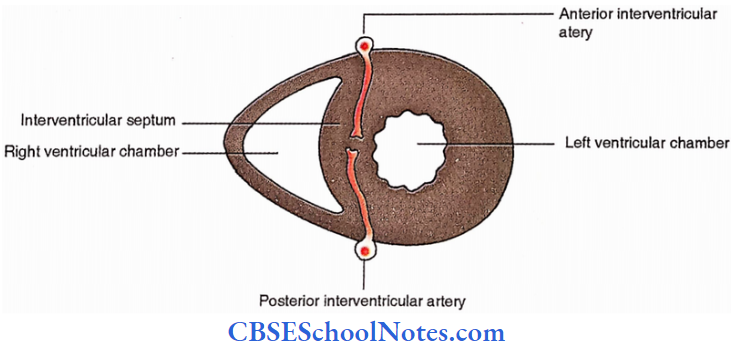
- Interventricular groove. It is the junction between two ventricles. Its sternocostal component is called the anterior interventricular sulcus.
- The groove on the inferior surface is called the posterior interventricular sulcus.
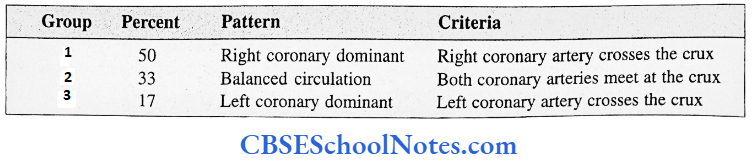
- The site where the coronary sulcus meets with the posterior interventricular sulcus is called the ‘crux’ of the heart.
Surface Projection Of The Heart
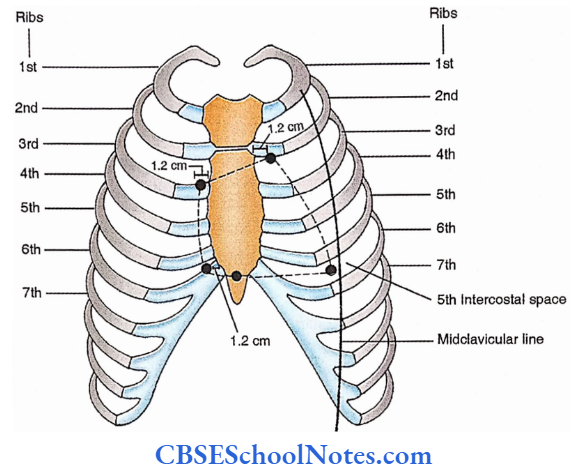
Mark the following points
Point 1. The lower border of the left 2nd costal cartilage is 1.2 cm from the side of the sternum.
Point 2. The upper border of the right 3rd costal cartilage is 1.2 cm from the side of the sternum.
Point 3. Right 6th costal cartilage, 1.2 cm from the side of the sternum.
Point 4. Midpoint of the xiphisternal joint.
Point 5. The apex of the heart, 5th left intercostal space, just medial to the midclavicular
line.
Join the above-mentioned points to draw the heart on the surface of the chest.
1 + 2 = Upper border of the heart.
2 + 3 = Right border of the heart.
3 + 4 + 5 = Inferior border of the heart.
5 + 1 = Left border of the heart.
Heart Applied Anatomy
- The heart deviates to one side with the mediastinal shift. Mediastinum is pushed to the opposite side by the tumours in the lung or pulled towards the same side by fibrosis or collapse of the lung.
- Cardiomegaly. The heart is enlarged due to multiple conditions, For example., aortic stenosis, aortic regurgitation and hypertension.
- Cardiac dullness. The heart can be mapped out by tapping the front of the thorax (percussion).
- The central area of the heart which is not covered with the lung can easily be detected by light percussion. This is called superficial cardiac dullness.
- Forceful percussion is needed to map out the exact size of the heart, i.e. even that part of the heart which is covered with the lung. This is called deep cardiac dullness.
Arterial Supply Of The Heart
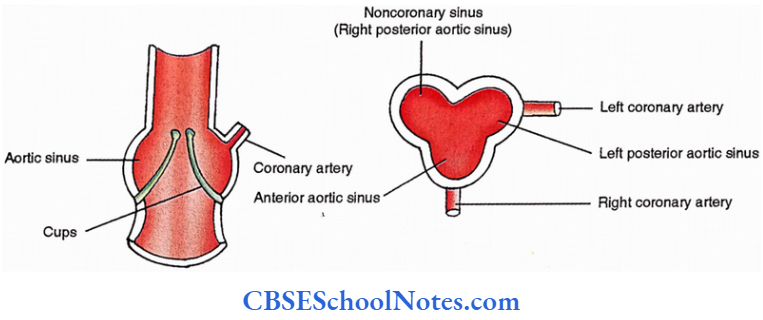
Two arteries supply the heart. These are called the right and left coronary arteries.
These originate from two of the ascending three outpouchings (anterior, right posterior, and left posterior aortic sinuses)at the commencement of the ascending aorta.
The right coronary artery emerges from the anterior aortic sinus while the left one appears from the left posterior aortic sinus.
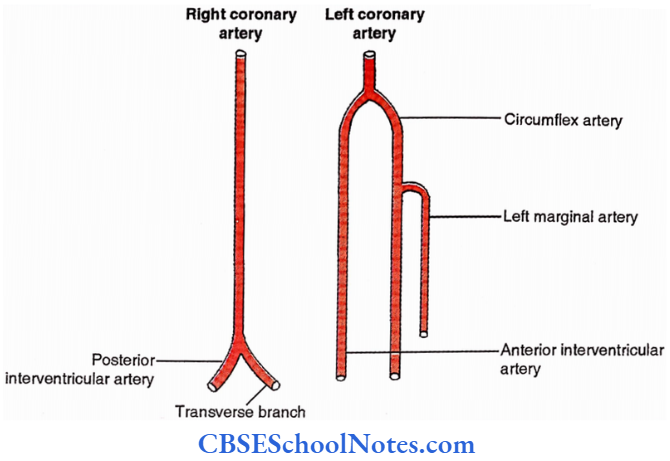
Right Coronary Artery
Course. The artery appears between the pulmonary trunk and the right auricle and runs a rightwards course in the right portion of the coronary sulcus on the sternocostal surface of the heart.
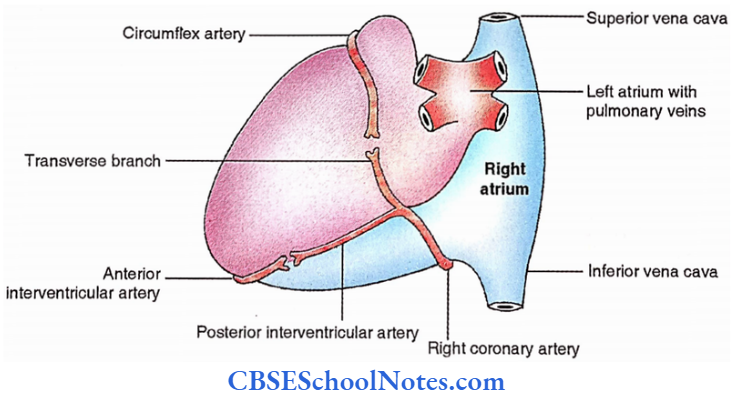
After winding around the inferior margin of the heart it runs a leftwards course on the diaphragmatic surface of the heart to reach the crux.
Branches
- Conus branch – for the upper portion of the right ventricle.
- Periventricular branch- for the front of the right ventricle.
- Right marginal branch. It runs towards the left close to the inferior margin of the heart.
- Nodal branches. In the majority of the cases, it emerges from the right coronary artery.
- SA node -55%
- AV node- 90%
- Small branches to the ascending aorta, pulmonary trunk and the right atrium.
- Terminal branches. At the crux of the heart, the right coronary artery terminates into a transverse branch (which continues into the left portion of the coronary sulcus to anastomose with the circumflex branch of the left coronary artery).
- And posterior interventricular artery (which runs into the posterior interventricular sulcus and anastomoses with the anterior interventricular branch of the left coronary artery).
Left Coronary Artery
Course. It appears between the pulmonary trunk and the left auricle. It runs a leftward course in the left portion of the coronary sulcus.
At the upper end of the anterior interventricular sulcus, the artery terminates.
Branches. Two terminal branches are emerging from the left coronary artery.
