
- Ascending and Descending Tracts Of The Spinal Cord
- Ascending Descending Tracts Of The Spinal Cord Notes
- Auditory And Vestibular Systems Notes
- Autonomic Nervous System Functions Notes
- Basal Nuclei Anatomy – Functions, Parts Notes
- Blood Supply Of The Brain And Spinal Cord Notes
- Brain Ventricles Anatomy Notes
- Brainsteam Pons Anatomy Notes
- Brainstem Medulla Multiple Choice Questions
- Brainstem Midbrain Notes
- Brainstem Pons Multiple Choice Questions
- Central Nervous System And Peripheral Nervous System Notes
- Cerebellum Anatomy Notes
- Cerebral Hemispheres Lobes Notes
- Cranial Nerves Nuclei Anatomy Notes
- Functional Cerebral Areas Of Cerebral Cortex Notes
- Functions Of Reticular Formation Notes
- Limbic System – Components, Functions Notes
- Medulla Oblongata Anatomy Notes
- Meninges And Cerebrospinal Fluid Notes
- Nervous System – Functions and Classifications Notes
- Nervous Tissue Types And Structure Notes
- Neuroanatomy Notes
- Neuroanatomy Visual System Notes
- Olfactory Anatomy Notes
- Spinal Cord – Anatomy, Structure, Function, & Diagram
- Subthalamus And Hypothalamus Anatomy Notes
- Thalamus, Metathalamus And Epithalamus Notes
- White Matter Of Cerebrum Notes
Neuroanatomy
Ascending and Descending Tracts Of The Spinal Cord
Ascending Descending Tracts Of The Spinal Cord Multiple Choice Questions
Question 1. The following statements regarding sensory pathways are true except
- Ascending spinal tracts are sensory
- Sensory pathways usually consist of two sensory neurons
- Some somatic impulses do not reach the level of consciousness
- The cell body of most of the first-order sensory neurons is located outside the CNS
- The cell bodies of the mesencephalic nucleus lie within the CNS though it contains first-order sensory neurons
Answer: 2. Sensory pathways usually consist of two sensory neurons
Read and Learn More Neuroanatomy
Question 2. Which of the following statements is true?
- The first-order sensory neuron of the sensory pathway lies in the dorsal root ganglion of the spinal nerve
- The second-order sensory neuron lies in the dorsal grey horn of the spinal cord.
- Third-order sensory neurons are located in the thalamus
- Axonal processes of second-order sensory neurons, as a general rule, cross to the opposite side.
- All ofthe above
Answer: 3. Axonal processes of second-order sensory neurons, as a general rule, cross to the opposite side.
Spinal Tracts
Question 3. Fasciculi gracilis and cuneatus are concerned with except
- Conscious proprioception
- Fine touch
- Vibration and deep pressure
- Two-point discrimination
- Crude touch
Answer: 5. Crude touch
Question 4. Which of the following statements about the ascending tracts of dorsal white columns is false?
- Fasciculus cuneatus is present medial to fasciculus gracilis in the dorsal white column
- Fibers of cuneate and gracile fasciculi terminate on the cell bodies of cuneate and gracile nuclei, respectively.
- Second-order fibers decussate in the midline to form great sensory decussation.
- After decussation, fibers run upwards to form the medial lemniscus.
Answer: 1. Fasciculus cuneatus is present medial to fasciculus gracilis in the dorsal white column
Question 5. Following are the major ascending (sensory) tracts of the lateral white column except
- Posterior spinocerebellar
- Anterior spinocerebellar
- Spinotectal
- Anterior spinothalamic
- Spino-olivary
Answer: 4. Anterior spinothalamic
Spinal Tracts
Question 6. The following statements are true regarding the anterior spinocerebellar tract except
- Anterior Spinocerebellar Tract is a crossed spinocerebellar tract
- Anterior Spinocerebellar Tract carries proprioceptive and exteroceptive impulses
- These impulses do not reach the level of consciousness
- This pathway consists of three sensory neurons
- The fibers of second-order sensory neurons cross twice
Answer: 4. This pathway consists of three sensory neurons
Question 7. The following statements are true regarding the lateral spinothalamic tract except
- Lateral Spinothalamic Tract carries the sensation of pain and temperature
- Lateral Spinothalamic Tract arises at all the levels of the spinal cord
- Lateral Spinothalamic Tract is an uncrossed tract
- The second-order neurons are situated in laminae 1, 4 and 5
Answer: 3. It is an uncrossed tract
Question 8. Which of the statements about the anterior corticospinal tract is false?
- Anterior Corticospinal Tract is formed mainly by axons arising from the somatomotor cortex
- Anterior Corticospinal Tract is a crossed-tract
- Anterior Corticospinal Tract terminates on the contralateral anterior horn cells of the spinal cord
- Anterior Corticospinal Tract extends throughout the spinal cord
Answer: 2. Anterior Corticospinal Tract is a crossed tract
Question 9. Which of the following statements about the corticonuclear tract is false?
- Fibers terminate on motor nuclei of cranial nerves
- Passes through the genu of the internal capsule
- Fibers usually terminate on the nuclei of both sides
- Injury leads to ‘lower motor neuron type’ of paralysis
Answer: 4. Injury leads to ‘lower motor neuron type’ of paralysis
Spinal Cord Tracts
Question 10. The following facts regarding the rubrospinal tract are true except.
- Rubrospinal Tract is a crossed-tract
- Rubrospinal Tract arises from the red nucleus
- Rubrospinal Tract is a part of the extrapyramidal system
- Rubrospinal Tract descends in the lateral funiculus of the spinal cord
- This tract terminates on the neurons of the posterior horn of the spinal cord.
Answer: 5. This tract terminates on the neurons of the posterior horn of the spinal cord.
Brainstem Medulla Multiple Choice Questions
Brainstem Medulla Oblongata Multiple Choice Questions
Question 1. The following statements about the brainstem are true except
- It consists of the pons, medulla and cerebellum
- It is continuous above with the thalamus, hypothalamus and cerebral hemispheres
- It is continuous below with the spinal cord
- It lies in posterior cranial fossa
Answer: 1. It consists of the pons, medulla and cerebellum
Question 2. Which of the following statements about the attachment of cranial nerves is false?
- The brainstem gives attachment to all the cranial nerves
- The nuclei of cranial nerves 3 to 7 are situated deep in the brainstem
- Cranial nerves 3 and 4 are attached to midbrain
- Cranial nerve 5 is attached to the pons
- Cranial nerves 6 to 7 are attached to the medulla
Answer: 1. Brainstem gives attachment to all the cranial nerves
Read and Learn More Neuroanatomy
Question 3. Which of the following statements about the ventral aspect of the medulla is false?
- On either side of the anteromedian fissure, there is the presence of a pyramid.
- Olive is present lateral to the anterolateral sulcus
- The posterolateral sulcus gives attachment to the cranial nerve 7 Ventral aspect of the medulla is related to basisphenoid (clivus)
- The anterolateral sulcus is present between the olive and pyramid
Answer: 3. Posterolateral sulcus gives attachment to cranial nerve 7 Ventral aspect of the medulla is related to basisphenoid (clivus)
Question 4. Which of the following statements about the posterior surface of the lower part of the medulla is true?
- This surface lies between the posteromedian sulcus and the posterolateral sulcus
- This surface is an upward continuation of fasciculi gracilis and cuneatus
- Fasciculi gracilis and cuneatus are continuous above as gracile and cuneate tubercles
- Lateral to fasciculus cuneatus, a swelling is seen that is known as tuberculum cinereum
- All of the above
Answer: 4. Lateral to fasciculus cuneatus, a swelling is seen that is known as tuberculum cinereum
Question 5. Which of the following statements about the transverse section of the medulla at the level of sensory decussation is false?
- This level is cranial to pyramidal decussation
- Nuclei gracilis and cuneatus are situated on the posterior aspect of the section
- The nucleus of the spinal tract of the trigeminal nerve is situated ventrolateral to the nucleus cuneatus
- Nucleus ambiguus is situated in the area of reticular formation
- None of the above
Answer: 3. The nucleus of the spinal tract of the trigeminal nerve is situated ventrolateral to the nucleus cuneatus
Question 6. Which of the following facts about the medial longitudinal bundle is false?
- In the medulla, it is present posterior to the media lemniscus
- It is present anterior to the hypoglossal nucleus
- It is present throughout the brainstem in the same paramedian position
- It consists of ascending and descending fibres connecting various cranial nerve nuclei (3, 4, 6 and 8).
- None of the above
Answer: 3. It is present throughout the brainstem in the same paramedian position
Question 7. Medial medullary syndrome is caused by to occlusion of
- Anterior spinal artery
- Posterior inferior cerebellar artery
- Pontine artery
- Vertebral artery
Answer: 1. Anterior spinal artery
Question 8. Lateral medullary syndrome is caused due to
- Occlusion of vertebral artery
- Anterior spinal artery
- Posterior inferior cerebellar artery
- Anterior inferior cerebellar artery
Answer: 3. Posterior inferior cerebellar artery
Question 9. Which of the following cranial nerve nuclei lie in the medulla?
- Facial nerve nucleus
- Abducent nerve nucleus
- Sensory nucleus of the trigeminal nerve
- The dorsal nucleus of the vagus
Answer: 4. Dorsal nucleus of the vagus
Question 10. The following sensations are carried by the tracts of the posterior spinal column (funiculus) except
- Proprioceptive sensation
- Tactile localisation
- Bladder distension
- Pain
Answer: 4. Pain
Question 11. Which is false regarding branches supplying blood to the medulla?
- Posterior inferior cerebellar artery
- Unnamed branches form vertebral arteries
- Posterior spinal artery
- Anterior inferior cerebellar artery
- Anterior spinal artery
Answer: 1. Posterior inferior cerebellar artery
Question 12. Which of the following statements about the connection of the medulla to the cerebellum is true?
- Through afferent fibres only
- Through both afferent and efferent fibres
- Through the middle cerebellar peduncle
- Through both middle and inferior cerebellar peduncles
Answer: 2. Through both afferent and efferent fibres
Brainstem Pons Multiple Choice Questions
Brainstem Pons Multiple Choice Questions
Question 1. Which of the following statements about pons is false?
- It lies in front of the cerebellum
- The posterior laulaco oi pons IN is formed by the upper surface of the Iho root of the fourth ventricle.
- The posterior surface of pons Is lit laterally by
superior cerebellar peduncles - The posterior surface of the pons Is released In the cerebellum
Answer: 2. The posterior laulaco oi pons IN is formed by the upper surface of the Iho root of the fourth ventricle.
Question 2. Which of the following statements about pons Is false?
- The ventral surface of pons Is bounded by upper and lower bonders
- The ventral surface of pons Is convex
- There is a shallow basilar groove In the midline, which lodges the basilar plexuses of veins
- Laterally, the ventral surface is continuous with the middle cerebellar peduncle
- The ventral surface of the pons is About the basisphenoid (clivus) bone
Answer: 3. Laterally, the ventral surface is continuous with the middle cerebellar peduncle
Read and Learn More Neuroanatomy
Question 3. All the following statements about the transverse section of the pons are true except.
- The section is divided into basilar and tegmental parts
- The basilar part contains transversely and vertically running white fibres
- The basilar part does not contain grey matter (nuclei)
- Transverse fibres run laterally to form the middle cerebellar peduncle
- Vertical fibres run downwards to form the pyramid
Answer: 3. The basilar part does not contain grey matter (nuclei)
Question 4. Which of the following descending fibres are present in the die basilar part of die pons?
- Corticospinal
- Corticonuclear
- Corticopontine
- All of the above
Answer: 4. All of the above
Question 5. Which of the following statements about the corticomotor cerebellar pathway is false?
- It arises from frontal, temporal, parietal and occipital lobes
- It terminates on pontine nuclei of the same side
- The fibres arising from pontine nuclei constitute transverse fibres (pontocerebellar) of the pons
- Pontocerebellar fibres enter the cerebellum on the same side through the middle cerebellar peduncle.
Answer: 4. Pontocerebellar fibres enter the cerebellum on the same side through the middle cerebellar peduncle.
Question 6. The Efforts of the vestibular a relay Million In die 1 in 3 pilot cerebellar pathway of die vrullbiilm mu leur complex form die following?
- Vestibulocerebeller tract
- Vestibulospinal tract
- Medial longitudinal bundle
- lateral lemniscus
- Medial lemniscus
Answer: 5. Medial lemniscus
Question 7. The trapezoid body is formed by
- Fibre of both dorsal and ventral cochlear nuclei
- Efferents iirlulng from superior olivary nuclei
- Efferents arising from (lie nucleus of die trapezoid body
- All of the above
Answer: 4. All of the above
Question 8. Which of the following menisci are present in the white mailer of tegmentum at the upper level of pons?
- Medial lemniscus
- Spinal lemniscus
- Trigeminal lemniscus
- Lateral lemniscus
- All of the above
Answer: 5. All of the above
Question 9. The following statements about pontine haemorrhage are true except
- It occurs due to occlusion or haemorrhage of pontine arteries
- Corticospinal fibres are damaged leading to hemiplegia on the opposite side of the body
- Facial paralysis on the opposite side of the body due to damage to the facial nucleus
- There is hyperpyrexia due to damage to sympathetic fibres through which the heat-regulating centre exerts its effect
- Pinpoint pupil due to damage to sympathetic fibres
Answer: 3. Facial paralysis on the opposite side of the body due to damage to the facial nucleus
Question 10. Which ofthe following facts about Raymond’s syndrome are true?
- It results from to occlusion of pontine branches of the basilar artery
- Damage occurs to corticospinal fibres
- Damage to abducent nerve fibres
- All of the above
Answer: 4. All of the above
Autonomic Nervous System Functions Notes
Autonomic Nervous System
The autonomic nervous system controls and coordinates the internal environment of the body. This system has two divisions:
- Sympathetic
- Parasympathetic
Both these divisions are complementary to each other. They function in coordination and adjust the body unconsciously to maintain the internal environment.
Most organs of our body receive innervations from both sympathetic and parasympathetic fibers. In general, a nerve impulse from one division stimulates the organ to increase the activity while the other will have the opposite action, i.e. decreases the activity.
For example, stimulation of sympathetic nerves increases the heart rate while stimulation of parasympathetic innervations decreases the heart rate.
Read and Learn More Neuroanatomy
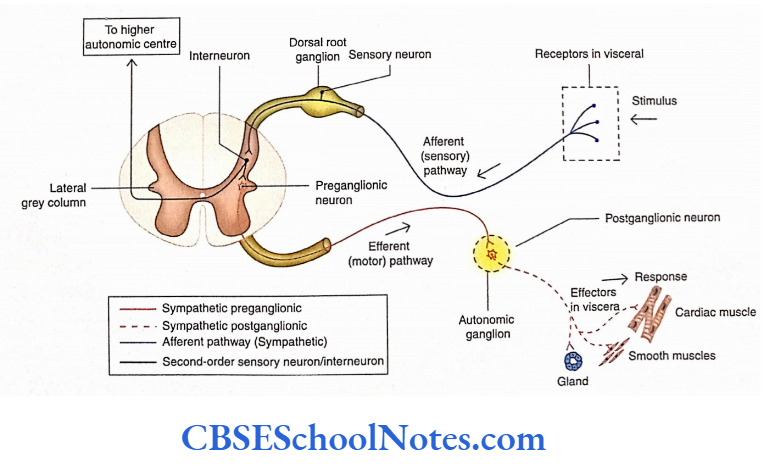
The ANS consists of both afferent (sensory) and efferent (Motor) components and an integration center.
Autonomic Sensory (Visceral Afferent) Component The sensations of the autonomic system are transmitted from the viscera to the CNS through somatosensory fibers.
The cell bodies of sensory neurons are located in the dorsal root ganglion of spinal nerves and the sensory ganglia of some cranial nerves.
Somatosensory neurons are also responsible for visceromotor reflex activities. Though these sensations hardly reach the level of consciousness, the sensations of nausea and pain in
the heart is perceived.
Integration and Control of the Autonomic Nervous System. The autonomic activities are integrated at higher levels. These centers are situated in the reticular formation of the brainstem, hypothalamus, limbic cortex, and prefrontal cortex.
The hypothalamus is considered the higher center (control and integration) of ANS. It controls both sympathetic and parasympathetic divisions of ANS.
The neurons of sympathetic and parasympathetic nuclei in the brainstem and spinal cord are connected with the nuclei of the hypothalamus through the reticular formation.
Autonomic Motor (Visceral Efferent) Component. The autonomic activities regulate body temperature, heart rate, respiration, blood pressure, gastrointestinal motility, and secretion from glands.
Thus, ANS consists of motor (efferent) fibers that innervate smooth muscle, cardiac muscle, and glands.
The effector cells of different organ systems are not under voluntary control; they work mostly at an unconscious level.
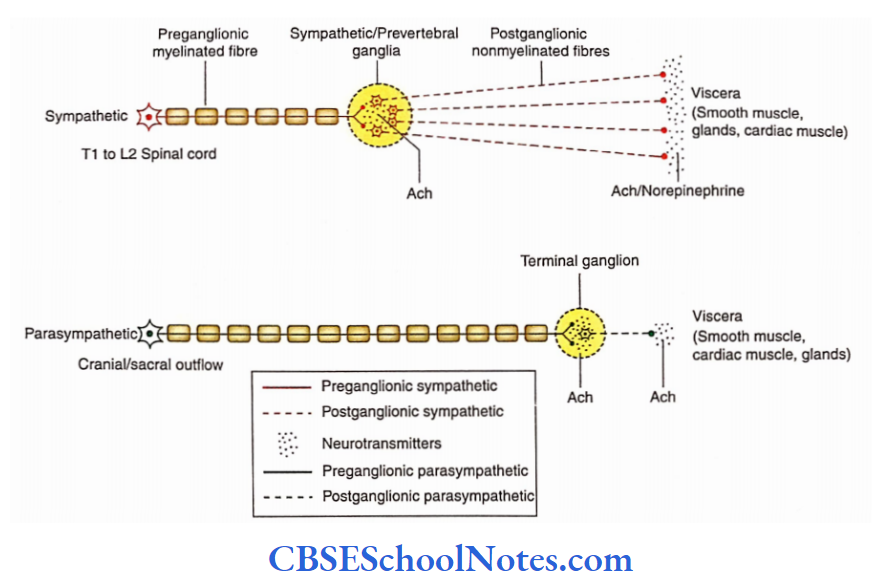
Both sympathetic and parasympathetic motor pathways consist of two motor neurons that conduct the impulses from the CNS to the effector organ.
The cell bodies of the first motor neurons are located in the grey matter of the CNS (brain and spinal cord). These are called preganglionic or presynaptic neurons.
The preganglionic neurons send their myelinated axonal processes to synapse with the second motor neurons in the pathway.
The axons of presynaptic neurons come out of the CNS as part of either the spinal or the cranial nerve.
The cell bodies of second motor neurons are located in the autonomic ganglia outside the CNS.
These are called post-synaptic or post-ganglionic neurons because presynaptic neurons make synaptic contact with them.
The axons of post-synaptic neurons are unmyelinated and terminate on the effector organs (smooth muscle, glands, or cardiac muscle).
