
Introduction To Abdomen
Abdomen Definition
Part of the trunk below the diaphragm
Abdomen Importance
Abdomen is important to,
- Physicians
- Gynaecologists and obstetricians
- Surgeons
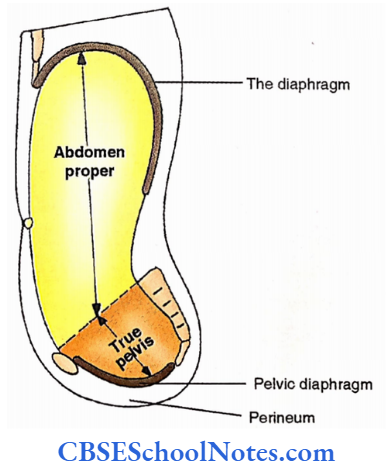
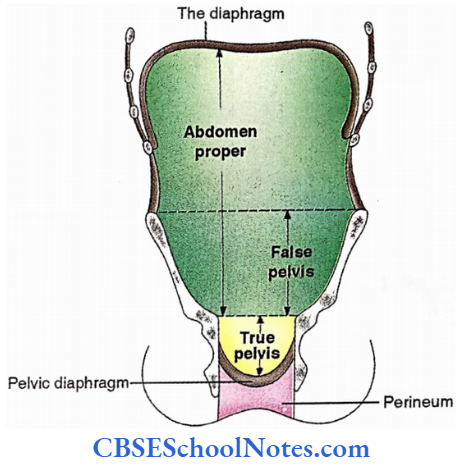
Abdomen Subdivisions
- Abdomen proper – Upper (Above the iliac crest) Lower (False pelvis)
- Pelvis – True pelvis (Between pelvic inlet and pelvic diaphragm) and Perineum (Below pelvic diaphragm)
Abdomen Bones
- Lower ribs and costal cartilage
- Lumbar vertebrae
- Sacrum and coccyx
- Hip bones
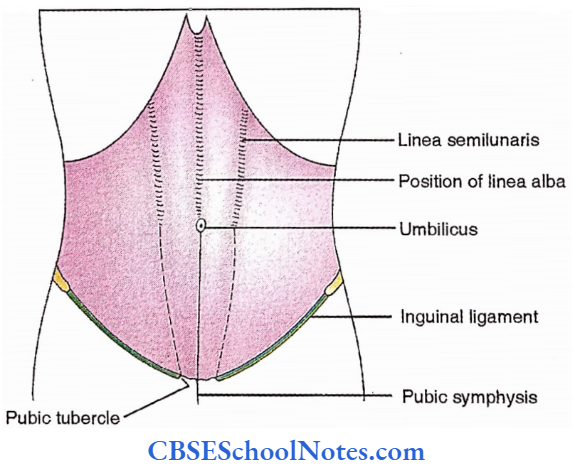
Abdomen Landmarks
- Infrastemal/subcostal angle (Anteriorly, between constal margins of two sides).
- Umbilicus,
- Costal margin
- Iliac crest (Superior border of ilium).
- Tubercle of iliac crest (Along outer lip, 5 cm from anterior superior iliac spine).
- Anterior superior iliac spine (Anterior extremity of the iliac crest).
- Inguinal ligament (Between anterior superior iliac spine and pubic tubercle).
- Pubic tubercle (Lateral end of pubic crest).
- Pubic crest (Superior border of the body of pubis).
- Pubic symphysis (In the midline, between the bodies of the pubis).
- Position of the linea alba (Midline groove between the xiphoid process and pubic symphysis).
- Linea semilunaris (Curved groove between the tip of 9th costal cartilage and pubic tubercle).
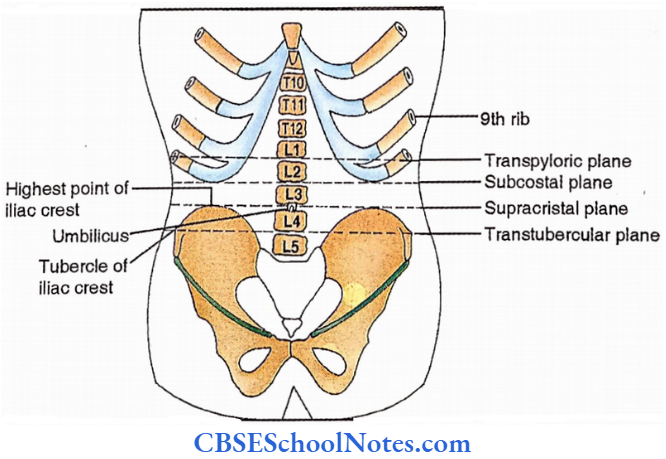
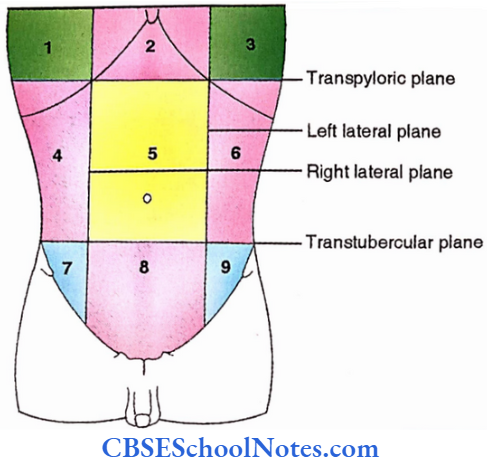
Divisions Of Abdomen Into Nine Regions
Two vertical (right and left lateral) and two horizontal (transpyloric and transtubercular) planes divide the abdomen into 9 regions.
A lateral plane passes through the mid-inguinal point (a point on the inguinal ligament between the anterior superior iliac plane and public symphysis).
The transpyloric plane is horizontal midway between the suprasternal notch and public symphysis. The transtunercular plane is a horizontal plane through tubercles of the iliac crest of two sides.
Regions from above downwards.
- 3 unpaired – Epigastric, Umbilical, Hypochondriac/public
- 3 Paired – Hypochondriac, Lateral/Lumbar, Inguinal /Iliac
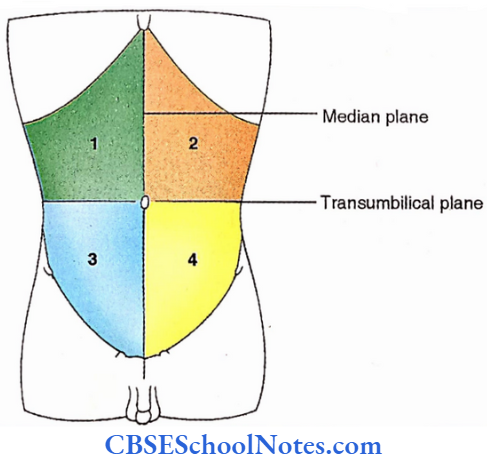
Divisions of the abdomen into four quadrants: by median and supracristal planes. The supracristal plane is a horizontal plane passing through the highest point of the iliac crest of two sides. 4 quadrants with important viscera are as follows;
- Upper right quadrant – Liver and gall bladder
- Upper left quadrant – Stomach and spleen
- Lower right quadrant – Caecum, appendix and ascending colon
- Lower left quadrant – Descending colon and sigmoid colon
Extent Of The Abdomen Proper
- Apparent
- Superior – Costal margin
- Inferior – Anterior – Inguinal ligament
- Lateral and posterior -Iliac crest
- Actual
- Superior – Diaphragm
- Inferior – Pelvic inlet
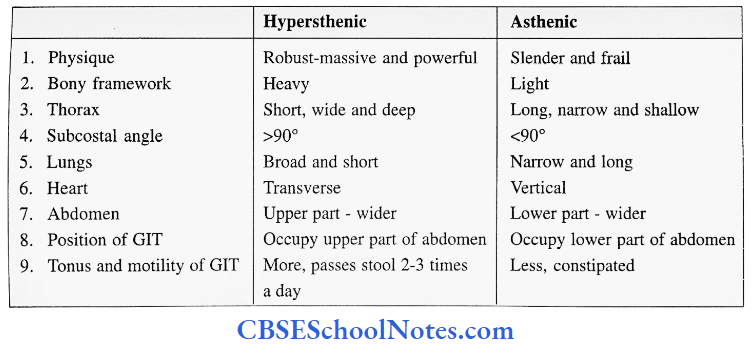
Bodily habitus (4 types)
- Hypersthenic – 5%
- Sthenic – 48%
- Hypersthenic – 35%
- Asthenic – 12%
Anterior Abdominal Wall Superficial Structures
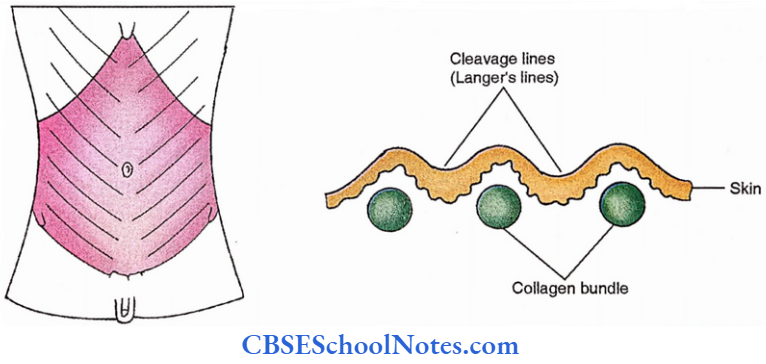
Langer’s Lines
These are produced by the directions of bundles of collagen fibres in the dermis.
- Horizontal in nature.
- An incision along these lines heal with hair-line scars (Important from a cosmetic point of view)
Cutaneous Nerves
- Anterior cutaneous branches of,
- T7-11 intercostal nerves
- Subcostal nerve (T12)
- Iliohypogastric nerve (L1)
- Lateral cutaneous branches of T10 and 11 intercostal nerves
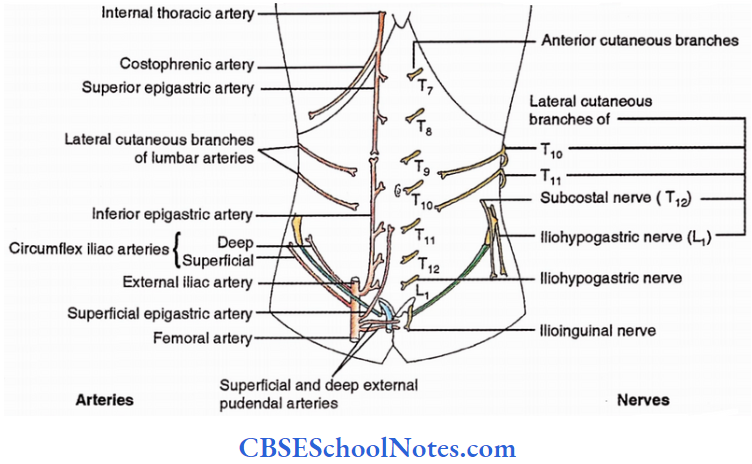
Cutaneous Arteries
- Accompanying cutaneous nerves,
- Anterior cutaneous arteries from superior and inferior epigastric arteries
- Lateral cutaneous branches of lumbar arteries
- Branches of the femoral artery (A little below the inguinal ligament),
- Superficial circumflexiliac artery. (Runs laterally towards the anterior superior iliac spine).
- Superficial epigastric artery (Runs upwards towards the anterior abdominal wall).
- External pudendal arteries (Superficial and Deep). These run medially in relation (superficial and deep) to the spermatic cord in males.
- Branches of external iliac artery (A little above the inguinal ligament).
- Deep circumflex iliac artery. (Runs towards the anterior superior iliac spine).
- Inferior epigastric artery (Ascends in the anterior abdominal wall).
Superficial Veins
- Radiating veins around the umbilicus
- Below the level of the umbilicus – superficial veins drain into a great saphenous vein
- Above the level of the umbilicus – superficial veins drain into a lateral thoracic vein
- Thoracoepigastric vein -It connects the lateral thoracic vein with a superficial vein of the lower abdomen.
- Para umbilical veins – These are located around the round ligament of the liver (ligamentum teres) and connect radiating veins around the umbilicus with the portal vein
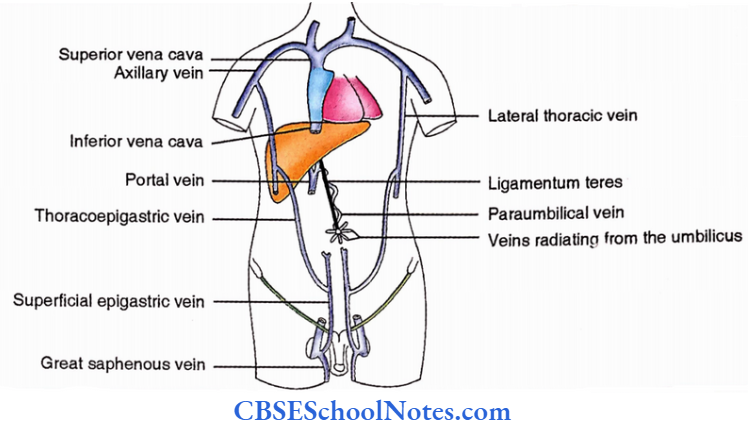
Superficial Veins Applied
- Portal obstruction – Caput medusae (Dilated radiating veins around the umbilicus)
- Obstruction of superior vena cava – Downward flow of blood in superficial veins
- Obstruction of inferior vena cava- Upward flow of blood in superficial veins
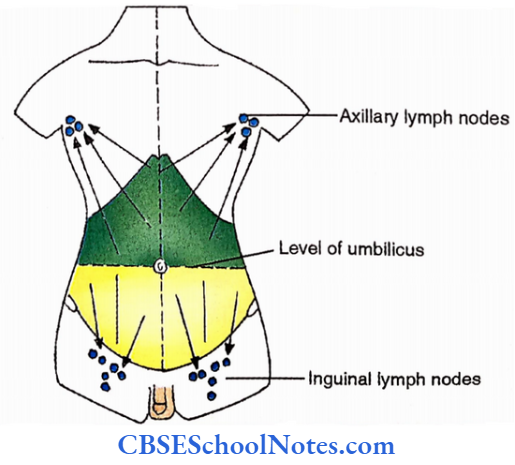
Superficial Lymphatics
- Above the umbilicus – Superficial lymphatics drain into axillary lymph nodes (Anterior and Posterior groups)
- Below the umbilicus – Superficial lymphatics drain into superficial inguinal lymph nodes (Medial and Lateral groups of horizontal chain)
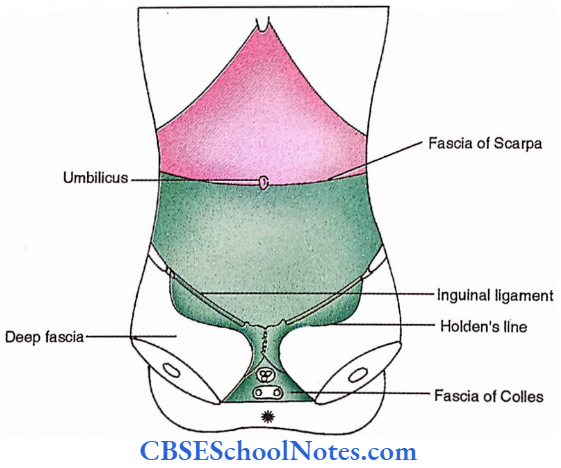
Superficial Fascia
1. Superficial Fascia Character
- Above the level of umbilicus – It is fatty connective tissue
- Below the level of the umbilicus
- Its superficial layer is fatty (Fascia of Camper)
- Its deep layer is membranous (Fascia of Scarpa)
2. Superficial Fascia Extent offascia of Scarpa,
Above – Umbilicus
Lateral – Midaxillary line
Below (Step ladder descent). It gets attached to,
- Iliac crest
- Holden’s line (1 cm below and parallel to the inguinal ligament)
- Body of pubis
- Ischiopubic ramus
- Posterior margin of perineal membrane
Midline – Fuses with linea alba and pubic symphysis
3. Continuity membranous layer beyond the anterior abdominal wall
- Into thigh (to Holden’s line)
- Into perineum – Here it is named Colles’ fascia
- Over penis – Fascia penis
- Into scrotum – Dartos muscle
4. Contributes to the fundiform ligament, an elastic sling holding shaft of the pen is
Superficial Fascia Applied
Urethral rupture leads to typical swelling in the lower abdomen and perineal region

Anterolateral Abdominal Muscles
Anterolateral Abdominal Muscles Classification
- 4 Large muscles
- 3 Flat muscles
- External oblique (EO)
- Internal oblique (10)
- Transversus abdominis (TA)
- 1 Strap-like muscle – Rectus abdominis (RA)
- 3 Flat muscles
- 2 Small muscles
- Cremaster
- Pyramidalis
Attachments Of Three Flat Muscles Origin
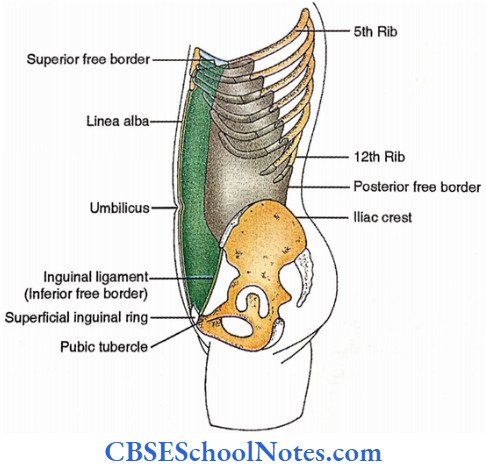
EO – Lower 8 ribs
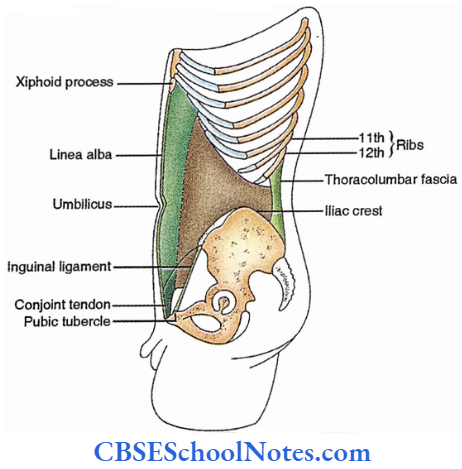
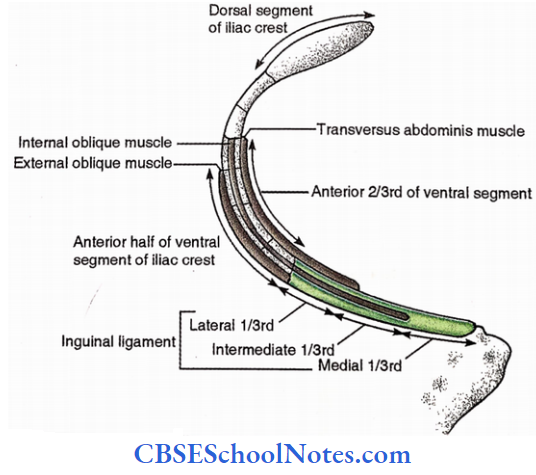
IO – Inguinal ligament (Lateral 2/3rd)
- Iliac crest (Anterior 2/3rd of ventral segment)
- Thoracolumbar fascia
TA – Inguinal ligament (Lateral l/3rd)
- Iliac crest (Anterior 2/3rd of ventral segment)
- Thoracolumbar fascia
- Lower 6 costal cartilages
Insertion
EO – Muscular – Iliac crest – (anterior 1/2 of ventral segment)
Aponeurotic – Its muscle is replaced by aponeurosis along the lateral border of the rectus abdominis and a line between the umbilicus and anterior superior iliac spine. The pneumatic free border between the anterior superior iliac spine and pubic tubercle forms the inguinal ligament. Aponeurosis extends medially to contribute to rectus sheath and linea alba
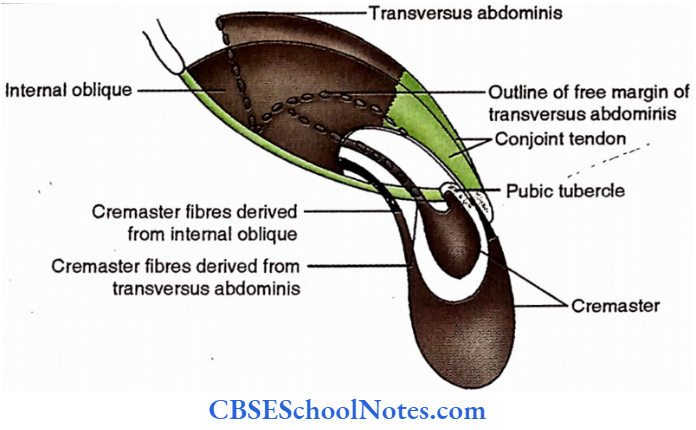
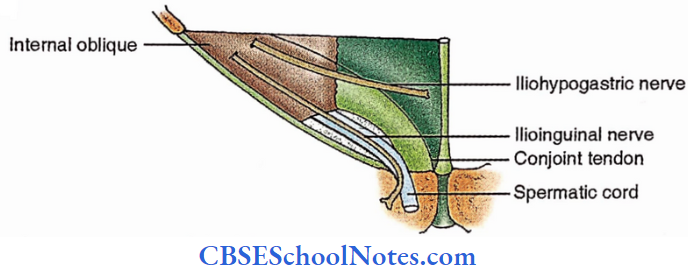
IO and TA – These are replaced by aponeuroses before reaching the lateral border of the rectus abdominous. Their aponeuroses derived from inguinal fibres combine to form a conjoint tendon (falx inguinalis) which gets attached to the pubic crest, aponeuroses from the rest of the muscles contribute to the walls of the rectus sheath and linea alba.

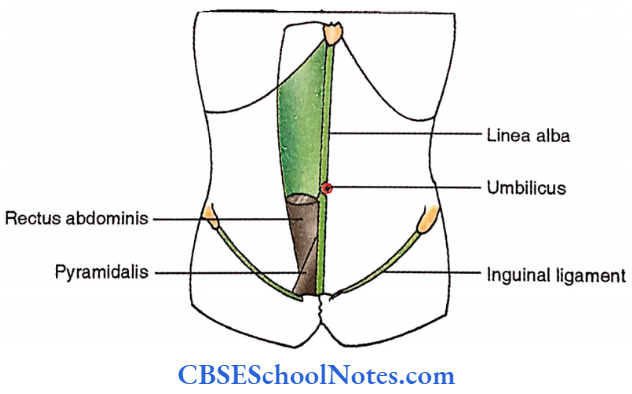
Attachments Of Rectus Abdominis
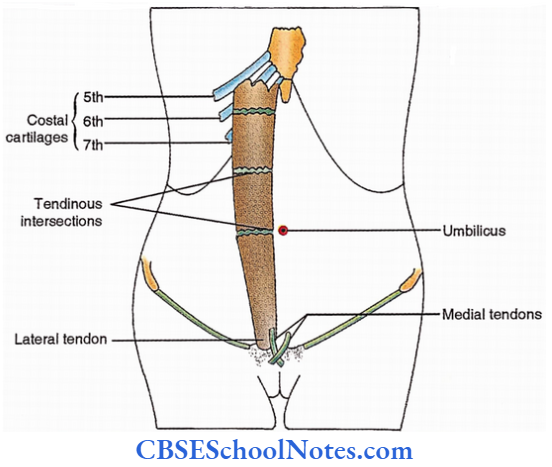
Rectus Abdominis Origin
- Medial tendon – Pubic symphysis
- Lateral tendon – Pubic crest
Rectus Abdominis Insertion
- 5th, 6th and 7th Costal cartilages.
- 3 Tendinous intersections are noticed at the level of xiphoid, umbilicus and in between respectively.
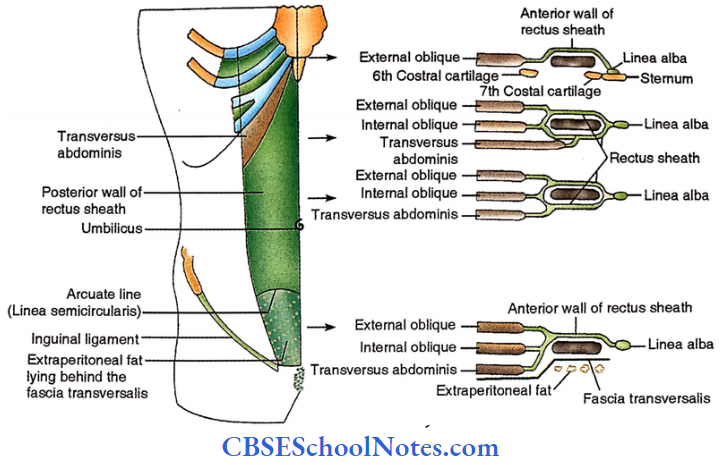
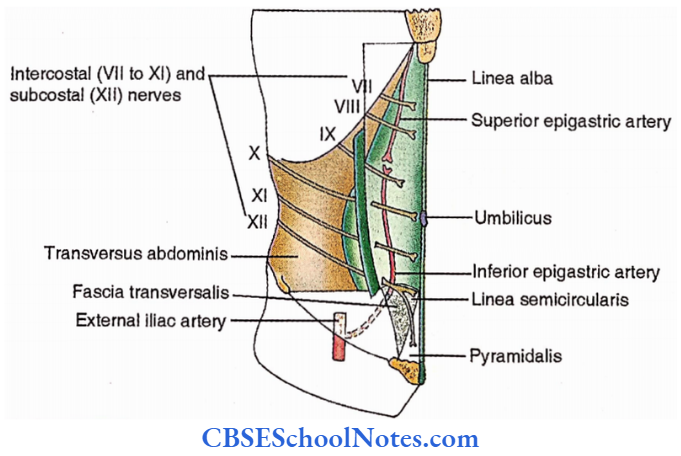
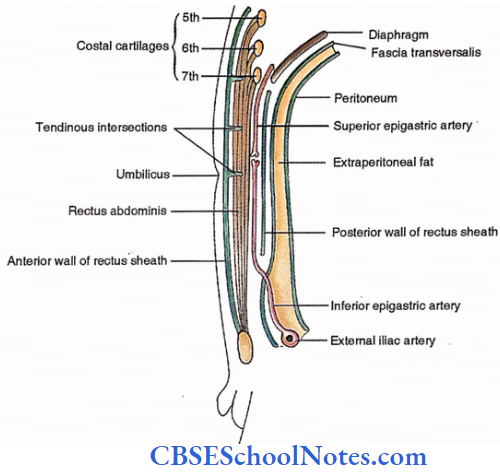
Formation Of Rectus Sheath And Linea Alba
Linea alba – Fibrous band from xiphoid to pubic symphysis
Rectus sheath
- Above costal margin – Only anterior wall (Contributed by the aponeurosis of EO only)
- Below the costal margin
- Upper 3/4th
- The anterior wall is contributed by the aponeurosis of EO and an anterior layer of the aponeurosis of I0.
- The posterior wall is contributed by the aponeurosis of TA and a posterior layer of the aponeurosis of I0.
- Lower l/4th-It has only the anterior wall contributed by the aponeurosis of all three muscles i.e., EO, IO and TA.
- Upper 3/4th
The lower free margin of the posterior wall is called the arcuate line (Linea semicircularis).
Pyramidalis
From pubic crest to lower l/4th of linea alba
Cremaster
Loops of muscle fasciculi along the spermatic cord derived from IO and TA.
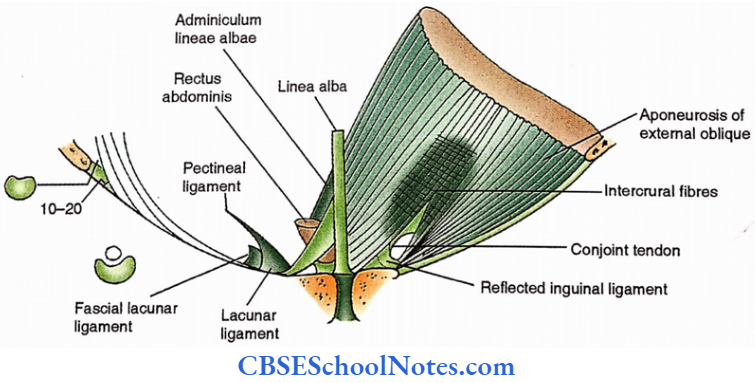
Special features of the aponeurosis of EO
- Inferior margin – Poupart’s ligament ( Inguinal ligament)
- 12 – 14 cm in length
- Between the pubic tubercle and anterior superior iliac spine.
- Lateral part – more oblique, rounded
- Medial part – less oblique, concave upward
- Lacunar ligament of Gimbemat – a triangular posterior extension of the medial end of the inguinal ligament.
- Pectineal ligament of Astley Cooper – a lateral extension of the posterior margin of the lacunar ligament over the pecten pubis.
- Reflected part of an inguinal ligament – an upward and medial extension of the medial end of the inguinal ligament behind the aponeurosis of EO and anterior to conjoint tendon.
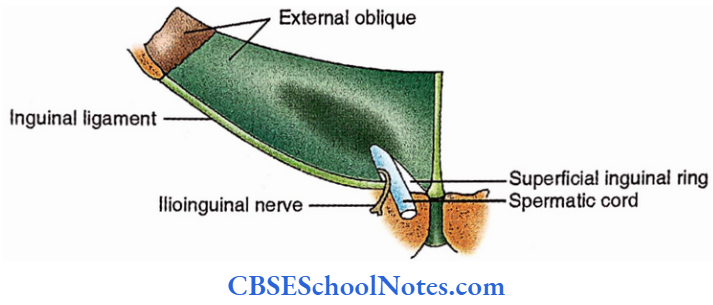
- Superficial inguinal ring
- Triangular, having – a base (Pubic crest), lateral crus and a medial crus.
- Intercrural fibres run across the aponeurotic fibres near the apex.
- Passage for – Spermatic cord in male. (Round ligament of the uterus in the female.)
- Ilioinguinal nerve.