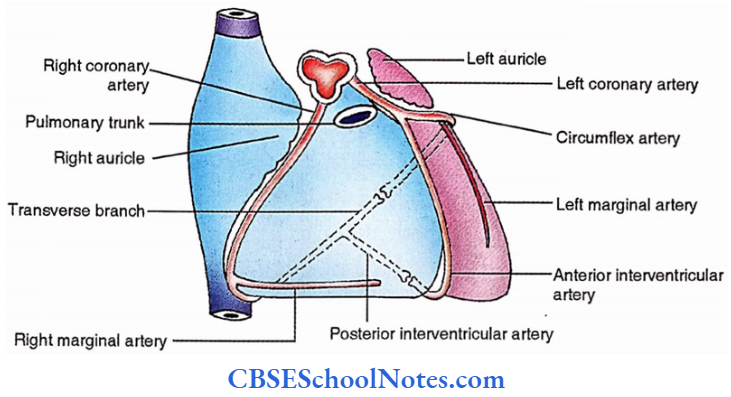
Anterior Interventricular Artery
It descends in the anterior interventricular sulcus and winds around the inferior margin of the heart to run in the posterior interventricular sulcus and anastomose with the posterior interventricular branch of the right coronary artery.
Circumflex Artery
It continues leftwards in the coronary sulcus and after winding around the left margin of the heart, runs a rightwards course to anastomose with the transverse branch of the right coronary artery.
It gives a descending branch along the left margin of the heart called the left marginal artery.
Schlesinger’s Grouping Of Arterial Pattern
Schlesinger divided the heart into three groups depending upon the relation of the coronary arteries with the crux of the heart as shown below
Collateral Circulation
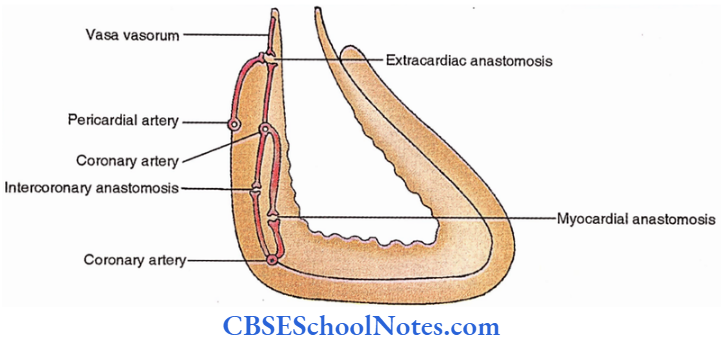
Cardiac anastomosis
- Myocardial anastomosis. Branches of the coronary arteries anastomose in the substance of the cardiac muscle.
- Intercoronary anastomosis. Branches of coronary arteries anastomose in the sulci, i.e. in the epicardial fat.
Extracardiac Anastomosis
Such anastomosis is noticed at the site where great vessels of the heart pierce the fibrous pericardium. Anastomosis takes place between the branches of coronary arteries on one hand and the vasa vasorum of great vessels or the pericardial arteries on the other hand.
Collateral Circulation Applied Anatomy
Angina pectoris. It is chest pain due to the narrowing of coronary arteries or its branches. Pain is usually produced when the lumen of a coronary artery is reduced to Vl or l/3rd of its original size.
Myocardial infarction. It is the ischaemia of the heart due to complete obstruction of the coronary arteries or its branches. The following three arteries are usually involved in descending order of their frequency-
- Anterior interventricular artery.
- Right coronary artery.
- Circumflex artery.
Coronary angiography. It is a visualization of the coronary arteries and their branches in a radiograph after introducing a radio-opaque dye. The dye is pushed with the help of an intravascular catheter at the level of the aortic sinus during the diastolic phase of the heart.
Coronary angioplasty. In this case, a small balloon at the tip of an intravascular catheter is carried at the site of the narrowing of the coronary artery and inflated to dilate.
The artery allows the resumption of normal blood flow to the cardiac tissue. Thrombokinase is also introduced to dissolve the clot.
Coronary bypass surgery. In this operation, normal blood flow is resumed in the coronary artery or its branches distal to the site of obstruction.
This can be achieved either by providing a bridge of venous graft (usually the great saphenous vein) across the obstruction or connecting an adjacent artery (usually the internal thoracic artery) with the diseased artery distal to the obstruction.
Venous Drainage Of The Heart
The following veins drain the heart.
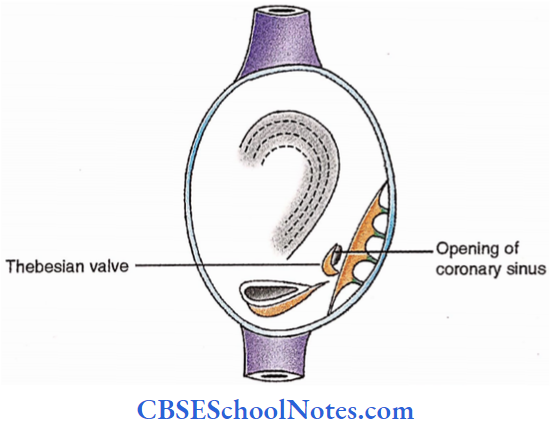
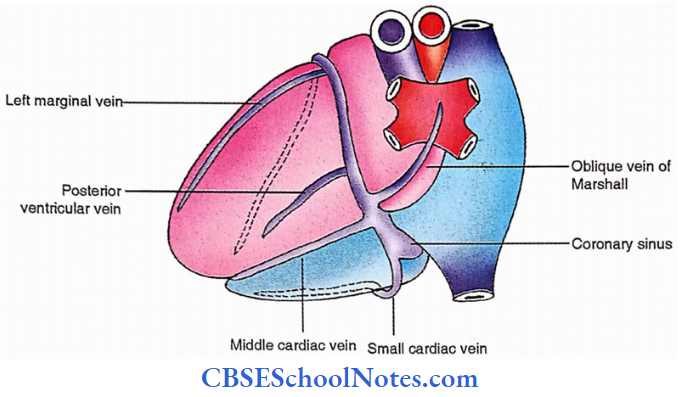
1. Coronary sinus. It is a wide venous channel, 2-3 cm in size, located in the posterior part of the coronary sulcus. It opens into the right atrium between the inferior vena cava and right atrioventricular orifices. Its opening is guarded by a small valve called the Thebesian valve.
Tributaries
- Great cardiac vein. It accompanies the anterior interventricular artery and circumflex artery to continue with the upper part of the coronary sinus. It is interesting to note that the blood flows in the same direction in this vein as well as the circumflex artery.
- Small cardiac vein. It accompanies the right marginal artery and winds around the inferior border of the heart to enter the terminal part of the coronary sinus.
- Middle cardiac vein. It accompanies the posterior interventricular artery and joins the middle of the coronary sinus.
- Oblique vein of Marshall. It descends from the back of the left atrium.
- Posterior ventricular veins. These drain the posterior surface of the left ventricle.
- Left marginal vein. It ascends close to the left border of the heart and joins the upper part of the coronary sinus.
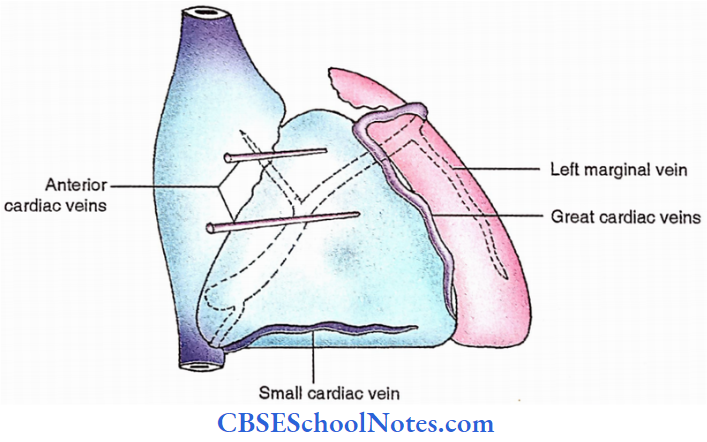
2. Anterior cardiac veins. Usually, two, run towards the right from the front of the right ventricle and drain directly into the right atrium.
3. The besian veins (venae cordis minimae). These are numerous small veins located in the wall of the heart and opening directly into the cardiac chambers. The majority of these are located in the wall of the right atrium.
Dissection Steps For The Blood Supply Of The Heart
Remove the visceral pericardium from the surface of the heart and identify the right coronary artery between the pulmonary trunk and the right auricle.
- The left coronary artery between the pulmonary trunk and left auricle and coronary sinus in the posterior part of the coronary sulcus.
- Scrape the fat present in the anterior interventricular sulcus and left part of the coronary sulcus and identify the anterior interventricular branch of the left coronary artery great cardiac vein and circumflex branch of the left coronary artery.
- Trace the anterior interventricular artery to the diaphragmatic surface of the heart. Remove the fat from the coronary sulcus and identify the right coronary artery; trace it to the anterior aortic sinus.
- Trace the posterior interventricular branch of the right coronary artery on the diaphragmatic surface in the posterior interventricular groove with the accompanying vein. Note the coronary dominance.
- Identify the crux of the heart and clean and trace the coronary sinus in the posterior part of the coronary sulcus.
Innervation Of The Heart
Nature – Autonomic
Source – Sympathetic. 3 cervical and upper 5 thoracic sympathetic ganglia (T1– T5). Parasympathetic – Vagus.