Sympathetic Division Of Autonomic Nervous System
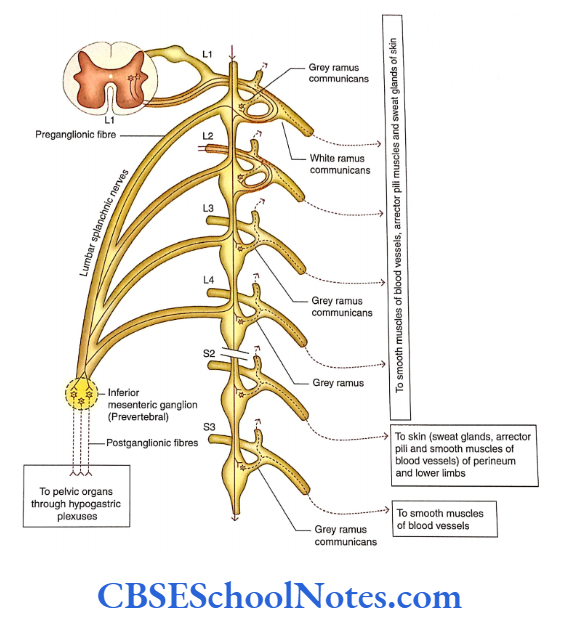
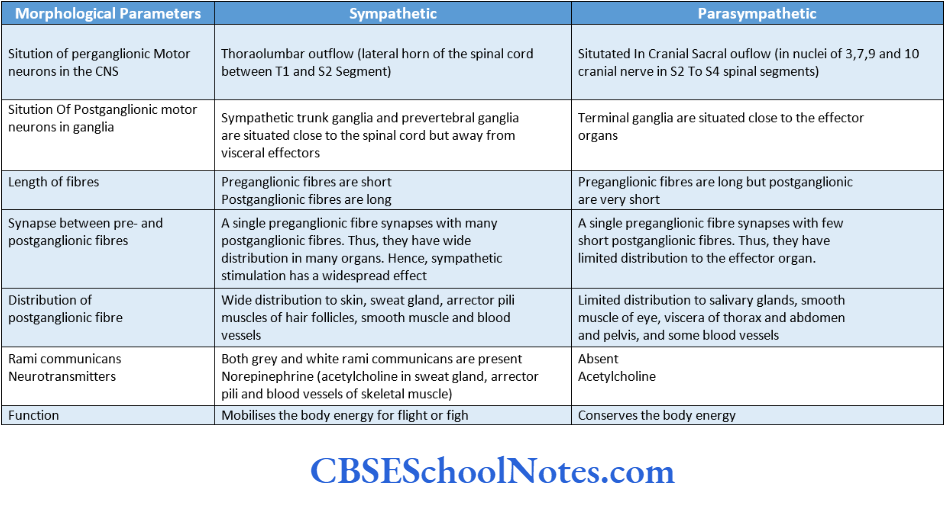
The sympathetic division of the autonomic nervous system is also called thoracolumbar outflow as the preganglionic nerve cells are situated in the thoracic and upper lumbar segments of the spinal cord.
The cell bodies of presynaptic neurons of the sympathetic division of ANS are located in the lateral grey column (horn) of the spinal cord between the T1 and L2 spinal segments.
The cell bodies of postsynaptic neurons are located in two groups:
- Paravertebral ganglion (sympathetic trunk ganglia) and
- Pacvcrtebral ganglion.
- Sympathetic trunk ganglia lie in a vertical row on either side of the vertebral column extending from the base of the skull to the coccyx.
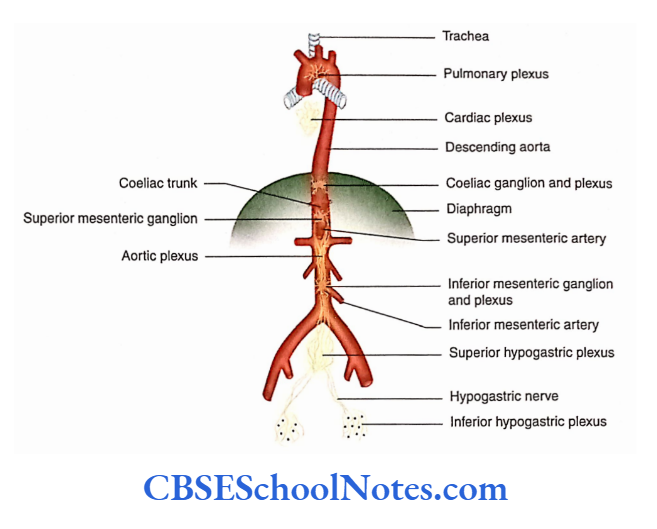
- On the other hand, prevertebral ganglia are situated anterior to the vertebrae and close to the origin of the main branches of the abdominal aorta.
- Examples of prevertebral ganglia are celiac ganglion, superior mesenteric ganglion, and inferior mesenteric ganglion close to the beginning of arteries of the same name.
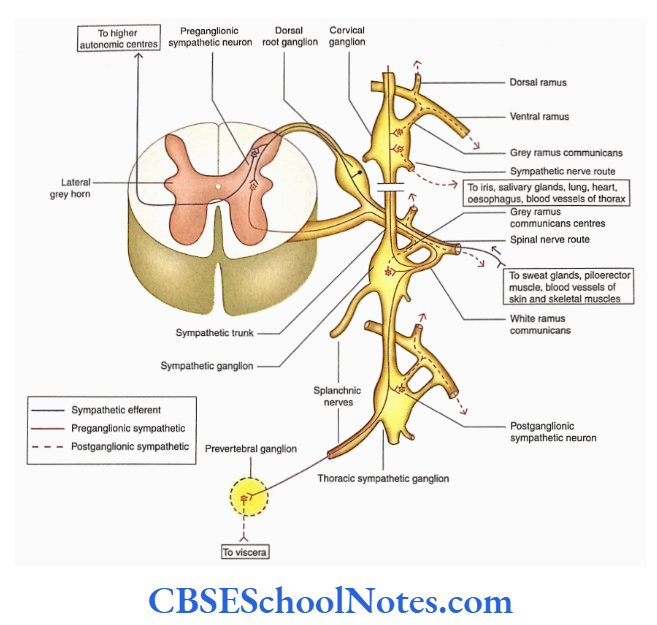
- The axons of presynaptic neurons leave the spinal cord through ventral roots and enter the ventral rami of spinal nerves (T1 to L2).
- These axons are myelinated fibers. They leave the ventral ramus as a slender branch called white ramus communicantes and enter the sympathetic trunk.
- The presynaptic fibers of white ramus communicantes, after entering the sympathetic trunk, may synapse with the postsynaptic neurons present in the sympathetic ganglion at the same level.
- These fibers may also ascend or descend in the sympathetic trunk for a few levels before forming synaptic connections.
- It may also happen that these fibers pass through the sympathetic trunk without synapsing and join the splanchnic nerve to reach the prevertebral ganglia and synapse with the post-ganglionic neurons there.
The splanchnic nerves of the thorax are as follows
- Greater (T5 to T9)
- Lesser (T10 and Til)
- Least (T12)
The splanchnic nerves of the thorax are greater (T5 to T9), lesser (T10 and Til), and least (T12) while lumbar splanchnic nerves take origin from LI to L4 sympathetic ganglia.
The post-synaptic neurons of sympathetic ganglia send their axons (post-synaptic sympathetic fibers) to the adjacent ventral rami of spinal nerves.
These axons are non-myelinated and are called gray rami communicantes. From the ventral rami, they go to all branches of the spinal nerve including the dorsal rami.
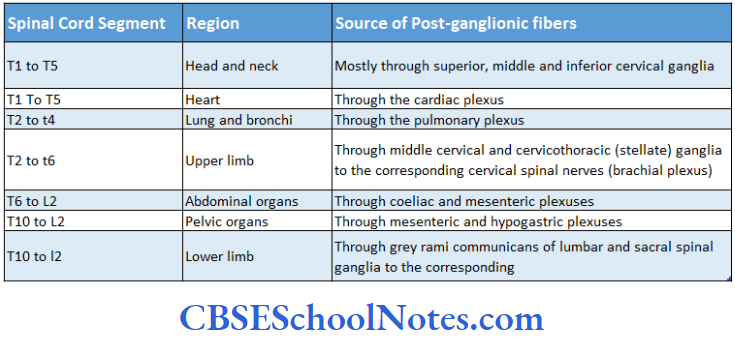
The post-ganglionic fibers from paravertebral sympathetic ganglia (sympathetic trunk ganglia) supply the blood vessels (vasomotor), sweat glands, and smooth muscle of hair follicles (erector pili) in the skin of limbs and body wall.
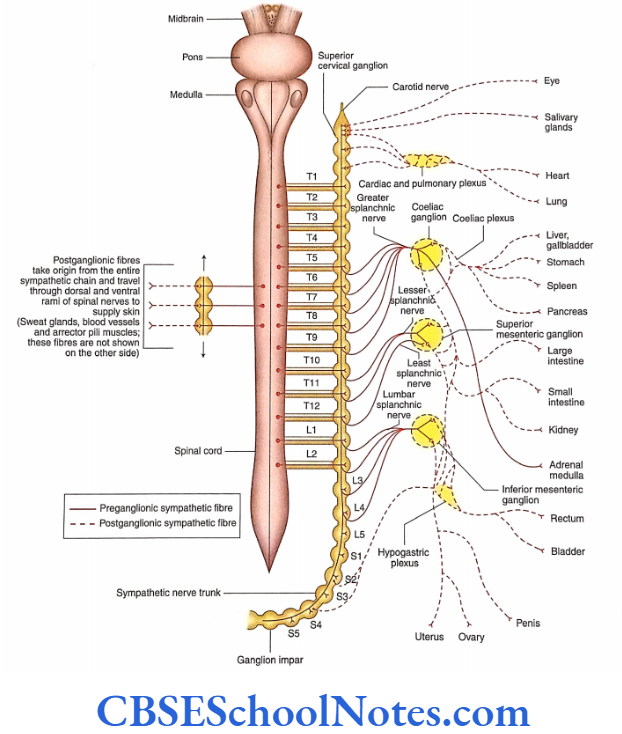
The post-ganglionic fibers from T1 to T5 supply thoracic viscera (heart, lung, trachea, and esophagus) via cardiac and pulmonary plexus.
The post-ganglionic fibers from prevertebral sympathetic ganglia (coeliac, superior and inferior mesenteric, and hypogastric ganglia, and plexuses) supply the abdominal and pelvic viscera (liver, kidney, stomach, intestine, rectum, colon, urinary bladder, genital organ, etc.)
The post-ganglionic fibers from the prevertebral sympathetic ganglia follow the course of various arteries.
(Students should note that the prevertebral ganglia consist of post-ganglionic sympathetic neurons only. However; these plexuses consist of both sympathetic and parasympathetic fibres.)
The sympathetic nervous activities are widely diffused activities that affect the whole body. The sympathetic reaction deals with emergencies or emotional stress.
The sympathetic reaction leads to the dilatation of the pupil, pale face (due to vasoconstriction in the skin), dry mouth, increased heart rate, and raised blood pressure.
The peristaltic movements of the intestine are suppressed and sphincters are closed. The blood vessels of skeletal muscles, heart, and brain dilate to supply more blood to these vital organs.
Parasympathetic Division Of Autonomic Nervous System
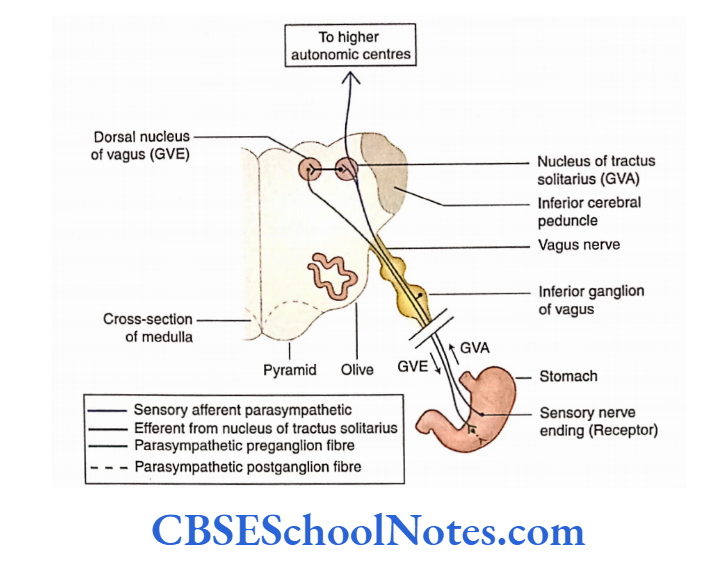
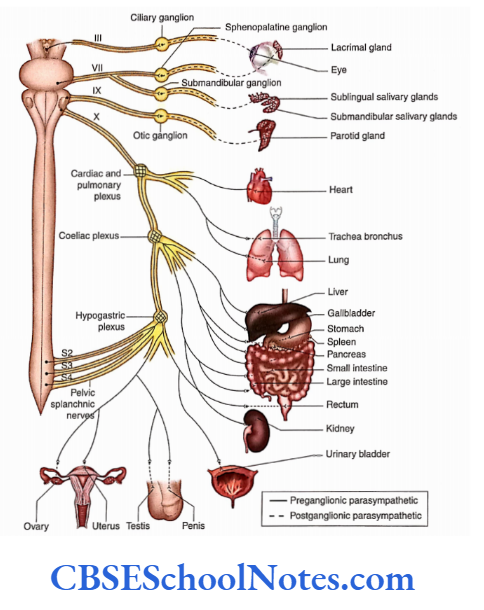
The parasympathetic division of ANS is also known as craniosacral outflow as preganglionic neurons are situated in the brain and sacral segment of the spinal cord.
Cranial outflow: The cell bodies of the cranial part of parasympathetic preganglionic neurons are situated in the brain and axons come out along with cranial nerves 3, 7, 9, and 10.
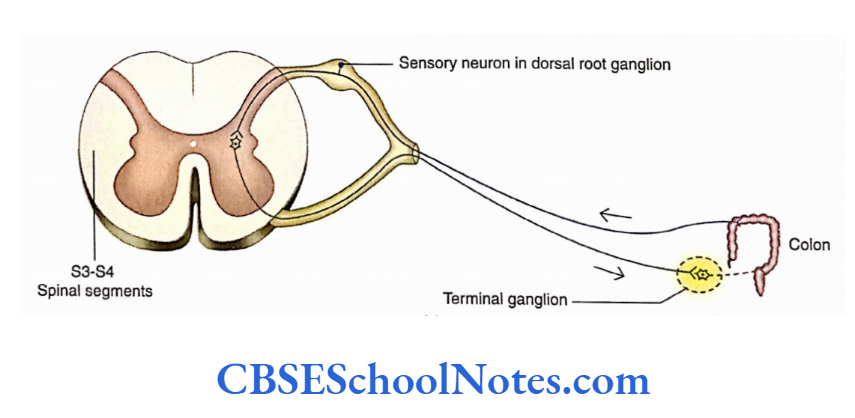
Sacral outflow: The sacral parts of preganglionic neurons are situated in the lateral grey column (horn) of spinal cord segments S2 to S4.
Their axons come out of the spinal cord through the ventral rami. The fibers from ventral rami then travel into pelvic splanchnic nerves.
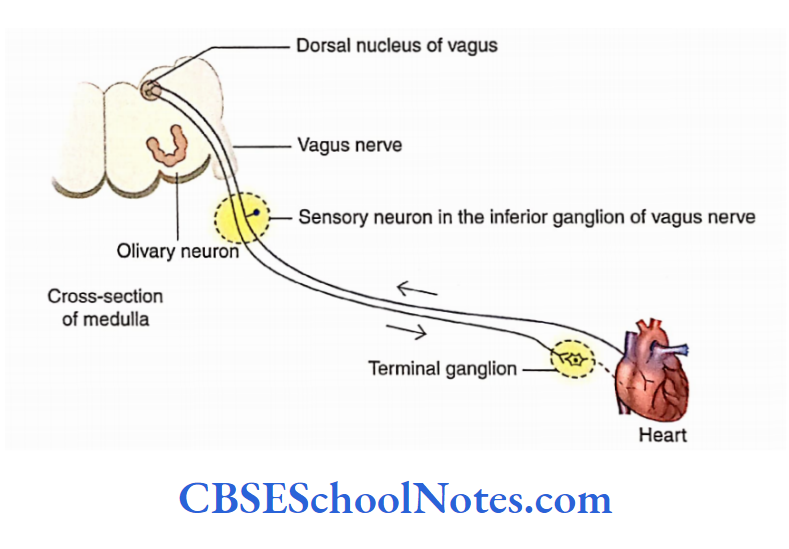
The axons of pre-ganglionic neurons are very long, as they reach up to the effector organs. Close to the organs or within the substance of the organ, there is the presence of ganglia called terminal ganglia.
The terminal ganglia consist of post-synaptic neurons. Pre-synaptic axons form synaptic contacts with these neurons.
The terminal ganglia consist of post-synaptic neurons. Pre-synaptic axons form synaptic contacts with these post-synaptic neurons.
As the terminal ganglia are close to the organ supplied by the parasympathetic nerve, the axons of post-synaptic neurons are very short. They innervate the smooth muscles and glands in the wall of an organ.
The terminal ganglia associated with cranial outflow are ciliary (3 cranial nerve), pterygopalatine ganglia, submandibular ganglia (4 cranial nerve), and otic ganglia (9 cranial nerve).
The post-ganglionic fibers from these ganglia supply the eye, salivary glands, and other structures of the head and neck.
The pre-ganglionic parasympathetic fibers in the vagus nerve extend to many terminal ganglia in the thorax and abdomen. The post-ganglionic fibers supply the heart and lungs in the thorax (through cardiac and pulmonary plexuses). They supply the liver, gall bladder, stomach pancreas, small intestine, and part of the large intestine pancreas, small intestine, and part of the large intestine in the abdomen (through coeliac and superior mesenteric plexuses).
The postganglionic fibers from sacral outflow supply smooth muscle and glands in the wall of the colon, ureter, urinary bladder, and reproductive organs (through the hypogastric plexus).
Sympathetic And Parasympathetic Systems A Comparison
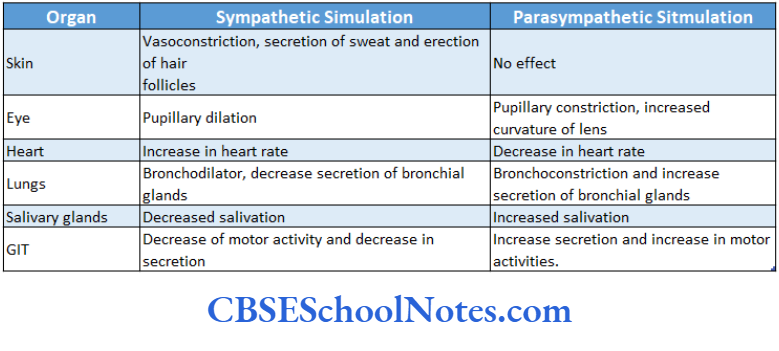
Most of the organs in the body receive both types of motor innervations (sympathetic and parasympathetic). These two types of motor innervations usually have opposite ctions (antagonistic); that is, if one type of innervation increases the activity (excitation) of viscera, then the other type will decrease (inhibition) the activity.
For example, sympathetic stimulation leads to decreased mobility of the intestine and contraction of sphincters. On the other hand, parasympathetic stimulation leads to increased motility of the intestine and relaxation of sphincters.
Sympathetic overactivity causes dilatation of the pupil while parasympathetic overactivity leads to its constriction.
In parasympathetic nerves, the neurotransmitter at pre- and post-synaptic nerve terminals is acetylcholine.
Acetylcholine is liberated at the sympathetic preganglionic nerve terminals while norepinephrine is liberated at postganglionic nerve terminals.