Nerves
EO and RA – T7 -12
IO and TA – T7 -12, Iliohypogastric nerve (LI)
Pyramidalis – Subcostal nerve (T12)
Cremaster – L2 (Gnital branch of genitofermoral nerve)
Functions
EO, IO, TA
- Compression of abdominal contents
- Forced expiration
- Coughing
- Sneezing
- Vomiting
- Defecation
- Micturition
- Parturition (childbirth)
- Helps in pushing and weight lifting
- Supports the abdominal contents
- Rotation of trunk for example. contraction of ipsilateral 10 and contralateral EO produces ipsilateral rotation
RA
- Flexion of vertebral column
- Protection from blow
Pyramidalis – Tensor of linea alba
Cremaster
- Elevatoin of testis for,
- Protection
- Cremasteric reflex
- Helps in thermoregulation of testis
Special features of the aponeurosis of EO Applied
- Hernia
- Inguinal
- Umbilical
- Surgical Incisions
- Median incision
- Paramedian incision
- Mc Burney’s gridiron incision.
Dissection Steps Of Anterior Abdominal Wall (See volume I of the book for incision numbers)
Place the body in the supine position and give incisions Nos. 3,4,8 and 9. Ensure to encircle the umbilicus while giving incision No. 8. Extend incision No. 9 posteriorly along the iliac crest.
Reflect the skin flaps leaving the superficial fascia on the anterior abdominal wall.
- Make a transverse incision through the superficial fascia from the anterior superior iliac spine to the median plane and separate the membranous layer of the superficial fascia from the external oblique aponeurosis.
- Now divide the superficial fascia vertically in the median plane and along the posterior axillary fold. Identify the muscles of the anterior abdominal wall, superficial inguinal ring and spermatic cord.
- Separate the superficial fascia by blunt dissection. Note the direction of the fibres of the external oblique muscle and define its attachments. Divide the external oblique from the costal margin to the iliac crest and reflect it medially.
- Now, note the direction of the fibres of the internal oblique muscle. Divide the internal oblique from the costal margin to the iliac crest, reflect it medially and separate it from the transversus abdominis lying deep to it.
Rectus Sheath
Rectus Sheath Definition
Fibrous compartment for rectus abdominis
Linea alba: It is a midline fibrous band from xiphoid to pubic symphysis between the rectus sheaths of two sides
Rectus Sheath Formation
Upper 3/4th
- Above the costal margins, it has only anterior walls contributed by the aponeurosis of the external oblique.
- Below the coastal margins that both anterior and posterior walls. The anterior wall is contributed by the aponeurosis of the external oblique and the anterior layer of the aponeurosis of the internal oblique.
The posterior layer is formed by aponeurosis of the transverses abdominis and a posterior layer of the aponeurosis of the internal oblique.
Lower l/4th – It has only the anterior wall contributed by aponeuroses of all three flat muscles i.e. external oblique, internal oblique and transversus abdominis.
Rectus Sheath Features
- Anterior wall
- Complete
- Fuses with tendinous intersections
- Posterior wall
- Incomplete
- Free from tendinous intersections
Rectus Sheath Function
Increases the efficiency of the rectus abdomen by keeping it in position
Rectus Sheath Contents
Muscles – Rectus abdominis and pyramidalis
Vessels
- Superior and inferior epigastric arteries
- Venae commitments
Nerves
- Lower five intercostal nerves (T7- 11)
- Subcostal nerve.
Rectus Sheath Applied
- Hernia:
- Umbilical – Congenital (Exomphalos), Acquired
- Epigastric – Due to the divarication of recti
- Spigelian – Along linea semilunaris
- Incisions
- Median
- Paramedian
- Zenker’s degeneration

Dissection Steps Of The Rectus Sheath
Identify the rectus sheath. Open the anterior layer of the rectus sheath medially along the middle fibres of the rectus abdominis.
Identify the rectus abdomen and detach it from the tendinous intersections. Reflect the anterior layer of the rectus sheath medially and laterally.
Lift the rectus abdomin divide it transversely at the middle and turn the parts superior and inferior. Identify the posterior layer of the rectus sheath; superior and inferior epigastric vessels and arcuate line.
Additional layers in the abdominal wall
- Fascial linings of the abdominal cavity,
- Over the anterolateral abdominal muscle – Fascia transversal
- Over psoas and iliacus – Iliac fascia/Fascia iliac
- Over diaphragm – Diaphragmatic fascia
- Over kidney – Renal fascia
- In the pelvis – Pelvic fascia
- Extraperitoneal fat
- Peritoneum
Inguinal Canal
Inguinal Canal Definition
The oblique intramuscular passage in the lower part of the anterior abdominal wall.
Inguinal Canal Location
A little above the medial part of the inguinal ligament.
Inguinal Canal Extent
From the deep inguinal ring to the superficial inguinal ring.
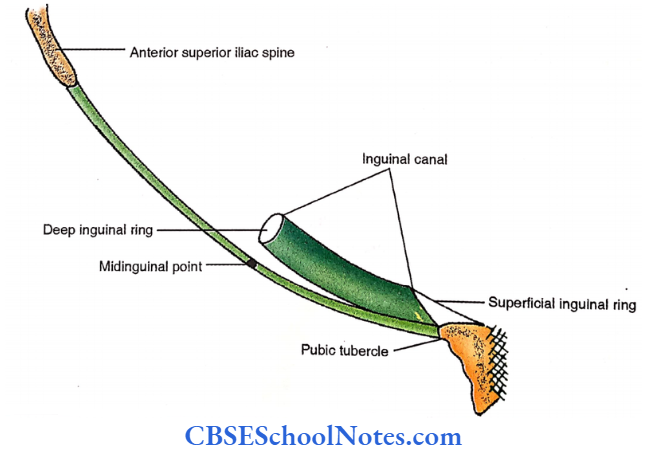
Inguinal Canal Length – 4cm
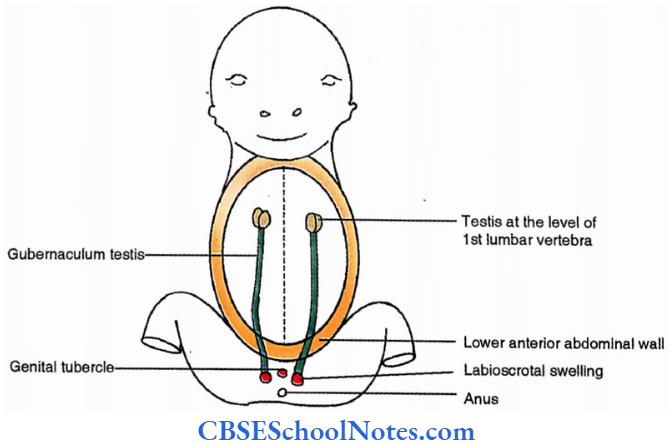
Inguinal Canal Development
- Occupation of passage by Gubemaculm testis (male) or Gubemaculum of ovary (female)
- Facilitated by the adaptation of the same passage by,
- Processus vaginalis and descending testis in male.
- Processus vaginalis (Canal of Nuck) in female.
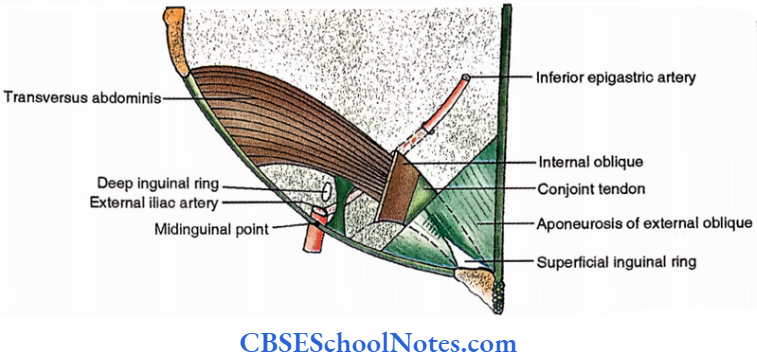
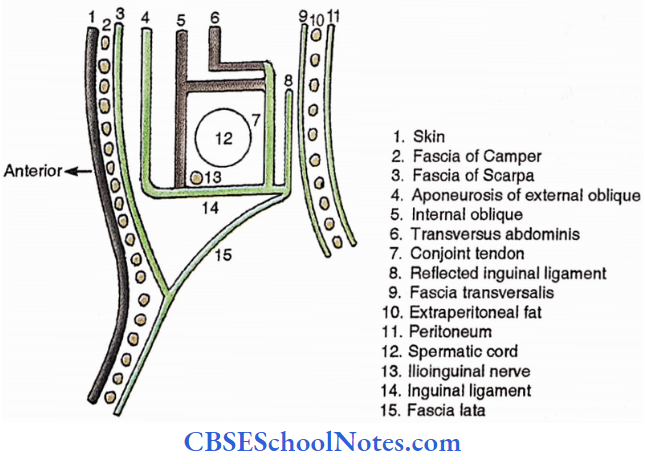
Inguinal Canal Boundaries
Anterior wall
- Skin
- Superficial fascia
- Aponeurosis of external oblique
- Internal oblique ( in the lateral part)
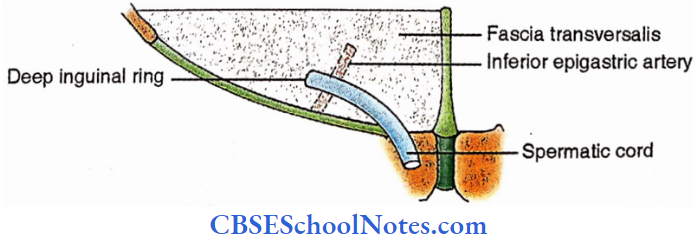
Posterior wall
- Peritoneum
- Extraperitoneal fat
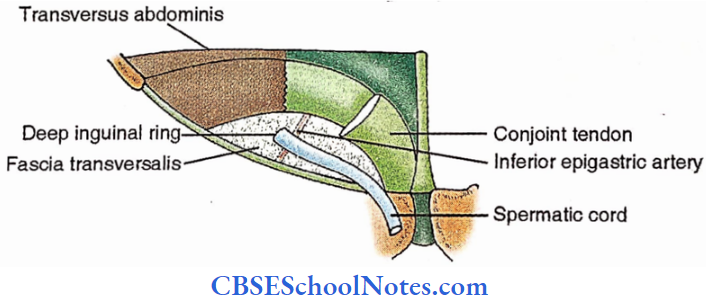
- Fascia transversalis
- Conjoint tendon (Falx inguinalis)
- Reflected inguinal ligament
Roof – Arched fibres of internal oblique and transversus abdominis
Floor – Inguinal and lacunar ligaments.
Inguinal Canal Contents:
- Male- Spermatic cord
- Female- Round ligament of uterus
- Ilioinguinal nerve
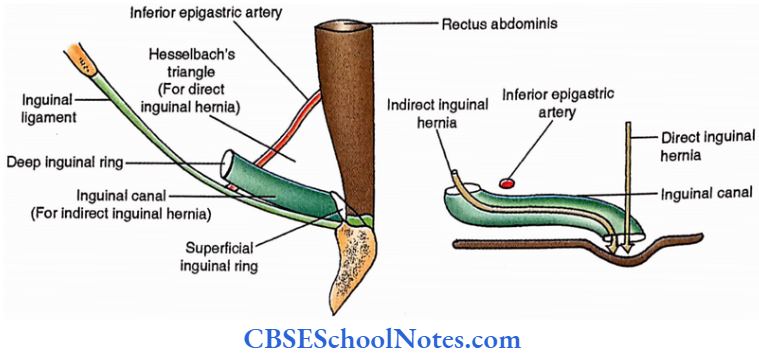
Mechanics of inguinal canal (Factors discouraging inguinal hernia)
- Obliquity – Superficial and deep inguinal rings don’t oppose each other (except in newborn)
- The superficial inguinal ring is strengthened by falx inguinal and reflected ligament
- The deep inguinal ring is strengthened by the internal oblique muscle
- Increased intra-abdominal pressure — Lowering of arched fibres of internal oblique and
transversus abdominis — Narrowing the canal (Shutter mechanism) - Contraction of internal oblique-Traction of the deep inguinal ring (Valvular safety mechanism).
- Squatting posture (during defecation and parturition) – Canal compressed by the thigh.
Inguinal Canal Applied
Inguinal hernia
- Developmental classification
- Incomplete (Bubonocele)
- Complete
- Anatomical classification
- Indirect
- Congenital – Incomplete (Funicular)
- Complete (Vaginal)
- Infantile
- Acquired
- Direct – through Hesselbach’s triangle (bounded by linea alba, inguinal ligament and inferior epigastric artery)
- Indirect
Dissection Steps Of Inguinal Canal
Study the formation of the inguinal canal; its anterior wall, posterior wall, floor and roof and structures passing through it.
Identify the inguinal ligament, superficial inguinal ring, deep inguinal ring, spermatic cord in males round ligament of uterus in females, ilioinguinal nerve and also the conjoint tendon.
Spermatic Cord
Spermatic Cord Definition
Structures which leave or enter the inguinal canal through a deep inguinal ring, together constitute the spermatic cord.
Spermatic Cord Location
- Upper – Inguinal canal
- Lower part – Scrotum
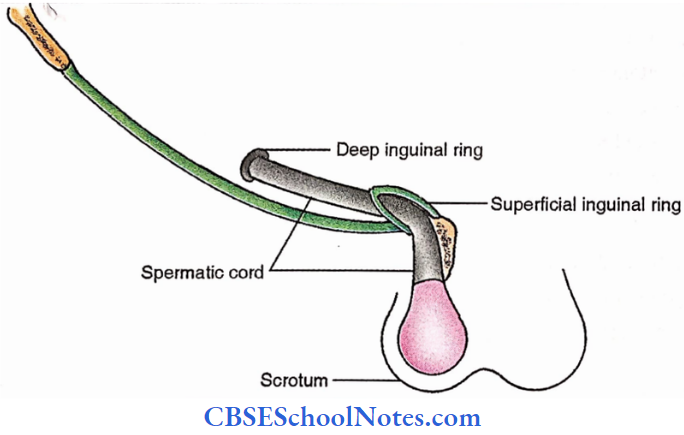
Spermatic Cord Extent
From deep inguinal ring to testis.
Spermatic Cord Constituents
3 Arteries
- Testicular artery (From aorta)
- Artery of vas deferens (From superior vesical artery – a branch of internal iliac artery)
- Cremasteric artery (From inferior epigastric artery)
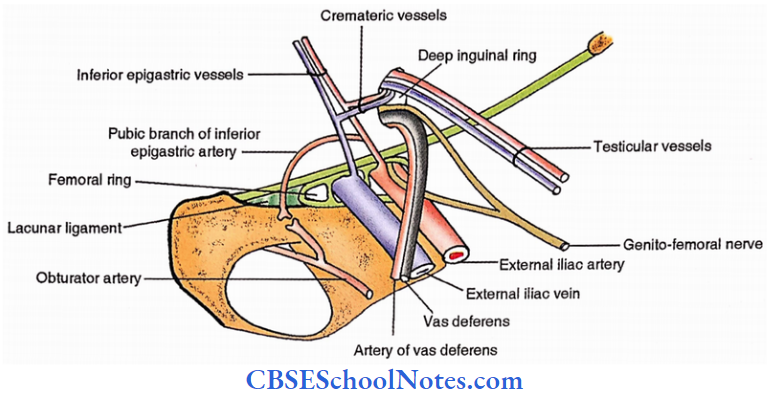
3 veins
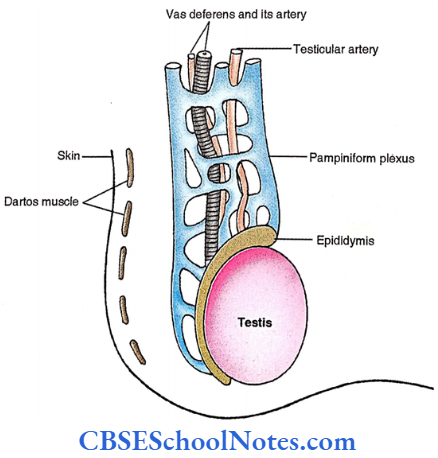
- Accompanying testicular artery (Pampiniform plexus in the scrotum, Venae comitantes in the inguinal canal, Testicular vein in the abdominal cavity)
- Vein of vas deferens which ultimately drains into internal iliac vein
- Cremasteric vein which drains into the external Iliac vein
3 Nerves
- Sympathetic and parasympathetic (autonomic fibres)
- Genital branch of genitofemoral nerve
- Ilioinguinal nerve
3 More structures
- Vas deferens
- Remnant of processus vaginalis
- Lymphatics
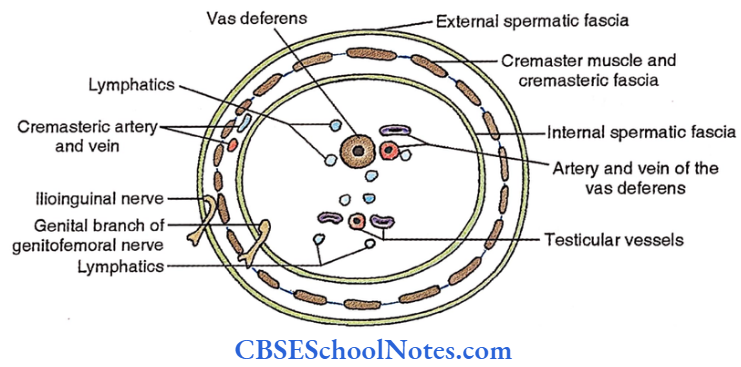
Coverings
- External spermatic fascia (Derived from aponeurosis of external oblique)
- Cremaster muscle and cremasteric fascia (Derived from internal oblique and transversus abdominis)
- Internal spermatic fascia (Derived from fascia transversalis)

Spermatic Cord Applied: Vasectomy
Dissection Steps Of Testis And Spermatic Cord
Make an incision extending from the superficial inguinal ring through the anterolateral aspect of the scrotum. Reflect the dartos muscle from the skin and then reflect the dartos from the loose areolar tissue deep into it.
- Now, lift the testis and spermatic cord from the scrotum cut the spermatic cord at the level of the superficial inguinal ring and remove it along with the testis. Clean and trace the blood vessels into the testis.
- Identify the spermatic cord, ductus deferens and testis. Identify the epididymis (its sinus opening laterally) and free the tail and body of the epididymis from the testis. Make a transverse incision through the testis. Examine it with a hand lens.
Scrotum
Scrotum Definition
Cutaneous fibromuscular pouch for testis and their associated structures
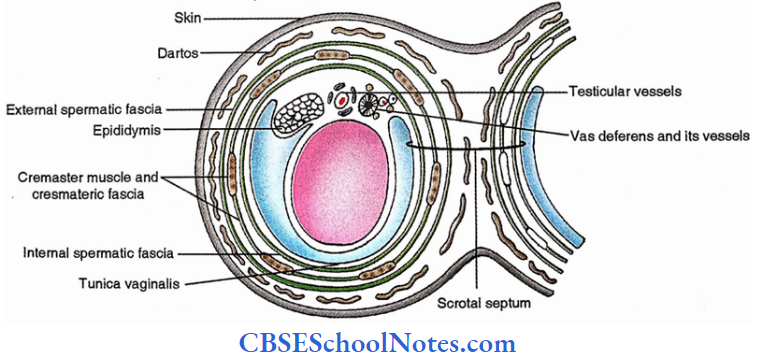
Scrotum Scrotal wall
- Skin
- Thin
- Often rugose
- Pigmented
- Excessive sweat glands
- Subcutaneous tissue
- No fat
- Dartos muscle (smooth muscle supplied by sympathetic fibres)
- External spermatic fascia
- Cremasteric fascia and cremaster muscle
- Internal spermatic fascia
(Note: All the layers, except skin, form the scrotal septum)
Scrotum Functions
- Support of testis
- Thermoregulation of testis
- The temperature of the testis is always maintained below body temperature by a system called Cremasterico -Dartos – Venous complex
- Cremaster undergoes reflex contraction due to excessive cold
- Dartos windows (the gap between muscle fasciculi) open (relaxed) or close (contracted) in response to hot and cold weather respectively to allow the transfer of heat from testicular arterial blood to the skin via pampiniform plexus. This is called a counter-current heat exchange mechanism.
Scrotum Contents (of each half)
- Testis
- Epididymis
- Constituent of the spermatic cord
Testis
- 5 (length) x 2.5 (width) x 3 (A.P. diameter) cm in size
- 10 -14 g in weight
- 2 Surfaces (Medial and lateral)
- 2 Margins (Anterior and Posterior)
- 2 Poles (Superior and Inferior)
- 3 Tunics, from superficial to deep
- Tunica vaginalis
- Parietal layer
- Visceral layer
- It covers, the testis from all its sides except the posterior.
- Tunica albuginea, a fibrous coat.
- Tunica vasculosa, a vascular coat.
- Tunica vaginalis
- Structure
- Septa from mediastinum testis (thickened tunica albuginea in the posterior part) divide the interior of the testis into 200 – 300 compartments
- Seminiferous tubules occupy these compartments (1-4 in each compartment)
- A major part of each seminiferous tubule is coiled except adjacent to the mediastinum, where
it becomes straight - Rete testis – It is a tubular plexus in which seminiferous tubules open
- Vasa efferentia. These are 6-12 thin tubules connecting the rete testis with the head of the epididymis
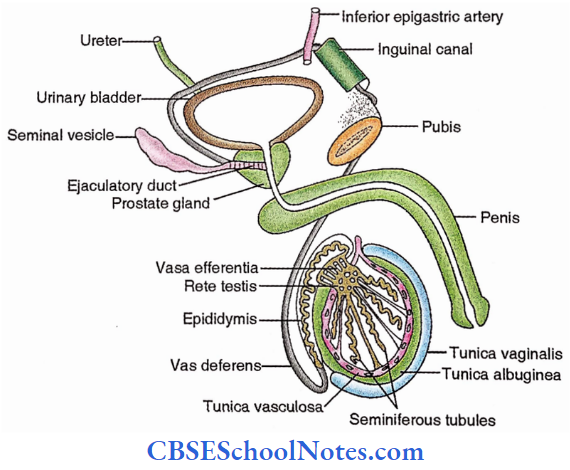
Epididymis
- It is located postero-lateral to the testis
- It is a coiled single-tube
- It has 3 Parts – Head, Body, Tail
- Tail continues with vas deferens which are located posterior to the testis and medial to the epididymis.
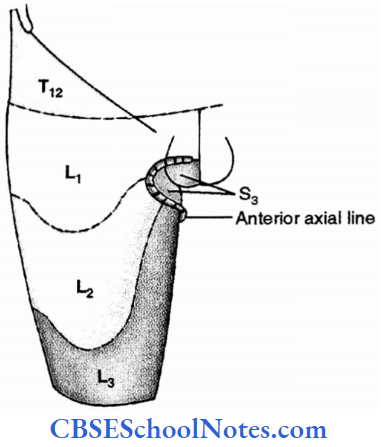
Nerves
- Skin-Posterior 2/3rd – S3 – Scrotal nerve. It is a branch of the perineal nerve, which itself arises from the pudendal nerve
- Perineal branch of the posterior cutaneous nerve of the thigh
- Anterior l/3rd – LI – Ilioinguinal nerve
- Dartos – Sympathetic (with the perineal branch of S4 or genitofemoral nerve).
- Coverings – Genital branch ofGenito-fermoral nerve.
- Testis – Sympathetic (T10) Preganglionic fibres —> Lesser splanchnic nerve —> Renal and aortic plexuses —> Postganglionic fibres run with testicular artery
- Epididymis – Sympathetic (T11, L2 and LI )
Arteries
- Skin – Pudendal arteries – Both superficial and deep external pudendal arteries arise from the femoral artery. The internal pudendal artery arises from the internal Iliac artery.
- Fibromuscular layers- Cremasteric artery- It is a branch of the external iliac artery.
- Testis – Testicular artery —It is a branch of the abdominal aorta.
Veins
- Skin – Pudendal veins – Both superficial and deep external pudendal veins drain into great
saphenous vein. - Venae comitantes ofinternal pudendal artery- These drain into internal iliac vein.
- Fibromuscular layers- Cremasteric vein – It is a tributary of the external iliac vein.
- Testis – Testicular vein- On the right side it drains into the inferior vena cava while on the left side, it enters into the left renal vein.
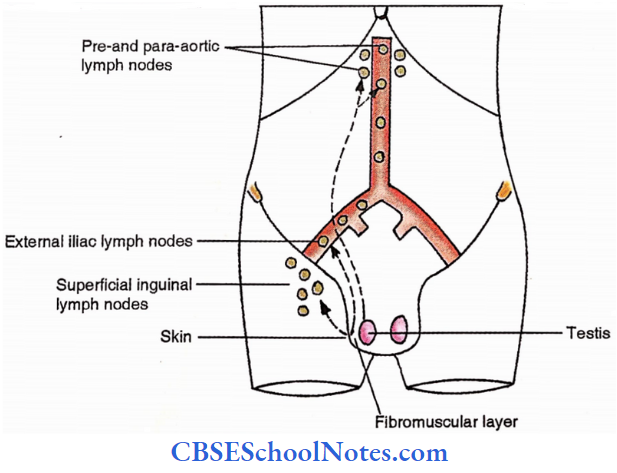
Lymphatics
- Skin – Superficial inguinal lymph nodes (Medial group of horizontal chain)
- Fibromuscular layer- External iliac lymph nodes
- Testis – Pre- and Para-aortic lymph nodes