Nerve Plexuses
- Cardiac Plexuses
- Superficial cardiac plexus. This is located in the concavity of the arch of the aorta to the right of the ligamentum arteriosum.
- It receives only two cardiac branches. 1st is derived from the left superior cervical sympathetic ganglion and 2nd is the lower of the two cardiac branches of the left vagus.
- Deep cardiac plexus. It is located on the posterior and right surface of the arch of the aorta. It is divisible into right and left halves.
- All the rest of the cardiac branches from sympathetic ganglia, vagus and recurrent laryngeal nerves contribute to its formation.
- Coronary Plexuses
- Right coronary plexus. It accompanies the right coronary artery. It receives fibres from the superficial cardiac plexus and the right half of the deep cardiac plexus.
- Left coronary plexus. It receives fibres mainly from the left half of the deep cardiac plexus.
Distribution
- Efferent Fibres
- Parasympathetic fibres. These supply the SA node, AV node, atria and fine branches of the coronary arteries.
- Sympathetic fibres. These supply the atria, ventricles and large branches of the coronary arteries.
- Afferentfibres.
- Pressure sensations from the great vessels run into the vagus. Pain fibres from the heart follow the sympathetic nerves.

Functions
- Sympathetic.
- Acceleration of the heart.
- Coronary artery dilatation.
- Parasympathetic
- Slows the heart.
- Causes coronary artery constriction.
Innervation Of The Heart-Applied Anatomy
Cardiac pain is referred to the medial side of the arm. This is because the heart receives sympathetic fibres from the segments of the spinal cord (T1-T5) whose major portion (T1 – T3) also supplies the medial side of the arm.
Chambers Of The Heart
There are four chambers in a heart, the right atrium, the right ventricle, the left atrium and the left ventricle. Both the right chambers constitute the right heart while the left ones form the left heart.
Though the atrium and ventricles of the same side communicate with each other through the atrioventricular orifice, the atria and ventricles themselves are separated by a complete interatrial and interventricular septum respectively.
The Right Atrium
External Features
It occupies the extreme right part of the heart. A vertical sulcus (sulcus terminalis) connects the front of the superior vena cava with that of the inferior vena cava.
The sulcus demarcates its right smooth part (derived from sinus venosus) from the left rough part (derived from the primitive atrium). The extension of the rough part upwards and towards the left forms its auricular appendage.

Internal Features
The sulcus terminalis corresponds with a vertical ridge (crista terminalis) when observed from inside the cavity of the right atrium. This ridge again demarcates the interior of the cavity into an anterior (rough part) and a posterior (smooth part).
Rough part – It is marked by transversely running ridges called the musculi pectinati.
Smooth part – This is also called sinus venarum. It shows the following features.
- Opening of the superior vena cava – It is present at its upper end.
- Opening of the inferior vena cava – It is present at its lower end. It is marked by an incomplete valve.
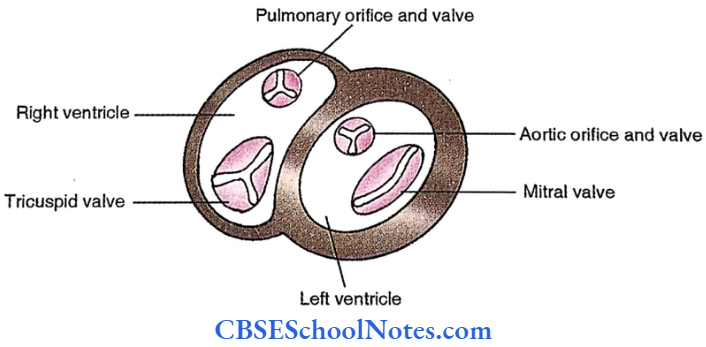
- Tricuspid orifice – This is the largest opening in the right atrium allowing three fingers to pass. It is located anteriorly.
- Opening of the coronary sinus. This is a small opening located in the posterior wall between the tricuspid and inferior vena caval orifices allowing only a little finger to pass. It is guarded by a valve called the Thebesian valve.
- Fossa ovalis. This is a thumb-sized depression in the posterior wall. It represents the septum primum of the developing interatrial septum.
- Limbusfossa ovalis. It is a crescent margin demarcating the anterosuperior aspect of the fossa ovalis. It represents the inferior free margin of the septum secondum.
- Intervenous tubercle. This is a faint elevation between the fossa ovalis and the superior vena canal orifice.
- The tubercle probably plays an important role in directing the blood from the superior and inferior vena cavae (to the right ventricle and left atrium respectively) during foetal circulation.
- Triangle of Koch. This is a small triangular location for the atrioventricular node. This is bounded by the septal leaf of the tricuspid valve, the opening of the coronary sinus and the tendon of Todaro.

Dissection Steps For Right Atrium
Remove the heart by cutting through the ascending aorta and pulmonary trunk. Note its anatomical position. Identify the external features of the heart – apex, base, borders and surfaces and sulci/ grooves.
- Dissect the arch of the aorta beyond the branches of the aortic arch. Now cut the left pulmonary artery beyond ligamentum arteriosum.
- Open the right atrium by giving a longitudinal incision from the lower end of the superior vena cava along the sulcus terminalis up to the opening of the inferior vena cava in the right atrium.
- Remove the blood clots if any reflect the flap to the left side and study the interior of the right atrium for various features – openings, rough and smooth surfaces and their developmental correlation.
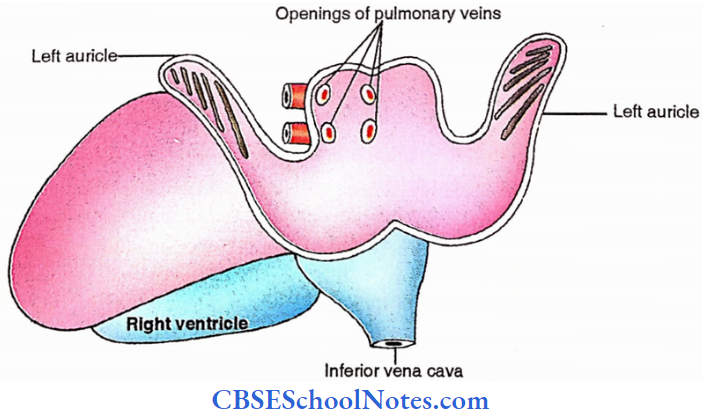
The Left Atrium
External Features
It is located posterior and to the left of the right atrium. Two right and two left pulmonary veins join the upper halves of their corresponding margins.
An extension from its lower half winds around the left border of the infundibulum to appear on the sternocostal surface of the heart. This is called the auricular appendage.
Internal Features
Roughpart. It is the auricular appendage showing elongated ridges. It’s derived from the primitive atrium.
Smooth part. The rest of the atrium is devoid of ridges. It is derived by the incorporation of pulmonary veins. The upper halves of its margins are marked by the opening of a pair of corresponding pulmonary veins.
The Right Ventricle
External Features
It contributes to the 2/3rd of the sternocostal surface and l/3rd of the diaphragmatic surface of the heart. Its sternocostal surface is triangular with a base towards the inferior border and an apex towards the pulmonary trunk.
Its junction with the right atrium is marked by the coronary sulcus while its junction with the left ventricle is marked by the anterior (on the sternocostal surface) interventricular sulcus.
Internal Features
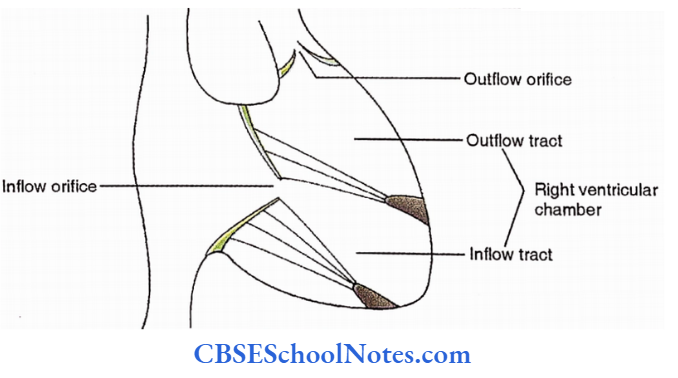
These are described under the following 4 headings.
- Inflow orifice (right atrioventricular orifice).
- Inflow tract (rough part).
- Outflow tract (smooth part).
- Outflow orifice (pulmonary orifice).