The autonomic innervations of some important organs of the body are described in brief in the following text
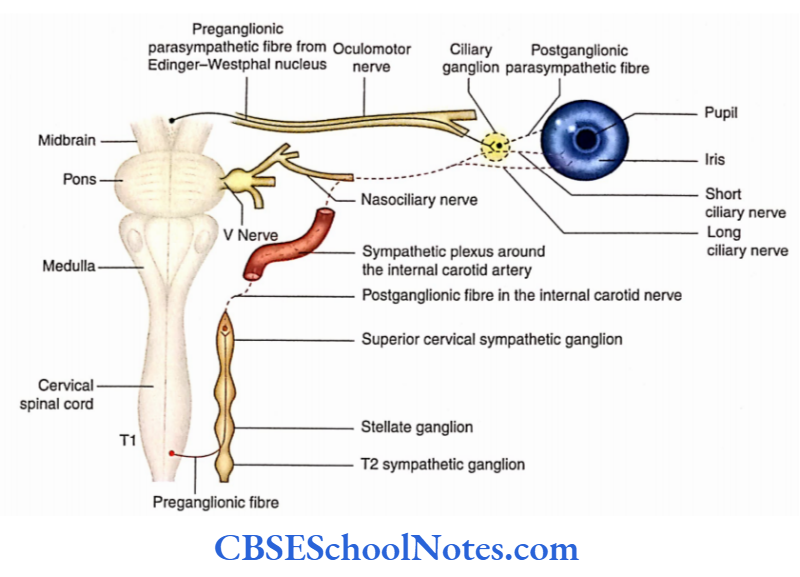
1. Eyeball
- Sympathetic innervation—from the Tl spinal cord segment
- Parasympathetic innervation—from the Edinger- Westphal nucleus
- Stimulation of sympathetic innervation causes dilatation of the pupil and relaxation of ciliary muscles.
- Stimulation of parasympathetic innervation causes constriction of pupil and ciliary muscle.
- Horner’s syndrome (which occurs due to deinnervations of sympathetic nerves of the head and neck) has the following characteristics: Constriction of a pupil, partial ptosis, absence of secretion on the face, flushing of the face, and enophthalmos.
2. Submandibular and sublingual salivary glands
- Sympathetic innervation—from Tl and T2 spinal segments
- Parasympathetic innervation—from the superior salivatory nucleus of the facial nerve
3. Lacrimal gland
- Sympathetic innervation—from Tl and T2 spinal segments
- Parasympathetic innervation—from the lacrimatory nucleus of the facial nerve.
4. Parotid gland
- Sympathetic innervation—from T1 and T2 spinal segments
- Parasympathetic innervation—from the inferior salivatory nucleus of the glossopharyngeal nerve
5. Heart
- Sympathetic innervation—from T1 to T5 spinal segments
- Parasympathetic innervation—from the dorsal nucleus of the vagus nerve.
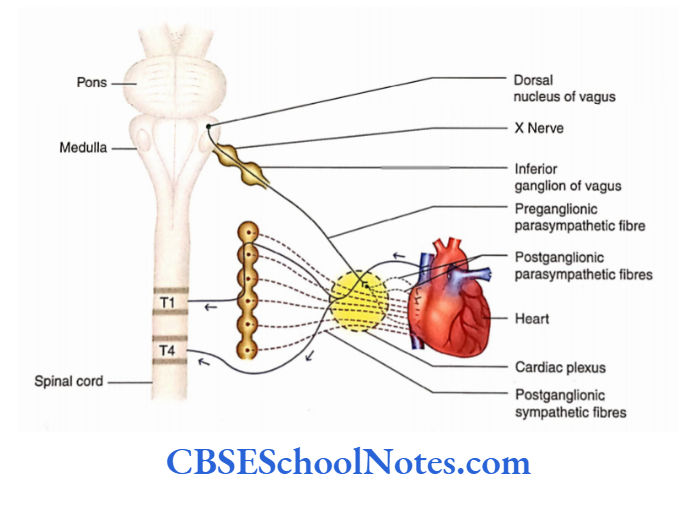
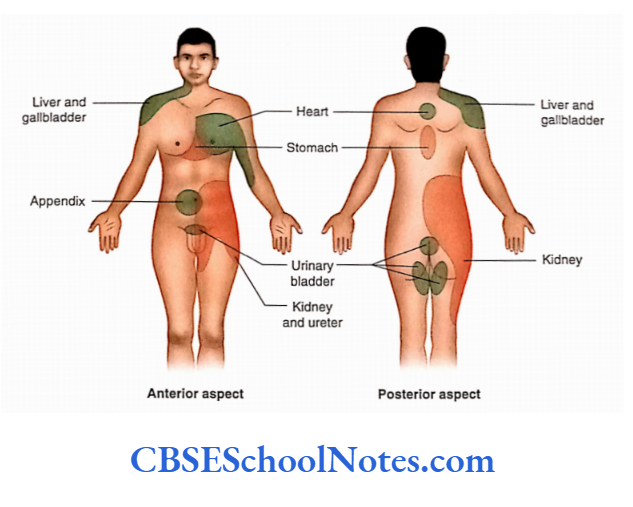
The pain of a heart attack is felt over the middle of the sternum, left shoulder, jaw, and medial aspect of the left arm.
This is because these areas are supplied by the same segments of the spinal coral as the heart (T1 to T5).
6. Lungs
- Sympathetic innervation—from T2 to T5 spinal segments
- The pain of a heart attack is felt over the middle of the sternum, left shoulder, jaw, and medial aspect of the left arm.
- This is because these areas are supplied by the same segments of the spinal coral as the heart (T1 to T5).
7. Gastrointestinal tract
- Sympathetic innervation—from T5 to L2 spinal segments
- Parasympathetic innervation—from the dorsal nucleus of the vagus and from the S2 to S4 spinal segment
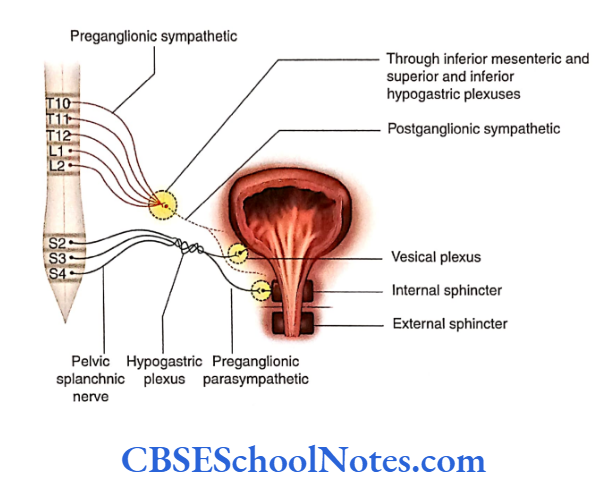
8. Urinary bladder
- Sympathetic innervation—from T10 to L2 spinal segments
- Parasympathetic innervation—from S2 to S4 spinal segments
- Sensory innervation—from T10 to L2 and S2 to S4
9. Arteries of the upper limb
- Sympathetic innervation—from T2 to T8
- Arteries of the lower limb
- Sympathetic innervation-from T10 to L2 spinal cord segments
- Autonomic innervations for the erection of the penis
- Parasympathetic innervation—S2 to S4 spinal segments
- Autonomic innervations for ejaculation from the penis
- Sympathetic innervations from the LI segment.
Localisation Of Visceral Pain
Viscera are usually insensitive to touch, heat, and cutting (cutting of the intestine in a conscious person does not elicit visceral pain).
But if receptors are stimulated in large areas (diffuse stimulation) due to inadequate blood supply, collection of metabolites, distension (stretch), and spasm, then visceral pain can be very severe. When the kidney stone obstructs and distends the ureter, it causes severe pain.
The visceral pain is poorly localized and dull because receptors are stimulated in a large area. The pain may be felt in the viscera itself or it may be felt just deep in the skin that overlies the viscera. However, in many cases, pain cord segments may also be felt in a surface area of the skin far from the stimulated organ. This phenomenon is called refereed pain.
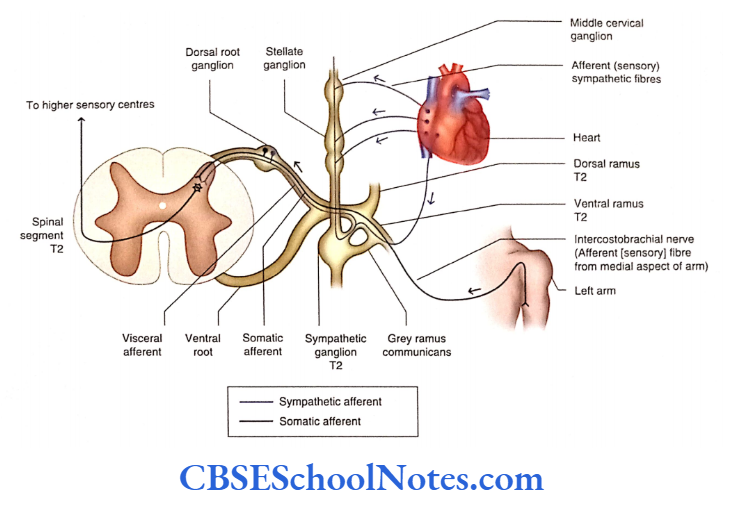
Pain originating from a particular viscus is usually felt at a distance from the site of the visceral organ involved. This may be because afferent fibers from the skin (dermatome) and viscera enter the same segment of the spinal cord.
The first-order neurons of the afferent fibers of both visceral and somatic are situated in the dorsal root ganglia of the spinal nerve.
Probably, both the fibers synapse with the common (same) second-order neuron of the dorsal grey horn of the spinal cord.
The axons of the second-order neuron reach higher centers (via the thalamus) which probably fail to recognize the source of pain (skin or viscera).
Functions Of Autonomic Nervous System
- Both sympathetic and parasympathetic systems of ANS innervate almost all the organs of the body. Thus, their action on one particular organ is antagonistic to each other.
- If one system stimulates (excites) the organ, the other system depresses (inhibits) it. This is because their postganglionic neurons secrete different neurotransmitters
- (Ach for parasympathetic and noradrenaline in case of sympathetic) and their effector receptors for parasympathetic and adrenergic receptors for sympathetic).
- As the hypothalamus is the higher center of ANS it controls and balances the sympathetic and parasympathetic activities.
- However, students should also note that organs such as sweat glands, arrector pili muscles, kidneys, adrenal medulla, and many blood vessels are innervated only by the sympathetic system of the autonomic nerves.
- As there is no parasympathetic innervation in these organs, they do not face opposition. Thus, sympathetic stimulation leads to action while its inhibition leads to cessation of action.
- For example, when sympathetic fibers release norepinephrine into the smooth muscles of blood vessels, blood pressure rises due to the contraction of smooth muscles by mediation of the al receptor.
- Meanwhile, the epinephrine of circulating blood acts on the same smooth muscles by mediation of P2 receptors in the cell membrane leading to vasodilatation and a fall in blood pressure. Parasympathetic fibers do not terminate on many blood vessels.
Enteric Nervous System
The enteric nervous system (ENS) is defined as the system of neurons that is found within the wall of the GIT, gallbladder, and pancreas.
The entire length of GIT is supplied by sympathetic and parasympathetic parts of ANS.
The ANS forms the following two different nerve plexuses in the gut wall:
Submucosal plexus (plexus of Meissner): Situated in the subamucosa
Myenteric plexus (plexus of Auerbach): Situated in between circular and longitudinal muscle coats
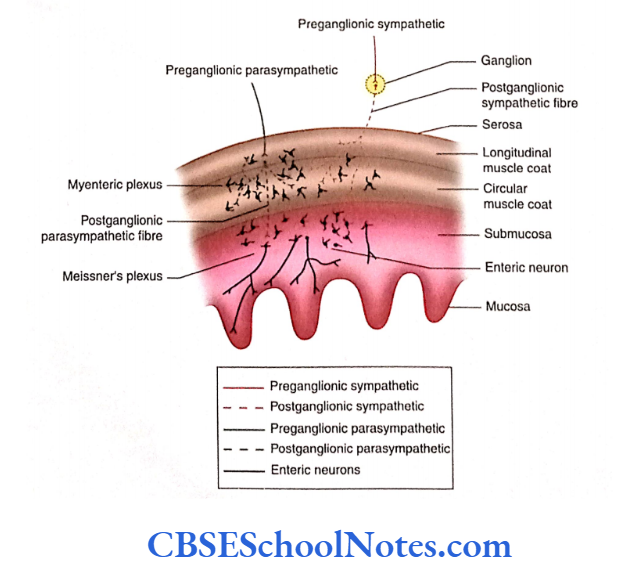
These plexuses consist of the following:
- Parasympathetic preganglionic fibers terminate on postganglionic parasympathetic neurons situated in the myenteric plexus.
- Postganglionic sympathetic and parasympathetic fibers forming a network in Meissner and myenteric plexuses
- Sensory and motor enteric neurons and their processes consist of 100 million neurons in the plexuses of GIT.
All these innervate the mucosa, submucosa, muscle coats, and blood vessels. These regulate the secretion from the mucosal gland and motility of GIT.
The gallbladder and pancreas also have ganglia and nerve plexus. The ENS was previously considered a part of ANS.
However, now it is considered a system separate from the ANS. The neurons of the ENS arise from neural crest; thus, they differ from the origin of sympathetic and parasympathetic neurons.
Functions of the Enteric Nervous System
- The functions of ENS include both sensory and motor.
- The sensory neurons of ENS monitor the stretching of the walls of the intestine and chemical changes within the gastrointestinal tract.
- The motor neurons of ENS control the contraction of the smooth muscle, secretion of the gastrointestinal gland, and endocrine cells associated with GIT.
Autonomic Nervous System Summary
- The autonomic nervous system (ANS) innervates the cardiac muscle, smooth muscle (present in the wall of viscera and blood vessels), and glands.
- The ANS works by forming the reflex arc which is organized in afferent (sensory) pathways, integrating higher centers and efferent (motor) pathways.
- Visceral sensation hardly reaches the level of consciousness. The cell bodies of sensory neurons are situated in the sensory ganglia of cranial nerves and the dorsal root ganglia of spinal nerves.
- The visceral activities are integrated at higher levels, especially in the hypothalamus.
- Efferent pathways convey motor impulses from the CNS to the cardiac muscle, smooth muscles, and glands.
Two neurons are involved in this pathway:
- Preganglionic and
- Postganglionic neurons.
The visceral motor signals reach various organs through two major subdivisions of the ANS:
- Sympathetic and
- Parasympathetic nervous systems.
Sympathetic nervous system
- The preganglionic motor neurons are situated in the lateral horn of the grey matter of the spinal cord from T1 to L2 segments.
- The postganglionic motor neurons of this division are situated in the sympathetic trunk ganglia and prevertebral ganglia.
- The preganglionic fibers reach the sympathetic trunk ganglion through white rami communicans while the postganglionic fibers after coming out through the sympathetic ganglia join the ventral ramus through grey rami communicans.
- Some preganglionic sympathetic fibers, which do not relay in the sympathetic chain (paravertebral), may relay in the prevertebral ganglion through splanchnic nerves.
Parasympathetic nervous system
- The parasympathetic nervous system consists of cranial and ‘sacral’ outflow.
- The preganglionic parasympathetic fibers of both cranial and sacral outflow end in ‘terminal ganglia’ containing postganglionic parasympathetic neurons.
- The terminal ganglia associated with cranial outflow are the ciliary, pterygopalatine, submandibular, and otic ganglia. The terminal ganglia of the vagus and sacral outflow are situated in the wall of the viscera and are unnamed.
- The actions of sympathetic and parasympathetic parts of ANS on any particular organ are antagonistic to each other.
Enteric nervous system
- The enteric nervous system (ENS) consists of motor, sensory, and interneurons, which are found within the walls of GIT.
- The functions of ENS include both sensory and motor.
Autonomic Nervous System Multiple Choice Questions
Question 1. The following structures are innervated by ANS except
- Smooth muscles of viscera
- Smooth muscles of blood vessels
- Cardiac muscles
- Glands
- Articular capsule of joints
Answer: 5. Articular capsule of joints
Question 2. Which of the following facts about visceral sensations are true?
- They hardly reach the level of consciousness
- Sensations of nausea and retrosternal pain are perceived
- The sensation of distension of the bladder and bowel reaches the level of consciousness
- Pain sensation from the viscera is perceived as secondary to a lack of oxygen supply
- All of the above
Answer: 3. Sensation of distension of bladder and bowel reach the level of consciousness
Question 3. Which of the following facts about the autonomic motor pathway is false?
- Visceral motor signals reach organs through the sympathetic and parasympathetic nervous systems
- Both sympathetic and parasympathetic pathways consist of two neurons—preganglionic and postganglionic
- Preganglionic neurons are situated in the CNS while postganglionic in the peripheral ganglion
- The axons of preganglionic neurons are myelinated and synapse with postganglionic neurons
- None of the above
Answer: 5. None of the above
Question 4. Which ofthe following statements about the sympathetic nervous system is false?
- Preganglionic sympathetic neurons are located in the lateral horn of the spinal cord from T1 to L2 and from S2 to S4 spinal segments
- Postganglionic sympathetic neurons are located in the sympathetic trunk (sympathetic chain) ganglia
- They are also located in prevertebral ganglia
- Prevertebral sympathetic ganglia are situated in front of the vertebral column
Answer: 1. Preganglionic sympathetic neurons are located in the lateral horn of the spinal cord from T1 to L2 and from S2 to S4 spinal segments
Question 5. Prevertebral sympathetic ganglia consist of the following except
- Pulmonary ganglion
- Superior mesenteric ganglio
- Inferior mesenteric ganglion
- Celiac ganglion
Answer: 1. Pulmonary ganglion
Question 6. Which of the following statements about splanchnic nerves is false?
- They arise from the thoracic sympathetic chain
- They are medically directed branches of the sympathetic trunk
- They contain postganglionic myelinated nerve fibers
- There are three splanchnic nerves—greater, lesser, and least splanchnic nerves
- These splanchnic nerves reach the prevertebral ganglion
Answer: 3. There are three splanchnic nerves—greater, lesser, and least splanchnic nerves
Question 7. The following facts about the distribution of sympathetic fibres are true except
- Preganglionic sympathetic fibers travel in the ventral spinal nerve root
- They then travel in the ventral ramus of spinal nerves
- They soon leave the ventral ramus to join the sympathetic trunk through the white ramus communicans to synapse with the postganglionic neurons
- The axons of postganglionic neurons join the ventral ramus again through grey ramus communicans
- Grey ramus communicans contain myelinated fibers of postganglionic neurons
Answer: 5. Grey ramus communicans contain myelinated fibers of postganglionic neurons
Question 8. Following is the location of preganglionic motor neurons of the parasympathetic nervous system except
- Few cranial nerve nuclei in the brainstem
- Lateral horn of spinal cord between S2 and S4 spinal segments
- Terminal ganglia of the parasympathetic nervous system
- Pterygopalatine ganglion
Answer: 3. Terminal ganglia of the parasympathetic nervous system
Question 9. Which of the following statements is false?
- Acetylcholine (ACh) is liberated at the terminals of preganglionic parasympathetic neurons
- ACh is liberated at the terminals of preganglionic sympathetic neurons
- Adrenaline is liberated at the terminal of postganglionic parasympathetic neurons
- ACh/norepinephrine is liberated at the terminals of
postganglionic sympathetic neurons
Answer: 3. Adrenaline is liberated at the terminal of postganglionic parasympathetic neurons Part of the thalamus, subthalamus, middle and posterior parts of the hypothalamus, part of the midbrain
Blood Supply Of The Brain And Spinal Cord Notes
Blood Supply Of The Brain And Spinal Cord
The brain is supplied by a pair of vertebral and a pair of internal carotid arteries. In the cranial cavity, both pairs of arteries divide extensively into many branches, some of which are anastomose with each other.