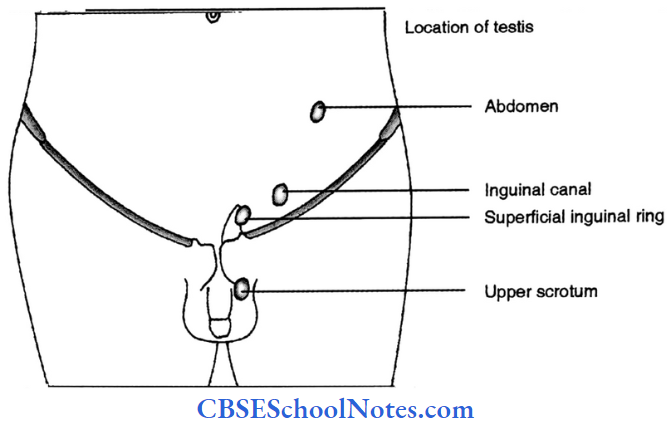
Scrotum Applied
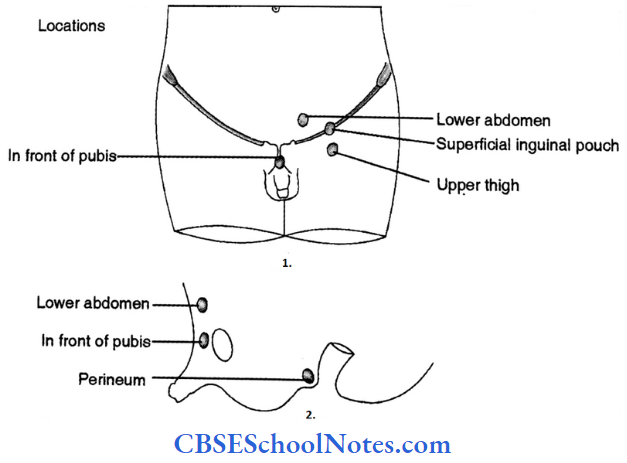
- Imperfect descent
- Incomplete descent
- Maldescent (Ectopic testis)
- Testicular pain -Referred to umbilicus due to common segmental (T10) innervation
- Malignancy of testis-Involves abdominal lymph nodes
- Varicocele of pampiniform plexus
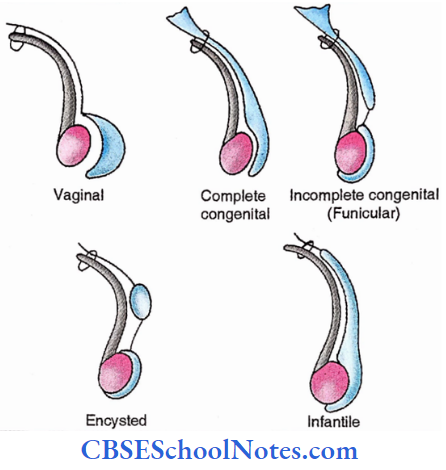
- Hydrocele
- Congenital
- Complete type
- Incomplete type (Funicular)
- Infantile
- Encysted
- Acquired (Vaginal)
- Primary (cause unknown)
- Secondary (known cause)
- Congenital
Peritoneum
Peritoneum Definition
The serous membrane lining the abdominal cavity and covering its viscera or connecting the two.
Peritoneum Parts
- Parietal layer – It lines the wall of the abdomen and pelvis
- Visceral layer – It covers the viscera of the abdomen and pelvis
- Folds – These are double layers of the peritoneum which connect the viscera or with abdomen wall. These are of the following types,
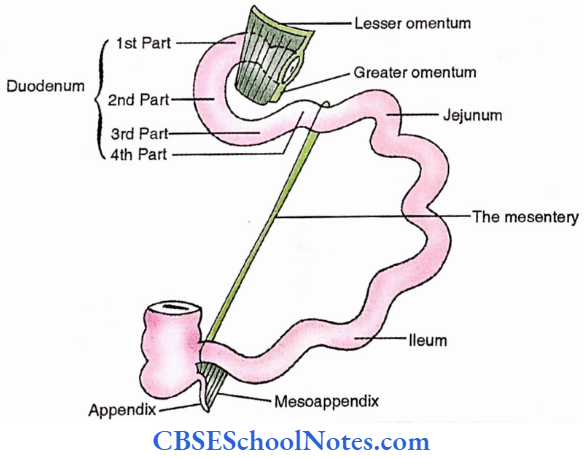
- Connecting mobile viscera with the abdominal wall. This is termed as “MESENTERY”. These are named after viscera For Example.,
- of the small intestine – The Mesentery
- of the colon – Mesocolon<Transverse mesocolon / Sigmoid mesocolon)
- of the appendix – Mesoappendix
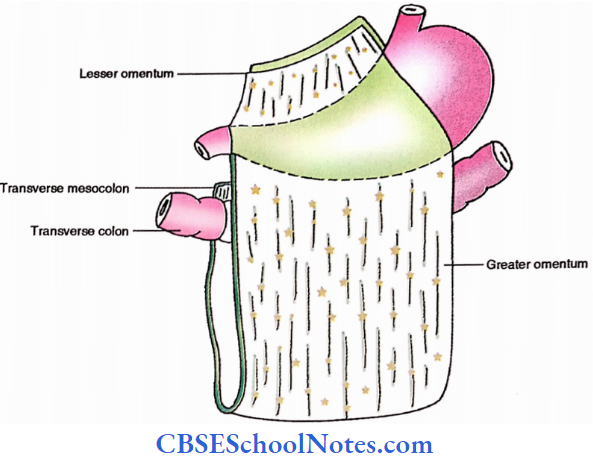
- Connecting stomach with adjacent viscus. This is termed as “OMENTUM”. These are named differently depending on the viscus to which it is connected, For Example.,
- With liver – Lesser omentum
- With a transverse colon – Greater omentum
- With spleen-gastrosplenic omentum
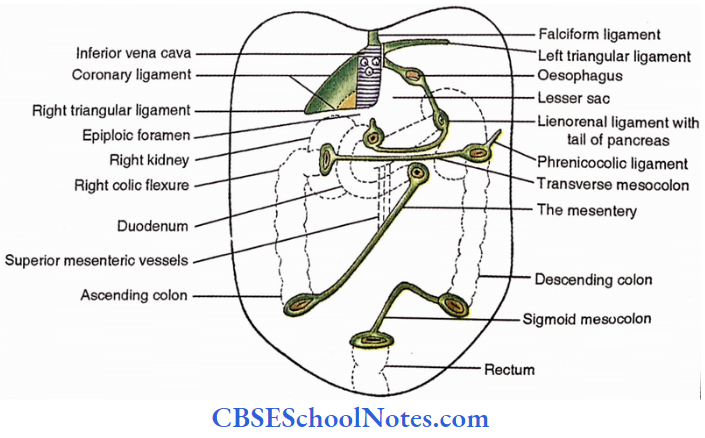
- Connecting relatively less mobile viscera (For Example., liver) with the abdominal wall.
- These are termed “LIGAMENTS” as shown below,
- Ligaments of the liver – Falciform, Coronary, Triangular.
- Ligament of spleen – Lienorenal ligament
- Connecting mobile viscera with the abdominal wall. This is termed as “MESENTERY”. These are named after viscera For Example.,
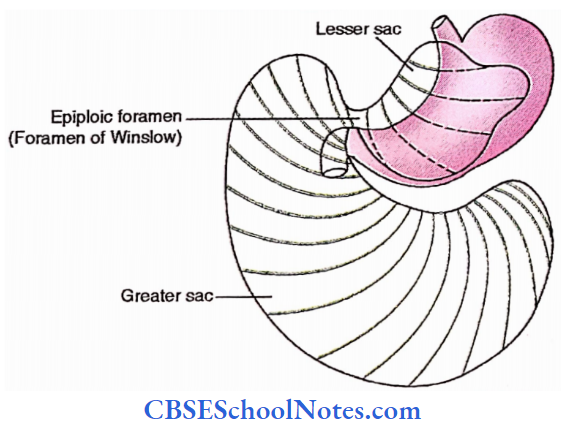
1. Peritoneal Cavity
Potential space between parietal and visceral layers is called the peritoneal cavity which can be broadly divided into,
- Greater sac
- Lesser sac
Communication between the two sacs is called epiploic foramen or foramen of Winslow.
Arrangement
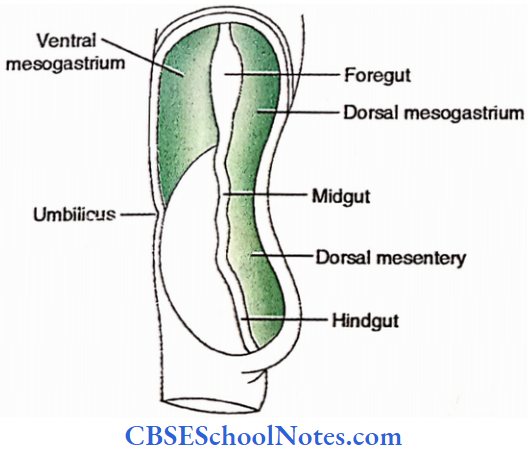
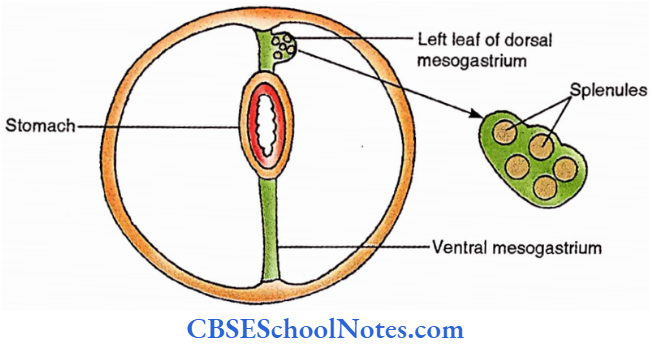
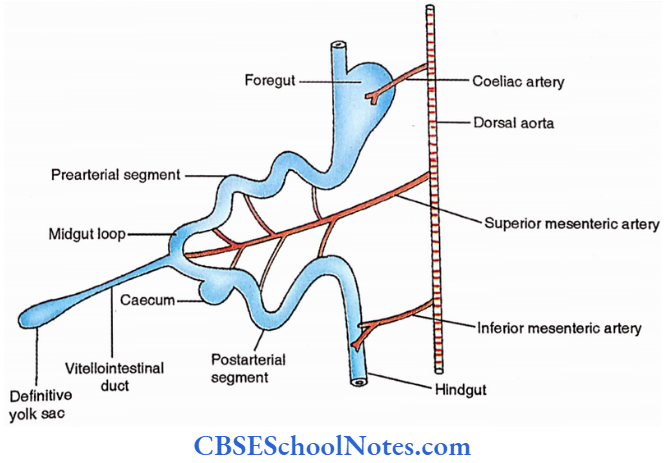
Developmental correlation
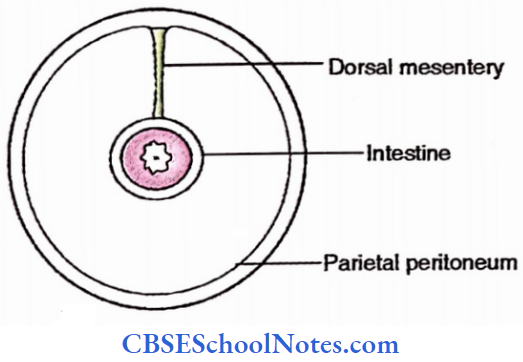
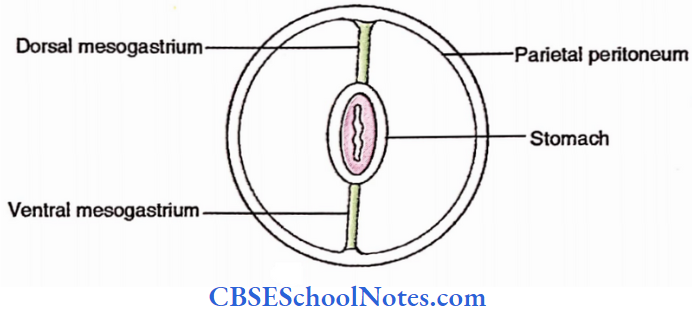
The mesentery of primitive gut,
- Dorsal – Present thought out the gut
- Ventral – It is present only in the region of the stomach and proximal duodenum and is therefore called ventral mesogastrium.
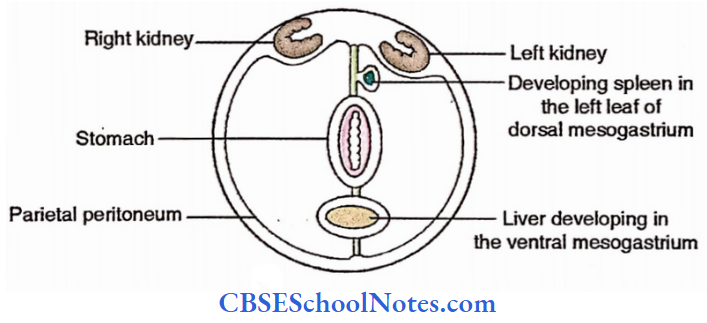
Spleen developsin dorsal mesogastrium dividingitinto lienorenal ligament and gastrosplenic ligament.
The liver develops in the ventral mesogastrium dividing it into falciform ligament and lesser omentum.

Rotation of the stomach brings the following changes,
- A smaller sac goes behind the stomach and the lesser omentum
- Spleen comes to lie in the left hypochondriac region
- The liver is shifted to the right hypochondriac region

- Gut with dorsal mesentery
- Fall of gut on the posterior wall
- The gut loses its mesentery and becomes retroperitoneal
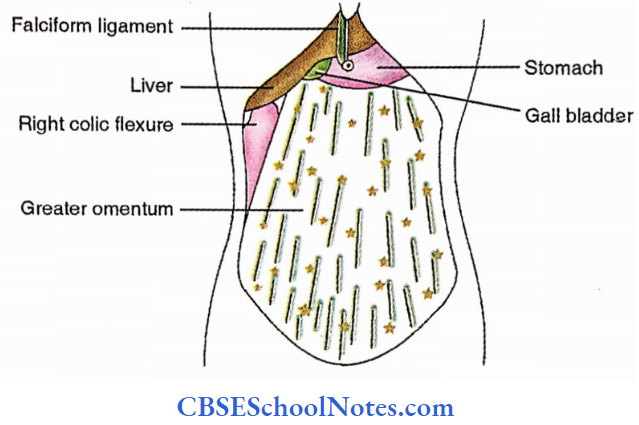
Peritoneal reflection observed by palpation
I – Immediately after opening the abdomen one can observe the following;
- Liver, Falciform ligament
- Gall Bladder
- Stomach
- Greater omentum
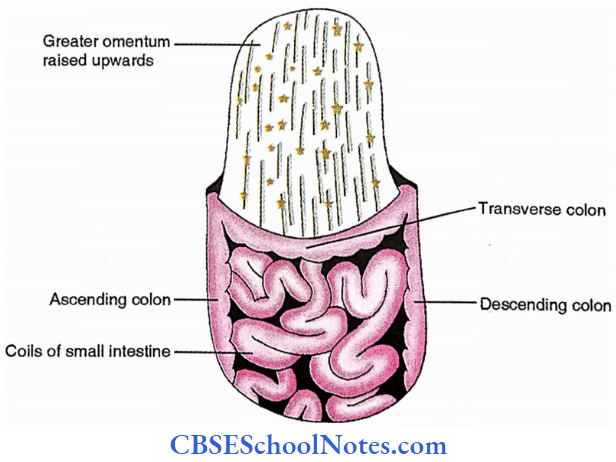
After elevation of the greater omentum following visceral parts are found,
- Coils of small intestine
- Colons – Transverse, ascending and descending
2. Further Exploration
1. Vertical disposition
Palpate the posterior surface of the anterior abdomen wall glide your hand upwards from the umbilicus and palpate the following in sequence,
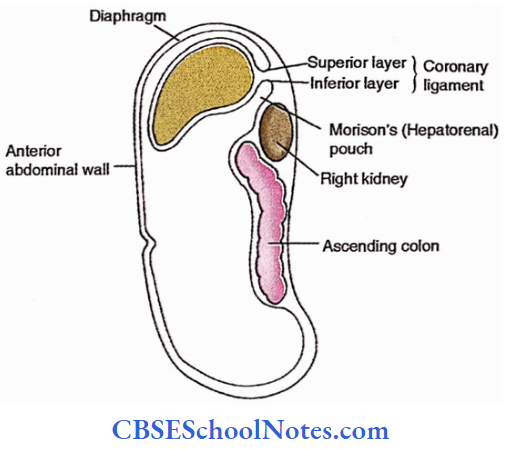
- First to the right falciform ligament
- Anterior abdominal wall —> Diaphragm —> Sperior layer of a coronary ligament —> Liver —> Inferior layer of a coronary ligament —> posterior abdominal wall (having, right kidney, right lateral paracolic gutter, ascending colon, right medial paracolic gutter).
- Secondly to the left of the falciform ligament.
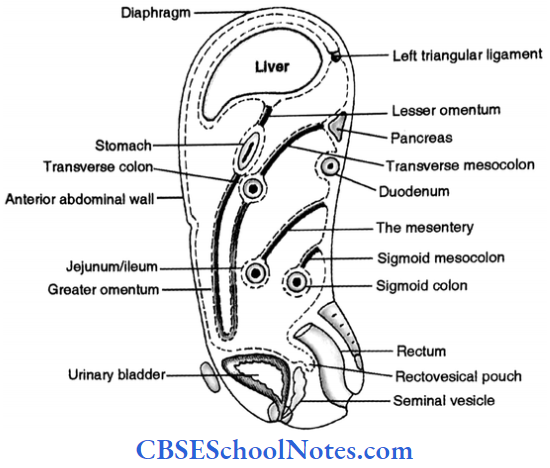
- Anterior abdominal wall —> Diaphragm —> Anterior layer of a left triangular ligament —> Liver —> Lesser omentum —> Stomach —> Greater omentum —> Transverse colon —> Transverse mesocolon —> Posterior abdominal wall (with the pancreas, duodenum, right medial paracolic gutter) —> Right infrasonic compartment —> Right layer of the mesentery —> Jejunum and ileum —> Left layer of the mesentery —> Left infrasonic compartment —> Sigmoid mesocolon and colon —> Rectum.
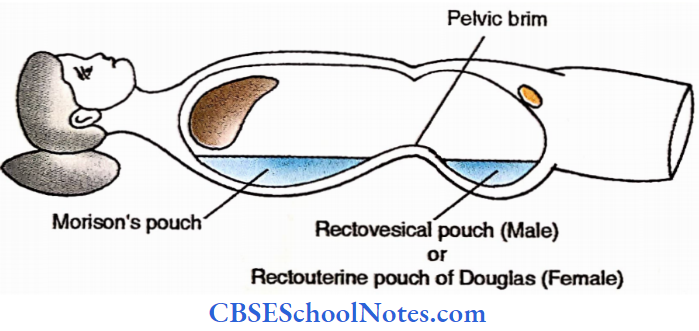
Peritoneal reflections (from posterior to anterior pelvis differ in males and females.
Male: Rectum —> Rectovesical pouch —> Urinary bladder
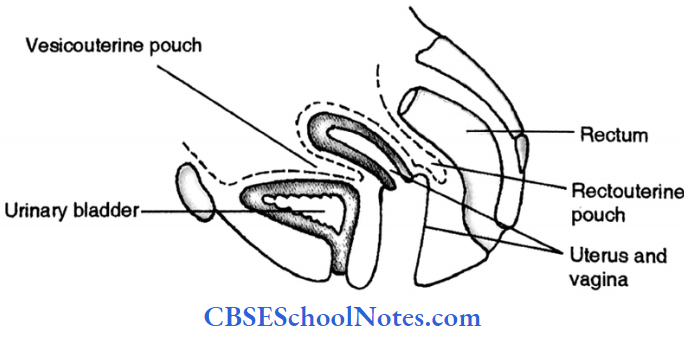
Female: Rectum —> Rectouterine pouch of Douglas —> Uterus and Vagina —> Vesicouterine pouch —> Urinary bladder
From the superior surface of the urinary bladder, the peritoneum continues over the anterior abdominal wall to reach the umbilicus.
2. Horizontal disposition
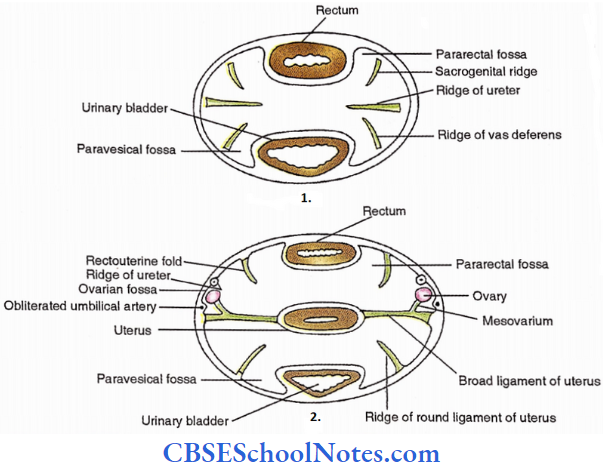
Pelvis
Fossae
- Pararectal fossa – By the side of rectum
- Ovarian fossa – In the lateral wall just anterior to internal iliac vessels
- Paravesical fossa – By the side of the urinary bladder Ridges.
- Urogenital ridge – It limits the pararectal fossa laterally in males.
- Ridge for vas deferens -It limits the paravesical fossa laterally in male
- Ridge for ureter – Located in the lateral wall of the pelvis just in front of internal iliac vessels
- Recto-uterine fold – It limits the para-rectal fossa laterally in females.
- Ridge for round ligament of the uterus – It limits the paravesical fossa laterally in female
- Broad ligament of the uterus -It connects the side of the uterus with the lateral wall of the pelvis.
Lower abdomen (Below umbilicus)
Anterior abdominal wall
- Folds
- Median umbilical fold – Raised by urachus
- Medial umbilical fold – Raised by obliterated umbilical artery
- Lateral umbilical fold – Raised by inferior epigastric artery
- Fossae
- Supravesical fossa – Between median and medial umbilical folds
- Medial inguinal fossa – Between medial and lateral umbilical fold
- Lateral inguinal fossa – Over deep inguinal ring. Just lateral to lateral umbilical fold.
- Femoral fossa – Over femoral ring

Posterior abdominal wall
- Paracolic gutters
- Right, about ascending colon.
- Left, to descending colon. (Both are medial as well as lateral)
- Colons – Ascending and descending
- The mesentery and ileum.
Upper abdomen (Above umbilicus)

Go towards the left from the falciform ligament on the posterior surface of the anterior abdominal wall and feel the following structures;
Falciform ligament —> Lienorenal ligament —> Spleen —> Gastrosplenic ligament —> Stomach —> Lesser omentum —> Epiploic foremen —> Anterior wall of lesser sac —> Gastrosplenic ligament —> Hilum of spleen —> Lienorenal ligament —> Posterior wall of lesser sac (pancreas, aorta, inferior vena cava) —> Epiploic foramen —> Right kidney —> Right abdominal wall —> Filciform ligament.
Dissection Steps Of Peritoneum
Identify the parietal peritoneum and cut it transversely at the level of the umbilicus and turn the upper and lower parts superior and inferior respectively.
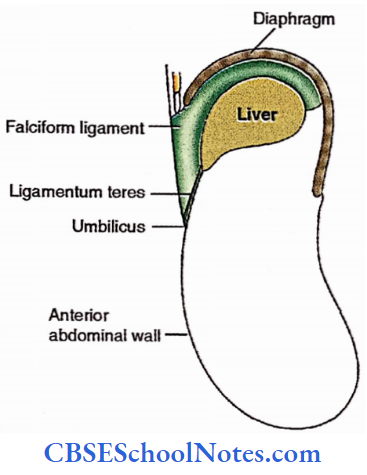
- Examine and identify the peritoneal ligaments falciform ligament and ligamentum teres hepatitis and also the ligaments in the infra umbilical portion from its deeper aspect.
- Identify the greater omentum and its parts and the lesser omentum and its parts as well as the transverse mesocolon. Note the locations of abdominal viscera in situ; supra-and infracolic compartments as well as epiploic foramen.
- Pull the stomach down and to the left and the liver up and to the right to locate the epiploic foramen. Pass the index and middle finger of the left hand through it and feel the surfaces.
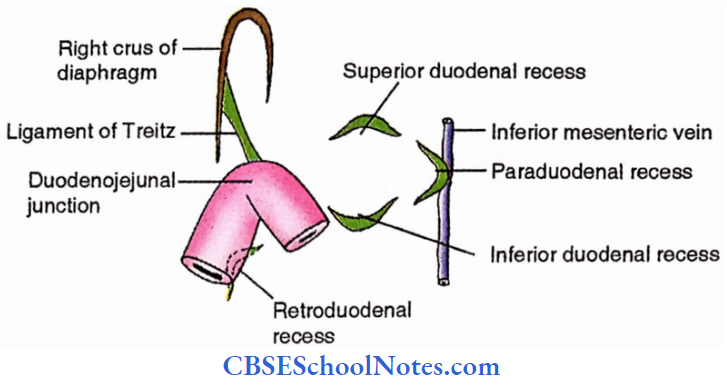
Peritoneal Recesses And Fossae
1. Doudenal recesses
- Paraduodenal recess (inferior mesenteric vein is related to it)
- Superior duodenal recess
- Inferior duodenal recess
- Retroduodenal recess
Recesses (1), (2) and (3) are located just to the left of the duodenojejunal junction while recess (4) is lying behind the 4th part of the duodenum.