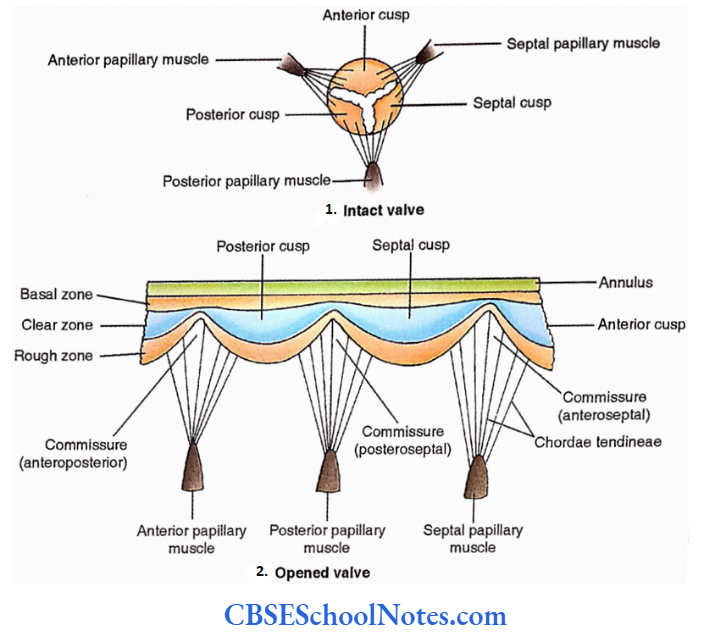
Right Atrioventricular Orifice
It is the largest opening of the heart. It connects the right atrium with the right ventricle and directs the blood to flow forward and towards the left.
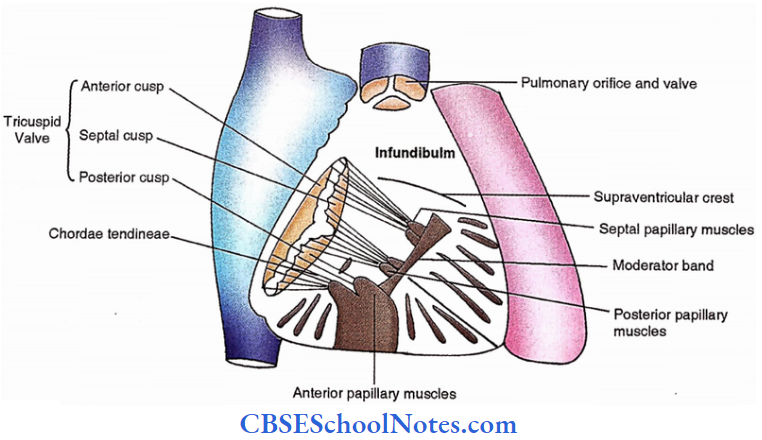
- A fibrous ring (annulus) along its margin provides attachment to the tricuspid valve whose three cusps are named anterior (largest), septal (smallest) and posterior.
- The junction of three cusps (commissures) are named after the cusps, i.e., anteroseptal, posteroseptal and anteroposterior.
Dissection Steps For Chambers Of The Heart
Make a T-shaped incision in the right ventricle in such a way that the vertical limb passes through the ventricular wall and the horizontal limb below the infundibulum. Open the cavity of the right ventricle study its interior and note the thickness of its wall.
- Note the shape of the cavity and bulging of the interventricular septum to the right. Note the right atrioventricular opening, smooth and rough parts of the cavity, chordae tendineae and cusps of the tricuspid valve. Identify the septomarginal (moderator) band
- Make an inverted T-shaped incision in the left ventricle in such a way the vertical limb passes through the ventricular wall and the horizontal limb through the inferior border up to the apex and opens the cavity.
- Study the interior note the thickness of its wall and compare it with the right ventricle. Note the rough and smooth parts, mitral opening and its cusps. Note the membranous and muscular parts of the interventricular septum.
- To open the left atrium 2 horizontal incisions are given through the pulmonary veins. Open the chamber and study its interior.
- Note openings of 4 pulmonary veins, smooth and rough parts, and left atrioventricular orifice from the atrial aspect. Locate the positions of the sinoatrial node, atrioventricular node and a bundle of His.
A cusp consists of a fibrous core covered by endothelium. The cusps are not uniform in thickness. Its central part is thinnest (clear zone) while the attached part (basal zone) and marginal part (rough zone) are relatively thicker.
All the cusps receive the attachment of fibrous thread-like structures (chordae tendinae) from the ventricular wall, along their margins and on their ventricular surfaces.

Rough part
It is the lower part of the right ventricle marked by a large number of elevations called the trabeculae camera. These elevations are of three types;
- Ridges – elongated elevations attached to the wall all along its length,
- – elongated elevation attached at its ends only (For Example., septomarginal/moderator band),
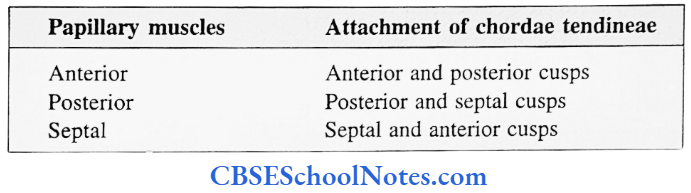
- Papillary muscles – conical elevations. Papillary muscles provide chordae tendineae to the cusps. Papillary muscles are arranged in three groups named, anterior, posterior and septal according to their relation with the ventricular walls.
Chordae tendineae from each group extend towards the commissure and get attached to the adjacent cusps.

Smooth Part
It is the upper part of the right ventricle devoid of the trabeculae camera. This is tunnel-shaped and therefore called the infundibulum or conus arteriosus.
The demarcation between the rough and smooth parts is the supraventricular crest (posteriorly) and the septomarginal band (anteriorly). The latter (also called the moderator band) extends from the interventricular septum to the anterior papillary muscle.
Pulmonary Orifice
It is located at the upper extreme of the right ventricle. A fibrous ring (annulus) along its margin provides attachment to the pulmonary valve.
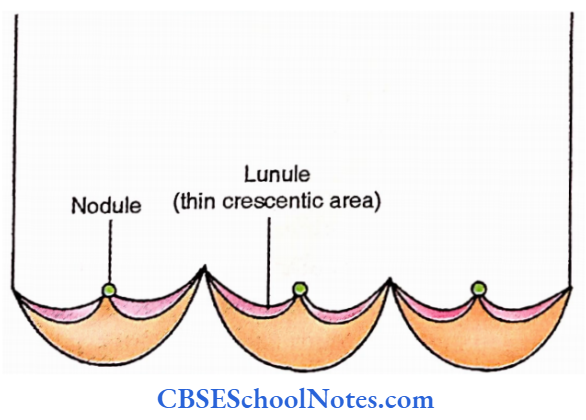
This valve consists of three cusps named according to their attachments, i.e., right anterior, left anterior and posterior. The centre of the cusp margin is marked by a fibrous nodule with thin crescentic areas lateral to it called lunules.
The Left Ventricle
External Features
The left ventricle contributes to a l/3rd of the sternocostal surface, 2/3rd of the diaphragmatic surface, the left border and the apex of the heart. Its wall is three times thicker than that of the right ventricle – a fact correlated with the blood pressure inside its chambers.
Internal Features
This is also described under similar 4 headings as follows,
- Inflow orifice (left atrioventricular orifice)
- Inflow tract (rough part)
- Outflow tract (smooth part)
- Outflow orifice (aortic orifice)
Left Atrioventricular Orifice.
It connects the left atrium with the left ventricle and directs the blood to flow forward and towards the apex of the heart. Its margin is marked by a fibrous ring (annulus) which receives attachment from a bicuspid (mitral) valve.
As the name suggests, the valve consists of two cusps, anterior (larger) and posterior (smaller). Truly speaking, the former is anteromedial and the posterior is posterolateral in position. Their two commissures therefore are anterolateral and posteromedial.
The posterior cusp is typical in the sense that it shows all three zones (rough, clear and basal) in its wall and receives attachment of chordae tendineae along its margin as well as on the ventricular surface.
The anterior cusp is atypical as its wall shows only two zones (rough and clear) and it receives attachment of chordae tendineae along its margin only.
Rough Part
It is the lower part of the left ventricle marked by the trabeculae camera, but here only two types of elevations are noticed, i.e., ridges and papillary muscles (bridges are lacking).
- Papillary muscles are grouped into anterior and posterior which provide chordae tendineae to the adjacent cusps of the bicuspid valves.
- Chordae tendineae from the anterior group extend towards the anterolateral commissure while those from the posterior group proceed to the posteromedial commissure.
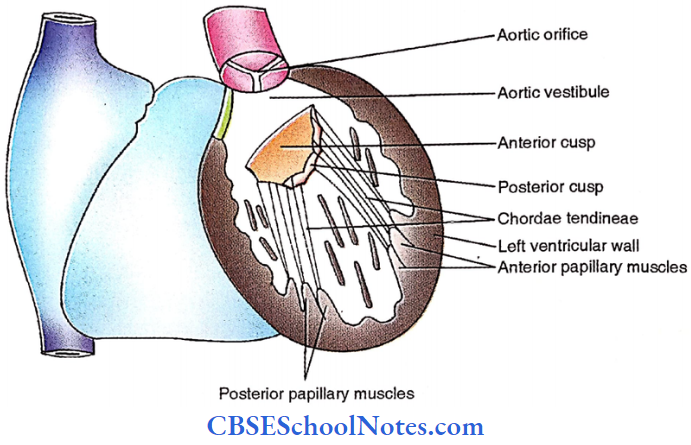
Smooth Part
It is the upper part of the left ventricle devoid of trabeculae camera. This is also called the aortic vestibule. It is located between its anterosuperior wall, the anterior cusp of the bicuspid valve and the membranous part of the interventricular septum.