The spinal cord is about a 45-cm long structure; hence, many arteries supply it. The spinal cord is supplied by branches of vertebral arteries and also by segmental arteries, i.e. intercostal and lumbar segmental arteries.
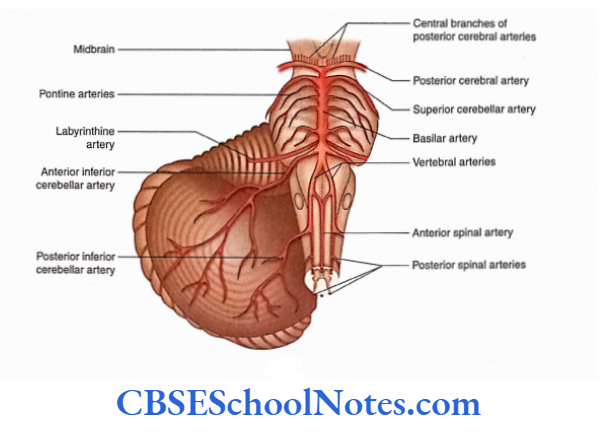
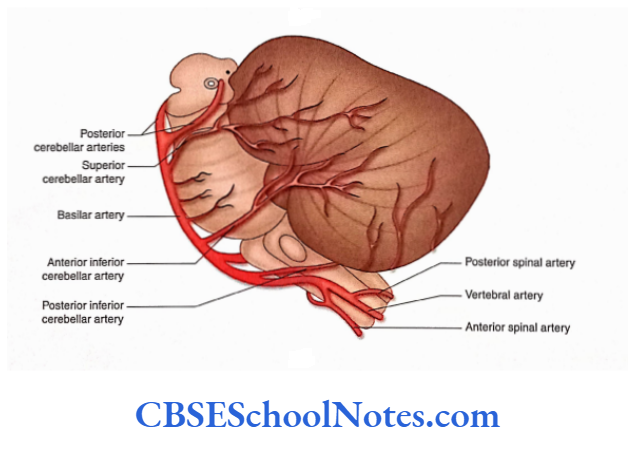
Vertebral Arteries. Each vertebral artery enters the cranial cavity through the foramen magnum after piercing the dura and arachnoid mater.
It curves around the ventrolateral aspect of the medulla and at the lower border of pons it joins with its fellow, from the other side, to form a median basilar artery. The branches of the vertebral artery are given in the following text.
Read and Learn More Neuroanatomy
- Posterior spinal artery: The posterior spinal artery on either side passes inferiorly along the spinal cord, among the dorsal rootlets of spinal nerves.
- Posterior inferior cerebellar artery: The posterior inferior cerebellar artery is the largest branch of the vertebral artery and arises near the lower end of the olive. Had) artery runs posteriorly on either side of the medulla. 1 lore, it supplies the choroid plexus of the fourth ventricle and reaches the cerebellum to supply the posterior part of its inferior surface
- Anterior spinal artery: The anterior spinal artery arises near the inferior border of the pons. It descends anteromedially in front of the medulla and joins its fellow, from the opposite side, to form a single trunk. It is the single trunk of the anterior spinal artery that runs in the anterior median fissure throughout the length of the spinal cord and supplies it
Basilar Artery and Its Branches: The basilar artery runs cranially in the median groove on the pons.
At the superior border of the pons, it divides into two terminal branches:
- Right and
- left posterior cerebral arteries.
The branches of the basilar artery are as follows:
Arteries of the labyrinth: On each side, these arteries arise close to the inferior border of pons and run along with the vestibulocochlear nerve towards the internal ear.
Anterior inferior cerebellar arteries: These arteries arise from the lower part of the basilar artery, on each side, and supply the anterior part of the inferior surface of the cerebellum.
Pontine arteries: These are many small branches that supply pons and the adjacent parts of the brain.
Superior cerebellar artery: On each side, the superior cerebellar artery arises near the upper border of the pons. It supplies the upper pons, lower midbrain and superior surface of the cerebellum.
Posterior cerebral arteries: These arteries are two large terminal branches of the basilar artery, which arise at the superior border of the pons.
Each artery breaks up into branches to supply the temporal and occipital lobes.
The branches of the posterior cerebral arteries are as follows:
Central branches: These are numerous small branches which enter the cerebrum through the posterior perforated substance between two crue
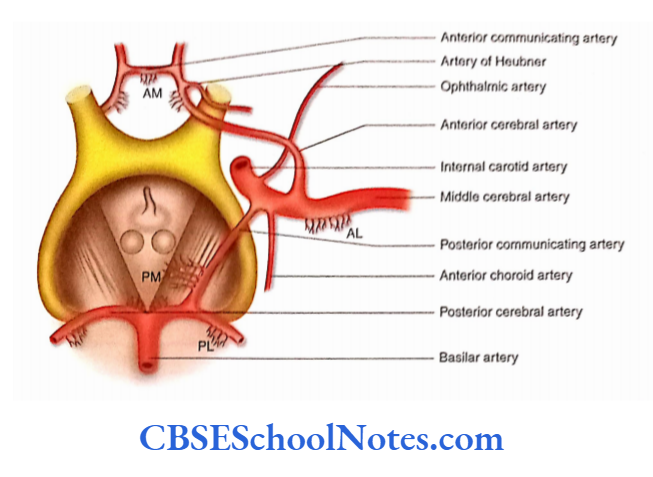
Internal Carotid Artery (ICA). After passing through the cavernous sinus, the ICA pierces the dura mater medial to the anterior clinoid process.
Here, the artery lies immediately inferior to the anterior perforated substance and lateral to optic chiasma.
The ICA has two major branches—anterior and middle cerebral arteries which are its terminal branches and middle cerebral arteries which are its terminal branches ICA also gives smaller branches—ophthalmic, posterior communicating and anterior choroidal arteries.
Anterior cerebral artery: The anterior cerebral artery is a smaller terminal branch of the ICA. After its origin, the right and left anterior cerebral arteries come close to each other and are joined by the anterior communicating artery.
The anterior cerebral artery now ascends in the longitudinal fissure and runs posteriorly along the corpus callosum. The artery gives central and cortical branches.
Central branches: They form the anteromedial group which enters deep inside the cerebral hemisphere by passing through the anterior perforated substance and lamina terminalis. These branches supply the rostrum, septum pellucidum and corpus.
Anterior cerebral artery: The anterior cerebral artery is a smaller terminal branch of the ICA. After its origin, the right and left anterior cerebral arteries come close to each other and are joined by the anterior communicating artery.
The anterior cerebral artery now ascends in the longitudinal fissure and runs posteriorly along the corpus callosum. The artery gives central and cortical branches.
Central branches: They form the anteromedial group which enters deep inside the cerebral hemisphere by passing through the anterior perforated substance and lamina terminalis. These branches supply the rostrum, septum pellucidum and corpus.
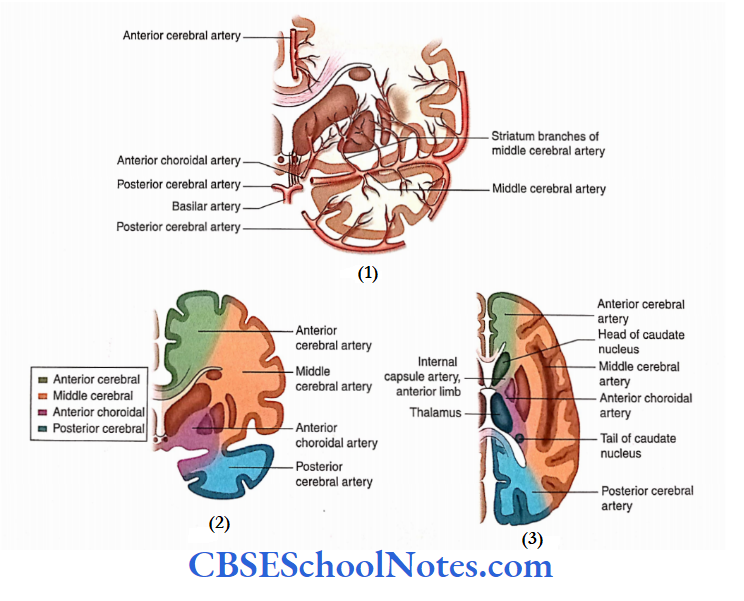
Middle cerebral artery: The middle cerebral artery is a larger terminal branch and a more direct continuation of the ICA. It runs in the stem of the lateral sulcus, between the frontal and temporal lobes, and then turns laterally in the posterior ramus of the lateral sulcus. It gives central and cortical branches.
Central branches: They form the anterolateral group and enter the deeper part of the cerebral hemisphere through the anterior perforated substance. These central branches are grouped into medial and lateral striate arteries.
The medial striate arteries ascend through the lentiform nucleus and supply the lentiform nucleus, internal capsule and caudate nucleus The lateral striate arteries ascend through the external capsule.
Then, they turn medially to supply the lentiform and caudate nuclei along with the internal capsule.
One of the larger lateral striate arteries is more susceptible to rupture; hence, it is called the artery of cerebral haemorrhage (Charcot’s artery of cerebral haemorrhage).
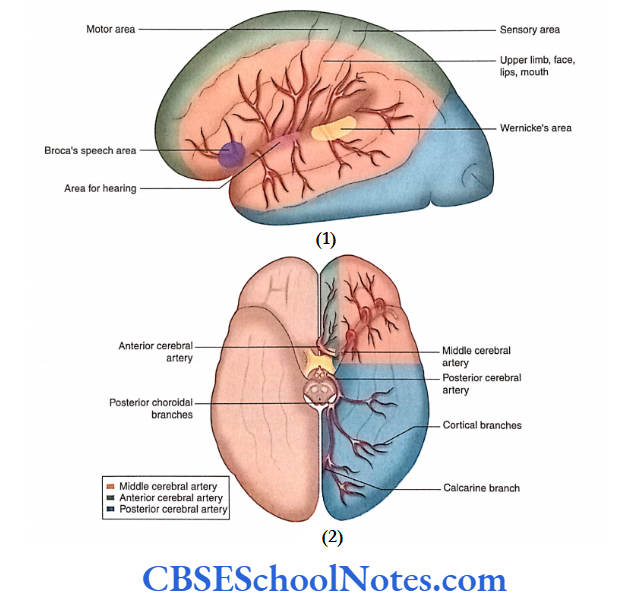
Cortical branches: They emerge in the superolateral surface of the cerebral hemisphere between the lips of the lateral sulcus.
These cortical branches supply most of the superolateral surface and the adjacent part of the orbital surface, tentorial surface and temporal pole.
This artery is responsible for supplying the motor and premotor areas, primary sensory and auditory areas in both hemispheres. The left cerebral hemisphere supplies Wernicke’s language area and Broca’s area of speech.
Occlusion of Cortical Branches of the Middle Cerebral Artery
- The thrombosis or occlusion of the cortical branches of the middle cerebral artery will lead to motor paralysis and sensory loss of the opposite half of the body above the leg.
- Involvement of motor and sensory speech areas of the left cerebral hemisphere (in right-handed persons) will result in aphasia (loss of speech).
- The thrombosis of the middle cerebral artery may also involve the auditory area with little hearing loss, as auditory impulses are projected to both the cerebral hemispheres.
- Occlusion of central branches may lead to hemiplegia
because of infarction of motor fibres in the internal capsule.
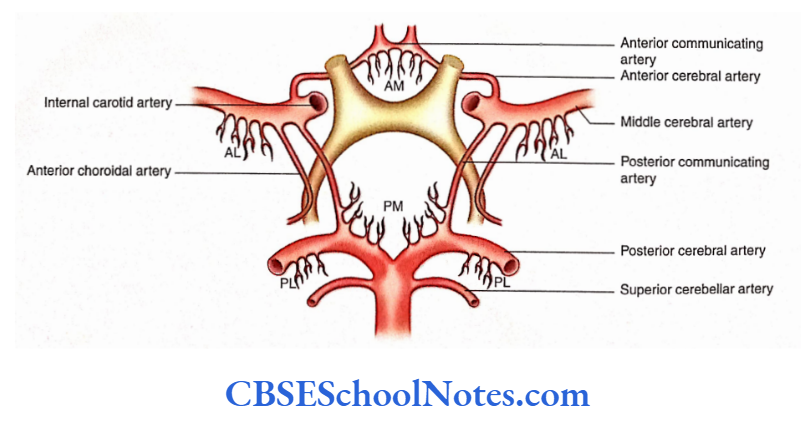
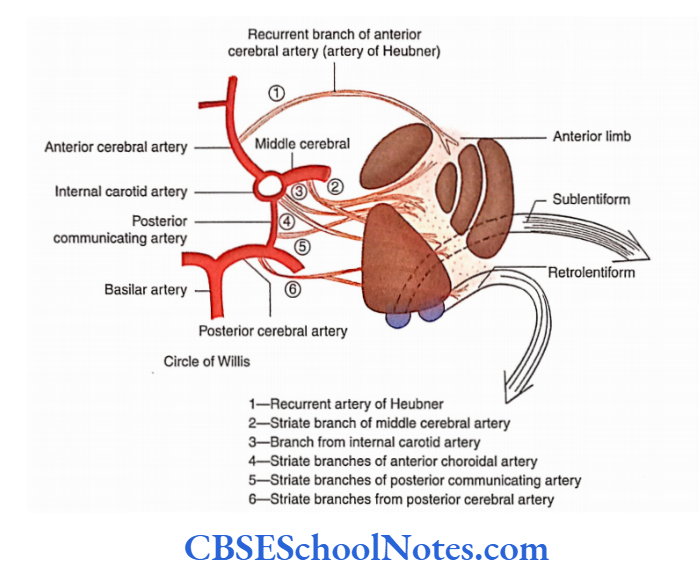
Circulus Arteriosus Circle Of Willis
Circulus arteriosus is a polygonal circle of arteries, present in the interpeduncular fossa. It is formed by posterior cerebral, posterior communicating, internal carotid, anterior cerebral and anterior communicating arteries.
Formation: The circulus arteriosus is bounded posteriorly by two posterior cerebral arteries that communicate with the middle cerebral artery on each side by the posterior communicating branch.
Anteriorly, two anterior cerebral arteries communicate with each other through the anterior communicating artery.
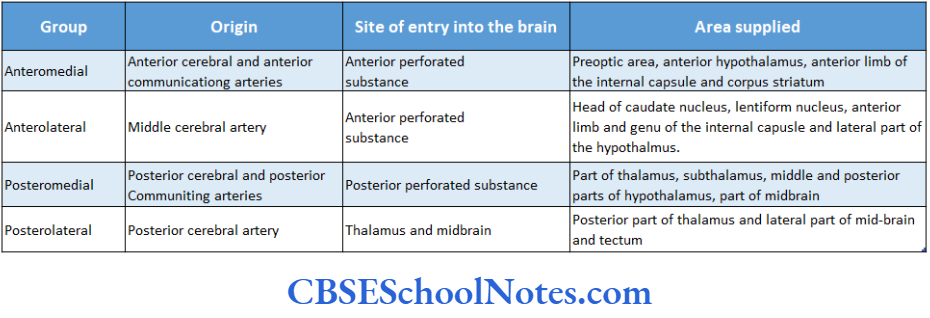
Branches: The circle of Willis gives origin to many slender central branches.
These arteries arise in four groups:
Anteromedial, Anterolateral, Posteromedial and Posterolateral.
These branches immediately pierce the surface of the brain (mostly through anterior and posterior perforated substances) to supply its internal parts such as the corpus striatum, thalamus, internal capsule and midbrain.
These arteries do not anastomose significantly within the brain substance. As these arteries act as end arteries, the damage to the branches entering the substance of the brain leads to the destruction of the brain tissue.
Significance of Circle of Willis
This arterial anastomosis acts as a route through which blood entering the ICA or the basilar artery may be distributed to any part of the cerebral hemisphere.
If one of the major arteries forming the circle of Willis is blocked, then this arterial anastomosis provides an alternative route through which blood can be supplied to the area of the blocked artery.
Arterial Supply Of The Individual Parts Of The Brain
After studying the major arteries and their branches supplying the brain, we shall now study the arterial supply Of the individual parts of the brain as follows
- Arterial supply of the cerebral cortex
- Arterial supply of the internal structures of the cerebral hemisphere
- Arterial supply of brainstem
- Arterial supply of the cerebellum
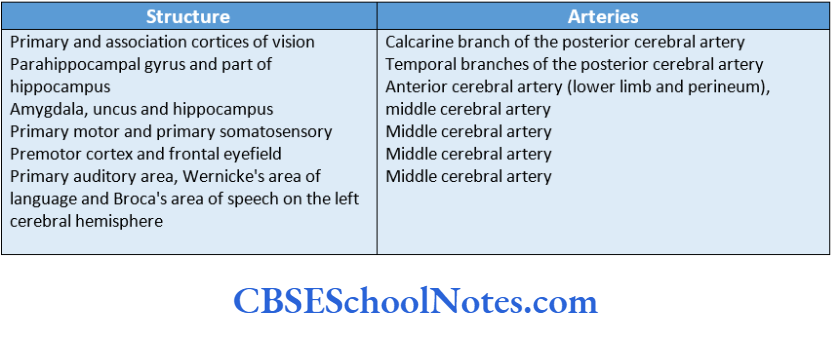
Arterial Supply Of The Cerebral Cortex
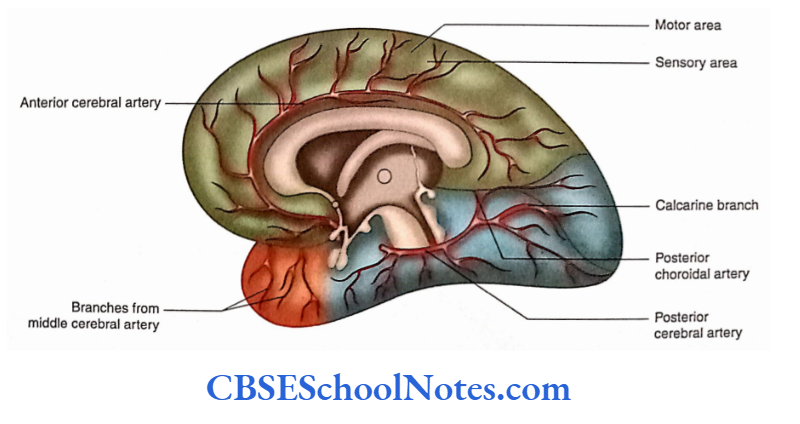
- The cortical branches of three cerebral arteries (anterior, middle and posterior) ramify on the medial, superolateral and inferior surfaces of the cerebral cortex and supply it
- Arterial Supply of Motor and Sensory Areas supply most of the superolateral surface and supply most of the superolateral surface and the temporal pole.
- The middle cerebral artery is responsible for supplying the motor and premotor areas, primary sensory and auditory areas, in both hemispheres. In the left cerebral hemisphere, it supplies Wernickes’ language area and Broca’s area of speech.
- The cortical branches of the anterior cerebral artery supply the motor and sensory areas for the leg and perineum of the opposite side. These areas are present on the medial surface of the cerebral hemisphere.
- The cortical branches of the posterior cerebral arteries supply the visual cortex (area 17) in the occipital lobe.