2. Caecal recesses
- Superior ileocaecal
- Inferior ileocaecal
- Retrocaecal
Recesses 1 and 2 are located about the ileocaecal junction while recess 3 is lying behind the caecum.
3. Intersigmoid fossa
It is enclosed by an inverted ‘V’ shaped attachment of sigmoid mesocolon.
Subphrenic spaces
- Extraperitoneal
- Right – Bare area of the liver (Near right suprarenal gland)
- Left – Near left suprarenal gland and upper pole of left kidney.
- Intraperitoneal
- Right
- Anterior (Between front of the right lobe of the liver, upper layer of coronary ligament and diaphragm).
- Posterior (Between right kidney, lower layer of coronary ligament and right lobe of the liver. This is also called hepatorenal or Morison’s pouch).
- Left
- Anterior (Between front of the left lobe of the liver, anterior layer of left triangular ligament and diaphragm).
- Posterior (Lesser sac)
- Right
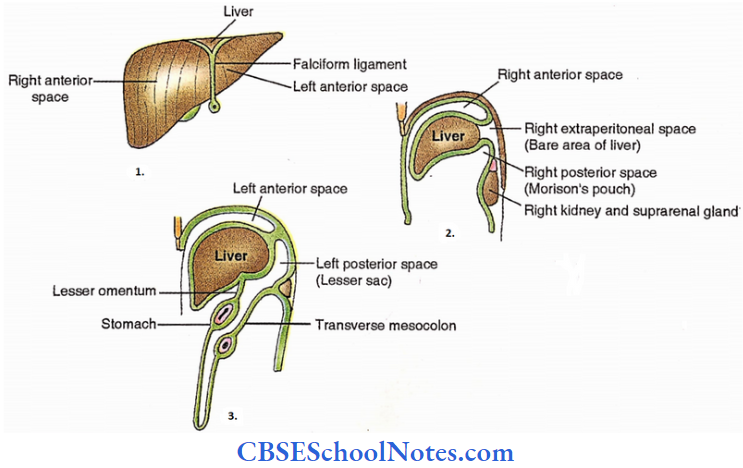
- About the front of the liver
- The sagittal section of the upper abdomen to the right of the falciform ligament
- The sagittal section of the upper abdomen to the left of the falciform ligament
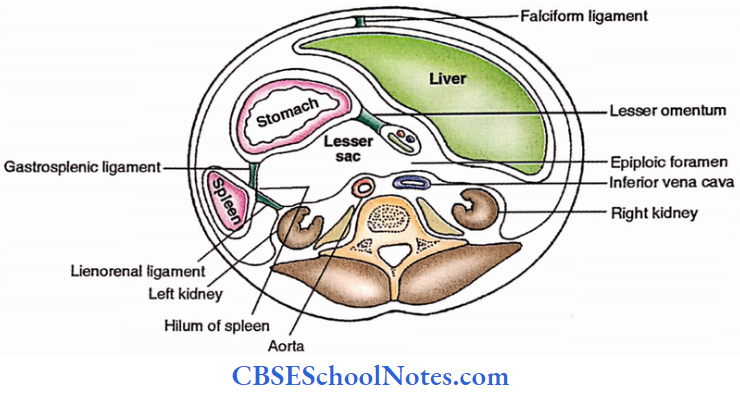
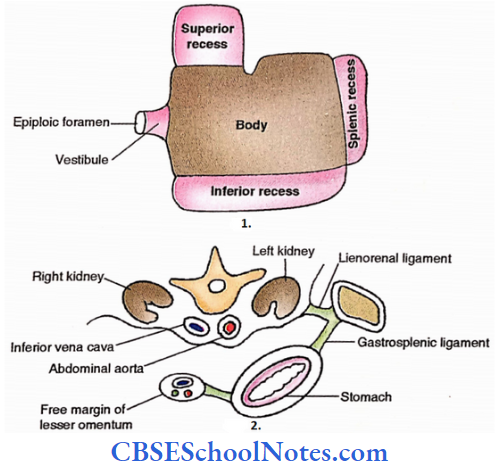
Lesser Sac
- The peritoneal cavity behind the stomach and lesser omentum
- 4 borders
- Superior – Extends to the diaphragm
- Inferior – Extends to the greater omentum
- Left – Extends to the hilum of the spleen
- Right – Has foramen of Winslow or Epiploic foramen
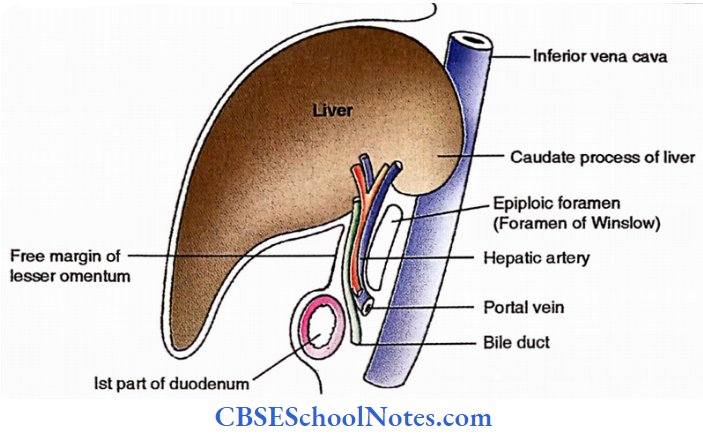
- Epiploic foramen – Its boundaries are as follows,
- Anterior – Free margin of lesser omentum (with portal vein, bile duct and hepatic artery)
- Posterior – Inferior vena cava
- Superior – Caudate process of liver
- Inferior – 1st Part of duodenum
- Parts
- Body – Central part. It is the main portion.
- Vestibular – It is the right extension which joins the body with the epiploic foramen
- Superior recess – Between body and superior border.
- Inferior recess – Between body and inferior border.
- Splenic recess – Between body and left border
- Relations
- Anterior – Stomach, lesser omentum, caudate lobe.
- Posterior – Stomach bed. (Transverse colon, transverse mesocolon, pancreas, left kidney, left suprarenal gland, diaphragm, spleen, splenic artery)
- Gastropancreatic folds in the posterior wall,
- Its right portion is produced by the hepatic artery while its left part is raised by the left gastric artery.
Lesser Sac Applied
- Internal abdominal hernia is common through epiploic foramen which sometimes leads to strangulations
- Perforation of posterior gastric ulcer leads to communication between the stomach and lesser sac.
Functions Of Peritoneum
- Lubrication
- Storage of fat
- Folds carry vessels and nerves to and from viscera
- Support of viscera
- Localization of inflammation
- The greater omentum is also called abdominal policeman as it covers the inflammatory sites and limits its spread.
- Absorption of peritoneal fluid.
- To resist the infection by leukocytes and antibodies
Nerves
Parietal peritoneum
- Diaphragmatic
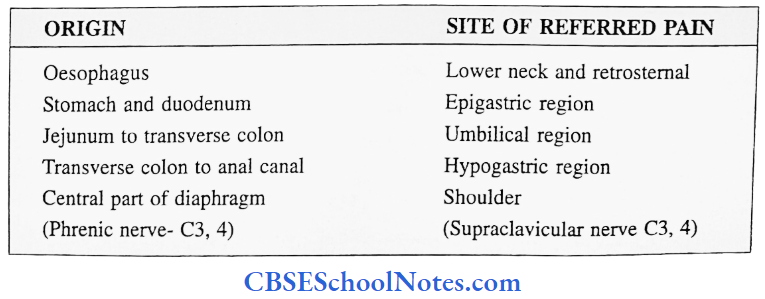
- The central part is supplied by the phrenic nerve explaining the referred pain to the shoulder.
- The peripheral part is innervated by lower intercostal nerves.
- Over abdominal wall
- It is supplied by lower intercostal. Iliohypogastric and ilioinguinal nerves
- Pelvic -It is innervated by the obturator nerve.
Visceral peritoneum
Autonomic nerves supplying the viscera also supply the peritoneum covering it.
Functions of peritoneum Applied
- Inflammation is termed as peritonitis
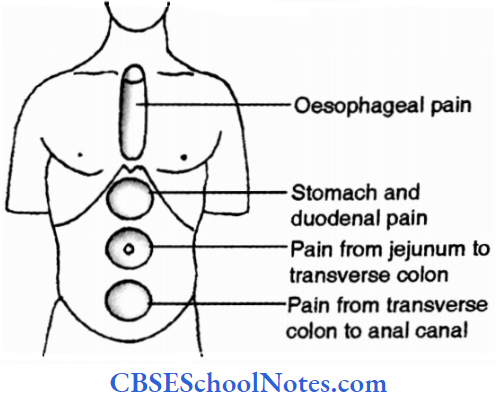
- Pain
- from parietal peritoneum -It is severe and precisely localized in nature
- from viscera-It is dull, poorly localized and referred to the anterior midline as shown below.
Greater omentum acts as an “Abdominal policeman”
- Peritoneal cavity
- The collection of fluid is called ascites
- Paracentesis is the procedure to drain excess fluid in the peritoneal cavity
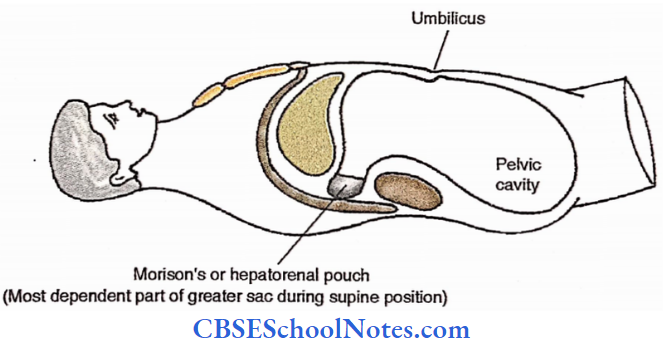
- Collection of pus in Morison’s and rectovesical pouches is common due to their being
most dependent parts of the abdominal cavity in supine posture. - If there is strangulation of the herniated intestinal loop in the para duodenal fossa, take care of an inferior mesenteric vein in its anterior wall during operation.
Stomach
Stomach Definition
The most dilated part of the foregut is situated between the oesophagus and duodenum.
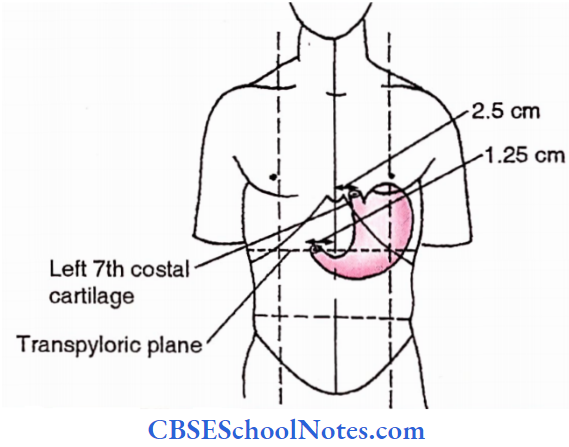
Stomach Location:
It occupies the following regions – Left hypochondriac, epigastric, umbilical
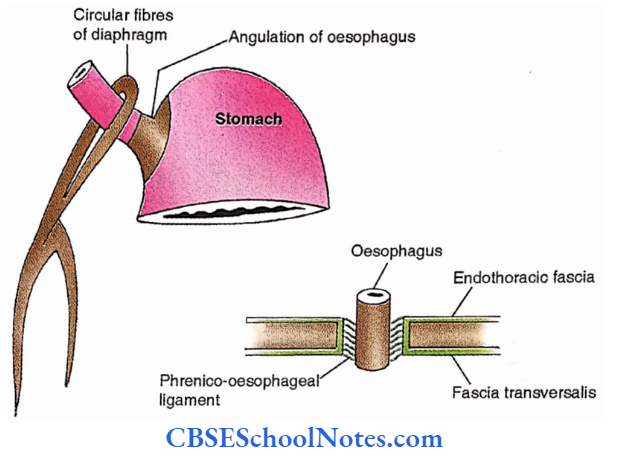
Stomach Two orifices
- Cardiac orifice (Proximal opening). This orifice acts as a physiological sphincter due to the following arrangements,
- Circular fibres of diaphragm, oesophagus and stomach
- Phrenico – oesophageal ligament
- Angulation of the oesophagus with stomach
- Mucosal folds
- Pyloric orifice (Distal opening)
- It has well well-defined anatomical sphincter i.e., a thick circular muscle coat in the wall.
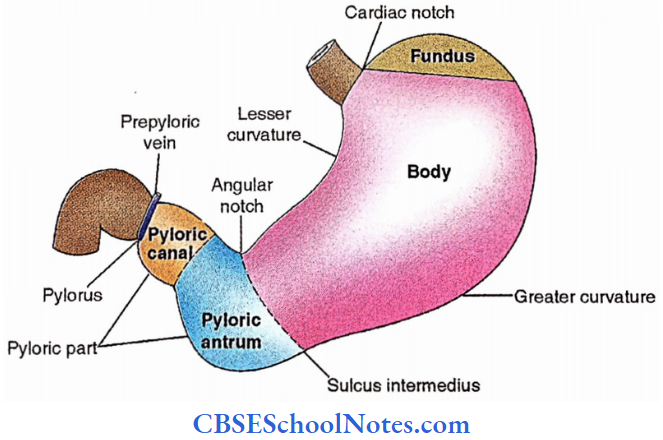
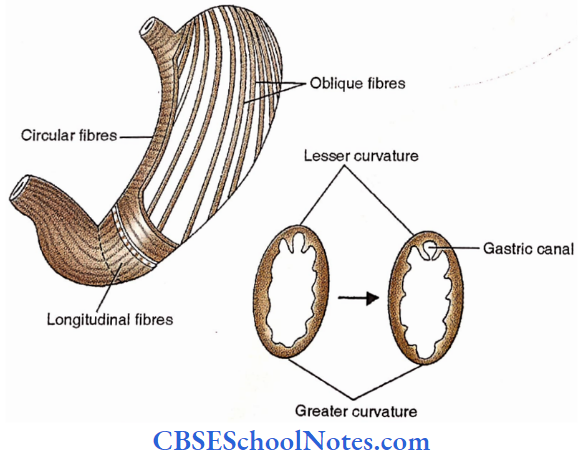
Stomach Two borders
- Lesser curvature- Small, concave, right border. A deep notch in its distal part is called an angular notch.
- Greater curvature- Large, convex, left border. A depression in its distal part is called sulcus intermedius
Stomach Two Surfaces
- Anterior – It faces anteriorly and superiorly.
- Posterior – It faces posteriorly and inferiorly
Stomach Parts
- Fundus – Part of the stomach above the level of the cardiac orifice.
- Body – Part of stomach between fundus and angular notch.
- Pyloric part – Part of stomach distal to angular notch. It has two components.
- Antrum – proximal portion
- Pyloric canal – distal portion
Stomach Capacity
- At birth- 30 ml
- At puberty – 1 litre
- In Adults – 1.5 litre
Stomach Structure
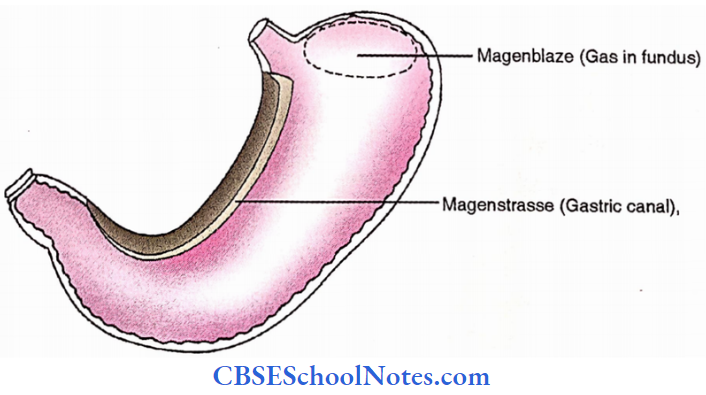
Magenstrasse (Gastric canal) – It is a narrow tunnel along lesser curvature produced due to the contraction of oblique fibres of the muscular coat of the stomach.
Magenblaze – It is gas in fundus
Stomach Relations
1. Peritoneal relations
- Lesser curvature receives lesser omentum from the liver. It has two parts,
- Hepatogastric ligament – Between liver and stomach.
- Hepatoduodenal ligament – Between the liver and 1st part of the duodenum
- Greater curvature receives attachments of greater omentum which has three parts,
- Gastrophrenic ligament – Between stomach and diaphragm.
- Gastrosplenic ligament – Between stomach and spleen.
- Gastrocolic ligament – Between stomach and transverse colon.

2. Visceral relations
- Anterior (LAD)
- L = Liver
- A = Anterior abdominal wall
- D = Diaphragm
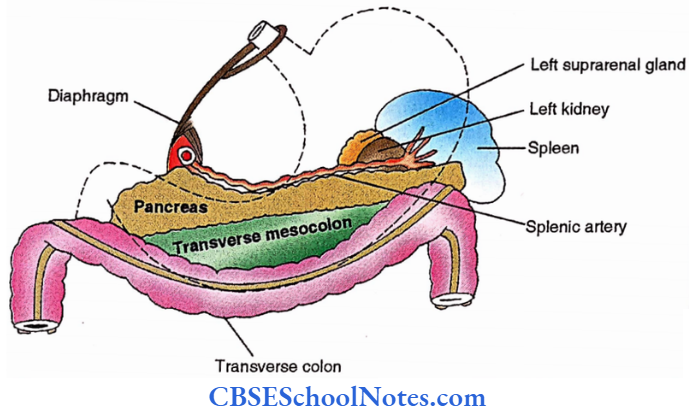
- Posterior – Lesser sac and stomach bed
(Tickle me please, killing sensations disappear so soon)
T = Transverse colon
M = Mesocolon (Transverse)
P = Pancreas,
K = Kidney (Left)
S = Suprarenal gland (Left)
D = Diaphragm
S = Spleen
S = Splenic artery
Stomach Functions
- Temporary storage
- Mixing
- Partial digestion
- Partial absorption
- Sense of fullness
- HCl secretion
- Intrinsic factor secretion (+ Extrinsic factor i.e. B12 = Hemopoietic factor)
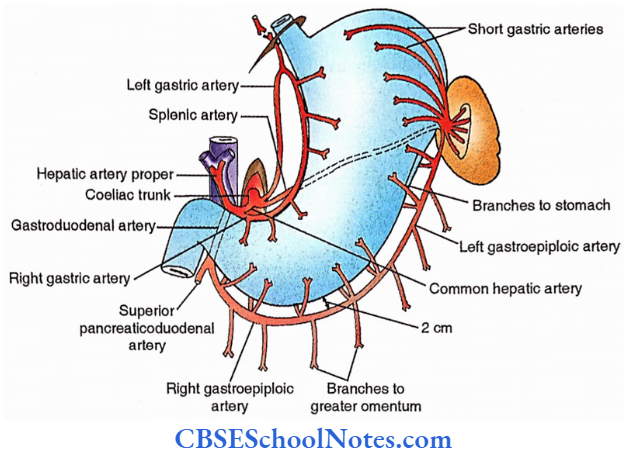
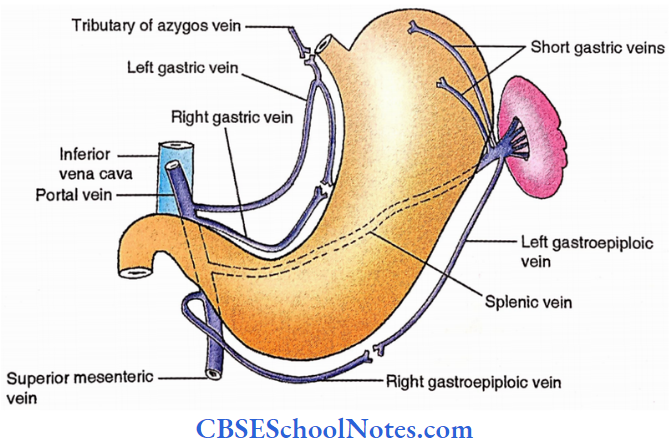
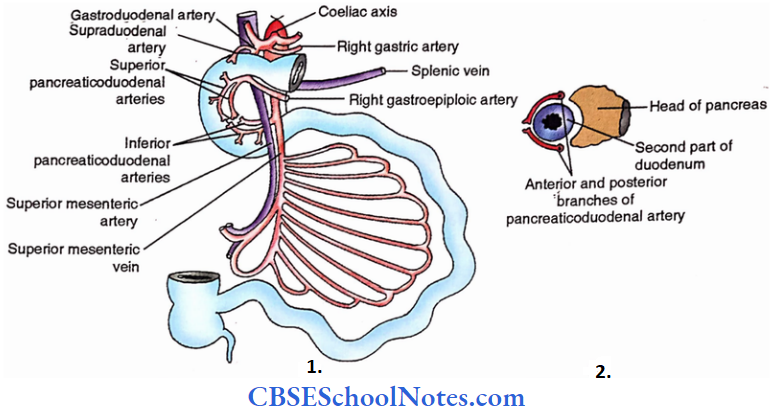
Stomach Arteries
Coeliac artery
- Gastric arteries
- Right gastric artery. It arises from the hepatic artery and runs towards the left along the right portion of lesser curvature.
- Left gastric artery. It arises from the celiac trunk and runs retroperitoneally towards the cardiac end where it enters the lesser omentum and follows the lesser curvature to meet its fellow artery.
- 5 Short gastric arteries arise from the splenic artery to supply the fundus and upper part of the body.
- Posterior gastric arteries arise from the splenic artery and supply its posterior surface.
- Gastroepiploic arteries
- The right gastroepiploic artery arises from the gastroduodenal artery and runs towards the left parallel to and 2 cm from the greater curvature
- The left gastroepiploic artery is a branch of the splenic artery and runs towards the right gastroepiploic artery.
- Gastroepiploic arteries supply both the stomach as well as greater omentum.
Stomach Veins
Portal vein
Accompany arteries of the same name and ultimately drain into the portal vein
Stomach Nerves
Parasympathetic
Anterior vagal trunk (Mainly contributed by left vagus)
Branches
- Gastric
- Hepatic
- Pyloric
Posterior vagal trunk (Mainly contributed by right vagus)
Branches
- Gastric
- Coeliac