Aortic Orifice
It connects the aortic vestibule with the ascending aorta. Attached to the fibrous ring (annulus) is an aortic valve which consists of three semilunar valvules or cusps.
Three cusps are named according to their orientation i.e., anterior, right posterior and left posterior. Nodule and lunule are similarly appreciated as in the pulmonary cusps.
Applied Anatomy Of The Chambers Of The Heart
- Atrial septal defect. Normally the foramen ovale (an opening in the interatrial septum during intrauterine life) closes after birth. A minor defect is compatible with life but a large opening needs surgical intervention.
- Ventricular septal defect. The defect is usually noticed in the region of the membranous part of the interventricular septum.
- A large defect will push a lot of blood from left to right resulting in right ventricular enlargement. The defect is corrected surgically.
- Pulmonary valve stenosis. Narrowing of the pulmonary orifice restricts the blood flow from the right ventricle to the pulmonary trunk. Increased load on the right ventricle results in its hypertrophy.
- Pulmonary valve incompetence. It results in pulmonary regurgitation and during diastole, a murmur (an abnormal sound) can be heard.
- Mitral valve stenosis and regurgitation. The mitral valve is a common site of valvular disease. It may be narrowed (stenosis) or unable to close during systole (regurgitation).
- Both conditions produce murmur, the former during diastole (diastolic murmur) and the latter during systole (systolic murmur).
- Aortic valve incompetence is usually congenital and results in a systolic murmur and left ventricular hypertrophy.
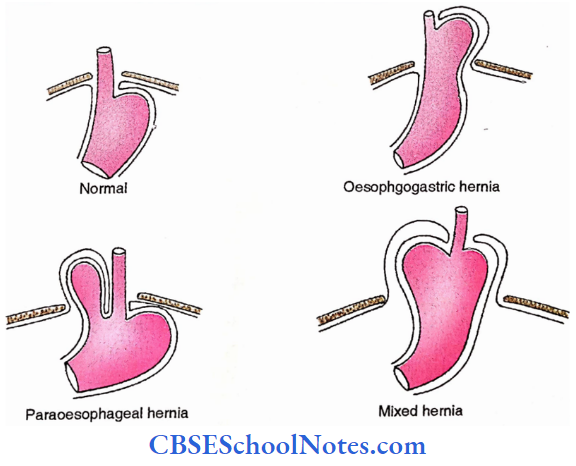
- Enlarged left atrium. Since the oesophagus forms the immediate posterior relation of the left atrium, a compression effect is observed in the ‘barium-swallow-radiograph’ in case of left atrium enlargement.
Structures Of The Walls Of The Heart
Fibrous Skeleton Of The Heart
Functions
- Ensures electrophysiological discontinuity between atrial and ventricular musculature.
- Provides attachments for the myocardium.
- Maintains the cardiac position.
- Forms base for the attachment of valves.
Components
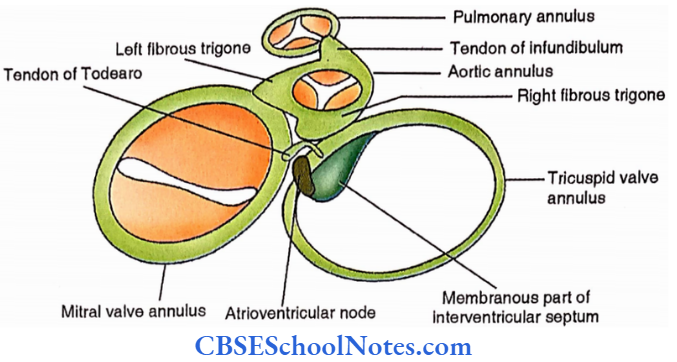
- Fourfibrous rings
- Tricuspid valve annulus.
- Mitral valve annulus.
- Pulmonary valve annulus.
- Aortic valve annulus.
- Two fibrous trigones. These are thickenings in the aortic annulus.
- Rightfibrous trigone. It is the central fibrous body and forms a structural and functional
link between aortic, mitral and tricuspid orifices. - Leftfibrous trigone. It connects the aortic annulus with the mitral valve annulus.
- Two tendons
- Tendon ofinfundibulum. It is a fibrous connection between the aortic annulus and the pulmonary annulus.
- Tendon of Todaro. It is a curved fibrous band between the mitral valve annulus and the tricuspid valve annulus. It is subendocardial in the right atrial wall and lying in its concavity is the atrioventricular node.
Membranous part of the interventricular septum. It is the posterior part of the interventricular septum close to the junction of the mitral valve annulus and tricuspid valve annulus. Its inferior margin is related to the atrioventricular bundle.
Musculature Of The Heart
Actual and ventricular musculatures are completely separated from each other by a fibrous skeleton. In both cases, muscle fibres form superficial and deep laminae.
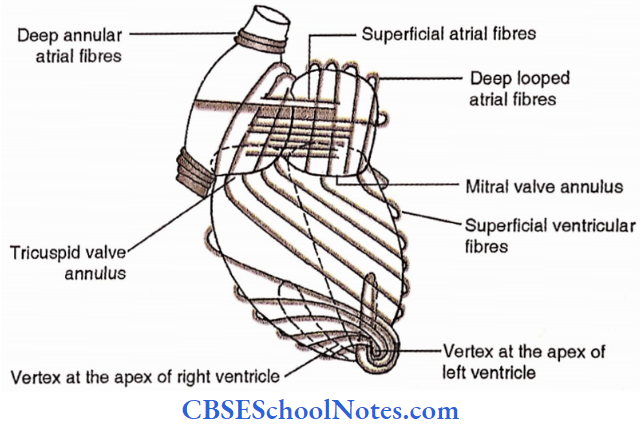
Atrial Musculature
Superficial fibres. These encircle two atria transversely, i.e., across the cardiac long axis.
Deep fibres.
- Looped deep fibres. These arise from the superior margin of the tricuspid and mitral valve annulus and after making a loop, get attached to the inferior margin of the corresponding annulus.
- Annular deepfibres. These are circular fibres adjacent to the termination of venae cavae.
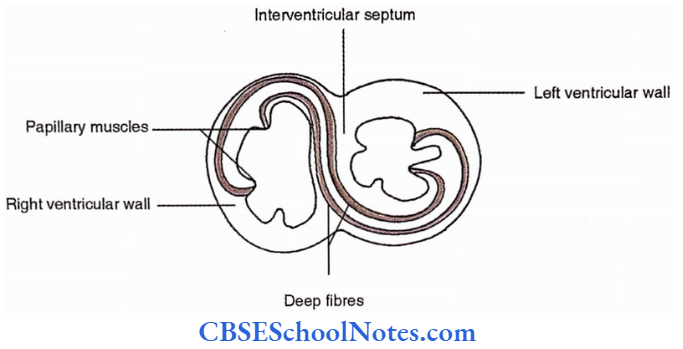
Ventricula Musculature
- Superficial fibres. These fibres arise from the tricuspid as well as mitral valve annulus and run spirally around the heart till they reach the apex of the right and left ventricles.
- These fibres make a whirl (called a vertex) at the corresponding apex and then run very deep to continue with the papillary muscles.
- Deepfibres. These fibres are located in the interventricular septum and connect the papillary muscles of the two ventricles.
Conduction System Of The Heart
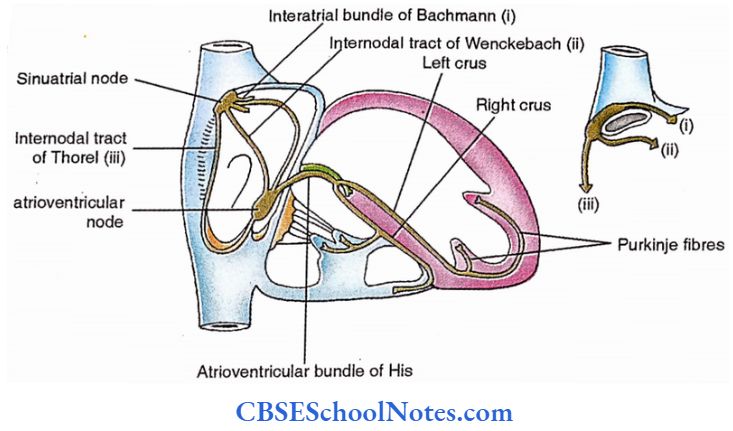
Specialized cardiac muscles organize to form this system to control the rate of heartbeat. Components of this system are as follows.