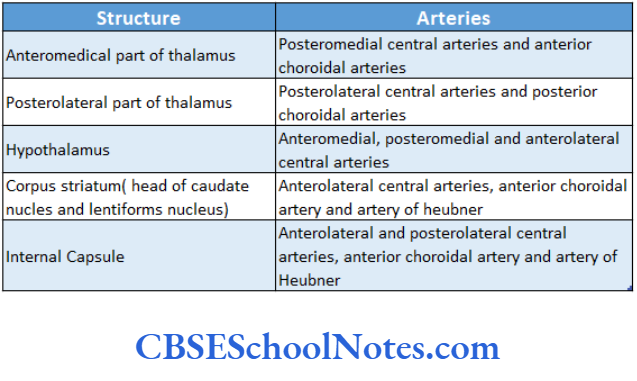
Arterial Supply Of The Internal Structures Of The Cerebral Hemisphere
The central branches enter the cerebral hemisphere and supply the thalamus, hypothalamus, corpus striatum and internal capsule.
Arterial Supply of Brainstem
The medulla is supplied by the anterior and posterior spinal arteries and the posterior inferior cerebellar arteries.
The pons are supplied by the basilar artery, anterior inferior cerebellar arteries and superior cerebellar arteries. The midbrain is supplied by the basilar, superior cerebellar and posterior cerebral arteries.
Arterial Supply Of Cerebellum
The superior and inferior surfaces of the cerebellum are supplied by the superior cerebellar and inferior cerebellar arteries.
Both of these arteries are branches of the basilar artery. The inferior surface is also supplied by the posterior inferior cerebellar artery which is a branch of the vertebral artery.
Venous Drainage of the Brain
The veins draining the brain are thin-walled because their walls are devoid of muscles. They are also without valves as functionally they have to drain towards the direction of gravity.
These veins drain their blood into dural venous sinuses after piercing through the arachnoid mater and inner layer of the dura mater.
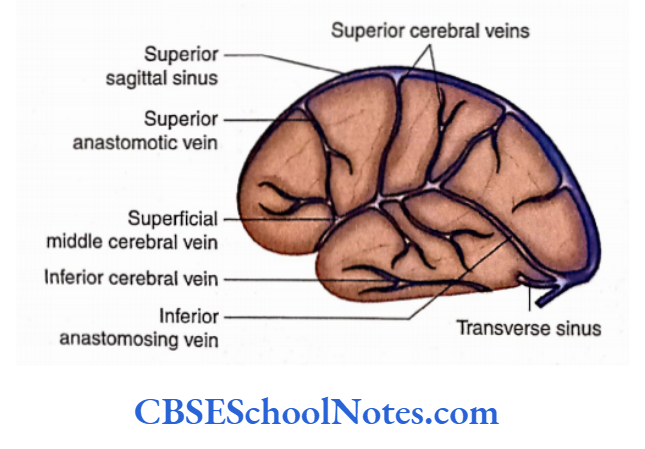
The cerebral veins are classified into external and internal cerebral veins.
The external cerebral veins lie in the subarachnoid space on the surface of the cerebral hemisphere. These are superior, middle and inferior cerebral veins.
The internal cerebral veins, on the other hand, drain the internal parts of the cerebrum and ultimately pour their blood into the great cerebral vein.
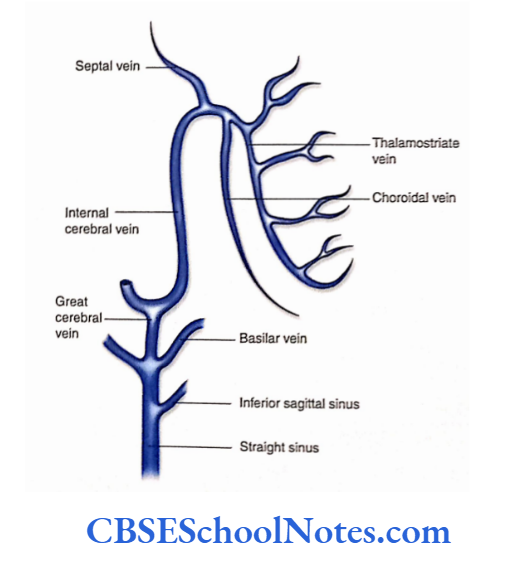
The internal cerebral vein is formed near the interventricular foramen by the union of the thalamostriate vein and choroid veins.
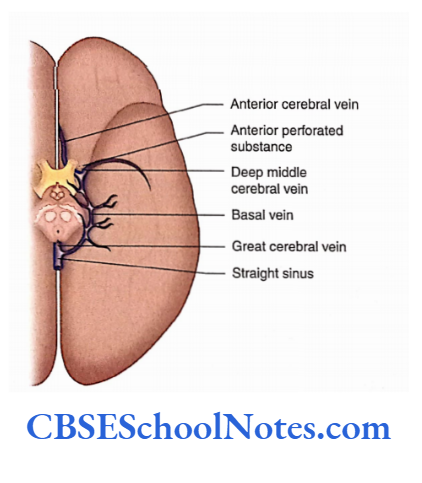
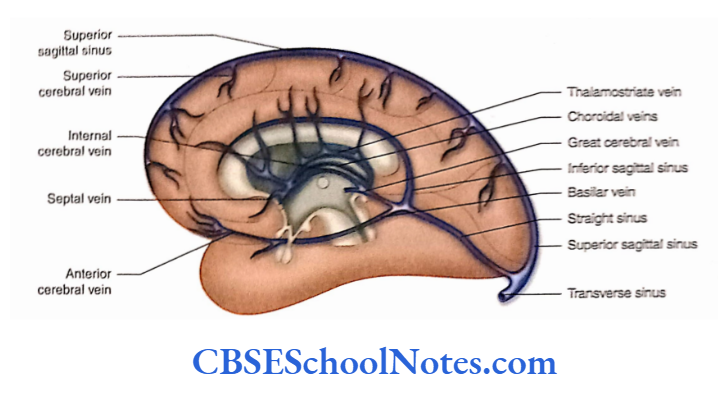
Internal Cerebral Veins
The internal cerebral vein is formed near the interventricular foramen by the union of the thalamostriate vein and choroid veins.
The right and left internal cerebral veins run posteriorly in the transverse fissure where they unite beneath the splenium to form the great cerebral vein.
This vein receives the right and left basal veins and then opens into the straight sinus.
Blood-Brain Barrier
The endothelial lining of brain capillaries does not permit some substances to pass from blood to brain tissue.
The barrier protects the delicate brain tissues from harmful (toxic) substances, lie blood-brain barrier is highly permeable to water, glucose, lipid-soluble substances, O2, C02 and drugs such as alcohol, coffee, nicotine and anaesthetics.
This barrier is, however, an obstacle to delivering drugs such as antibiotics and cancer drugs.
The following structures form the blood-brain barrier:
- The endothelial lining of capillary: There is the presence of tight junctions between endothelial cells.
- The basal lamina of endothelium
- The perivascular end feet of astrocytes on the basal lamina
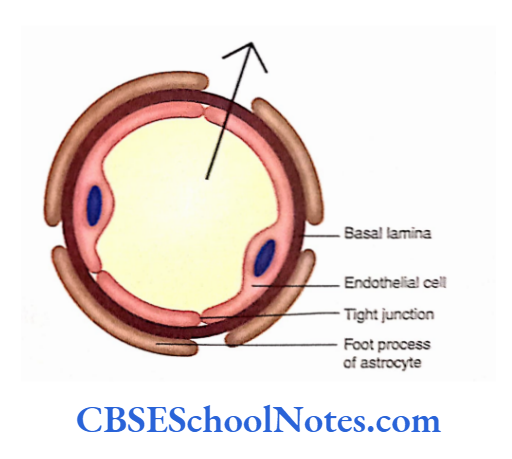
The barrier is mainly formed by the endothelial cells resting on the basal lamina and not by the astrocytes as they do not fully surround the capillary. However, the foot processes stimulate the formation of tight junctions between endothelial cells.
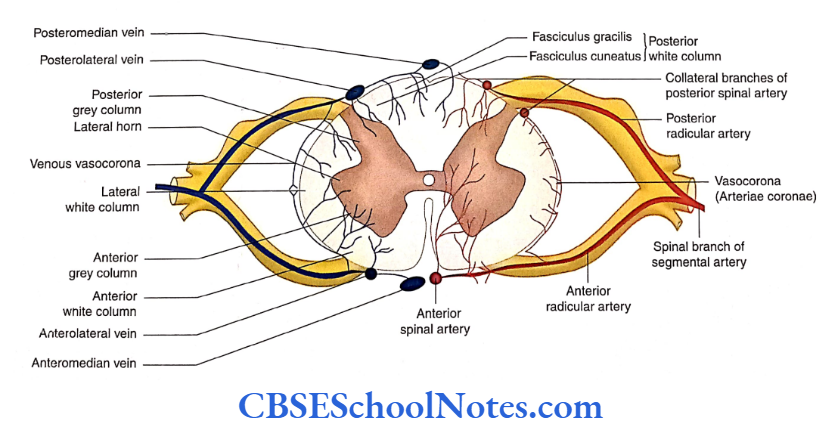
Blood Supply Of The Spinal Cord
The spinal cord is a long structure present in the vertebral canal. Because of its length, the spinal cord is supplied by many arteries. It is drained by longitudinally arranged veins which further drain into radicular veins.
Arterial Supply
The arteries supplying the spinal cord can be grouped into the following:
- Branches of the vertebral arteries, i.e. one anterior and two posterior spinal arteries.
- Multiple spinal branches of segmental arteries
- Radicular arteries
Branches of the vertebral arteries: As the right and left vertebral arteries lie on the anterolateral surface of the medulla, each artery gives two branches that supply the spinal cord. These are the anterior and posterior spinal arteries.
The anterior two-thirds of the spinal cord is supplied by the anterior spinal artery while the posterior one-third is by the posterior spinal arteries.
Segmental arteries: As the spinal cord is a long structure, many segmental arteries supply it.
The spinal branches of the segmental arteries (vertebral, deep cervical, posterior intercostals and lumbar arteries) enter the vertebral canal through the corresponding intervertebral foramen.
Radicular arteries: Each spinal artery divides into anterior and posterior radicular arteries, which run towards the spinal cord along the ventral and dorsal nerve roots, respectively.
The total number of anterior radicular arteries varies from 12 to 17 (mostly six in cervical, two to four in thoracic and two to three in lumbar segments).
Out of these radicular arteries, a single anterior radicular artery is very large and is called the arteria radicularis magna (artery of Adamkiewicz) which usually arises from the lower thoracic or upper lumbar level.
Venous Drainage
Six longitudinally running veins that drain the spinal cord are as follows:
- One along the anterior median fissure
- One along the posterior median sulcus
- Two along the line of right and left ventral nerve rootlets
Two along the line of right and left dorsal nerve rootlets All these veins freely communicate with each other and are drained by anterior and posterior radicular veins.
Blood Supply Of The Brain And Spinal Cord Summary
- The brain has a rich blood supply. It is supplied by a pair of vertebral arteries and a pair of internal carotid arteries.
- The branches of vertebral arteries in the cranial cavity are posterior spinal, posterior inferior cerebellar and anterior spinal arteries.
- Two vertebral arteries join each other to form a median basilar artery at the lower border of the pons.
- The branches of the basilar artery are the artery of the labyrinth, anterior inferior cerebellar artery, pontine arteries and superior cerebellar arteries. It terminates in two posterior cerebral arteries.
- The circle of Willis is formed by the posterior cerebral, posterior communicating, anterior cerebral and anterior communicating arteries.
- The circle of Willis gives origin to many central branches. These arteries arise in four groups:
- Anteromedial,
- Anterolateral,
- Posteromedial and
- Posterolateral.
- Various surfaces of the cerebral cortex are supplied by the cortical branches of the anterior, middle and posterior cerebral arteries.
- The superolateral, medial and inferior surfaces are supplied by all three cerebral arteries:
- Anterior, Middle and Posterior cerebral arteries.
- The corpus striatum and internal capsule are supplied by central branches of the anterior and middle cerebral arteries.
- The thalamus is supplied by the central branches of the posterior cerebral artery and basilar arteries.
- The veins of the brain are grouped as external cerebral veins and internal cerebral veins.
- The veins of the brain drain into intracranial dural venous sinuses.
- The blood-brain barrier is formed by capillary endothelial cells and their basement membrane.
- The spinal cord is supplied by branches of vertebral arteries, namely the anterior spinal artery and two posterior spinal arteries.
- The spinal cord is also supplied by multiple spinal branches of segmental arteries.
- Six longitudinally running veins drain the venous blood from the spinal cord.
Blood Supply Of The Brain And Spinal Cord Multiple Choice Questions
Question 1. Which of the following is not a branch of the vertebra artery?
- Posterior spinal arteries
- Anterior spinal artery
- Superior cerebellar artery
- Posterior inferior cerebellar artery
- Anterior inferior cerebellar artery
Answer: 3. Posterior inferior cerebellar artery
Question 2. Which of the following are the branches of the basilar artery?
- Anterior inferior cerebellar artery
- Pontine artery
- Superior cerebellar artery
- Posterior cerebral artery
- All of the above
Answer: 5. All of the above
Question 3. The Circle of Willis is formed by the following arteries except
- Posterior cerebellar artery
- Post communicating artery
- Anterior cerebral artery
- Middle cerebral artery
- Anterior communicating artery
Answer: 4. Anterior communicating artery
Question 4. Which of the following arteries supply the internal capsule?
- Anterolateral central arteries
- Posterolateral central arteries
- Anterior choroidal artery
- Artery of Heubner
- All of the above
Answer: 5. All of the above
Question 5. Which of the following are the group of central arteries?
- Anteromedial
- Anterolateral
- Posteromedial
- Posterolateral
- All of the above
Answer: 5. All of the above
Question 6. Which of the following is not a tributary of the internal cerebral vein?
- Septal vein
- Thalamostriate vein
- Choroidal vain
- Great cerebral vein
Answer: 4. Great cerebral vein
Meninges And Cerebrospinal Fluid Notes
Meninges And Cerebrospinal Fluid
- The delicate nervous tissue of the central nervous system is protected by structures such as bones, meninges, and cerebrospinal fluid (CSF).
- Meninges are connective tissue membranes, which cover the brain and the spinal cord. The CSF surrounding the brain and the spinal cord acts as a cushion.
- The meninges surrounding the brain are called cranial meninges and those surrounding the spinal cord are called spinal meninges.
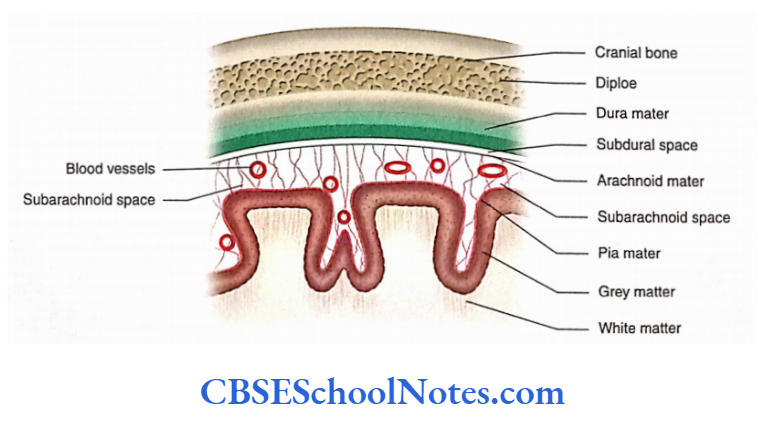
- Meninges are of three different types: From without inwards they are named as Dura mater, Arachnoid mater, and Pia mater.
Read and Learn More Neuroanatomy
Cranial Meninges
Dura Mater
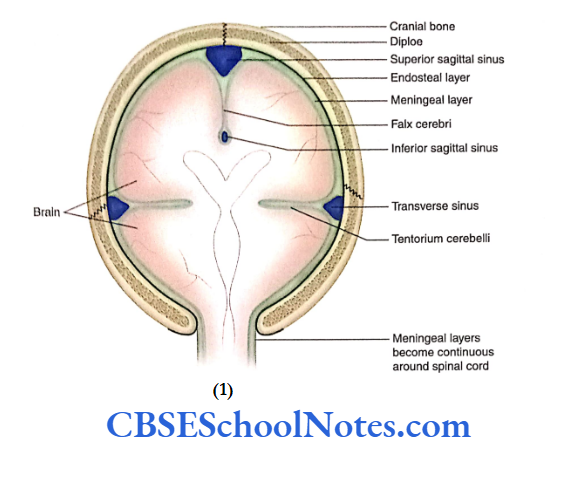
The dura covering the brain is known as cerebral dura. The cerebral dura is made up of an outer endosteal layer and an inner meningeal layer. The endosteal layer of the dura mater is nothing but the endocranium or the inner periosteum.
The meningeal layer of the dura mater is the membranous layer. It covers the brain and then becomes continuous with the dura mater covering the spinal cord.
The two layers of dura mater are tightly fused except in a few places. At these places, the meningeal layer separates from the endosteal layer to form a double-layered fold or partition.
These folds of dura mater extend between the major parts of the brain. As the meningeal layer separates from the endosteal layer, a triangular space is formed.
This space encloses the dural venous sinus. Here, the internal surface of the dura mater is smooth, shining, and lined by endothelial cells.
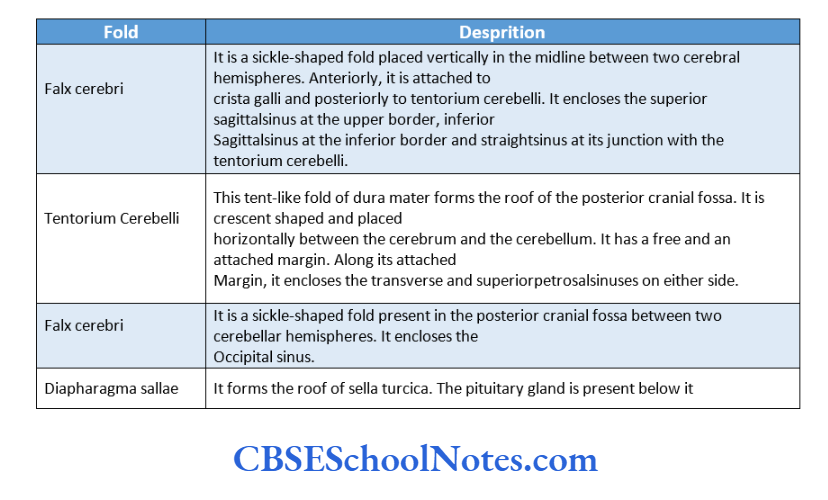
Folds of Dura Mater
The folds of the dura mater play an important role in supporting the brain tissue.
The following folds or septa of the dura mater are formed in the cranial cavity due to duplication of the meningeal layer of the dura.
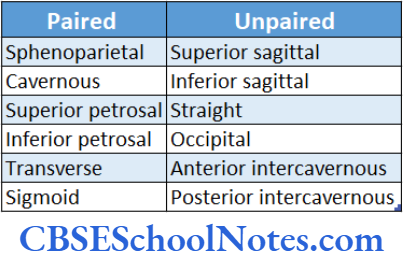
Dural Venous Sinuses
- As mentioned earlier, the dural venous sinuses are formed due to the separation of meningeal and endosteal layers.
- The dural venous sinuses formed between the layers of the dura mater can be paired or unpaired.
- The dural venous sinuses drain the blood from some cranial bones, meninges, and brain. They ultimately pour the blood into the internal jugular veins.