Functions
- Motor to glands
- Motor to muscles
- Inhibitory to pylorus
Stomach Sympathetic
Fibres originate from the 6th to the 9th thoracic segments of the spinal cord.
These runs in greater (T5-9) and lesser (T9-10) splanchnic nerves to relay in the coeliac plexus. Branches of celiac plexus accompany the branches of the coeliac trunk.
Functions
- Motor to vessels
- Motor to pylorus
- Sensory
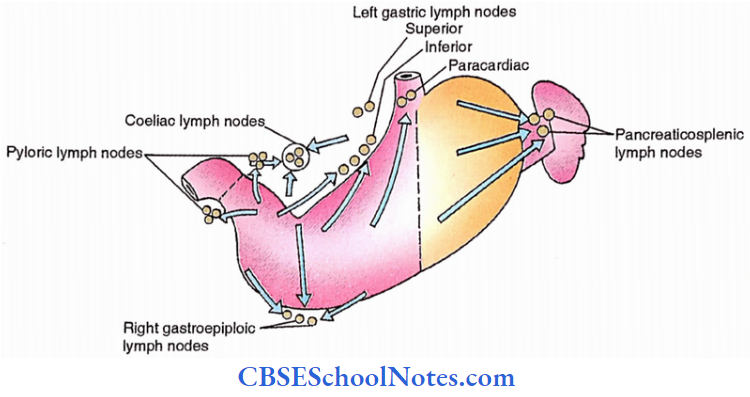
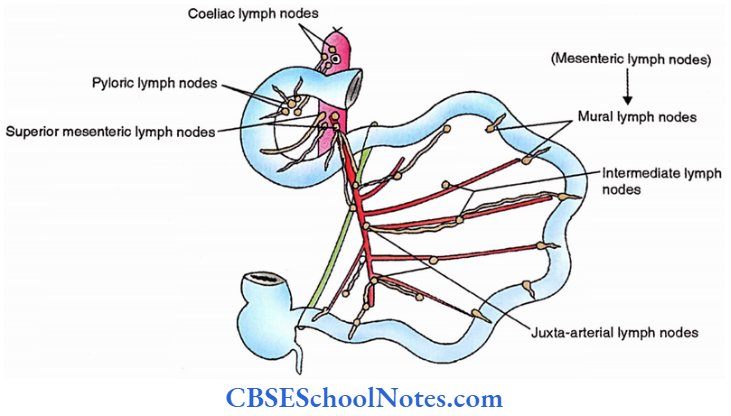
Lymphatic drainage
Coeliac lymph nodes ultimately receive lymphatics from the stomach after being interrupted by the following lymph nodes.
- Left gastric lymph nodes (about the superior left gastric artery) These can be superior, inferior and pericardiac.
- Right gastroepiploic lymph nodes (About right gastroepiploic artery)
- Pancreatic – splenic lymph nodes (Concerning the hilum of the spleen)
- Pyloric lymph nodes (About the pyloric end of the stomach)
Dissection Steps Of Stomach
Identify the organ in situ and note its gross features. Note the cardiac and pyloric ends and their differences. Identify the peritoneal folds of the stomach. Note the vessels in the greater omentum.
- Tie two ligatures some distance apart right to the pyloric sphincter. Turn the stomach along the right gastric and right gastroepiploic vessels to the left side and then identify the omental bursa.
- Strip off the peritoneum along the lesser curvature and identify the celiac trunk and its branches; left kidney and suprarenal. Pull the cardiac end down tie 2 ligatures some distance apart and cut in between the two ligatures.
- Cut at the pyloric end and remove the stomach and while doing so identify the branches of the splenic artery. Study the gross features of the stomach. Identify the pyloric region and sphincter.
- Note the structures forming the stomach bed. Open the stomach along the greater curvature and examine its interior. Strip off muscles from a part of the stomach and study.
Stomach Applied
- Gastric ulcers can be treated by vagotomy and partial gastrectomy. The latter removes the gastrin-bearing area of the stomach i.e. anterior part.
- Gastric malignancy needs radical gastrectomy.
- Gastroscopy is an endoscopic procedure with the help of a gastroscope to visualize the interior of the stomach.
Spleen
Spleen Definition
Largest single lymphoid organ
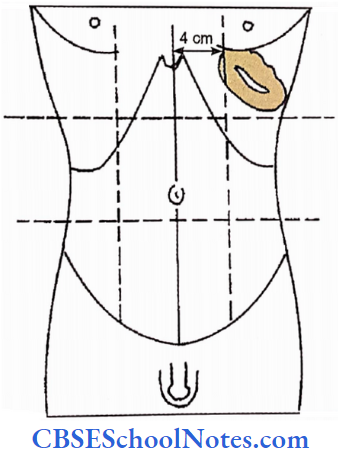
Spleen Location
Left hypochondriac region
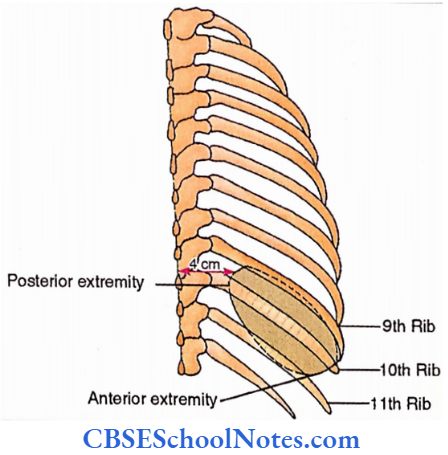
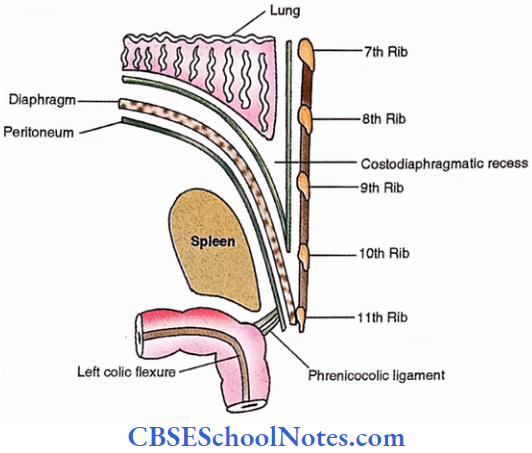
Spleen Extent
Horizontal – From the side of the rounded vertebral column to the midaxillary line
Vertical – From 9th to 11th rib
Spleen Development
It develops at the age of the 7th week of intrauterine life in the left leaf of the upper dorsal mesogastrium.
Weight – 150 g
Spleen Measurements
Thickness = 3-4 cm
Width = 7 cm
Length = 12 cm
Spleen Extremities – Anterior and Posterior
Spleen Borders
- Superior – It is notched
- Inferior
- Intermediate (Margo intermedialis)
Spleen Surfaces
- Diaphragmatic
- Visceral
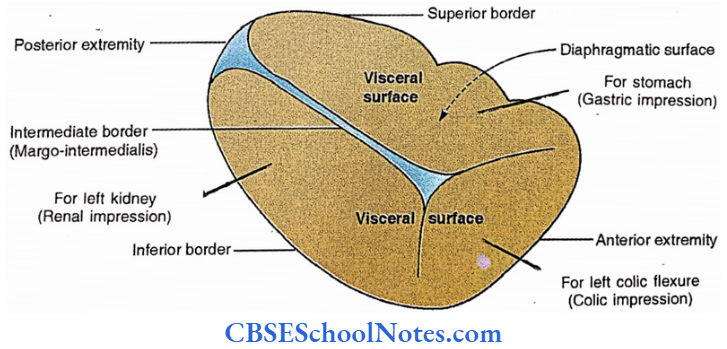
Spleen Relations
1. Peritoneal
Most of the surfaces of the spleen are covered with peritoneum except the hilum on the visceral surface which is bare for the passage of splenic vessels and the tail of the pancreas (pancreatic impression).
Ligaments

2. Adjacent relations
- The diaphragmatic surface is related to,
- Diaphragm
- Left lung and costodiaphragmatic recess
- 9-11 ribs and intercostal space
- The visceral surface has the following- Impressions
- Gastric for stomach
- Renal for the left kidney
- Colic for left colic flexure
Spleen Functions
- Phagocytosis (Graveyard)
- Immune responses (Guard)
- Cytopoiesis (Factory)
- Lymphopoiesis
- Haemopoiesis (In foetus)
- Erythrocyte storage – (Blood bank)
In humans – it is discharged by elastic recoil.
In lower mammals – it is discharged by contraction of the capsule
Artery
Splenic artery- 5 branches enter the spleen
Vein
Splenic vein- 5 tributaries appear from the spleen
Lymphatic
Pancreaticosplenic lymph nodes in the hilum drain the spleen. Their efferents drain into coeliac lymph nodes.
Nerves
The Coeliac plexus provides innervation to the spleen which is sympathetic.
Spleen Segmentation
84 % — 2 Segments — Superior and inferior
16 % — 3 Segments — Superior, intermediate, inferior
Dissection Steps Of Spleen
Palpate spleen in the left hypochondrium. Push the stomach to the right and identify the upper part of the greater curvature. Identify the fold of the peritoneum extending from there to the hilum of the spleen.
- Identify the vessels in the gastrosplenic ligament. Push the transverse colon downward on the left including the left colic flexure and push the spleen upwards towards the left dome of the diaphragm and note the fold of the peritoneum extending between the spleen and the left kidney.
- Examine the organ in situ note its anatomical position and also note the relations. Cut ligaments at the hilum remove the organ and study its gross features including various impressions on its visceral aspect.
Spleen Applied
- Splenomegaly (Enlargement of spleen )— Spleen is palpated when it is double the size.
Splenomegaly is noticed in Malaria, Typhoid, Portal hypertension - Splenectomy (Surgical removal of spleen). Tail of the pancreas should be saved during operation which is located in the lienorenal ligament.
- Kehr’s sign
Small Intestine
Small Intestine Extent
Gastroduodenal (Pyloroduodenal) Junction to Ileocaecal junction
Small Intestine Parts and lengths
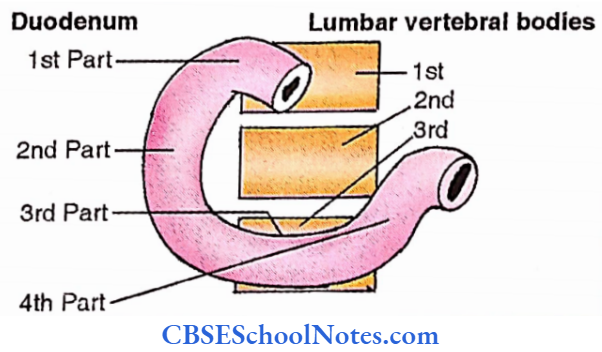
- Duodenum – 10″ / 25cm
- 1st / Superior part – 2″
- 2nd / Descending part – 3″
- 3rd / Horizontal part – 4″
- 4th / Ascending part – 1″
- Jejunum – 2/5th, 87 240 cm / 2.4 m
- Ileum – 3/5th, 12′ / 360cm / 3.6 m
Jejunum and ileum together – 20′ / 6m
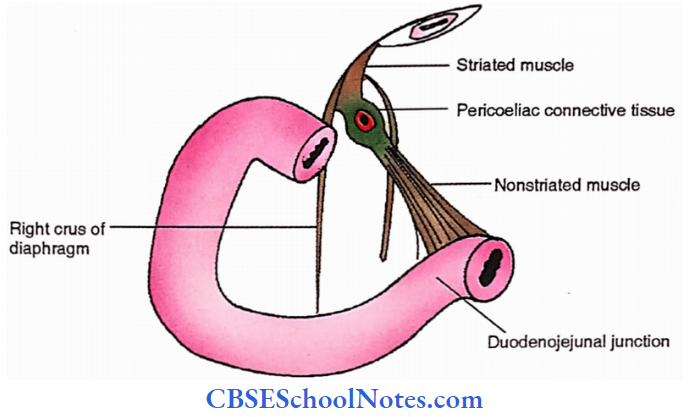
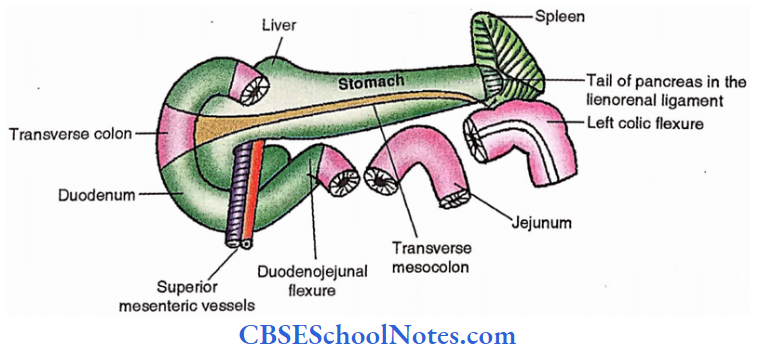
Duodenojejunal Junction is marked by the ligament of Treitz which is a fibromuscular band connecting the junction with the right crus of the diaphragm.
Small Intestine Relation
1. Peritoneal relations
1st inch of the superior part of the duodenum is covered by the peritoneum and receives lesser and greater omenta along its superior and inferior borders respectively
Rest of duodenum- Retroperitoneal
The jejunum and ileum are mobile but attached to the posterior wall of the abdomen by a double layer of peritoneum called the mesentery. Features, of the mesentery, are as follows,
- Fan shaped
- Free margin – holds jejunum and ileum.
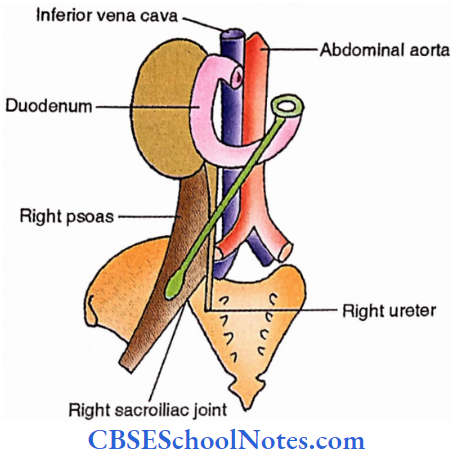
- The attached margin is called the root of the mesentery, it extends from the left side of the 2nd lumbar vertebra to the right sacroiliac joint. It is 15 cm in length. This root crosses the following structures,
- Duodenum (3rd part)
- Aorta
- Inferior vena cava
- Right ureter
- Right psoas
- The average width of the mesentery is 20 cm
- Between two layers are enclosed vessels, nerves, lymph nodes and fat.
2. Adjacent relations
Duodenum
- Vertebral relations
- 1st Part — To the right of 1st lumbar vertebra.
- 2nd Part — To the right of 2nd and 3rd lumbar vertebrae.
- 3rd Part — Across the 3rd lumbar vertebra.
- 4th Part — To the left of the 2nd lumbar vertebra.
- Structures in vicinity
1st Part
- Superior
- Epiploic foramen
- Hepatic artery
- Lesser sac (related to 1st inch only)
- Inferior
- Head of the pancreas
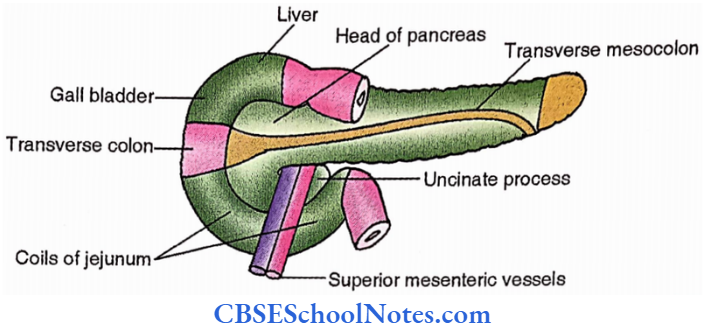
- Anterior
- The quadrate lobe of the liver
- Gall bladder
- Posterior
- Common bile duct
- Gastroduodenal artery
- Portal vein
- Inferior vena cava
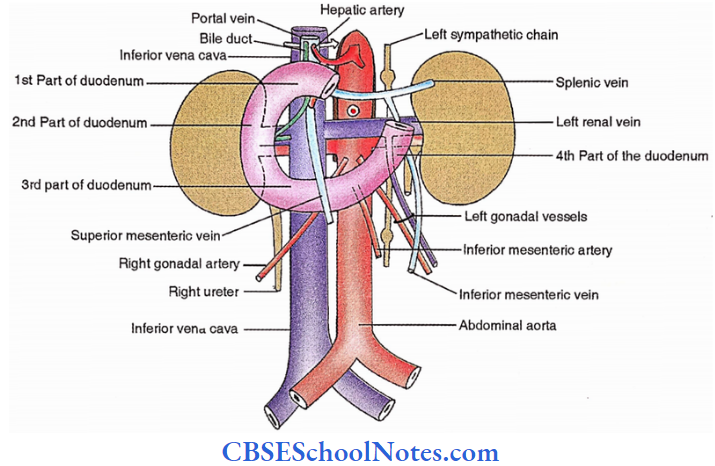
2nd Part
- Anterior
- Gall bladder
- The right lobe of the liver
- Transverse colon
- Coils of intestine
- Posterior
- Hilum of the right kidney
- Right pelvis and ureter
- Right renal vessels
- Inferior vena cava
- Right psoas
- Lateral
- The right lobe of the liver
- Medial
- Head of a pancreas
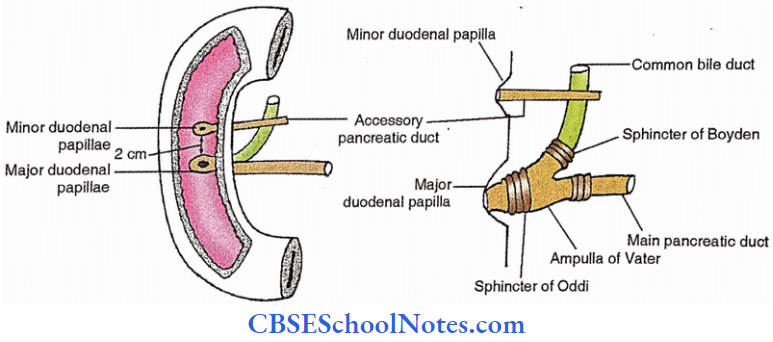
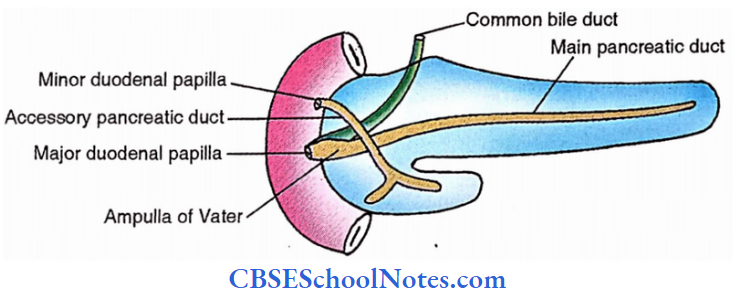
The posteromedial wall is pierced by main and accessory pancreatic ducts producing major and minor duodenal papillae respectively on the mucosal surface.
3rd Part
- Anterior
- The root of the mesentery
- Superior mesenteric vessels
- Coils of jejunum
- Posterior
- Right crus of diaphragm
- Right psoas
- Inferior vena cava
- Aorta
- Right gonadal artery
- Origin of inferior mesenteric artery
- Right ureter
- Superior
- Head of the pancreas
- Inferior
- Coils of jejunum
4th Part
- Superior
- Body of pancreas
- Anterior
- Transverse colon and mesocolon
- Posterior
- Left psoas
- Left sympathetic trunk
- Left gonadal and renal vessels
- Inferior mesenteric vein
- Right
- Beginning of root of mesentery
- Left
- Left kidney and ureter
Jejunum and ileum
- Location
- Jejunum – Upper abdomen
- Ileum – Lower abdomen and pelvis
Feature of small intestine
- Duodenum
- Most proximal
- Smallest
- Widest
- Most sessile
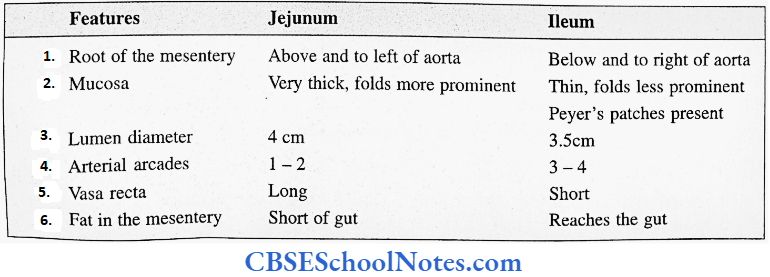
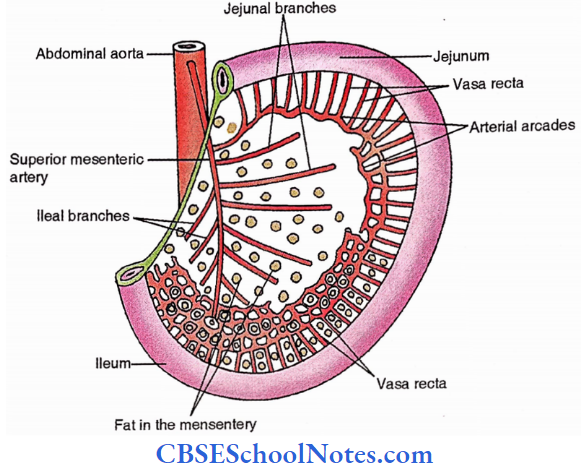
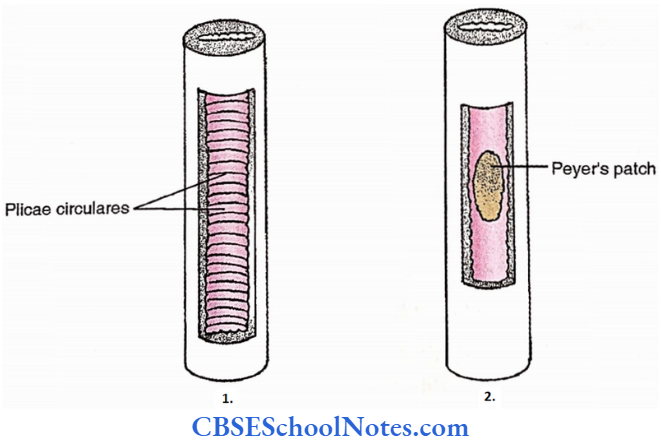
- Jejunum and Ileum
Meckel’s diverticulum (Ileal diverticulum)
- Definition – Persistence of intra-abdominal part of vitello-intestinal duct
- Incidence – 3%
- Location – 1 meter proximal to ileocaecal junction
- Length – 5 cm
- Applied
- Intestinal obstruction is more common.
- Meckelian diverticulitis – resembles appendicitis
- Peptic ulcer may occur if the gastric mucosa develops in Meckel’s diverticulum.
- Littre’s hernia (Herniation of Meckel’s diverticulum)
Arteries of small intestine
- Ultimate artery
- Up to the middle of 2nd part of the duodenum – Coeliac trunk
- Rest of small intestine – Superior mesenteric artery
- Named branches
Duodenum
- Supraduodenal artery from gastroduodenal artery.
- Right gastric artery.
- Right gastroepiploic artery.
- Superior pancreaticoduodenal artery
- Inferior pancreaticoduodenal artery
Jejunum and Ileum
12-15 Jejunal and ileal branches of the superior mesenteric artery
Veins of small intestine
- Portal vein – Veins of the small intestine drain into the portal vein directly or indirectly via a superior mesenteric vein.
- The prepyloric vein is a surgical guide to the pylorus – It drains into the right gastric vein.
Lymphatic drainage of the small intestine.
- Duodenum
- Upper part — Pyloric lymph nodes- Coeliac lymph nodes
- Lower part — Superior mesenteric lymph nodes
- Jejunum and ileum
- Mesenteric lymph nodes
- Mural lymph nodes (close to intestinal wall)
- Intermediate lymph nodes
- Juxta-arterial lymph nodes.
- Superior mesenteric lymph nodes (close to the origin of an artery)
- Mesenteric lymph nodes
Nerves of small intestine
- Ultimate source
- Sympathetic – T9-10, via splanchnic nerves
- Parasympathetic – Vagus
- Supply
- Upper duodenum – Coeliac plexus
- Rest – Superior mesenteric plexus
Applied anatomy of the small intestine
1. Duodenum
- Ulcers
- Anterior wall – Common
- Posterior wall – Uncommon. If perforated, causes erosion of the gastroduodenal artery and profuse bleeding
- Paraduodenal fossa may be site of internal abdominal hernia.
- Adjacent relations of the duodenum are surgically important.
2. Jejunum and ileum
- Tumour or cyst of the mesentery is more mobile across the attachment of the mesentery
- Referred pain is felt usually at the umbilicus
- Thrombosis/embolism of the superior mesenteric artery leads to gangrene of the small intestine.
Dissection Steps Of Small Intestine
Pull duodenojejunal flexure downwards. Tie two ligatures at the duodenojejunal flexure some distance apart (1″). Cut small intestine between these ligatures. Pass two ligatures 2 inches proximal to the iliocaecal junction and cut the small intestine.
- Cut the mesentery along the attachment on the posterior abdominal wall. Remove the small intestine and flush its lumen thoroughly.
- Cut a piece of jejunum and ileum along with the mesentery (about 6 inches in length). Study both parts and note their differences. Open the jejunum and ileum along their antemesenteric border and study the interior.
Pancreas
Pancreas Definition
Lobulated, soft, exo-endocrine gland
Pancreas Length 12 – 15 cm
Pancreas Parts
- Head with uncinate process
- Neck (2 cm wide)
- Body
- Tail
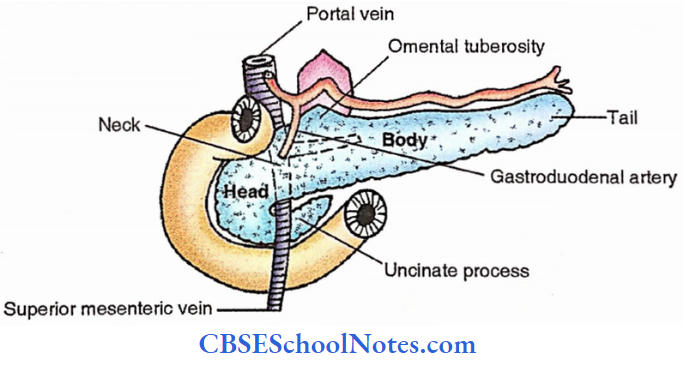
Pancreas Relation
- Head
- Margin- Concavity of duodenum
- Anterior – Transverse colon
- Jejunum
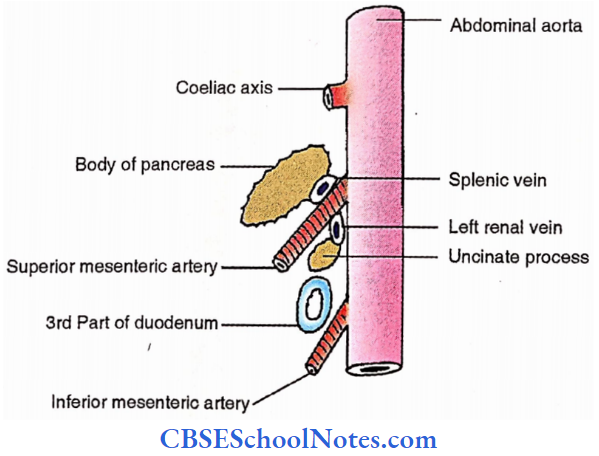
- Superior mesenteric vessels (anterior to uncinate process)
- Posterior- Inferior vena cava
- Neck
- Anterior- Gastroduodenal artery
- Posterior- Superior mesenteric vein and portal vein
- Body
- 3 Surfaces
- Anterosuperior
- Lesser sac and stomach
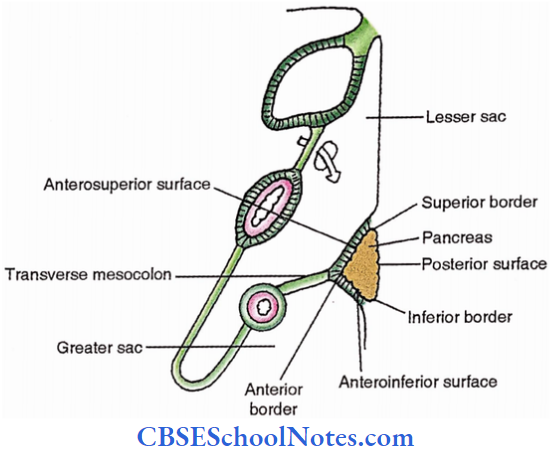
Anteroinferior
- Jejunum
- Two flexures, duodenojejunal and left colic flexures
Posterior
- Aorta
- Superior mesenteric artery
- Left crus of the diaphragm
- Left renal vessels
- Left kidney and suprarenal gland
- Splenic vein