- Sinuatrial node. This is also called a ‘pacemaker’ because the impulses are initiated here. This is named sinoatrial because originally it is a part of ‘sinus venosus’ which is absorbed later to form part of the right atrium.
- The node is subepicardial in the junctional region between the superior vena cava and the right atrium at the upper end of the sulcus terminalis.
- Atrioventricular node. It is subendocardial and located in the posterior wall of the right atrium just above the opening of the coronary sinus.
- Atrioventricular bundle of His. It runs along the inferior margin of the membranous part of the interventricular septum. It terminates into two crura.
- Right crus. It runs in the interventricular septum, mostly subendocardially, towards the right ventricular chamber.
- The majority of it passes to the anterior papillary muscles and the anterior wall of the right ventricle through the moderator band, and is then distributed via their fine branches called the Purkinje fibres.
- Left crus. It pierces the interventricular septum to reach its left aspect and immediately splits into multiple bands. These are distributed to the left ventricle via their Purkinje fibres.
- Accessory tracts. There are three specialized tracts which connect the SA node with the AV node. These are called the internodal tracts.
- Anterior internodal tract. It is one of the branches of the interatrial bundle of Bachmann arising from the SA node. The tract runs to the left, anterior to the opening of the superior vena cava and descends to join the AV node.
- Middle internodal tract of Wenckebach. It passes along the posterior margin of the opening of the superior vena cava and then descends along the limbus fossa ovalis to join the AV
node. - Posterior internodal tract of Thorel. It descends in the crista terminalis and runs to the left along the attached margin of the valve of the inferior vena cava to enter the AV node.
Applied Anatomy Of The Conducting System Of Heart
- Injury to the AV node and AV bundle. Damage to the conducting system is usually caused by the ischaemia resulting from coronary artery disease.
- Heart block is caused by damage to the AV node or AV bundle as the impulses are unable to reach the ventricle from the SA node. A pacemaker implantation is usually useful in such cases.
- Artificial cardiac pacemaker. The instrument is useful in the cardiac block. It has three components; a battery, a wire and an electrode. Battery is inserted subcutaneously whereas electrode is passed in the right ventricle through the venous channel and inserted subendocardially.
- Cardiac massage. It is applying pressure over the lower part of the sternum and then releasing it. The process is repeated at regular intervals and is found to be very useful in reviving the heart in cases of cardiac arrest.
- Abnormal heart rate. A pulse rate above 100 beats/min in adults is said to be ‘SINUS TACHYCARDIA’ and below 60 beats/min is considered to be ‘SINUS BRADYCARDIA’.
- Extrasystole. It is due to ectopic beat arising from foci in the heart which stimulates the heart before the next sinus beat is due. Extra systole therefore comes prematurely and is followed by a pause.
Superior Mediastinum
Superior Mediastinum Boundaries
Anterior – Sternum (monubrium stemi)
Posterior – Upper 4 thoracic vertebral bodies.
Lateral – Mediastinal pleurae
Superior – Inlet of the thorax
Inferior – Horizontal plane at the level of the sternal angle.
Superior Mediastinum Contents
Retrosternal structures
- Sternothyroid.
- Sternohyoid
- Thymus.
- Superior vena cava
- Brachiocephalic vein
- Left superior intercostal vein
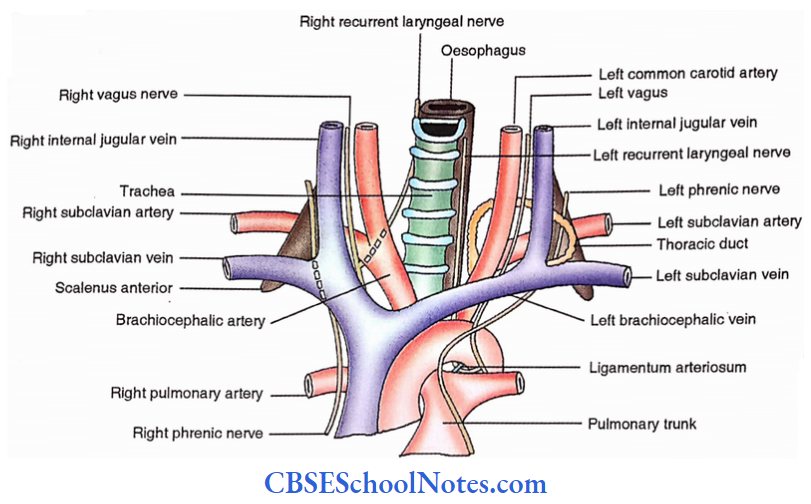
Prevertebral structures
- Longus colli
- Trachea
- Oesophagus
- Left recurrent laryngeal nerve
- Thoracic duct
Intermediate Structures
- Arch of aorta
- 3 branches of the arch of the aorta (brachiocephalic, left common carotid and left subclavian)
Paired nerves and plexuses
- Vagus nerve – right and left
- Phrenic nerve- right and left
- Cervical cardiac branches from the left superior cervical ganglion and left vagus.
- Cardiac plexuses – superficial and deep
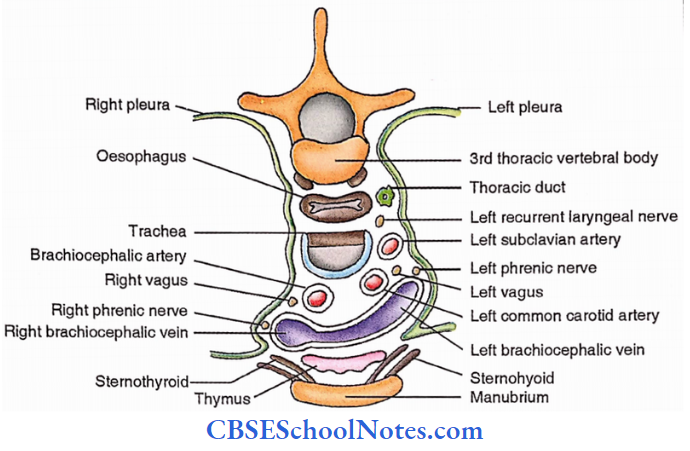
Arch Of Aorta
The Arch of the aorta commences at the level of the sternal angle as a continuation of the ascending aorta. It courses backwards and towards the left to terminate as a descending thoracic aorta at the same level.
Arch Of Aorta Surface Marking
The Arch of the aorta is related to the posterior surface of the lower half of the manubrium stem. It is marked by joining the right and the left ends of the sternal angle with an upward bold convexity reaching the midpoint of the manubrium.
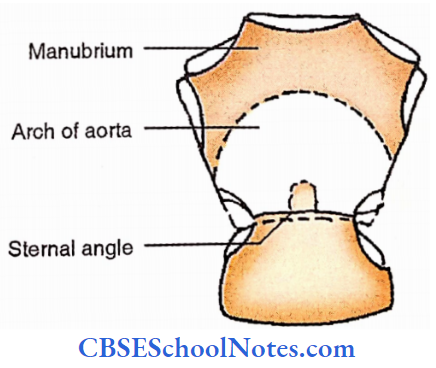
Arch Of Aorta Curvatures
- In vertical plane
- Superior- convex
- Inferior- concave
- In horizontal plane
- Right- concave
- Left- convex
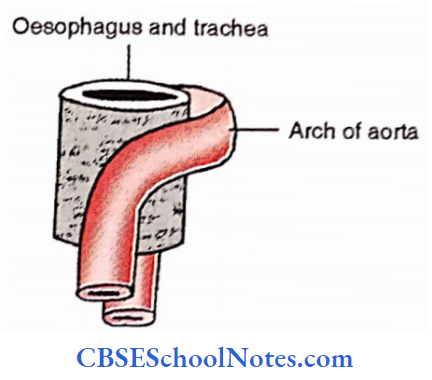
Arch Of Aorta Branches
From proximal to distal these are-
- Brachiocephalic artery
- Left common carotid artery
- Left subclavian artery
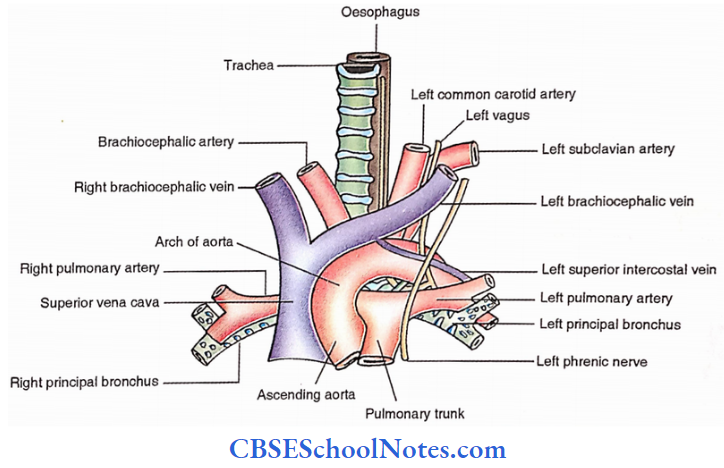
Arch Of Aorta Relations
- Superior
- Three branches of the arch of the aorta
- Left brachiocephalic vein
- Inferior
- Ligamentum arteriosum
- Bifurcation of the pulmonary trunk and left pulmonary artery
- Left principal bronchus
- Left recurrent laryngeal nerve
- Superficial cardiac plexus
- Anterior and to the left
- Left vagus
- Left phrenic
- Two cervical cardiac branches to the superficial cardiac plexus
- Left superior intercostal vein
- Posterior and to the right
- Trachea
- Oesophagus
- Thoracic duct
- Left recurrent laryngeal nerve
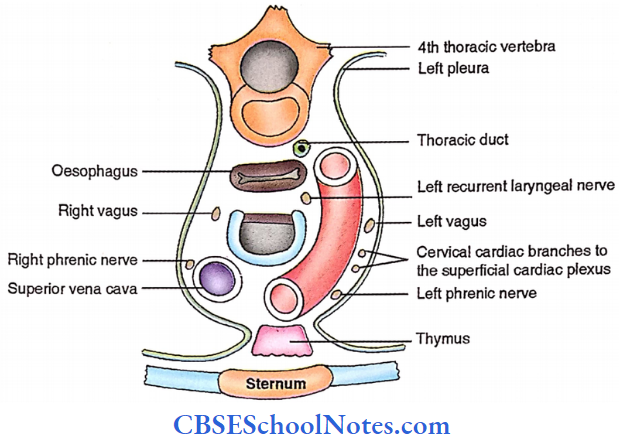
Superior Mediastinum Applied Anatomy
- The left brachiocephalic vein is located in the lower neck of children. This is of great importance in operations like tracheostomy.