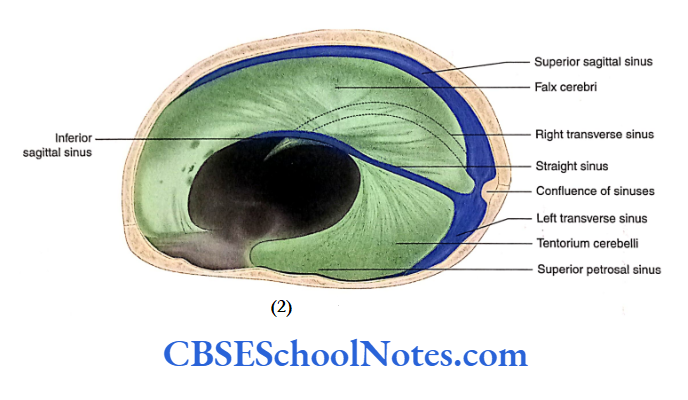
Superior Sagittal Sinus
- The superior sagittal sinus runs at the superior border of the falx cerebri. It begins at the crista galli and is formed by venous blood that is drained from the frontal sinus and veins of the nose.
- This sinus drains superior cerebral veins and becomes continuous with the right transverse sinus at the internal occipital protuberance.
- The inferior sagittal sinus is present at the inferior border of the falx cerebri and drains the falx and medial surface of the cerebral hemisphere. Posteriorly, it becomes continuous with the straight sinus.
Straight Sinus
- The straight sinus is present at the junction of the falx and tentorium.
- The union of the inferior sagittal sinus and the great cerebral vein forms the straight sinus. At the internal occipital protuberance, it becomes continuous with the left transverse sinus.
Transverse Sinus
- The transverse sinus is present on each side of the attached margin of tentorium cerebelli. This sinus extends from the internal occipital protuberance to the base of the petrous temporal bone.
- The right transverse sinus is formed by the continuation of the superior sagittal sinus while the left transverse sinus is formed by the continuation of the straight sinus.
- The transverse sinuses receive blood from the veins of the occipital lobe of the cerebrum and cerebellum and ultimately drain into the right and left sigmoid sinuses.
The sigmoid sinus is situated behind the base of the petrous temporal bone.
This S-shaped sinus is the continuation of the transverse sinus. It passes through the jugular foramen to form the internal jugular vein.
Cavernous Sinus
The right and left cavernous sinuses are situated on either side of the body of the sphenoid. These are formed due to the separation of the endosteal and meningeal layers of the dura mater. These layers are lined by endothelium.
Extension: From the superior orbital fissure anteriorly to the apex of the petrous temporal bone posteriorly.
Tributaries: Superior and inferior ophthalmic veins, cerebral veins, sphenoparietal sinus and frontal trunk of the middle meningeal vein.
Drainage: Into superior and inferior petrosal sinuses and to the basilar plexus of veins.
Communication: With the facial vein through the superior ophthalmic vein, with the pterygoid plexus through the emissary’s veins and with the internal vertebral plexus through the basilar venous plexus
Thrombosis of Cavernous Sinus
- Sometimes, infection may reach the cavernous sinus from the dangerous area of the face and scalp through deep facial and ophthalmic veins.
- This septic thrombosis of the cavernous sinus compresses nerves passing through its lateral wall, and this produces the corresponding symptoms.
- Cavernous thrombosis also causes pain in the eye and swelling of the eyelids.
Nerve Supply of Dura
- The branches of the trigeminal nerve supply the dura mater of the anterior and middle cranial fossae.
- The dura of the posterior cranial fossa is supplied by the vagus nerve and the meningeal branches of Cl to C3 spinal nerves.
Arterial Supply of Dura
Several branches of the following arteries supply the dura mater:
External carotid: Branches of the middle meningeal, ascending pharyngeal and occipital arteries.
Internal carotid
Subclavian: Vertebral branch of the subclavian artery
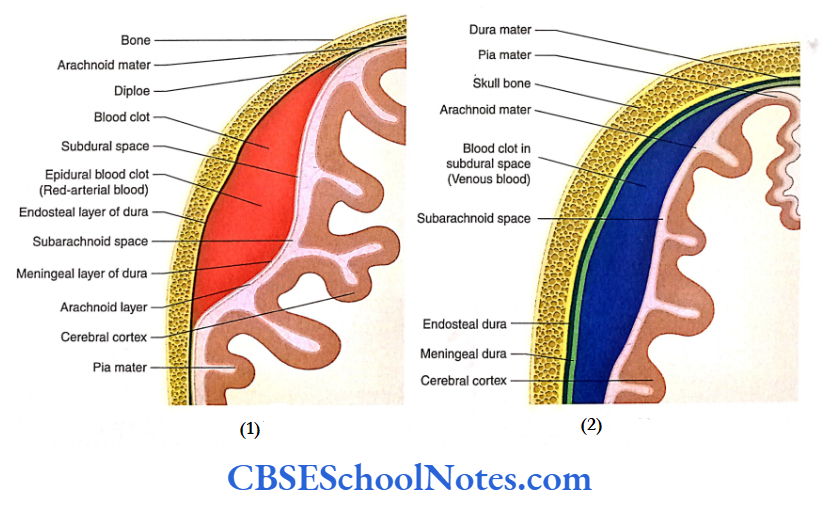
Extradural (Epidural) Haemorrhage
- Epidural haemorrhage occurs due to the rupture of meningeal vessels running between the endosteal and meningeal layers of the dura mater.
- The tear in the meningeal vessels is usually secondary to the fracture of the skull.
- The most common artery affected is the anterior branch of the middle meningeal artery and vein, which lies in the area of the pterion.
Subdural Haemorrhage
- The superior cerebral veins open into the superior sagittal sinus. Just before their opening in the sinus, they run for a short distance in the subdural space.
- Trauma to the head (forceful movement of the brain within the cranial cavity) may tear the superior cerebral vein(s). This results in the collection of blood in subdural space.
Arachnoid Mater
- Deep to dura mater, there lies a delicate, thin and almost transparent membrane known as arachnoid mater.
- It is separated from the dura mater by a capillary space which is called subdural space- it contains a thin film of fluid.
The subarachnoid space lies beneath the arachnoid mater, between the arachnoid and pia mater.
It is filled with CSF. The CSF acts as a buffer, which distributes and equalises the pressure on the surface of the brain.
A meshwork or filaments (trabeculae) extends through the fluid-filled subarachnoid space between the arachnoid and pia mater.
The arteries, veins and cranial nerves, while entering or leaving the brain, lie in the subarachnoid space.
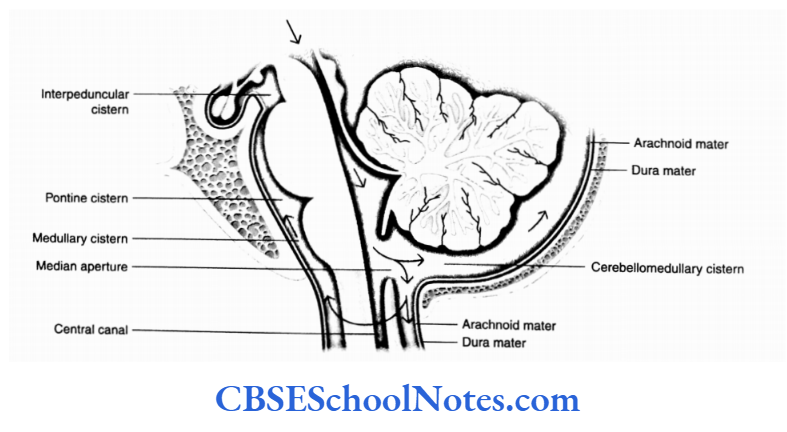
Subarachnoid Cisterns
The arachnoid mater forms bridges over sulci and other irregularities on the surface of the brain. In some situations, on the surface of the brain, the pia and arachnoid mater are widely separated from each other to form subarachnoid cisterns. Large cisterns are formed around the brainstem and cerebellum.
Cisterna Magna
Cisterna magna is the largest cistern and is also known as the cerebellomedullary cistern. It lies in the angle between the cerebellum and the medulla oblongata.
This cistern is continuous above the fourth ventricle through its median aperture and below the subarachnoid space of the spinal cord.
Cisterna Pontis
Cisterna pots lie anterior to the pons and medulla and contain vertebral and basilar arteries.
Cistnrna Intetrpeduncularis
Cisterna interpeduncularis lies between two cerebral
peduncles. It contains the circle of Willis.
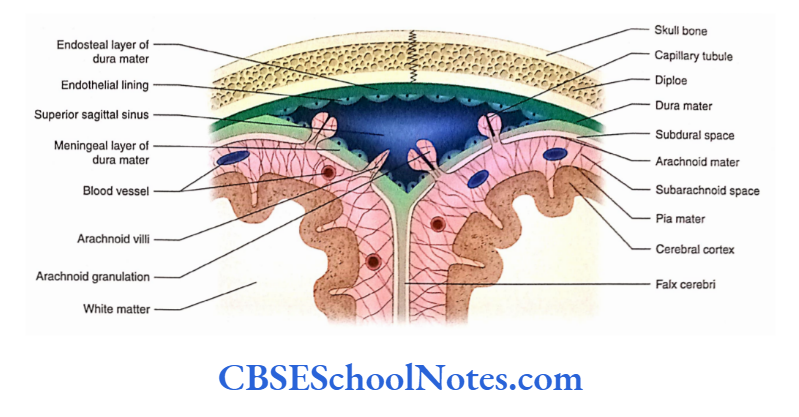
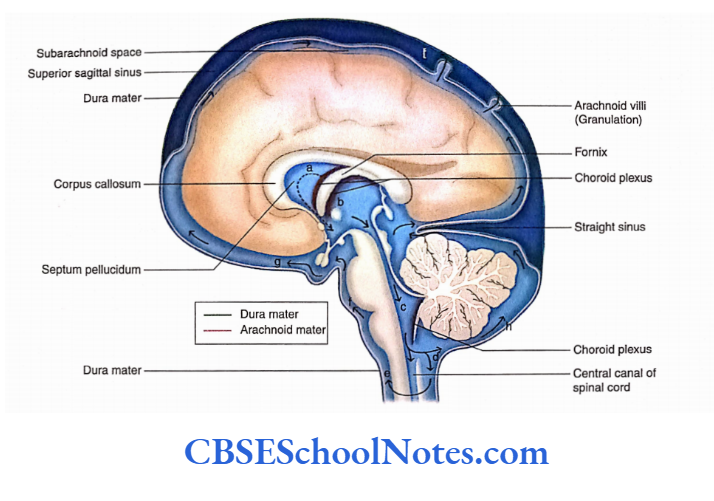
Arachnoid Villi and Granulations
Arachnoid villi arc minute finger-like elevations of arachnoid mater that project into the dural venous sinuses (especially the superior sagittal sinus) through apertures in dura mater. These act as channels of communication between the subarachnoid space and the dural venous sinus.
However, these capillaries (tubules) act as a valve or a one-way communicating channel for the escape of CSF into the venous blood.
The CSF from the subarachnoid space passes into the bloodstream of dural venous sinuses through these villi.
As the age advances, the arachnoid villi become large and globular in shape. These arachnoid villi are now known as arachnoid granulation.
Pia Mater
The pia mater is a delicate, thin membrane adherent to the surface of the brain, i.e. covering the gyri and sulci. It is made up of flattened mesothelial cells. There exists a microscopic subpial space between the pia and the brain.
The blood vessels present in the subarachnoid space anastomose with the neighbouring vessels on the surface of the pia before penetrating the pia mater. Thereafter, the blood vessels pass into the substance of the brain as end arteries.
At certain places, the wall of the ventricles of the brain is thin and only lined by ependyma. In this situation, the fold of the pia mater along with the blood capillaries invaginates into the ventricular cavities.
This invaginating vascular tuft is known as the choroid plexus of the ventricles. It is made up of (from outside to inside) ependyma, pia mater and blood vessels.
The pia mater of the choroid plexus is called tela choroidea. In the ventricles, the choroid plexus forms the CSF.
Meninges of the Spinal Cord
- Similar to the cranial meninges, the spinal meninges also consist of the spinal dura mater, arachnoid mater and pia mater.
- These tubular membranes cover the spinal cord and extend into the vertebral canal from the foramen magnum to the level of the second sacral vertebra.
Spinal Dura Mater
- The spinal dura mater is a tough fibrous membrane, which is continuous with the cranial dura at the level of the foramen magnum.
- Below, it narrows at the lower border of the S2 vertebra and covers the thin filum terminale. A the level of the coccyx, it blends with the periosteum covering the posterior aspect of the coccyx.
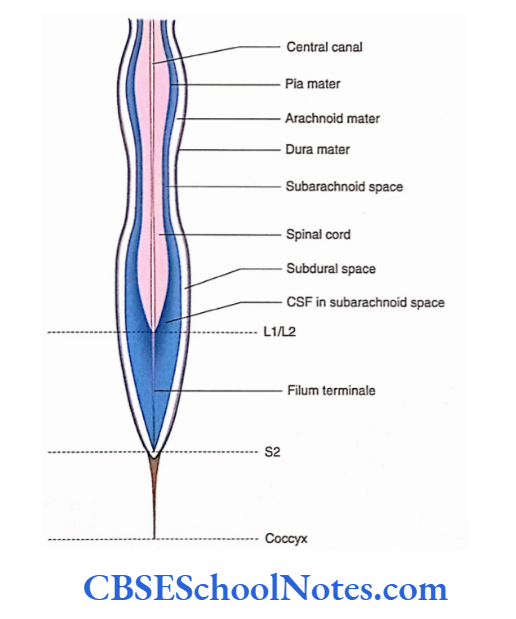
Arachnoid Mater
The arachnoid mater is the continuation of the cranial arachnoid mater. Similar to the dura, it also extends from the foramen magnum to the S2 vertebra where it blends with
the filum terminale.
Pia Mater
- The pia mater closely covers the spinal cord. Above, it is in continuation with the pia mater covering the brain. At the lower end of the spinal cord (conus medullaris), it covers the filum terminale.
- On each side of the spinal cord, the pia mater is present in the form of a fold. This fold is attached between the origin of dorsal and ventral spinal roots. It is known as ligamentum denticulatum.
Cerebrospinal Fluid
- The CSF is a clear, colourless liquid containing a small amount of protein, glucose and potassium and a large amount of sodium chloride.
- The CSF is present in the ventricles and subarachnoid space surrounding the brain and the spinal cord.
- It protects the brain and the spinal cord from physical injuries and carries oxygen and nutrients from blood to neurons and neuroglia.
Formation of the Cerebrospinal Fluid
The CSF is produced by choroid plexuses of the lateral, third and fourth ventricles. The net production of CSF is about 400-500 mL/day.
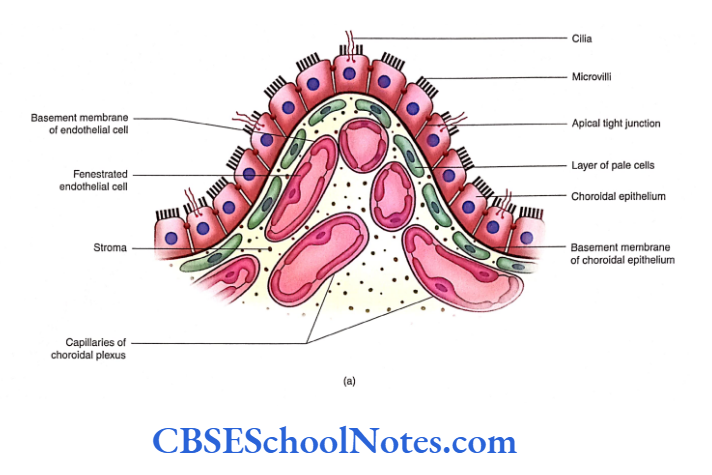
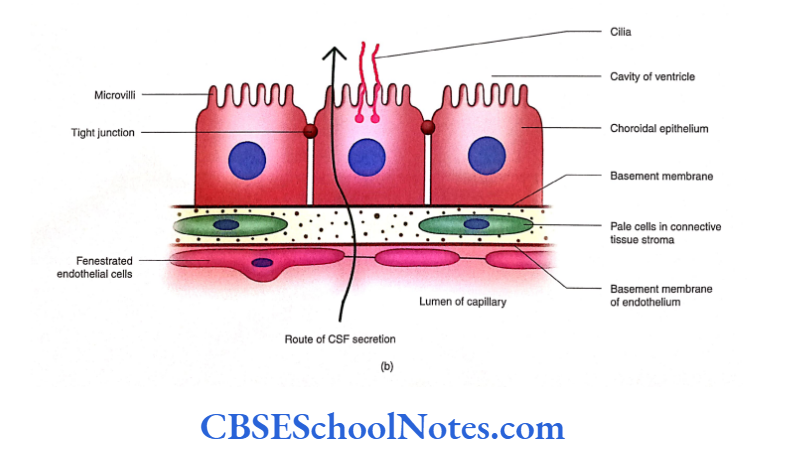
Blood-CSF Barrier
The choroid plexues are made up of a single layer of cuboidal epithelium (modified ependyma) enclosing an extensive capillary network embedded in the connective tissue stroma. Thus, the blood-CSF barrier is formed by the following structures:
- Endothelial cells which are fenestrated
- Basement membranes of endothelial cells
- Layer of pale cells and their processes (derived from pia mater)
- The basement membrane of the choroidal epithelium
- Choroidal epithelium (modified ependymal cells) with tight junctions
The CSF is formed due to the passage of materials through these barriers and also by active secretions from the choroidal epithelium.
The barrier protects the brain and spinal cord from potentially harmful blood-borne substances.
Circulation and Absorption of the Cerebrospinal Fluid
- After being produced by the choroid plexus, the CSF circulates through the ventricles ofthe brain, subarachnoid space and central canal of the spinal cord.
- The movement of the vertebral column and the pulsation of arteries present in the subarachnoid space assist the movement of CSF.
- The CSF is reabsorbed into the venous blood through arachnoid villi and granulation. Ependyma, arachnoid capillaries and lymphatics of meninges also absorb some CSF.
Functions of the Cerebrospinal Fluid
- The CSF surrounds the brain and the spinal cord; therefore, it serves as a cushion between the delicate nervous tissue and the surrounding cranial and vertebral bones.
- The CSF provides a medium for the exchange of nutrients and waste products between the nervous tissue and blood.
- By providing a medium for the exchange of nutrients and removal of waste products, the CSF maintains intracranial pressure.
- Certain hormones are transported by the CSF; for example, the secretion of the pineal gland is carried by the CSF to the pituitary gland.
Hydrocephalus
Hydrocephalus is defined as excessive collection of CSF leading to an increase in CSF pressure. High CSF pressure causes atrophic changes in the brain substance.
Hydrocephalus may be caused due to the following reasons:
Blockage in the normal circulation of CSF
In rare cases, it may also be due to excessive production of CSF as in the case of a tumour of choroid plexus Lumbar Puncture (Spinal Tap)
The CSF can be obtained for biochemical analyses by a procedure called lumbar puncture.
Lumbar puncture is sometimes also used to inject drugs into the subarachnoid space, for example, spinal anaesthesia.
The CSF is obtained by inserting a long needle into the lumbar subarachnoid space in the midline between the third and fourth lumbar spine.
Apart from lumbar puncture, CSF can also be obtained from cisternal puncture.
Summary
- The three meninges—dura mater, arachnoid mater and pia mater—are connective tissue membranes, which cover the brain and the spinal cord.
- Arachnoid and pia are collectively called leptomeninges.
- The cerebral dura mater consists of two layers:
- Endosteal and Meningeal.
- At places, the meningeal layer separates from the endosteal to form a double-layered fold known as ‘dural folds’. These folds or septa lie between the major parts of the brain, for example, falx cerebri and tentorium cerebelli.