3 borders
- Anterior – Transverse mesocolon
- Superior- Splenic artery. It has omental tuberosity which is related to liver
- Inferior – Superior mesenteric vessels
Tail -It passes through the splenorenal (lienorenal) ligament to reach the hilum of the spleen
Ducts of pancreas
Main pancreatic duct – It unites with the common bile duct to form the ampulla of Vater whose wall is marked by the sphincter of Oddi. It opens on the summit of the major duodenal papilla, a smooth elevation in the mucosa of the posteromedial wall of 2nd part of the duodenum.
Accessory pancreatic duct – It opens on the summit of the minor duodenal papilla located in the duodenal mucosa above the major duodenal papilla.
Artery
- Head – Superior and inferior pancreaticoduodenal arteries
- Rest of pancreas – Splenic artery.
Vein – Veins draining the pancreas open into the portal, superior mesenteric and splenic veins.
Lymphatics
- Pancreaticosplenic lymph nodes
- Pancreaticoduodenal lymph nodes
- Efferents from the above two groups drain into coeliac or superior mesenteric lymph nodes.
Nerves
- The Coeliac plexus provides autonomic fibres to the pancreas
- Parasympathetic-> Right vagus — to parenchyma
- Sympathetic → T7-9 — To parenchyma, Vasomotor
Pancreas Applied
- Diabetes mellitus – Reduced Insulin — Increased blood sugar
- Cancer of the head – Persistent obstructive jaundice
Dissection Steps Of Pancreas And Duodenum
Turn the tail and body of the pancreas to the right. Strip the splenic vessels from its posterior surface. Divide the bile duct near the superior part of the duodenum. Remove the duodenum and pancreas as one piece.
- Make 2 cuts on the posterior surface parallel to the superior and inferior margins of the body of the pancreas. Tease away the lobules of the gland between the cuts to expose the main pancreatic duct which is greyish-white.
- Note its tributaries (herringbone pattern). Now, expose the accessory pancreatic duct and its tributaries coming from the head of the pancreas. Follow both ducts to the duodenum. Cut open the duodenum vertically along its right wall and wash it.
- Identify the openings (at major and minor duodenal papilla) on the internal aspect of the posteromedial surface of the 2nd part of the duodenum.
Large Intestine
Large Intestine Extent
From caecum to anal canal
Large Intestine Parts and lengths
Vermiform appendix 2-20 cm, excluded from the total length

Total length- 155 cm
- Caecum – 5 cm
- Ascending colon – 15 cm
- Transverse colon – 45 cm
- Descending colon – 30 cm
- Sigmoid colon – 45 cm
- Rectum and anal canal – 15 cm
(Rectum- 12 cm.; Anal canal – 3cm)
Large Intestine Features
1. General Features
- Large lumen (wider)
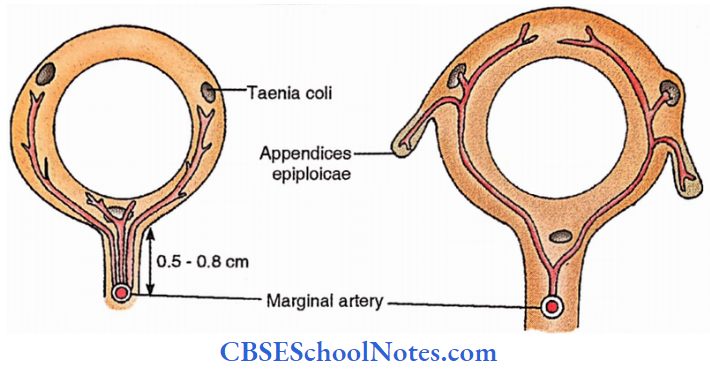
- Taenia (e) coli. These are three longitudinal muscular bands as follows,
- Taenia libra
- Taenia mesocolic
- Taenia omental
These bands are anterior, posteromedial and posterolateral respectively in the ascending and descending colons. Their positions change in the transverse and sigmoid colon.
- Sacculations (Haustrations) – These form a series of dilatations separated by constrictions through the colon.
- Appendices epiploicae – These are a large number of peritoneal sacs along taenia coli.
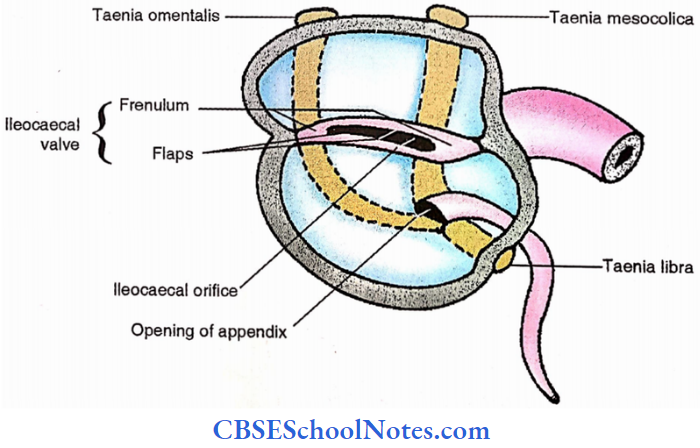
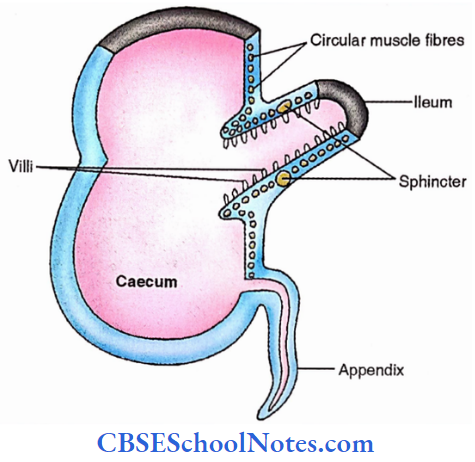
2. Specific features
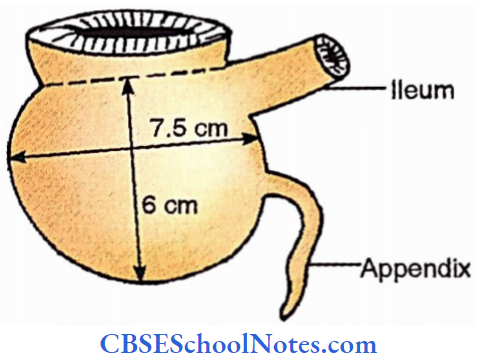
Caecum – 6 cm (Height) x 7.5 cm (Width)
Posteromedially is the opening of the ileum guarded by the ileocaecal valve. A little below the side opening is a rounded orifice of the vermiform appendix.
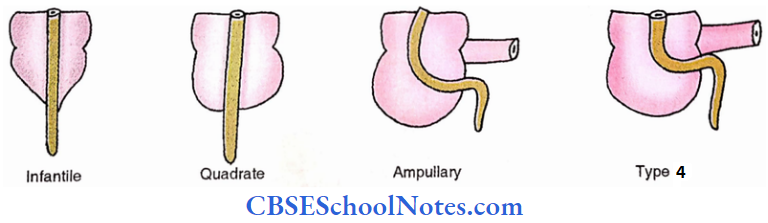
Types
- Infantile (Type 1) – 2%
- Quadrate (Type 2) – 3%
- Ampullary (Type 3) – 90%
- Type 4 – 4%
Vermiform appendix
Length – 2 – 20 cm
Shape – Worm-like
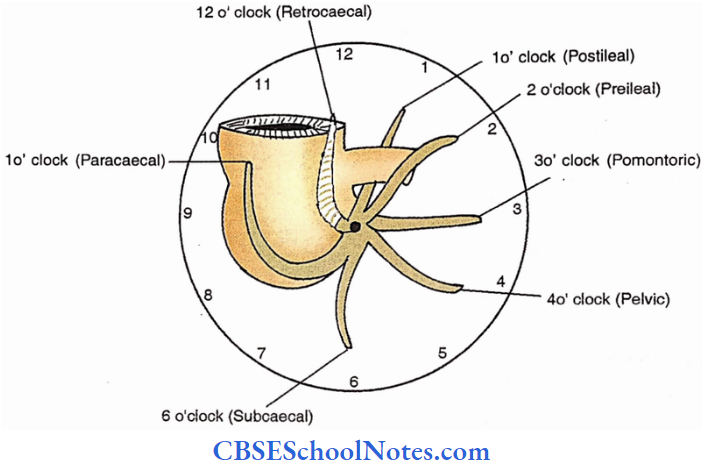
Locations of appendix
Retrocaecal – 12 o’clock – position – 65%
Pelvic – 4 o’clock – position – 31%
Subcaecal – 6 o’clock – position – 2%
Preileal – 2 o’clock – position – 1%
Postileal – 1 o’clock position – 0.4%
Paracaecal – 11 o’clock position
Promontoric – 3 o’clock position
Location of the base of the appendix
All three teenage coli converge to it (Surgical importance)
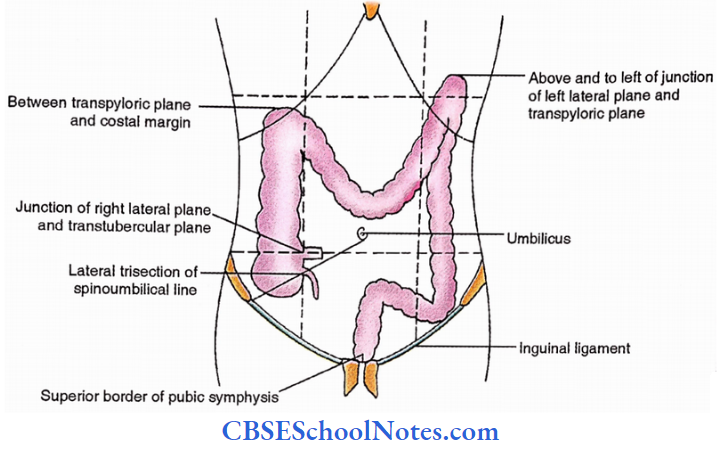
Surface marking of large intestine
- The base of the appendix – Lateral trisection of spinoumbilical line.
- Junction of ileum with large intestine (at caecocolic junction). Junction of right lateral with trans tubercular plane
- Caecum
- Right iliac region
- Ascending colon
- Right lumbar region
- Transverse colon
- Right lumbar region
- Umbilical region
- Left lumbar region
- Left hypochondriac region
- Descending colon
- Left hypochondriac region
- Left lumbar region
- Left iliac region
- Sigmoid colon
- Hypogastric region
Relations of large intestine
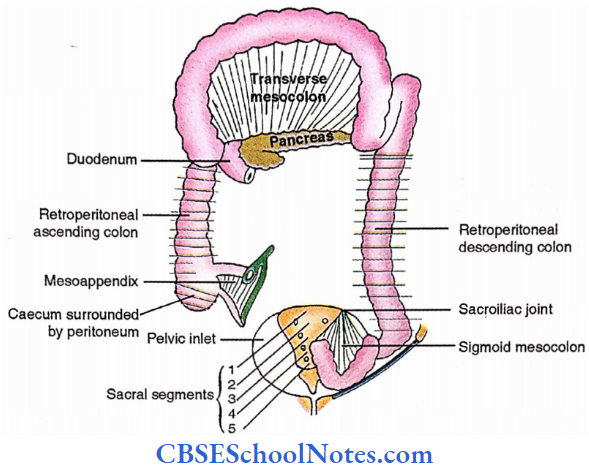
1. Peritoneal relations
- Appendix – It has a mesoappendix formed by a double layer of peritoneum derived from the left leaf of the mesentery.
- Caecum – It is covered by the peritoneum from all sides. A retrocaecal fossa is usually present.
- Ascending and descending colons
- Retroperitoneal – 52%
- Ascending mesocolon only (Double layer of peritoneum connecting ascending colon with
posterior wall) – 12% - Descending mesocolon only (Double layer of peritoneum connecting descending colon with
posterior wall). – 22% - Both ascending and descending mesocolon – 14%
- Transverse colon – It has a transverse mesocolon i.e. layer peritoneum connecting the transverse colon with posterior wall.
- Sigmoid colon – It has a sigmoid mesocolon, which is a double layer of peritoneum holding the sigmoid colon. Its attachment is inverted ‘V’ (A) shaped
- Upper limb attachment
- Along the external iliac artery (Pelvic brim)
- Halfway from the sacroiliac joint to the inguinal ligament
- 5 cm in length
- Lower limb attachment
- Front of the upper sacrum
- From left sacroiliac joint to 3rd sacral segment
- 5 cm in length
- Upper limb attachment
2. Adjacent relations
- Anterior relations
- Transverse colon
- Anterior abdominal wall.
- Rest of colon
- Anterior abdominal wall
- Coils of small intestine
- Greater omentum.
- Transverse colon
- Posterior relations
- Caecum
- 2 Muscles
- Psoas
- Iliacus
- 2 Nerves
- Lateral cutaneous nerve of thigh
- Femoral nerve
- 2 Vessels
- External iliac artery
- Gonadal vessels
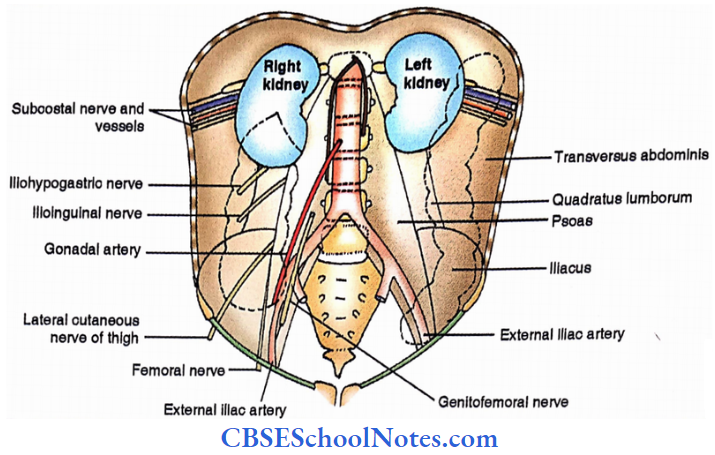
Ascending colon
- 4 Muscles
- Psoas
- Hiatus
- Quadratus lumborum
- Transversus abdominis
- 2 Nerves
- Iliohypogastric nerve
- Ilioinguinal nerve
- 1 Gland
- Right kidney
- Transverse colon (Near right colic flexure)
- Duodenum
- Head of the pancreas
- Descending colon – It is related to the following structure on the left side.
- Muscles – Psoas, Iliacus, Quadratus lumborum, Transversus abdominis
- Nerves – Subcostal, Iliohypogastric, Ilioinguinal, Genitofemoral, Lateral cutaneous nerve of the thigh, Femoral
- Vessels
- Subcostal
- External iliac
- Gonadal
Arteries of large intestine
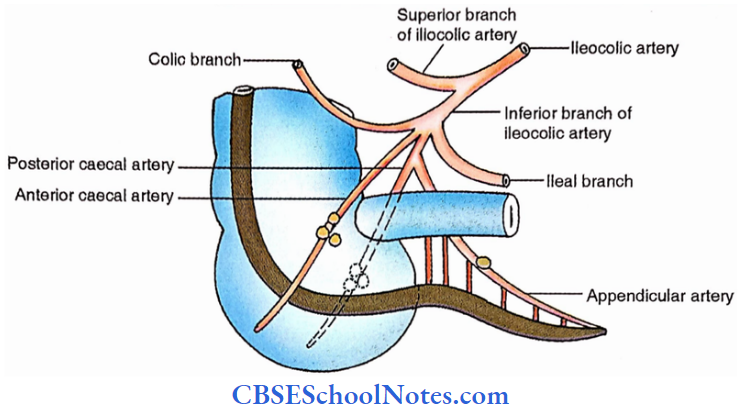
- Caecum and appendix
- Inferior branch of the iliocoic branch of the superior mesenteric artery.
- Named branches
- Anterior caecal artery. It descends in the form of caecum
- Posterior caecal artery. It descends behind the caecum.
- The appendicular artery arises from this branch.
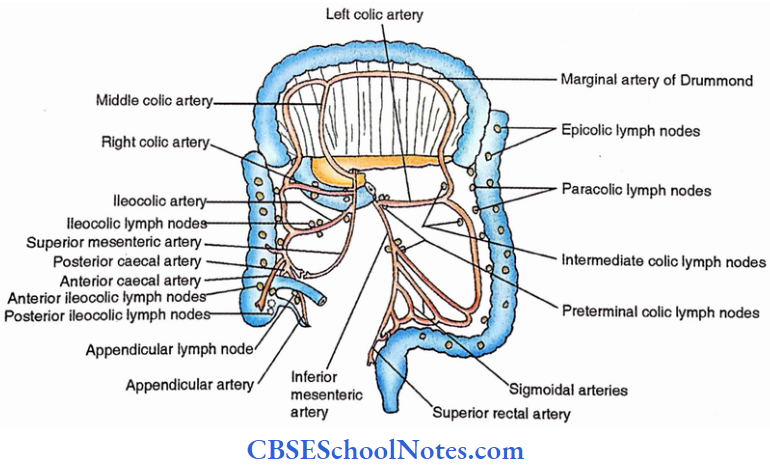
Colon– Marginal artery of Drummond
- Formed by colic branches of superior and inferior mesenteric arteries
- Extent- From the beginning of the ascending colon to the end of the sigmoid colon.
- Long and short branches appear from the marginal artery and supply wall of the colon including taeniae coli and appendices epiploicae.
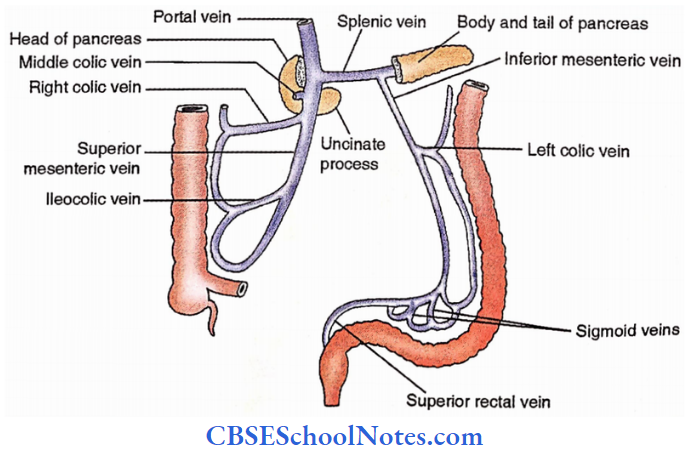
Veins of large intestine
- Superior mesenteric vein (mid gut)
- Inferior mesenteric vein (hindgut)- It drains into the splenic vein.
- Superior mesenteric and splenic veins unite to form a portal vein.
Lymphatics of the large intestine
- Caecum and appendix
- Anterior ileocolic lymph nodes
- Posterior ileocolic lymph nodes
- Appendicular lymph nodes
- (Efferents of the above lymph nodes drain into ileocolic lymph nodes → → Superior mesenteric lymph nodes)
- Colon — Colic lymph nodes
- Epicolic – over the colon
- Paracolic – adjacent to colon
- Intermediate colic
- Preterminal colic – at the origin of colic arteries
- (Efferents of the above lymph nodes drain into superior and inferior mesenteric lymph nodes)
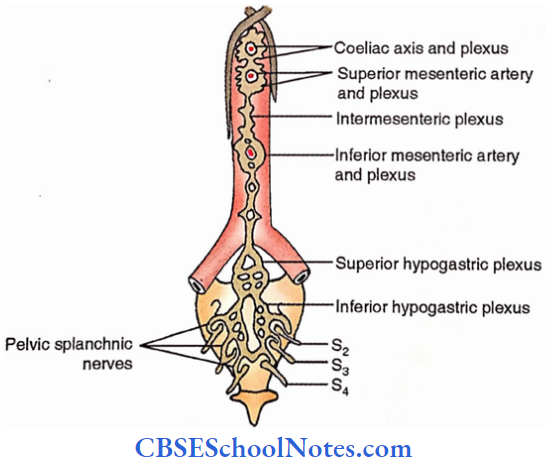
Nerves of the large intestine
- Up to junctions of right 2/3rd with left l/3rd of transverse colon, it is supplied by autonomic plexus about mid gut artery (superior mesenteric artery) called superior mesenteric plexus.
- This plexus receives sympathetic fibres from spinal segments T 10-11 and parasympathetic fibres from the vagus.
- The rest of the colon receives autonomic fibres from the inferior mesenteric plexus which accompanies the artery of the hindgut i.e. inferior mesenteric artery. It receives sympathetic fibres from spinal segments T 10-11 and parasympathetic fibres from the hypogastric plexus (S 2,3,4).
Dissection Steps Of Large Intestine
Study the large intestine in situ and note its cardinal features. Note the peritoneal covering of the large intestine. Clean and define the caecum and turn it upwards. Identify the appendix and note its position.
- Note the convergence of all taeniae to the base of the appendix. Note posterior relations of caecum. Cut the lateral wall of the caecum, wash and identify the ileocaecal orifice and orifice of the appendix.
- Divide the peritoneum along the lateral margin of the descending colon and turn the colon medially. Note the attachment of sigmoid mesocolon. Tie two ligatures at the junction of the descending colon and sigmoid colon.
- Divide the colon between these ligatures. Remove the large intestine and wash it. Take about a 6″ piece of the large intestine. Open it longitudinally and examine its interior.
Large Intestine Applied
- Appendix
- Appendicitis i.e. inflammation of the appendix.
- Perforation of the appendix. It is a complication of appendicitis.
- Referred pain from the appendix is felt at the umbilicus due to a common source (T10) of innervation
- Caecum and colon
- Cancer of the colon – Partial colectomy is preferred.
- Diverticulosis – Evagination of mucosa through the wall.
- Large bowel obstruction. Caecum is full of faeces. (In cases of small intestinal obstruction caecum is empty).
Portal Vein
Portal Vein Length – 8 cm
Portal Vein Commencement
- Between the neck of the pancreas and the inferior vena cava.
- Formed by the union of superior mesenteric and splenic veins
Portal Vein Course
Ascends behind the 1st part of the duodenum, in the free margin of the lesser omentum
Portal Vein Termination
At porta hepatis; it terminates by dividing into right and left branches.
Portal Vein Territory Of Drainage
- Alimentary canal from the lower end of the oesophagus to the upper anal canal
- Pancreas
- Spleen
- Gall bladder
- Bile duct
Portal Vein Tributaries
- Splenic vein
- Superior mesenteric vein
- Left gastric vein
- Right gastric vein
- Paraumbilical vein
- Cystic vein
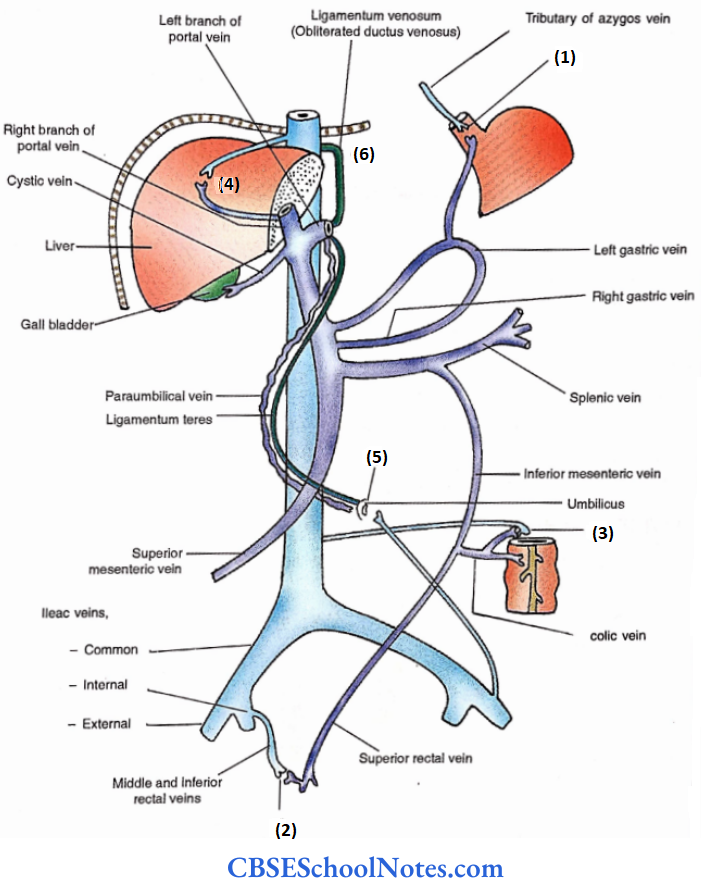
Portal Vein Applied
Obstruction of portal vein leads to,
- Splenomegaly (enlargement of spleen)
- Ascites (Collection of fluid in the peritoneal cavity)
- Varicose veins at the sites of portosystemic anastomoses, i.e.
- Lower 3rd of the oesophagus (Oesophageal varices)
- Middle anal canal (Haemorrhoid)
- Behind retroperitoneal viscera.
- Bare area of liver
- Umbilicus (Caput Medusae)
- Patent ductus venosus.
Dissection Steps Of Portal Vein
Lift the tail of the pancreas from the spleen and separate the body of the pancreas from the posterior abdominal wall. Identify the inferior mesenteric, splenic, superior mesenteric and portal veins over the posterior surface of the pancreas.
Clean and trace the splenic vein to the junction of the superior mesenteric vein behind the neck of the pancreas and note the beginning of the portal vein. Follow the inferior mesenteric vein and note its termination. Trace the various tributaries of the portal vein.
Liver
Liver Peculiarity
Largest gland of the body
Liver Weight
- Male – 1.4 – 1.8 kg.
- Female – 1.2 – 1.4 kg.
Liver Situation – Mainly – Right hypochondriac and epigastric regions
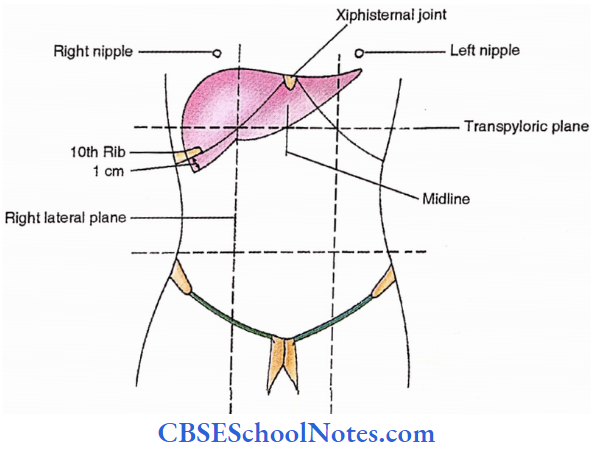
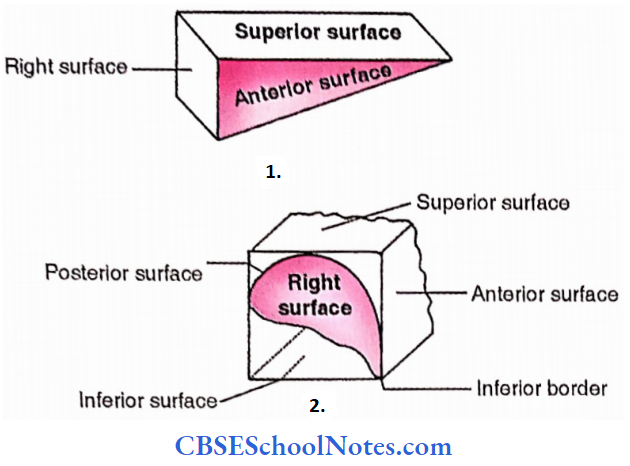
Liver Surfaces
- Superior
- Anterior
- Right
- Posterior
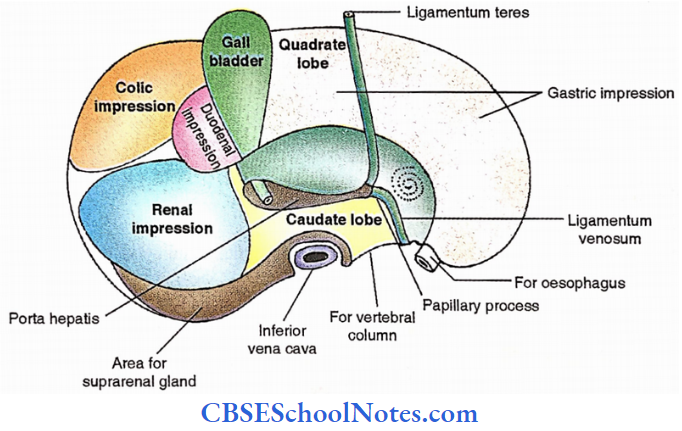
- Inferior (Visceral)
One border – Inferior
Liver Relations
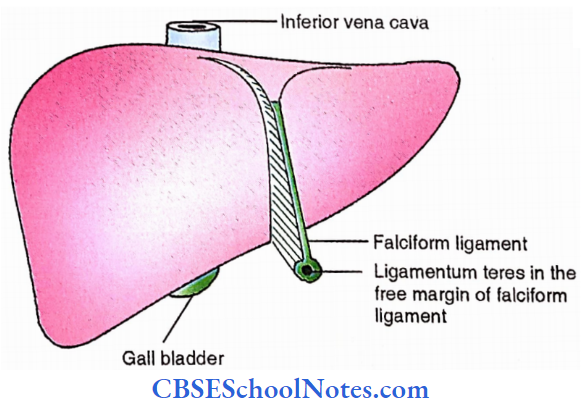
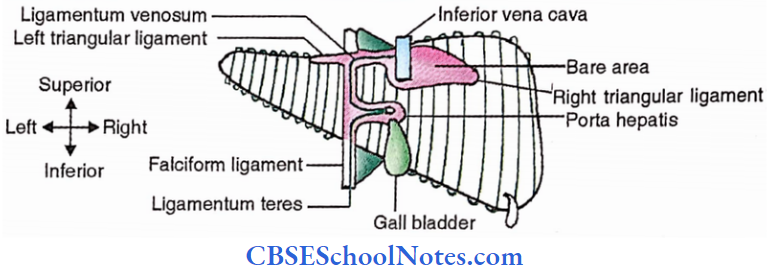
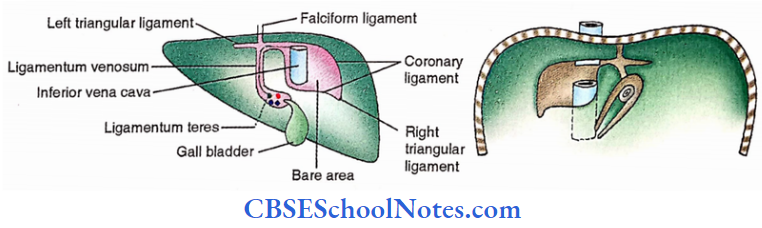
1. Peritoneal relations
- Anterior and superior – Falciform ligament extends from the liver to the anterior wall of the abdomen above the umbilicus
- Posterior and Inferior – Coronary ligaments – Its upper and lower layers bound the bare area of the liver superiorly and inferiorly respectively.
- Right triangular ligament. Formed by the union of two layers of the coronary ligament at the extreme right of the bare area.
- Left triangular ligament. It is located on the back of the left lobe of the liver and is an extension of the left leaf of the falciform ligament.
- Lesser omentum. Coronary and triangular ligaments connect the liver with the diaphragm while It extends between the liver and lesser curvature of the stomach.
2. Adjacent relations
- All surfaces (except visceral),
- Diaphragm – Separates liver from pleural and pericardial cavities as well as lungs and heart.
- Anterior abdominal wall- Related to the anterior surface.
- Right suprarenal gland- Related to bare area near inferior vena cava.
- Superior- Central concavity for heart and pericardium.
- Posterior- 3 Concavities – which are meant, from right to left,
- For inferior vena cava
- For vertebral column
- For oesophagus
- Visceral surface is related to the following,
- Stomach and lesser omentum
- Duodenum
- Right kidney
- Right colic flexure
- Gall bladder.
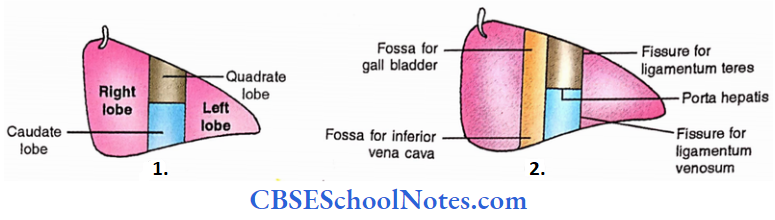
Liver Segmentation
The liver is divided into lobes, parts, segments and regions as mentioned below.
1. Right and left lobes
- Anatomical lobes – Here the criteria is attachment of falciform ligament and therefore caudate and quadrate lobes are parts of the right lobe.
- Physiological lobes – Here the criteria is the plane of inferior vena cava and gall bladder and therefore caudate and quadrate lobes are parts of the left lobe but the caudate process is excluded.