- Anomalies of the branches of the arch of the aorta. In about 27% of cases left common carotid artery originates from the brachiocephalic artery.
- In 2.5% of cases, the right common carotid and right subclavian arteries arise independently from the arch.
- The presence of two brachiocephalic arteries and the origin of the vertebral artery from the arch is also often observed.
- Abnormal arterial conditions cause pressure on the trachea and oesophagus.
- Retro-oesophageal right subclavian artery. In such cases, the right subclavian artery is the distalmost branch of the arch of the aorta.
- Double aortic arch. Two aortae arise from a vascular ring around the trachea and oesophagus.
- Aortic aneurysm. It is a localized dilatation of the aorta.
- Coarctation of aorta. It is an abnormal narrowing (stenosis) of the aorta diminishing blood flow to the lower part of the body.
- Patent ductus arteriosus. Ductus arteriosus (communication between the left pulmonary artery and arch of the aorta during intrauterine life) is soon fibrosis to form ligamentum arteriosum.
- If it persists (patent ductus arteriosus), there is mixing of oxygenated and deoxygenated blood. The surgical ligation of the duct corrects the problem.
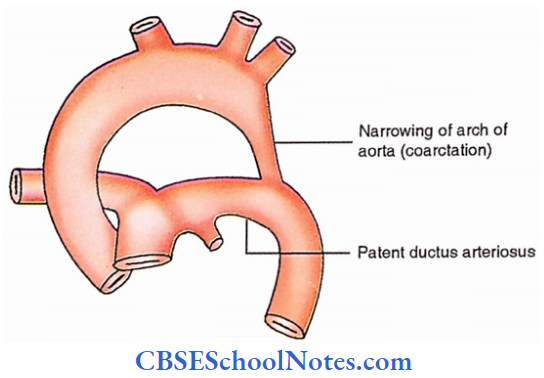
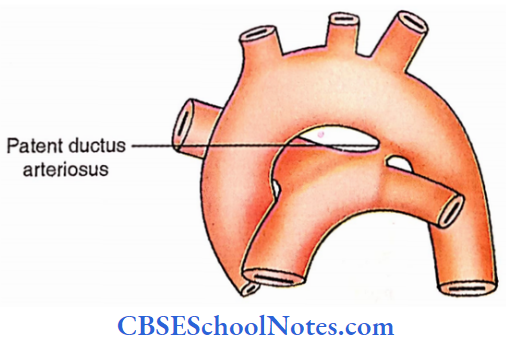
Posterior Mediastinum
Posterior Mediastinum
Posterior Mediastinum Boundaries
- Anterior
- Tracheal bifurcation
- Pulmonary vessels
- Pericardium
- Diaphragm
- Posterior – Lower eight thoracic vertebra
- Sides – Mediastinal pleurae
- Inferior – Diaphragm
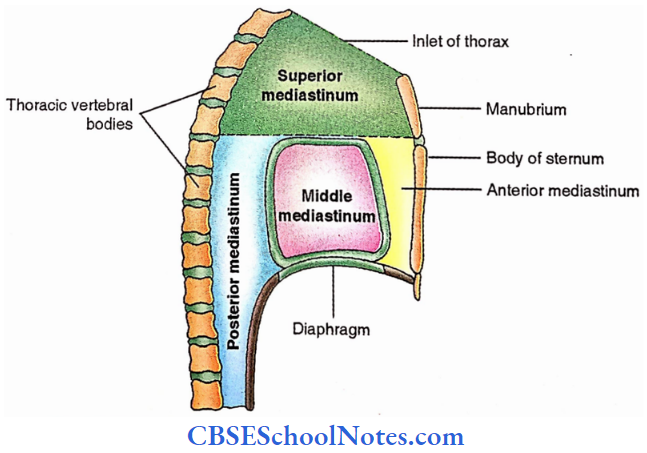
Posterior Mediastinum Contents
- Vertical structures
- Descending thoracic aorta
- Azygos, hemiazygos and accessory hemiazygos veins
- Oesophagus
- Thoracic duct
- Vagus
- Splanchnic nerves (greater, lesser and least)
- Horizontal structures
- Right posterior intercostal arteries
- Posterior intercostal veins
- Terminal parts of hemiazygos and accessory hemiazygos veins
- Right to left course of thoracic duct
Posterior mediastinal lymph nodes
Inter-relationship of the contents
In general, horizontal structures pass behind the vertical structures.
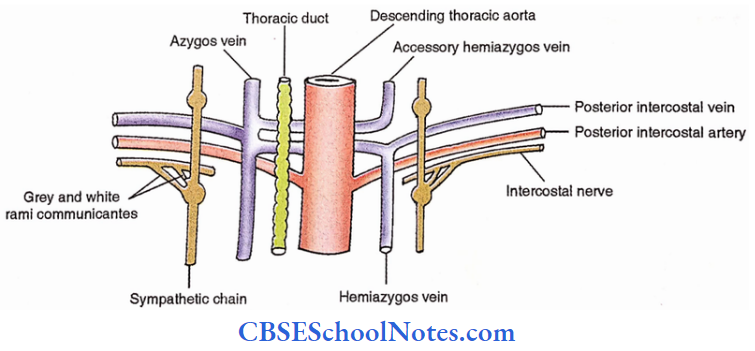
Descending Thoracic Aorta
It is a continuation of the arch of the aorta at the level of the intervertebral disc between the 4th and 5th thoracic vertebrae. It descends to the left of the midline in the upper part while in the midline in the lower part.
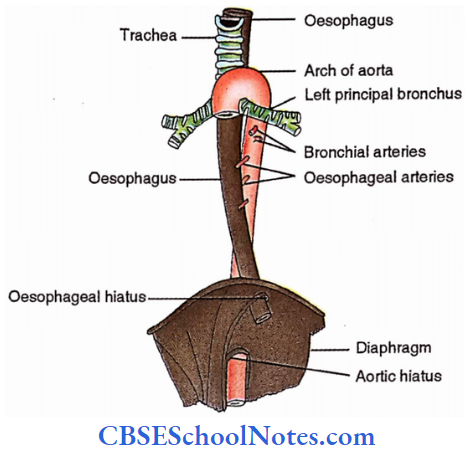
Posterior mediastinal lymph nodes Relations
- Posterior
- Terminal part of hemiazygos vein
- Accessory hemiazygos vein
- Posterior and to the right
- Posterior and to the left
- Hemiazygos vein
- Accessory hemiazygos vein
- Sides
- Anterior
- Root of the left lung
- Pericardium
- Oesophagus
- Diaphragm
Posterior mediastinal lymph nodes Branches
- One right and two left bronchial arteries.
- Pericardiophrenic branches
- Lower 9 pairs of posterior intercostal arteries
- Superior phrenic arteries
- Three oesophageal arteries
- Mediastinal arteries
- Subcostal arteries
Dissection Steps For The Posterior Mediastinum
Define the boundaries of the posterior mediastinum. Identify and divide the ligmentum arteriosum. Trace the left recurrent laryngeal nerve branches to the deep cardiac plexus located in front of the tracheal bifurcation.