- At places, the separation of meningeal and endosteal layers of dura encloses a triangular space. This space encloses
the ‘dural venous sinus’. - The extradural haemorrhage occurs between the endosteal and meningeal layers of the dura mater.
- Superior sagittal, cavernous and sigmoid sinuses are common sites of thrombosis.
- The arachnoid mater is a delicate, thin and transparent membrane.
- The cerebellomedullary cistern is the largest cistern, which lies at the angle between the cerebellum and the medulla oblongata.
- Arachnoid villi and granulations are minute projections of arachnoid mater into dural venous sinuses.
- The spinal cord is also covered by three meninges:
- Dura, Arachnoid and Pia mater
- The dura and arachnoid mater extend from the foramen magnum to the S2 vertebral level where they blend with the filum terminale.
- The pia mater closely covers the spinal cord, rootlets and filum terminale.
- CSF is produced in choroid plexuses, which are present in the ventricles of the brain.
- The fold of the pia mater along with blood capillaries invaginates into ventricular cavities. This invaginating vascular tuft is known as the choroid plexus of the ventricles.
- A blood-CSF barrier is formed by choroidal epithelium, a layer of pale cells and fenestrated capillary epithelium.
- The movement of CSF, in the spinal subarachnoid space, is assisted by the pulsation of the arteries which are situated around the spinal cord. The movement of CSF is also assisted by the movement of the vertebral column.
Multiple Choice Questions
Question 1. The delicate nervous tissue of the CNS is protected by the following structures except
- Bones
- Meninges
- Ligamentum denticulatum
- Cerebrospinal fluid
Answer: 3. Ligamentum denticulatum
Question 2. Which of the following is known as leptomeninges?
- Dura mater
- Arachnoid mater
- Dura and arachnoid mater
- Arachnoid and pia mater
- Pia mater
Answer: 4. Arachnoid and pia mater
Question 3. Which are the structures drained by dural venous sinuses?
- Cranial bones
- Brain
- Meninges
- All of the above
- Only b and c
Answer: 4. Only b and c
Question 4. The following are the paired dural venous sinuses except
- Cavernous
- Sigmoid
- Occipital
- Sphenoparietal
- Inferior petrosal
Answer: 3. Sphenoparietal
Question 5. The following facts about extradural haemorrhage are correct except
- Most commonly, it occurs due to rupture of the middle meningeal artery
- It is usually secondary to a fracture of the skull in the area of the pterion
- Blood collects between the endosteal and meningeal layers of dura mater
- The shape of the blood clot, in the CT scan, is biconcave
- The blood clot presses the lateral surface of the cerebrum
Answer: 4. The shape of the blood clot, in the CT scan, is biconcave
Question 6. Which are the subarachnoid cisterns surrounding the brainstem and cerebellum?
- Cerebellomedullary cistern
- Pontine cistern
- Medullary cistern
- Interpeduncular cistern
- All of the above
Answer: 5. All of the above
Auditory And Vestibular Systems Notes
Auditory And Vestibular Systems
- Hearing and equilibrium are two special somatic senses. The receptors for these two special senses are housed in a complex sensory organ, the membranous labyrinth.
- Encased in a bony labyrinth, the membranous labyrinth is situated in the internal ear.
- The cochlear part of the membranous labyrinth is concerned with auditory impulses. The vestibular part of the membranous labyrinth, on the other hand, has receptors for equilibrium.
Auditory System
The auditory impulses travel through the external ear, middle ear, and cochlear part ofthe internal ear. Thereafter, impulses travel through the cochlear nerve before finally reaching the cerebral cortex.
Read and Learn More Neuroanatomy
Cochlear Nerve
The cochlear nerve is predominantly a special somatic sensory nerve. It also contains a small motor (somatic efferent) component. Thus, it is a mixed nerve.
Sensory Component
- The cochlear nerve arises as the central processes (axons) of bipolar neurons of the spiral ganglion. Most of these fibers are myelinated.
- The nerve passes through the internal acoustic meatus along with the vestibular nerve.
- After coming out through the internal acoustic meatus, the nerve reaches the pontomedullary junction where it bifurcates to enter the brainstem.
- One branch of the cochlear nerve ends in the dorsal cochlear nucleus while the other ends in the ventral cochlear nucleus.
- The fibers of the nerve ending in both the nuclei in an orderly sequence (i.e. fibers responding to high frequencies terminate in dorsal regions and those of low frequencies in ventral regions).
Motor Component
- The outer and inner hair cells of the cochlea are innervated by cholinergic neurons of the superior olivary nuclei of both sides.
- The fibers after arising from the superior olivary nucleus of both sides form an olivocochlear bundle and travel through the cochlear nerve to the hair cells of the organ of Corti.
- The stimulation of efferent fibers inhibits auditory nerve response to acoustic stimuli (reduces the sensitivity of the ear).
- Central inhibition is necessary to suppress the background noise when attention is being paid to a particular sound.
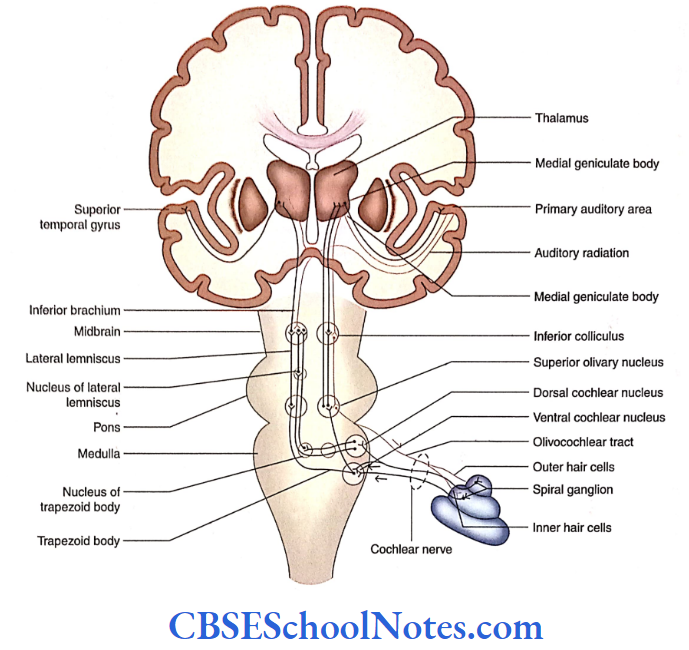
Location and Parts of Cochlear Nerve Nuclei
The cochlear nerve nucleus consists of two parts:
- Dorsal and
- Ventral cochlear nuclei.
These nuclei are situated on the dorsal and ventral aspects of the inferior cerebellar peduncle, respectively. These nuclei are located at the level of the pontomedullary junction.
Auditory Pathway
The impulses in the auditory pathway travel between the receptors and the auditory area of the cerebral cortex. The receptors in this case are the hair cells in the organ of Corti.
Sensory Neurons in the Auditory Pathway
The following sensory neurons are involved in the auditory pathway:
Bipolar neurons:
- The bipolar cells of spiral ganglia are first-order sensory neurons.
- The central processes of bipolar neurons form a cochlear nerve, which bifurcates to terminate in the dorsal and ventral cochlear nuclei on the same side.
Cochlear nuclei: The dorsal and ventral cochlear nuclei are the second-order sensory neurons in the auditory pathway.
Superior olivary nucleus:
- The neurons of the superior olivary nucleus consist of third-order sensory neurons.
- This nucleus is present in the lower pons at the level of the motor nucleus of the facial nerve.
- The nucleus of the trapezoid body and the nucleus of the lateral lemniscus are considered a part of the superior olivary nucleus and represent the third-order sensory neurons in the auditory pathway.
Inferior colliculus:
- The neurons of the inferior colliculus constitute fourth-order sensory neurons in the auditory pathway. The inferior colliculus is concerned with the integration of acoustic impulses.
Medial geniculate body: The neurons of the medial geniculate body (MGB) constitute the first-order sensory neurons in the auditory pathway.
Fibers of the Auditory Pathway
The nuclei in the auditory pathway are interconnected by fibers that form different bundles or tracts. These are as follows:
- Trapezoid body: The axons from the ventral cochlear nucleus run towards the ipsilateral superior olivary nucleus.
- Some of these fibers terminate here while others cross the midline to terminate in the opposite superior olivary nucleus.
- The crossing fibers of two sides form a prominent band called the trapezoid body.
- Lateral lemniscus: It is the ascending tract formed mainly by the axons of the superior olivary nucleus. This lemniscus contains both crossed and uncrossed fibers.
- The fibers of the lateral lemniscus make synaptic contact with the neurons of the inferior colliculus.
- Inferior brachium: The axons of the inferior colliculus travel in the inferior brachium to terminate in the MGB.
- Auditory radiation: The axons of the MGB form the auditory radiation, which travels in the sublentiform part of the internal capsule to reach the primary auditory cortex of the temporal lobe.
Cortical Area For The Auditory Pathway
- The primary auditory area (areas 41 and 42) is located on the floor of the lateral sulcus on the dorsal surface of the superior temporal gyrus.
- The recognition and interpretation of sound based on experience occur in the auditory association cortex. It is located posterior to the primary auditory cortex (areas 41 and 42).
Auditory Reflexes
The important auditor)’ reflexes are given in the following text.
Reflexes Turning of the Head and Conjugate Movement of the Eyes
- This occurs in response to a sudden loud sound. As indicated earlier, some fibers from the inferior colliculus connected to the superior colliculus.
- The superior colliculus through the tectospinal tract is connected with motor neurons innervating the neck muscles.
- Similarly, the collateral branches of the lateral lemniscus are connected with the nuclei of extraocular muscles via medial longitudinal fasciculus (MLF).
- These pathways are responsible for turning the head and conjugating the movement of eyes toward the source ofthe sudden loud sound.
Reflexes Reduction in Vibration of the Tympanic Membrane
- This occurs following a loud sound. The fibers of the superior olivary nucleus are in synaptic contact with the motor nuclei of 5 and 7 cranial nerves.
- The motor nuclei of these nerves innervate the tensor tympani and stapedius muscles, respectively.
- Following the loud sound, reflex contraction of tensor tympani and stapedius muscles occurs, which finally results in the reduction of vibration of the tympanic membrane and stapes (stapedius reflex).
- This reflex protects the delicate structures of the cochlea.
Vestibular System
- The vestibular system is concerned with the maintenance of equilibrium of the body and the fixity of gaze.
- Apart from the vestibular apparatus, the cerebellum plays an important role in the maintenance of the body equilibrium.
Vestibular Nuclei: Central Connections
The vestibular nuclei are present in the lower pons and upper medulla beneath the vestibular area of the floor of the ventricle.
The vestibular area consists offour vestibular nuclei:
Superior, Lateral, Medial, and Inferior.
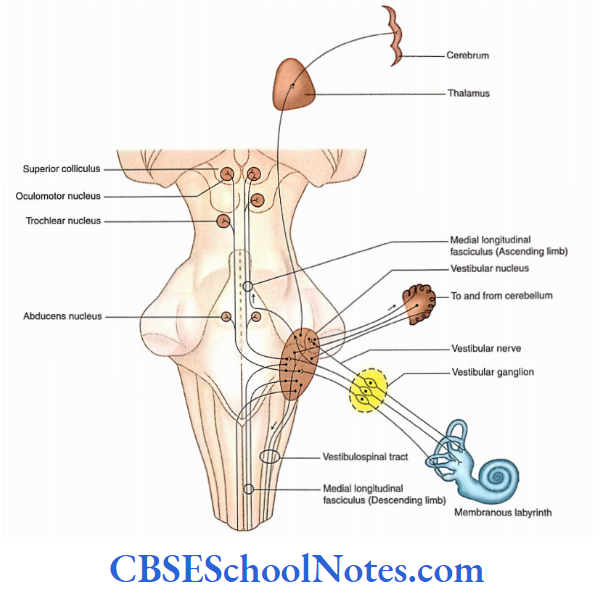
Afferent Connections of Vestibular Nuclei
- The vestibular nuclei receive afferents from vestibular receptors through the vestibular nerve, cerebellum, and vestibular nuclei of the opposite side.
- The vestibular pathway consists of first-order neurons (bipolar neurons), second-order neurons (vestibular nuclei), and third-order neurons (in the thalamus).
- The third-order neurons of this pathway project to the postcentral gyrus, the cortical area for vestibular sensation.
Efferent Connections of Vestibular Nuclei
The efferents from vestibular nuclei project to the cerebellum, brainstem (motor nuclei of cranial nerves), spinal cord, and cerebral cortex.
Vestibulospinal Tract
- The vestibulospinal tract originates from the cells of the lateral vestibular nucleus.
- The fibers of this tract are uncrossed and descend in the medulla dorsal to the inferior olivary nucleus and continue throughout the spinal cord in the ventral funiculus.
- The vestibulospinal fibers terminate in the anterior horn cells (motor neurons) that supply skeletal muscles.
- This tract is concerned with the maintenance of balance by regulating the tone of the muscles involved in posture.
Medial Longitudinal Fasciculus
- The axons of medial and inferior vestibular nuclei descend in the MLF (medial vestibulospinal tract) of both sides.
- These fibers travel through the floor ofthe fourth ventricle and medulla to terminate in the cervical part of the spinal cord.
- This tract influences the cervical motor neurons which move the head in such a way that equilibrium and fixation of gaze are maintained.
Medial Longitudinal Fasciculus Functions
- The vestibular nerve is concerned with conveying impulses associated with equilibrium The hair cells in the ampulla of the semicircular canal are sensors of kinetic balance (rotation of the head in any plane).
- The hair cells of the utricle are sensors of changes in gravitational forces, linear acceleration in the long axis of the body, and position of the head in space (i.e. static balance).
- The hair cells of the saccule are sensors of linear acceleration in the ventrodorsal axis of the body.
Stimulation of Labyrinth
- Vertigo is a sensation of movement in which the surrounding environment seems to revolve.
- It is a common symptom of the disease of the vestibular system. Probably, the cortical projections are responsible for the sense of vertigo.
Motion sickness: It is characterized by many symptoms such as nausea, headache, dizziness, and vomiting.
- This disease is caused due to motion during travel by road, sea, or air.
- Motion sickness occurs due to different messages received by the vestibular apparatus and eyes.
- For example, while traveling in a vehicle, the vestibular apparatus senses the motion but the eyes looking at the interior of the vehicle perceive it as still. These conflicting messages give the feeling of nausea.
Auditory And Vestibular Systems Summary
Hearing and equilibrium are two special somatic senses. The cochlear part of the membranous labyrinth is concerned with the reception of sound waves while the vestibular part of the labyrinth contains receptors for equilibrium.
Auditory system
- The cochlear nerve ends in dorsal and ventral cochlear nuclei.
- The axons of cochlear nuclei terminate on the superior olivary nucleus.
- The axons of the superior olivary nucleus form the lateral lemniscus.
- The lateral lemniscus ends on the neurons of the inferior colliculus whose fibers terminate on the medial geniculate body.
- The fibers of the medial geniculate body form auditory radiation which terminates on the auditory cortex.
Vestibular system
- The vestibular nuclei are present in the lower pons and upper medulla beneath the ‘vestibular area’ of the floor of the fourth ventricle.
- The vestibular part of the vestibulocochlear nerve ends in these nuclei.
- The afferent connectors of vestibular nuclei are from the vestibular nerve, from the cerebellum, and the opposite vestibular nuclei.
- The efferent connections of vestibular nuclei go to the cerebellum, brainstem, spinal cord, and cerebrum.
Auditory And Vestibular Systems Multiple Choice Questions
Question 1. Which of the following statements is false?
- Hearing and equilibrium are two special visceral senses
- The receptors for these two special senses are located in the membranous labyrinth
- The membranous labyrinth is located in the internal ear
- The cochlea is concerned with hearing
- The vestibular part of the membranous labyrinth has receptors for equilibrium
Answer: 1. Hearing and equilibrium are two special visceral senses
Question 2. Which of the following steps is false in the transmission of sound from the tympanic membrane to the cochlea?
- Vibration of the tympanic membrane
- Vibration of malleus, incus and stapes
- Vibration of the membrane covering the round window
- Vibration of perilymph of scala vestibule and scala tympani
- Vibration of the basilar membrane
Answer: 3. Vibration of perilymph of scala vestibule and scala tympani
Question 4. Which are the parts of a membranous labyrinth?
- Utricle
- Saccule
- Semicircular canals
- Cochlea
- All of the above
Answer: 1. Utricle
Question 5. Which of the following functional components are present in the cochlear nerve?
- General somatic efferent
- Special visceral efferent
- General somatic efferent
- Special somatic efferent
Answer: 3. General somatic efferent
Question 5. Which of the following ganglia/nuclei is not involved in the auditory pathway?
- Bipolar cells of the spiral ganglion
- Cochlear nuclei
- Inferior olivary nucleus
- Inferior colliculus
- Medial geniculate body
Answer: 3. Inferior colliculus
Question 6. Which of the following is not a part of the vestibular apparatus?
- Scala vestibule
- Utricle
- Saccule
- Semicircular ducts
Answer: 1. Scala vestibule
Question 7. The vestibular area consists ofthe following nuclei except
- Superior
- Inferior
- Medial
- Lateral
- Dorsal
Answer: 5. Dorsal
Neuroanatomy Visual System Notes
Visual System
The visual system is concerned with the special sense of vision. The visual system or the optic pathway begins from the retina in the eyeball and ends in the visual cortex of the occipital lobe
Optic Chiasma
The optic nerves of two sides cross and form optic chiasma. In optic chiasma, the fibres of the optic nerve arising from the nasal half cross to the opposite side while fibres from the temporal half do not.
Optic Tract
Each optic tract consists of crossed and uncrossed axons that project from optic chiasma to the lateral geniculate body (LGB) of that side. The optic tracts curve around the midbrain before they terminate in the LGB.
Each optic tract consists of fibres from the temporal half of the retina from the same eye and the nasal half of the retina from the opposite eye.
Read and Learn More Neuroanatomy
Retina
The retina is the innermost coat of the eyeball. The retina consists of a layer of pigmented epithelium, a layer of rods and cones, a layer of bipolar cells and a layer of ganglion cells.
Optic Nerve
The axons of ganglion cells form the optic nerve, and these fibres exit the eyeball at the optic disc’. As soon as optic nerve fibres come out of the sclera, they acquire a myelin sheath.
The optic nerve which has about 1 million fibres is surrounded by the meningeal layers, i.e. pia, arachnoid and dura.
The central artery and central vein of the retina are present in the anterior part of the optic nerve.