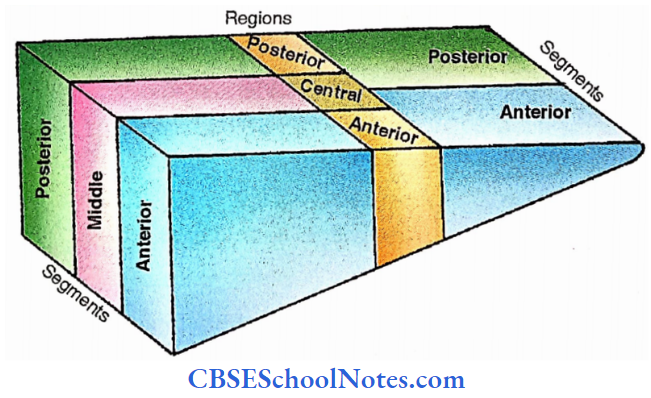
2. Segments, parts and regions
- 3 Segments in the right lobe – Anterior – intermediates (middle) and posterior 2 Parts in the left lobe – Medial and lateral.
- Subdivisions in the left lobe
- Medial part- Anterior region, central region and posterior region.
- Lateral part- Anterior segment, and posterior segment
- All subdivisions may be divided into upper and lower
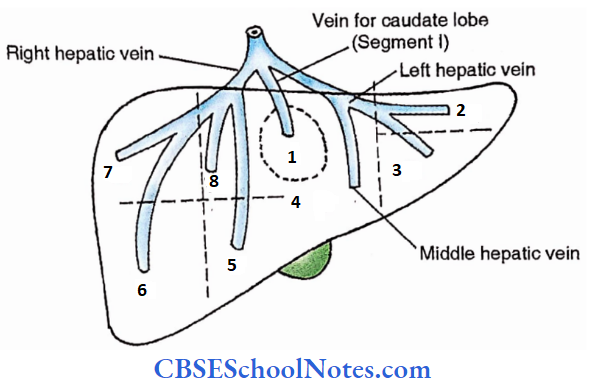
3. Based on drainage by hepatic veins, the liver is divided into 8 surgical segments i.e. from 1 to 8.
Liver Blood supply
20% – Hepatic artery
80% – Portal vein
Liver Venous drainage
2-3 Hepatic veins drain into the inferior vena cava.
Lymphatic drainage
1. Superficial lymphatics
- The left portion of the posterior surface
- The posterior portion of the inferior surface
- The middle portion of the superior surface
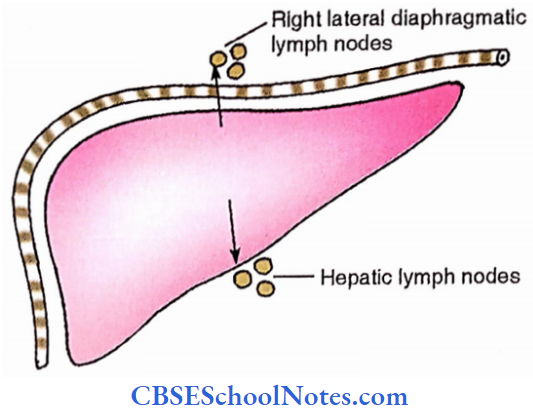
- From a, b, and c lymphatics drain into right lateral diaphragmatic and paracardiac lymph nodes, both located above the diaphragm.
- The right portion of the posterior surface is drained by coeliac lymph nodes about the origin of the coeliac artery.
- The rest of the liver is drained by hepatic lymph nodes located at porta hepatis.
2. Deep lymphatics
- Ascending- Right lateral diaphragmatic lymph nodes (Near the entrance of inferior vena cava)
- Descending- Hepatic lymph nodes
Nerves
- Parasympathetic – Vagus – Hepatic branch of the anterior vagal trunk and coeliac branch of the posterior vagal trunk.
- Sympathetic – T7 -9, via greater splanchnic nerve and coeliac plexus.
- Nerves follow the hepatic artery to reach the liver.
Liver Applied
- Hepatitis (inflammation of the liver)
- Amoebic hepatitis
- Infective hepatitis (Viral)
- Icterus / Jaundice – Yellowish pigmentation of skin due to a high level of bilirubin in the blood.
- Hepatomegaly (Enlargement of the liver) Massive hepatomegaly is observed in cancer and hydatid cysts.
- Cirrhosis – It leads to portal obstruction
Dissection Steps Of Liver And Gall Bladder
Identify the liver and gall bladder in situ. Pull the liver down and cut the layers of the left triangular and coronary ligaments. Identify and feel inferior vena cava and cut it above and below the liver.
Remove the liver along with the segment of the inferior vena cava. Study the liver for its different lobes, fissures, grooves, ligaments, and porta hepatis. Identify the various parts of the gall bladder and extrahepatic biliary apparatus.
Extrahepatic Biliary Apparatus
Gall Bladder
- Pear shaped
- Measurement and capacity.
- The gall bladder is 3 cm in width and 10 cm in length. Its capacity is approximately 30-50 ml.
- 4 parts
- Fundus – Portion of gall bladder beyond the inferior border of the liver.
- Body
- Infundibulum (Hartmann’s pouch) – It is bending in the upper part of the gall bladder which connects the body with the neck.
- Neck – It is a narrow uppermost part of the gall bladder which turns to the left to continue as a cystic duct.

Gall Bladder Relations
- Peritoneal
- In the majority of cases, the anterior surface of the body is in contact with the inferior surface of the liver while the rest of it is covered with the peritoneum. Rarely the gall bladder has mesentery.
- Adjacent relations
- Anterior
- Liver,
- Anterior abdominal wall,
- Posterior
- Duodenum
- Transverse colon
- Anterior
- Artery– Cystic artery from the right hepatic artery
- Veins– Cystic vein draining into right branch of portal vein
- Lymphatics
- Cystic lymph nodes —» Hepatic lymph nodes —> Coeliac lymph nodes
- Nerves
- Coeliac plexus- Sympathetic and parasympathetic
- Phrenic nerve (via communicating branch with coeliac plexus) – This explains the referred pain to the right shoulder.

Function – To store and concentrate the bile.
Applied
- Inflammation of the gall bladder is called cholecystitis. It can be acute or chronic
- Stone in the gall bladder is called cholelithiasis
- + ve Murphy’s sign —» Catch in breath on palpation if the organ is inflamed.
Cystic duct
- 4 cm in length
- Connects neck of gall bladder with common hepatic duct
Right and left hepatic ducts
Appear from porta hepatis
Common hepatic duct
- 4 cm in length.
- The common hepatic duct unites with the cystic duct to form a common bile duct.
Common bile duct
- 8 cm in length.
- 3 parts
- 1st part – Supraduodenal ( In the free margin of lesser omentum)
- 2nd part – Retroduodenal ( Behind duodenum)
- 3rd part – Infraduodenal (Behind the head of the pancreas)
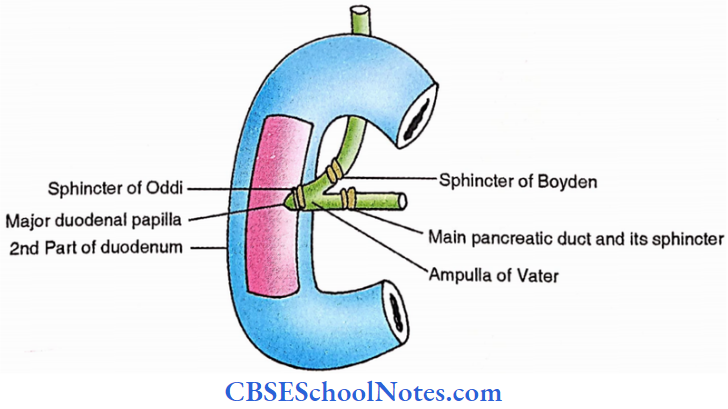
The Sphincter of Boyden guards the terminal part of the common bile duct.
- It terminates in the substance of the head of the pancreas by joining the main pancreatic duct to form the ampulla of Vater. Ampulla is guarded by the sphincter of Oddi and itself opens on the summit of the major duodenal papilla in the posteromedial wall of 2nd part of the duodenum.
- Artery
- The upper part is supplied by the cystic artery
- The lower part is supplied posterior branch of the superior pancreaticoduodenal artery.
The Diaphragm
The Diaphragm Definition
Musculotendinous partition between thorax and abdomen
The Diaphragm Attachments
Origin (Peripheral attachments)
Sternal – Xiphoid – 2 slips
Costal – Lower 6 costal cartilages
- Vertebral – Crura – Right crus – It is attached to the upper three lumbar vertebral bodies
- Left crus – It is attached to the upper two lumbar vertebral bodies
- Arcuate ligaments – Median – It connects its two cura in front of the 12th thoracic vertebral body.
- Medial – It connects the 2nd lumbar vertebral body with the 1st lumbar transverse process.
- Lateral – It connects 1st lumbar transverse process with the 12th rib
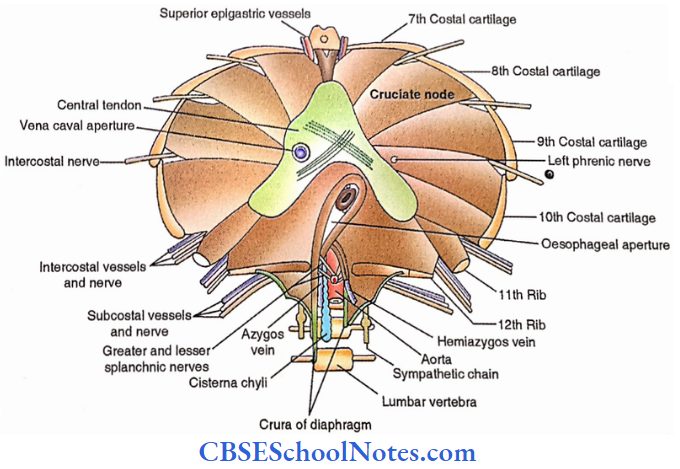
- Insertion (Central tendon) – Trefoil / Trifoliate in nature. It has the following parts
- Central part – Cruciate node-It is formed due to crossing connective tissue fibres
- Right leaf
- Anterior leaf
- Left Leaf
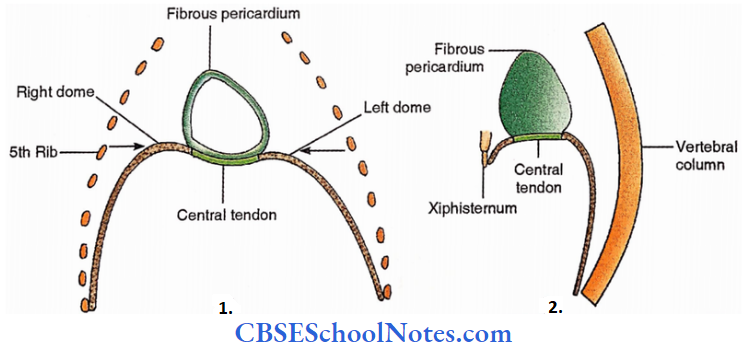
The Diaphragm Shape
From front – Two domes (Right and Left) and a concavity
- Both the domes reach the level of the 5th rib (the right dome is higher) and correspond with the
concavities of the base of the lungs. - The middle part fuses with fibrous pericardium.
From side – Inverted T-shaped.
The Diaphram Functions
- Respiration
- Abdominal strainings
- Defaecation
- Micturition
- Parturition
- Weight lifting
The Diaphragm Openings
- Large openings
- Aortic aperture – It is present at the level of the 12th thoracic vertebral body.
- Structures passing through it are,
- Aorta
- Thoracic duct
- Vena azygos
- Lymphatics
- Oesophageal aperture – It is located at the level of the 10th thoracic vertebra and allows the following structures to pass through it,
- Oesophagus
- Anterior and posterior vagal trunks
- Oesophageal vessels from/to left gastric vessels
- Venacaval aperture – It is located at the level of the 8th thoracic vertebra. Following structures pass through it,
- Inferior vena cava
- Right phrenic nerve
- Lymphatics
Small Passages – for,
- Superior epigastric vessels.
- Lower 5 (7th to 11th) intercostal nerves, 10th and 11th posterior intercostal vessels.
- Subcostal nerve and vessels.- These pass under lateral arcuate ligaments.
- Sympathetic chains – These pass under medial arcuate ligaments.
- Greater and lesser splanchnic nerves- These pierce the crura of the diaphragm.
- Left phrenic nerve.
- Hemiazygos vein.
Dissection Steps For Diaphragm
Strip the parietal peritoneum from the undersurface of the diaphragm and identify its various parts and openings. Clean and define the attachments of crura and arcuate ligaments.
- Clean and define the major openings (caval, oesophageal and aortic) in the diaphragm with structures passing through them. Work out their levels about the thoracic spines.
- Explore various other minor openings (for superior epigastric vessels, subcostal vessels and nerves, sympathetic trunk and splanchnic nerves) and structures passing through them.
- Openings for the superior epigastric vessels, lower 5 intercostal nerves and hemiazygos vein may also be located.
The Diaphragm Nerves
- Motor – Phrenic nerve – (C3, 4, 5)
- Sensory
- Central part -Phrenic nerve.
- Peripheral part – Lower intercostal nerves (T7-11)
Nerves Arteries
- Inferior phrenic arteries from the abdominal aorta.
- A musculophrenic artery from the internal thoracic artery.
- A pericardiacophrenic artery from the internal thoracic artery.
Nerves Applied
Hiatus hernia – Abdominal contents protrude into the thoracic cavity through openings in the diaphragm.
- Sliding / Oesophagogastric – 85%
- Rolling / Paraoesophageal – 10%
- Mixed or Transitional -5%
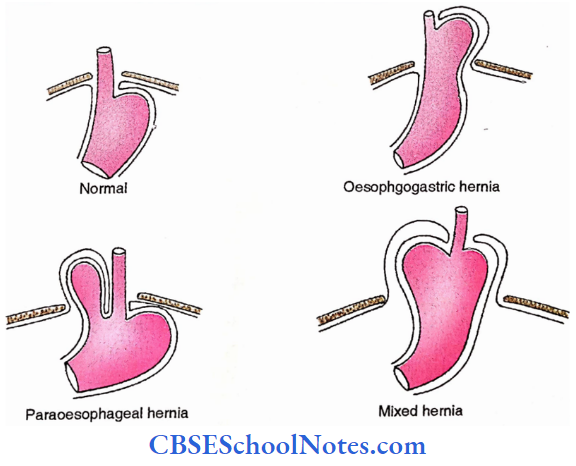
Posterior Wall Of Abdomen
Muscles Of The Posterior Abdominal Wall
1. Quadratus lumborum
Origin – Iliac crest and lower lumbar transverse processes
Insertion – 12th Rib and upper lumbar transverse processes.
Nerve – Directly from lumbar plexus (L 1-4)
Actions – Lateral flexion of spine Respiration
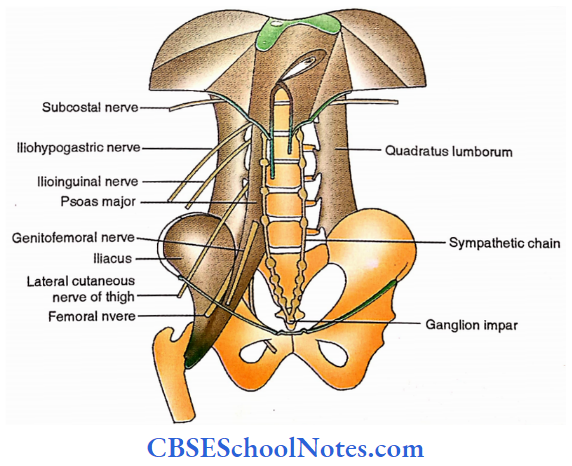
Thoracic-Iumbar fascia– It has the following three layers
- Anterior layer – On the anterior surface of quadratus lumboram.
- Middle layer – On the posterior surface of quadratus lumborum.
- Posterior layer – Over erector spinae.
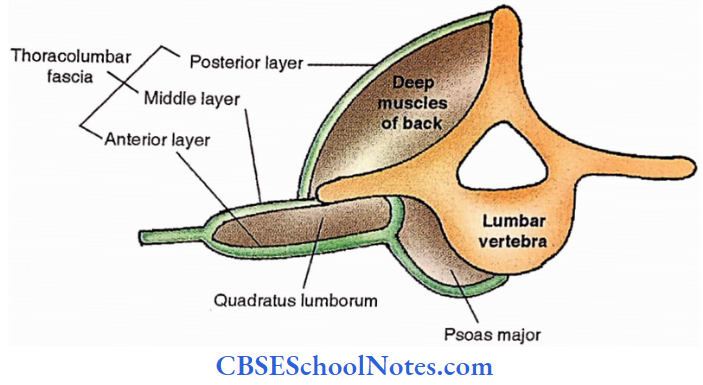
2. Psoas major
- Origin – Bodies and transverse processes of lumbar vertebrae.
- Insertion – Lesser trochanter of femur.
- Nerve – Directly from lumbar plexus ( LI-4.)
- Actions – Lateral flexion of the spine.
- Flexion and medial rotation of the thigh.
3. lilacs
- Origin – Iliac fossa.
- Insertion – Lesser trochanter.
- Nerve – Femoral nerve.
- Actions – Flexion and medial rotation of the thigh.
Nerve Supply Of Posterior Abdominal Wall
- Subcostal nerve
- Runs laterally under lateral arcuate ligaments.
- Branches of lumbar plexus ( L1-4)
- Directly from roots of lumbar plexus for quadratus lumborum and psoas
- Iliohypogastric nerve (LI) – Runs laterally over the quadratus lumborum muscle
- Ilioinguinal nerve (LI)- Runs laterally just below the iliohypogastric nerve.
- Genitofemoral nerve (LI,2). Descends in front of the Psoas major muscle.
- The lateral cutaneous nerve of the thigh (L2,3). Extends towards the anterior superior iliac spine
- Femoral nerve (L2,3,4). Descends in the groove between the psoas and iliacus.
- Obturator nerve – (L2,3,4). Descends along the medial border of psoas.
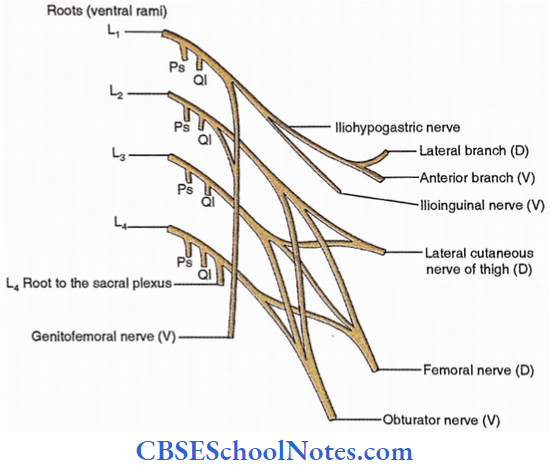
3. Sympathetic chain
- Ganglia
- 4 lumbar ganglia lie in the groove between lumbar vertebral bodies and psoas
- 4 sacral ganglia lie over sacral feramina or medial to them,
- 1 ganglion impair is located over the coccyx
- Grey and white rami communicantes (latter from upper two lumbar ganglia only)
- Lumbar splanchnic nerves from the lumbar ganglia join the hypogastric plexus.
4. Autonomic plexuses
- Coeliac plexus (About coeliac artery from the aorta)
- The right and left coeliac ganglia in the coeliac plexus on each side of the coeliac artery receive greater (T5-9) and lesser (T10-11) splanchnic nerves.
- Communicating nerve from phrenic nerve joins coeliac plexus
- Coeliac branch of posterior vagal trunk also joins oeliac plexus
- Phrenic plexus – Follows inferior phrenic artery.
- Left gastric plexus -Follows left gastric artery.
- Splenic plexus – Follows splenic artery.
- Hepatic plexus – Follows hepatic artery.
- Renal plexus (Along renal artery) – It has a renal ganglion which receives fibres from the least splanchnic nerve (from the last thoracic ganglion)
- Superior mesenteric plexus- Follows superior mesenteric artery.
- Abdominal aortic (Intermesenteric) plexus- over the abdominal aorta between origins of
superior and inferior mesenteric arteries. - Inferior mesenteric plexus- Follows inferior mesenteric artery.
- Superior hypogastric plexus- Concerning sacral promontory.
- Inferior hypogastric plexus (pelvic plexus)- Behind the rectum, in front of the sacrum.
Dissection Steps Of Posterior Abdominal Wall
Clean the posterior abdominal wall and denude it from all fascia and identify the inferior vena cava and its tributaries, abdominal aorta and its branches.
- Clean the muscles of the posterior abdominal wall and identify the quadratus lumborum, and psoas major and minor.
- Clean and trace the subcostal, iliohypogastric, ilioinguinal, femoral and obturator as well as lateral cutaneous nerves on the posterior abdominal wall.
Abdominal Aorta
Extent -From aortic hiatus (T12) to L4 vertebra
Abdominal Aorta Branches
1. Ventral (unpaired) branches.
- Coeliac artery. Appears at T12 vertebra.
- Superior mesenteric artery. Appears at Lj vertebra.
- Inferior mesenteric artery. Appears at L3 vertebra.
2. Lateral (paired) branches. (Actually, these are anterolateral)
- Inferior phrenic artery- To the inferior surface of the diaphragm.
- Middle suprarenal artery- To suprarenal gland.
- Renal artery- To kidney.
- Gonadal (Testicular or Ovarian) artery- To gonad.
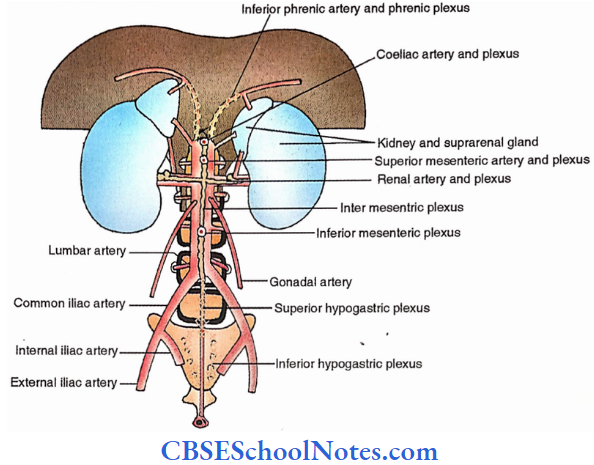
3. Dorsal branches
- Lumbar arteries (posterolateral) – There are four paired lumbar arteries opposite the upper four lumbar vertebrae
- Median sacral artery (posterior) – Arises from the bifurcation of the aorta and descends in front of the sacrum in the middling.
4. Terminal branches
The aorta terminates at the level of the 4th lumbar vertebra into the right and left common iliac arteries These terminate at the level of the sacroiliac joint into external and internal iliac arteries.
Inferior Vena Cava
Inferior Vena Cava Extent – From L5 vertebra to T8 vertebra (Venacaval orifice)
Inferior Vena CavaTributaries
- Common iliac veins – These unite to form the inferior vena cava at the level of the 5th lumbar vertebra.
- Lumbar veins, from the abdominal wall. These accompany the lumbar arteries.
- Right gonadal (Testicular or ovarian) veins, from right gonad (testis in male and ovary in
female). - Renal veins, from kidneys.
- Right suprarenal vein, from right suprarenal gland.
- Right inferior phrenic vein, from under the surface of the right portion of the diaphragm.
- Hepatic veins- 3, from liver.
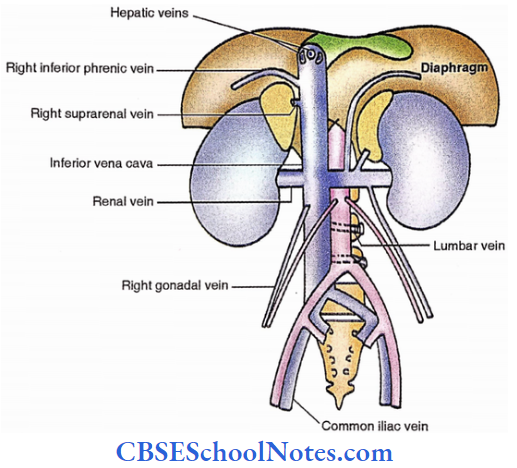
Lymph Nodes
These are named after their relations with arteries.
- Internal iliac lymph nodes.
- External iliac lymph nodes.
- Common iliac lymph nodes.
- Lumbar lymph nodes (Along the aorta and inferior vena cava.)
- Preaortic lymph nodes
- Coeliac lymph nodes (With the origin of a coeliac artery).
- Superior mesenteric lymph nodes (About the origin of the superior mesenteric artery)
- Inferior mesenteric lymph nodes (About the origin of the inferior mesenteric artery)
- Efferents from the above lymph nodes form a single intestinal trunk which drains into cistema chyli in its middle.
- Lateral aortic (Para-aortic) lymph nodes. Their efferents unite to form right and left lumbar trunks which join the lower part of cisterna chyli.
- Retroaortic lymph nodes (Lying behind the aorta).
- Preaortic lymph nodes