- Clean and identify the descending thoracic aorta and note its branches. trace the upper part of the thoracic duct to its termination at the left Jugulosubclvian junction. Trace the posterior Intercostal veins to the azygos, hemiazygos and accessory hemiazygos veins.
- Clean and identify the sympathetic chain about the heads of the ribs and note the different splanchnic nerves. Note the various structures at the level of T4.
Oesophagus
It begins at the level of the 6th cervical vertebra as a continuation of the pharynx in the midline. It descends to the left of the midline but comes to lie in the midline at the level of the 5th thoracic vertebra.
Reaching the level of the 7th thoracic vertebra it gradually turns to the left till it reaches the level of the 10th thoracic vertebra where it pierces the diaphragm. It terminates by joining the stomach at the level of the 11th thoracic vertebra.
The oesophagus is approximately 25 cm in length. It is divided into three parts according to its location, i.e., cervical, thoracic and abdominal. Normally four constrictions are noted in the oesophagus.
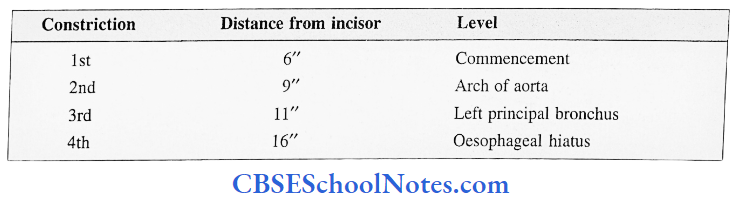
Vascular supply is tabulated below.
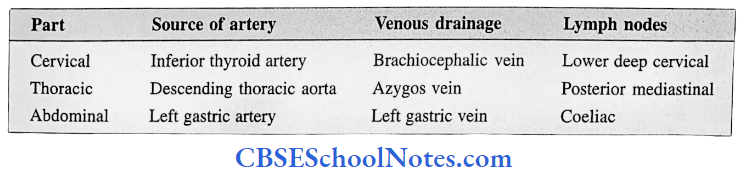
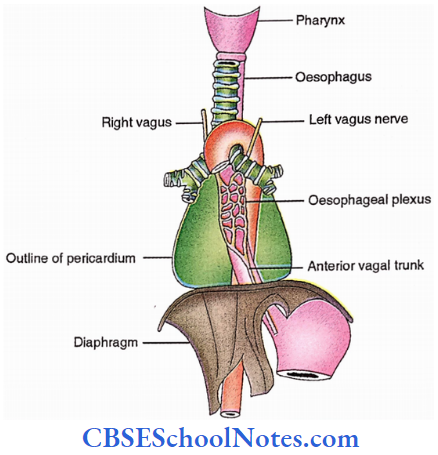
Innervation
The oesophagus receives autonomic innervation as tabulated below.
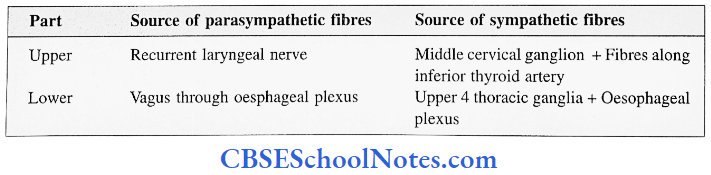
Oesophagus Applied Anatomy
- Dyspepsia – difficulty in swallowing. It is a serious symptom usually due to benign or malignant tumours of the oesophagus.
- Oesophageal injury – though rare, but very important because of its fatal outcome. Injury to the oesophagus is usually accompanied by injury to the trachea due to its immediate anterior relation.
- Tracheo-oesophageal fistula – This is the most common congenital anomaly of the oesophagus. Associated oesophageal atresia is a usual combination. In the majority of anomalies, the trachea communicates with the distal part of the oesophagus.
- Oesophageal cancer – It reduces the lumen of the oesophagus. The patient develops dysphagia when the lumen is reduced by 30 to 50%. Involvement of recurrent laryngeal nerve causes hoarseness of voice.
Azygos System Of Veins
Azygos vein
It commences in the abdomen by the union of right ascending lumbar and right subcostal veins. It enters the thorax by passing through the aortic hiatus to the right of the thoracic duct. Its tributaries are:
- 2nd to 11th right posterior intercostal veins
- Hemiazygos and accessory hemiazygos veins.
- Veins from the thoracic viscera.
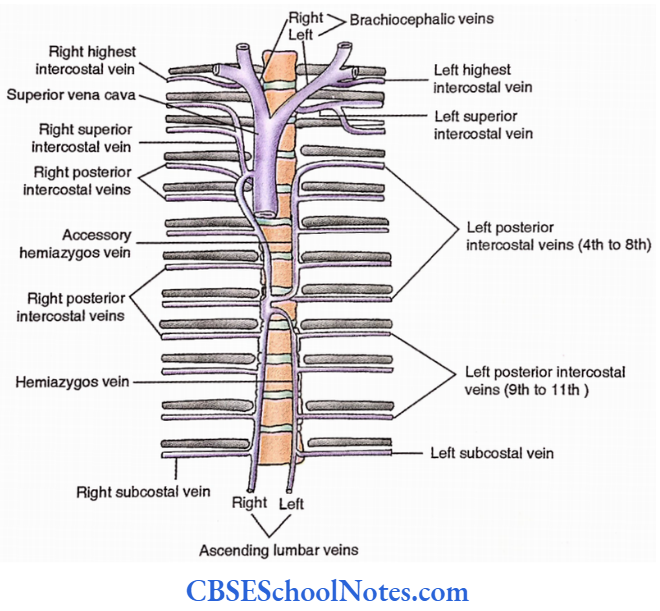
Accessory Hemiazygos Vein
It is a vertical vein in the upper part of the thorax on the left side of the vertebral column. It receives left 4th to 8th posterior intercostal veins.
It descends from the level of the 4th left intercostal space to the 8th thoracic vertebral body where it crosses to the right to join the azygos vein.
Hemiazygos vein
Its commencement is like azygos vein i.e., left subcostal and left ascending lumbar veins unite to form it. It enters the abdomen by piercing the left crus of the diaphragm.
It ascends to the left of the vertebral column till it reaches the 8th thoracic vertebral body where it turns to the right to join the azygos vein. During its course, it receives 9th to 11th left posterior intercostal veins.
Thoracic Duct
This is the largest lymphatic channel in the body which drains almost the whole body except the right upper limb and right half of the head neck and thorax.
- It ascends from the upper part of the cistema chyli (a lymphatic sac lying vertically in the abdomen against the upper two lumbar vertebrae) and enters the thorax through the aortic hiatus.
- It ascends to the right of the midline till it reaches the level of the sternal ‘ angle.
- During this part of the course, it lies anterior to the lower thoracic vertebral bodies, posterior to the oesophagus, to the right of the descending thoracic aorta and to the left of the azygos vein.
- At the sternal angle, it turns to the left and then ascends to the left of the midline to reach the root of the neck.
- At the level of the 7th cervical vertebra, it again turns to the left to drain into venous blood at the junction of the left internal jugular and left subclavian veins.
- The thoracic duct measures approximately 18″ (45 cm). It is beaded in appearance due to the presence of multiple valves in it.
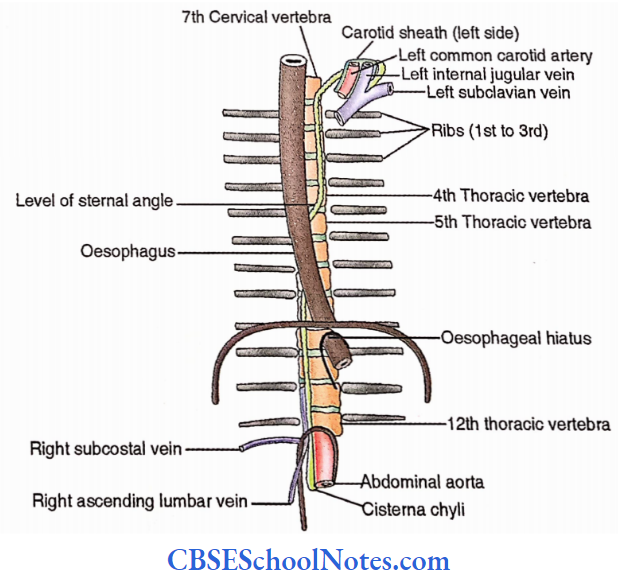
Accessory Hemiazygos Vein Applied Anatomy
- Laceration of thoracic duct – The thoracic duct is colourless, therefore it is difficult to visualize it during surgical procedures and therefore prone to injury during operation in the posterior mediastinum.
- Lymph (chyle) may enter the pleural cavity, this condition is called chylothorax.
- Variation of the thoracic duct. There are two lymphatic vessels during intrauterine life running parallel to each other and draining symmetrically in the root of the neck.
- Since the thoracic duct is the persistence of part of both these channels, anomalous thoracic duct (For Example., double thoracic duct) may be noticed in adults.