Suprarenal Glands
Suprarenal Glands Location: Near the kidney’s upper pole.
Suprarenal Glands Weight: 5 grams.
Suprarenal Glands Measurements: Height- 5 cm, Width- 3 cm, Thickness- 1 cm.
Suprarenal Glands Coverings: Perinephric fat and renal fascia.

Differences between two glands
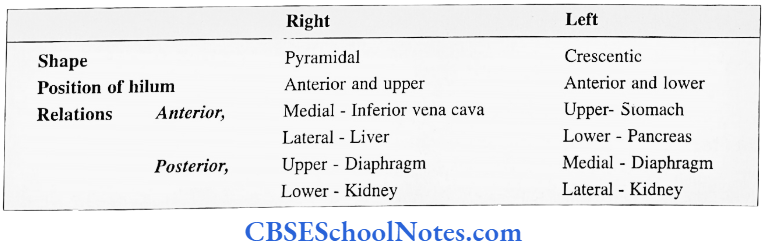
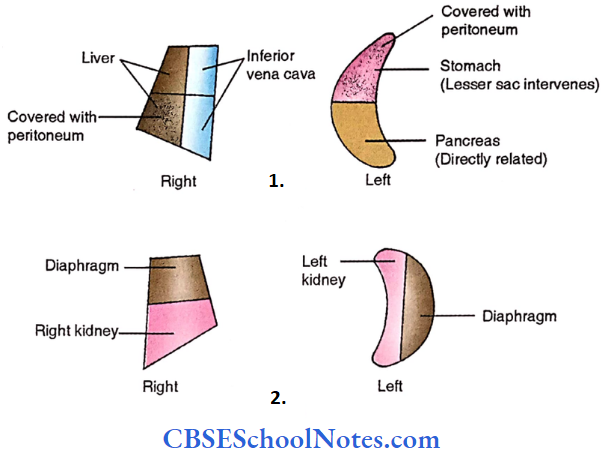
Arteries
- Three in number,
- Superior suprarenal artery – from the inferior phrenic artery.
- Middle suprarenal artery – from aorta
- Inferior suprarenal artery – from renal artery
- All three arteries enter the gland away from the hilum.
Veins – One in number. It appears from the hilum and drains on the right side into the inferior vena cava and on the left side into the left renal vein.
Lymphatics – Drain into lateral aortic lymph nodes.
Nerves – Preganglionic sympathetic fibres are derived from coeliac plexus (TIO- LI)
Suprarenal Glands Applied
- Cortex
- Decreased secretion → Addison’s disease
- Increase secretion —> Cushing’s syndrome – It causes masculinization in females and feminization in males.
- Medulla – Phaeochromocytoma – It is a benign tumour leading to an increase in its secretion followed by hypertension.
Kidneys
Kidneys Weight: 135 — 150 grams, (less in females)
Kidneys Measurements: Height-11 cm (>4″), Width-6cm (>2″) Thickness-3cm (>1″).
Kidneys Surface projection
- Hilum- It lies in a transpyloric plane about 5 cm from the midline.
- Anterior —> This plane passes through the tips of the 11th costal cartilage.
- Posterior → This plane passes through the spine of 1st lumbar vertebra
(Note: Right hilum is located a little below and left, a little above the plane)
Upper pole – 2.5 cm from midline.
Lower pole – 7.5 cm from midline.
Size – 4.5 x 11 cm
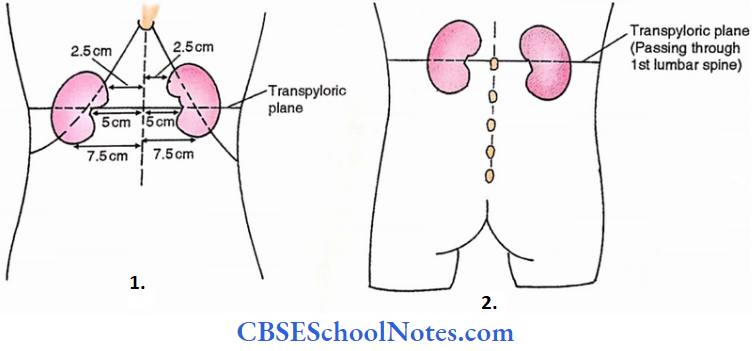
Hilum and renal sinus: Hilum is a concavity along the medial border of the kidney to receive renal vessels. Deep to the hilum is a space for the renal pelvis, major and minor calyces, renal vessels and some connective tissue. This space is called the renal sinus.
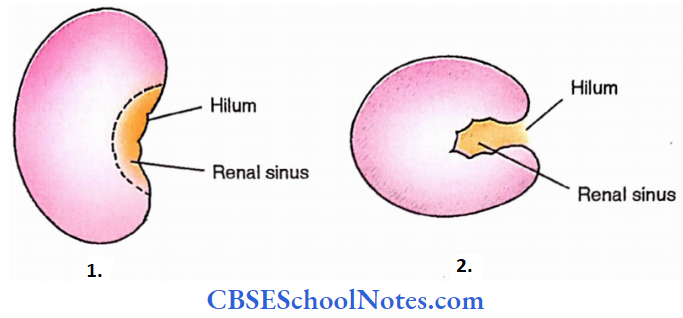
Coverings of kidney

Capsule – It is immediate connective tissue covering.
Perinephric (perirenal)fat – It is a fatty layer next to the capsule.
Renal fascia – It is a well-defined membrane over perinephric fat. This fascia along with perinephric fat also encloses the suprarenal gland.
The fascia on the front and back of the kidney, meet laterally but continue downwards and medially without meeting with each other. Medially they fuse with adventitia of great vessels i.e. renal vessels, inferior vena cava and abdominal aorta.
Paranephric (pararenal) body – This is fatty aggregation in the paravertebral gutter behind the kidney.
Kidneys Relations
- Posterior relations are almost symmetrical on two sides.
- 4 muscles
- Quadratus lumborum
- Diaphragm
- Psoas major
- Transversus abdominis
- Subcostal nerve and vessels
- Medial and lateral arcuate ligaments
- Hiohypastric and ilioinguinal nerves
- Ribs- 12th (on both sides) and 11th (on left side only)
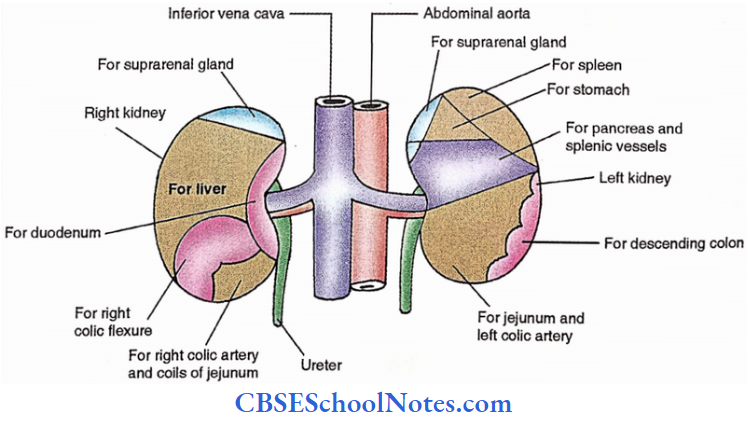
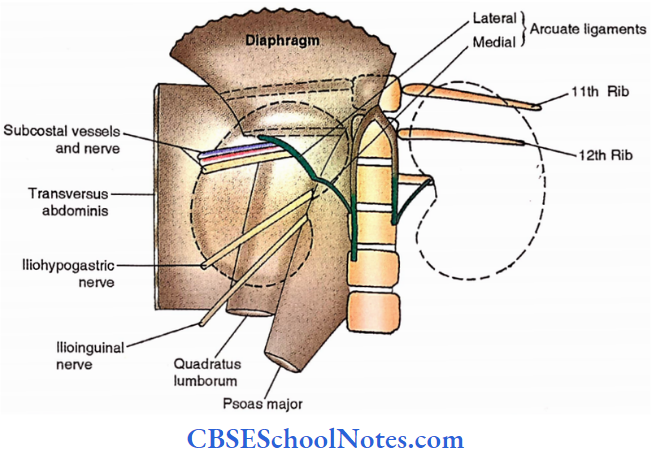
Anterior relations are different on two sides
- Right kidney
- Right suprarenal gland
- Duodenum
- Liver
- Right colic flexure
- Right colic artery
- Small intestine (Coils of jejunum)
- Left kidney
- Left suprarenal gland
- Spleen
- Stomach
- Pancreas
- Jejunum
- Descending colon
Kidney Arteries
- Renal artery – It divides into anterior and posterior divisions. The former is further divided into four branches.
- Vascular segmentation of kidney – Based on arterial supply, the kidney is divided into 5 segments:
- Apical segment
- Superior segment
- Middle segment
- Inferior segment
- Upper 4 segments are supplied by 4 branches of anterior division.
- Posterior segment- Supplied by posterior division.
- Bloodless line of Brodel (1901) – It is a vertical line along the lateral border of the kidney. An incision along this line results in relatively less bleeding.

- Arteries Of Kidney
- Lateral View Of Right Kidney
- Medial View Of Left Kidney
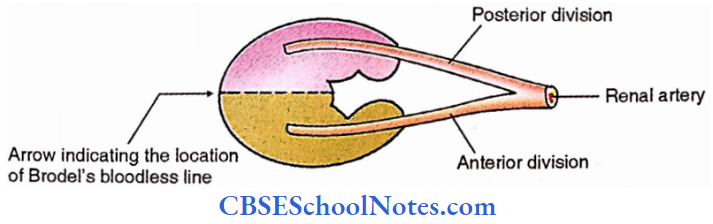
Kidney Vein
Renal vein
Kidney Lymphatics
Drain into para-aortic lymph nodes.
Kidney Nerves
Sympathetic (T12-L1)
Preganglionic fibres are derived from least splanchnic and lumbar splanchnic nerves which relay into renal ganglion. Postganglionic fibres further run a course in the renal plexus before supplying the kidney.
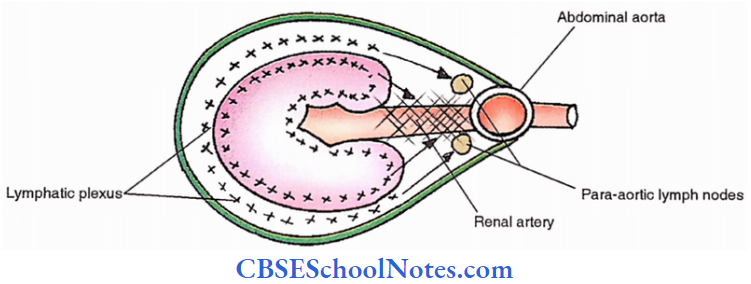
Dissection Steps Of Kidneys And Suprarenal Glands
Remove fat and fascia from the anterior surface of the kidneys and suprarenal glands. Indentify kidney and suprarenal in situ, and renal vessels. Identify the opening of the suprarenal vein, gonadal vein and renal vein on the left side.
- Clean and trace the ureters. Note their relations at the hilum. Mobilise both the kidneys and turn them medially. Separate suprarenals from the renal fascia and note their relations. Remove suprarenals and note the differences in their shape.
- Cut the ureters at the lower poles of the kidneys and the renal vessels 2 cm from the hilum and remove them. Study the posterior relations.
- Cut one kidney along its lateral border into two halves (anterior and posterior) and study the cut sections for the cortex, medulla, pyramid, calyces and pelvis of the ureter.
Kidneys Applied
- Congenital anomalies,
- Congenital polycystic kidney
- Horseshoe kidney
- Pelvic kidney
- Acquired – Renal stones.
- IVP – Intravenous pyelography. Introducing intravenous radio-opaque fluid and visualising the kidney, ureter and urinary bladder in the radiograph.

Ureters
Length: 30 cm
Diameter: 3 mm
Commencement: Continuation of renal pelvis.
Termination: Ends by entering the base of the urinary bladder.
Two parts
- Abdominal part – 15cm
- Pelvic part – 15 cm
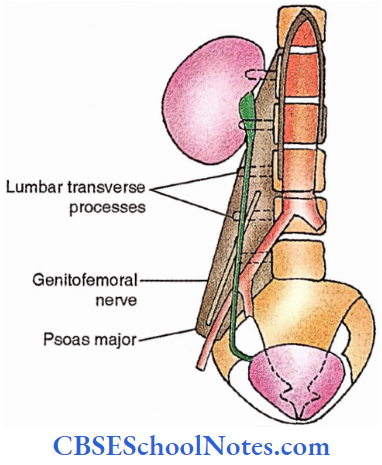
Ureters Relations
The posterior relation is symmetrical on two sides, i.e.,
- Psoas,
- Tips of lower 4 lumbar transverse processes.
- Genitofemoral nerve
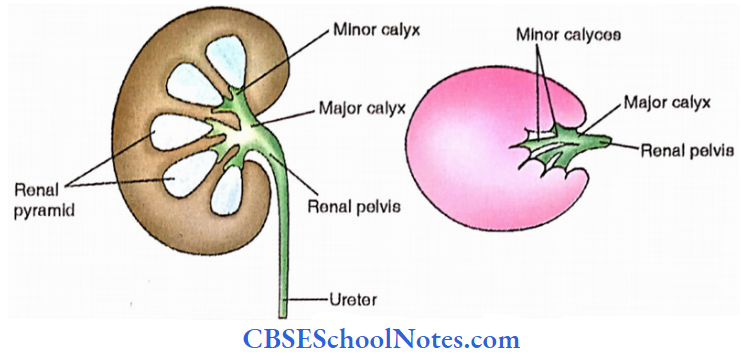
Anterior relations arc differently on two sides, as given below,
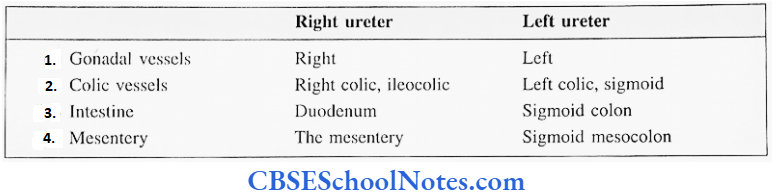
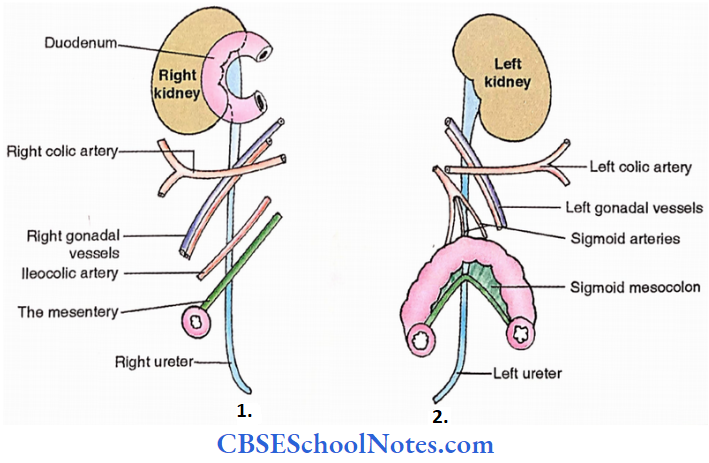
Surface projection (on the anterior abdominal wall)
Hilum Of kidney to public tubercle
Ureters Constructions
- At Commencement- At the tip of the transverse process of the second lumbar vertebra.
- At Middle- At the pelvic brim over the sacroiliac joint
- At the Lower end Slight medial to the ischial spine
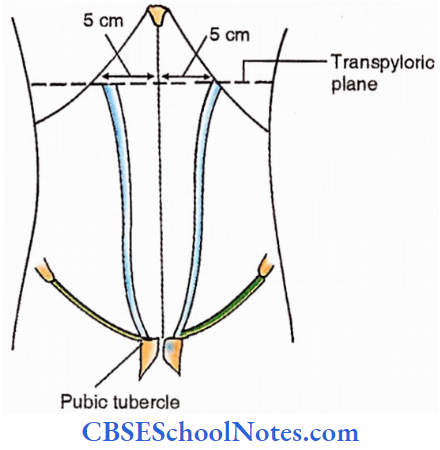
Ureters Arteries
Upper abdominal part
It is supplied by branches from the renal artery, abdominal aorta and gonadal artery.
Lower abdominal part
It is supplied by branches from the common iliac artery.
Pelvic part
It is supplied by branches from vesical arteries, and uterine arteries (in females).
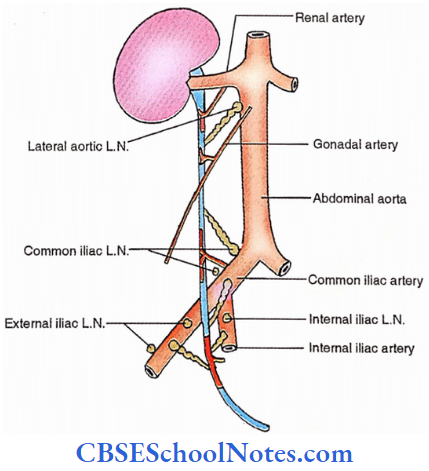
Ureters Lymphatics
- Upper abdominal part – Lymphatics drain into lateral aortic lymph nodes.
- Lower abdominal part – Lymphatics drain into common iliac lymph nodes.
- Pelvic part – Lymphatics drain into common iliac lymph nodes, external iliac lymph nodes and internal iliac lymph nodes.
Nerves are derived from the following autonomic plexuses
- Renal plexus.
- Aortic plexus.
- Superior hypogastric plexus.
- Inferior hypogastric plexus.
Sympathetic – T10 — LI
Parasympathetic – S2,3,4
Ureters Applied
- Renal or ureteric colic – Pain is referred to the testis (T10 segment) or medial side of the thigh (LI segment).
- Obstruction of the ureter may result in hydronephrosis- dilatation of calyces.
- Pyelography. In this procedure kidney, ureter and urinary bladder are visualized by using radioopaque fluid. The drug can be introduced by intravenous injection (descending pyelography) or by catheter into the ureter (ascending pyelography).