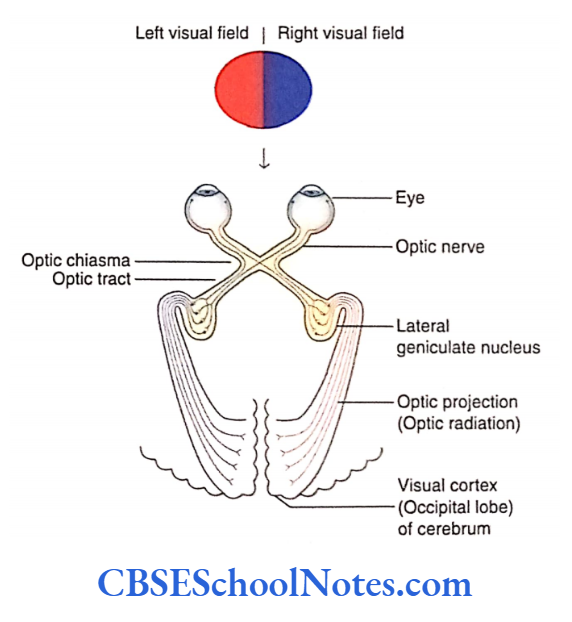
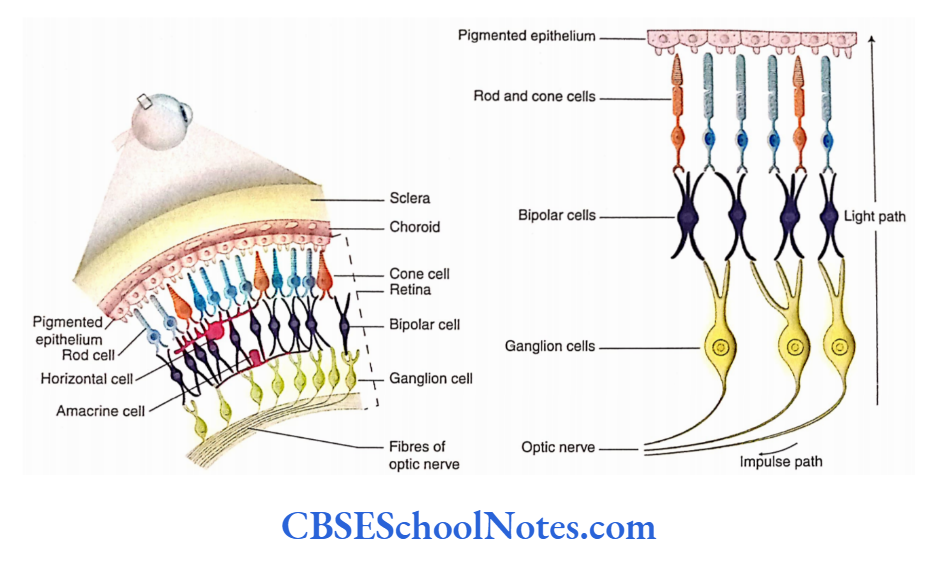
Lateral Geniculate Body
- The LGB is the main terminus for input to the primary visual cortex (striate cortex, area 17).
- The LGB is a small projection from the pulvinar part of the thalamus retina of the opposite side (crossed fibres) and terminates in layers 1, 4 and 6 while those from the ipsilateral retina (uncrossed fibres) end in layers 2, 3 and 5.
- The fibres from the temporal half of each retina terminate in the LGB of the same side while those from the nasal half terminate in the LGB of the opposite sides.
Geniculocalcarine Tract (Optic Radiation]
- The fibres arising from the LGB first traverse the sub lentiform and then the retrolentiform parts of the internal capsule.
- Thereafter, these fibres terminate in the visual cortex (area 17) ofthe same side. These fibres constitute the geniculocalcarine tract or the optic radiation.
Visual Cortex
The visual cortex consists of a primary area and an association area. The association area or the association cortex is involved in the recognition of objects and perception of colours, depth and motion.
Primary Visual Cortex
- The primary area or the primary visual cortex is an area where optic impulses reach the level of consciousness The visual cortex has a representation of the retina.
- The central part of the retina is represented on the occipital pole while its peripheral part is represented at the anterior part of the visual cortex.
Visual Association Cortex
The association cortex (areas 18 and 19) is involved in the recognition of objects and perception of colours, depth and motion. This is achieved by relating the present to past visual experience.
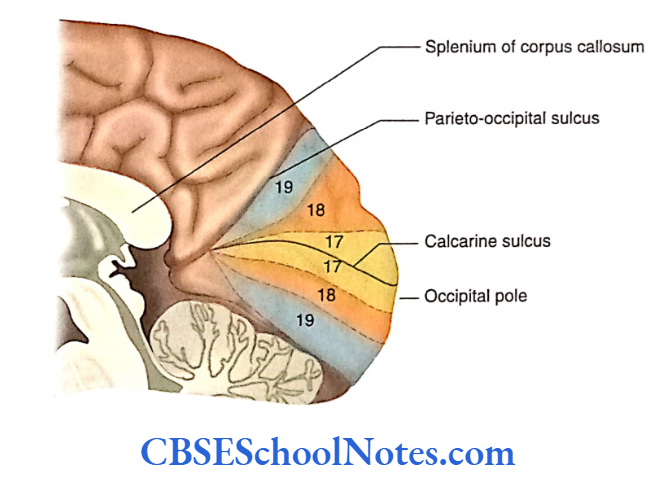
Visual Field
- The area seen by one eye, when one looks ahead with the eyes fixed, is the visual field of that eye. The visual field of each eye is divided into the nasal half and the temporal half.
- The light rays from an object situated in the temporal half of the visual field fall on the nasal half of the retina and the light rays from an object situated in the nasal half of the visual field fall on the temporal half of the retina.
- The upper half of the visual field projects onto the inferior half of the retina while the lower half of the visual field projects to the superior half of the retina.
- Therefore, damage to the upper retina will produce a deficit in the lower visual field. It should be noted that due to the presence of a convex lens in the eye, the visual image that is formed on the retina is inverted.
Visual Field Defects
- Visual field defects are characterised by the loss of a part of the normal area of vision in one or both eyes.
- The visual field defects may range from loss of area at the outer edges of vision (peripheral vision), or from a small blind spot or from a large area to complete blindness.
- Hemianopia means loss of vision in one half of the visual field. The visual defects may be caused by damage to any part of the visual pathway.
Reflexes Associated With Vision
Reflexes associated with vision include pupillary light reflex and accommodation reflex.
Pupillary Light Reflex
The pupillary light reflex includes both a direct response and a consensual response.
Direct Light Reflex
- When light is thrown on one eye with the help of a torch, it causes constriction of the pupil (iris) in that eye. This is known as direct response or direct light reflex.
- The pupillary constriction or the constriction of the constrictor muscles of the iris occurs due to stimulation of the Edinger-Westphal nucleus.
Consensual Light Reflex
Simultaneously with the direct light reflex, the pupil of the other eye also constricts. This is known as consensual response or consensual light reflex.
This reflex is seen because of the following two facts:
- Each retina sends afferent signals to the optic tracts of both sides. Fibres cross in the optic chiasma; these fibres later terminate in the pretectal nuclei of both sides.
- The pretectal nucleus of each side sends connections to the Edinger-Westphal nuclei of both sides.
Accommodation Reflex
After looking at a distance for some time and then looking at a near object, the visual responses that are observed are given in the following text.
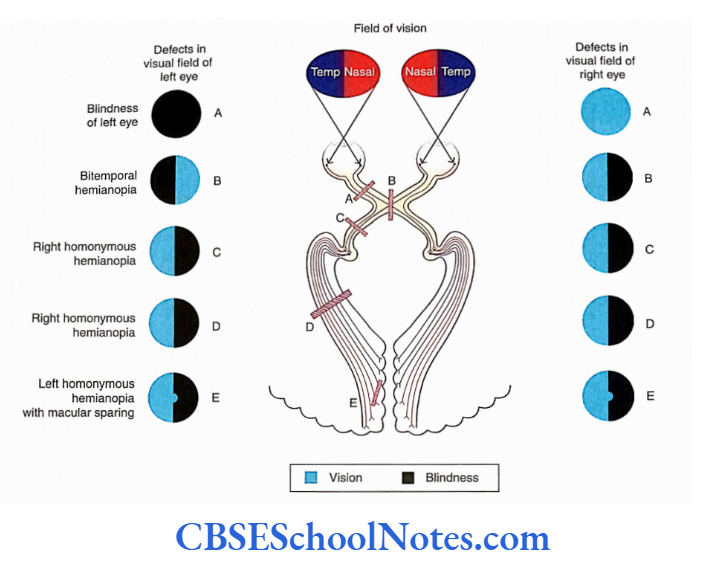
Ocular Convergence
When we look at a close object, our eyes must rotate medially to focus the light rays on the same corresponding points on both the retinas. This is achieved by the contraction of the medial recti muscles on both sides.
Accommodation
- As the eye focuses on close objects, the lens becomes more curved. This increase in curvature of the lens for the near vision is called accommodation.
- The accommodation is achieved through the contraction of the ciliary muscles.
- As a result of the contraction of ciliary muscles, the tension in the lens and suspensory ligaments is released and the lens therefore becomes more convex.
Constriction of Pupil
- Simultaneously with the accommodation and convergence, the pupil also constricts due to the constriction of circular muscle fibres of the iris.
- This helps to prevent the light rays from entering the eye through the periphery of the lens. This is needed to prevent blurring of vision and to achieve sharpness of image on the retina.
- The pathway of these responses observed during the accommodation reflex is illustrated.
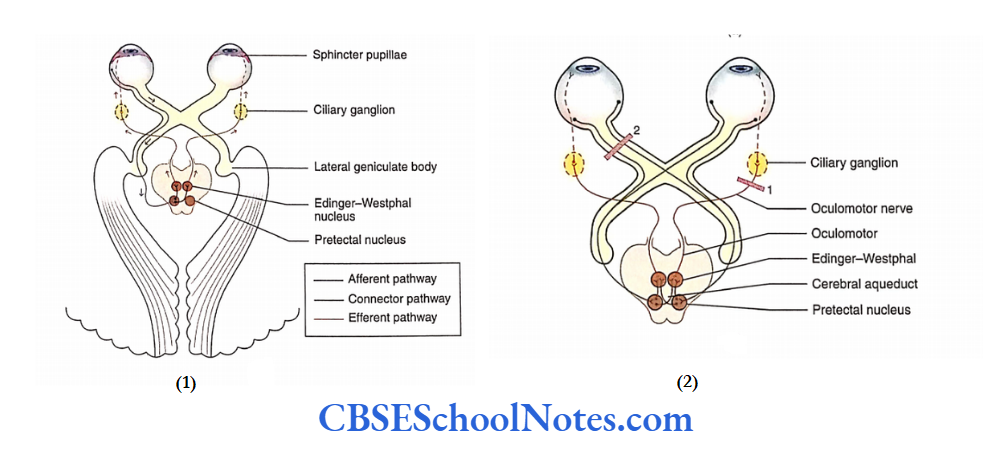
Argyll Robertson Pupil
- In certain central nervous system lesions (e.g. syphilis), the pupillary light reflex is abolished without affecting the accommodation reflex.
- This means that the constriction of the pupil after exposure to torch light gets abolished; however, constriction of the pupil occurs when the eyes are focused on a near object. The condition is known as Argyll.
- Robertson pupil. This indicates that the pathways of the light reflex and those of the accommodation reflex are different.
- In the case of light reflex, the pretectal nucleus and its axons are involved which are probably destroyed in syphilis (tabes dorsalis) due to dilatation of the cerebral aqueduct. On the other hand, the accommodation reflex involves the visual cortex and not the pretectal nucleus.
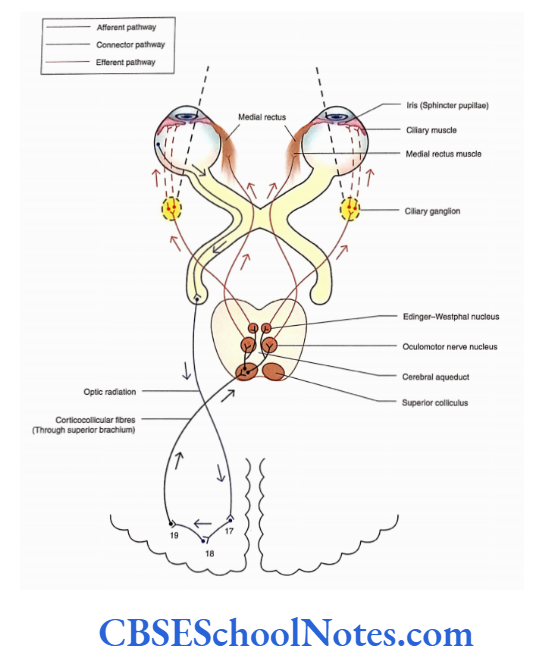
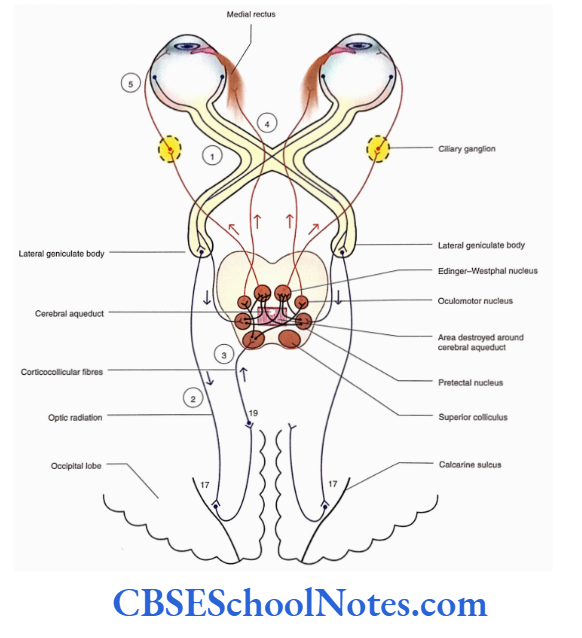
Visual System Summary
- The visual system is concerned with the special sense of vision.
- The retina contains rod and cone cells that convert stimuli of light into various electrical Impulses.
The retina consists of four layers:
- Pigment epithelial,
- Rods and cones,
- Bipolar cells and
- Ganglion.
- Rods are more sensitive to dim light while bright light stimulates cones.
- Bipolar cells are neurons connecting rods and cones with ganglion cells.
- The axons of ganglion cells form the optic nerve. The optic nerves of two sides now cross at optic chiasma to form optic tracts.
- The optic tracts curve around the midbrain and terminate in lateral geniculate bodies.
- The fibres arising from the lateral geniculate body terminate in the visual cortex (area 17) on the same side. There, fibres constitute optic radiation.
- The optical impulses reach the level of consciousness in the primary visual cortex (area 17).
- The association visual cortex (areas 18 and 1 9) is involved in the recognition of objects and perception of colours, depth and motion.
Visual System Multiple Choice Questions
Question 1. Which of the following cells are not present in the retina?
- Pigment epithelial cells
- Rods and cones
- Bipolar cells
- Ganglion cells
- Stellate cells
Answer: 5. Stellate cells
Question 2. Which of the following statements about rod cells is false?
- Each retina contains about 120 million rod cells
- Rods are absent in the central part of the fovea
- Rods are more sensitive to dim light
- Rods are involved in colour vision
- Rods are specialised for night vision
Answer: 4. Rods are involved in colour vision
Question 3. Which of the following facts about the macula lutea is false?
- It lies lateral to the optic nerve
- It lies along the visual axis of the eye
- Its central part is known as the fovea
- It contains only cone cells
- None of the above
Answer: 3. It contains only cone cells
Question 4. Which of the following statements about the optic nerve is false?
- The optic nerve is formed by the axons of ganglion cells of the retina
- The fibres of the optic nerve are myelinated
- These fibres come out of the sclera through the macula lute
- The optic nerve is surrounded by dura, arachnoid and pia mater
- The optic nerve has about 1 million fibres
Answer: 3. The optic nerve is surrounded by dura, arachnoid and pia mater
Question 5. Which of the following is not a part of the optic pathway?
- Optic nerve
- Optic chiasma
- Optic tract
- Medial geniculate body
- Geniculocalcarine tract
Answer: 3. Medial geniculate body
Question 6. Name the fibres received by the right geniculate body.
- From the temporal half of the right retina
- From the nasal half of the right retina
- From the temporal half of the left retina
- From the nasal half of the left retina
Answer: 1. From the temporal half of the right retina
Question 7. The visual association cortex (areas 18 and 19) is involved in which of the following functions?
- Recognition of object
- Perception of colour
- Depth of vision
- Motion
- All of the above
Answer: 3. Motion
Question 8. Which of the following responses is not associated with the accommodation reflex?
- Ocular convergence
- Accommodation
- Constriction of pupil
- Saccadic eye movements
Answer: 4. Saccadic eye movements
Brain Ventricles Anatomy Notes
Ventricles Of The Brain
- Ventricles of the brain are cavities that are present inside the brain. They are lined with ependyma and filled with cerebrospinal fluid (CSF).
- The ventricles are four in number and are named lateral ventricles (a pair) third and fourth.
- These CSFs flow from the lateral ventricles to the third ventricle and from the third to the fourth ventricle.
- The fourth ventricle is continuous with the subarachnoid space through openings in its roof (refer to Chapter 23 for circulation of CSF).
- The choroid plexus, which is responsible for the production of CSF, is present in all the cavities (ventricles).
Lateral Ventricle
- Each cerebral hemisphere has a cavity called the lateral ventricle, which consists of the anterior horn, body, posterior horn, and inferior horn.
- The central part or the body of the lateral ventricle is situated in the parietal lobe.
- The central part of the right and left lateral ventricles lies close to the median plane separated from each other by septum pellucidum.
- The anterior horn extends into the frontal lobe, the posterior horn extends into the occipital lobe and the inferior horn extends into the temporal lobe.
- Each lateral ventricle communicates with the third ventricle through the interventricular foramen.
- Central part
- Anterior horn
- Posterior horn
- Inferior horn
Central Part
Read and Learn More Neuroanatomy
The central part of the lateral ventricle extends J anteroposteriorly between the interventricular foramen and the splenium of the corpus callosum. The central part becomes continuous anteriorly with the anterior horn while posteriorly with the posterior and inferior horns. Moreover, the central part of the ventricle is triangular in cross-section and thus has three walls.
- Roof: It is formed by the undersurface of the corpus callosum.
- Floor: It is formed from the lateral to the medial side by the caudate nucleus, thalamostriate vein and stria terminalis, upper surface of the thalamus, choroid plexus and fornix.
- Medial wall: It is formed by the septum pellucidum.
Most medially, there is a slit-like space between the upper surface of the thalamus and fornix. ‘Ibis space is called a choroid fissure through which the choroid plexus invaginates the lateral ventricle.
Anterior Horn
The anterior horn is present anterior to the interventricular foramen and extends forwards, laterally and downwards in the frontal lobe of the brain. It is triangular in section and has
- Roof: Undersurface of corpus callosum
- Floor: Upper surface of the rostrum of the corpus callosum
- Medial wall: Septum pellucidum
- Lateral wall: Head of the caudate nucleus
- Anterior wall: Genu of corpus callosum.
Posterior Horn
The posterior horn extends backwards and medially into the occipital lobe
Roof and lateral wall: Tapetum of corpus callosum
Medial wall: Formed by two elevations, i.e. bulb of the posterior horn and calcar avis.
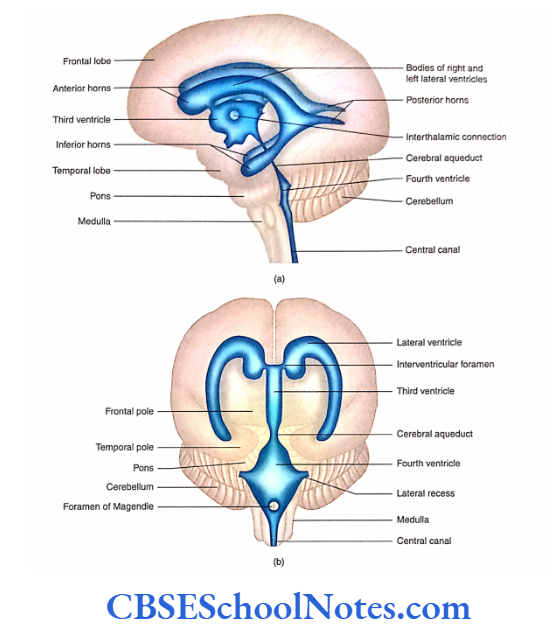
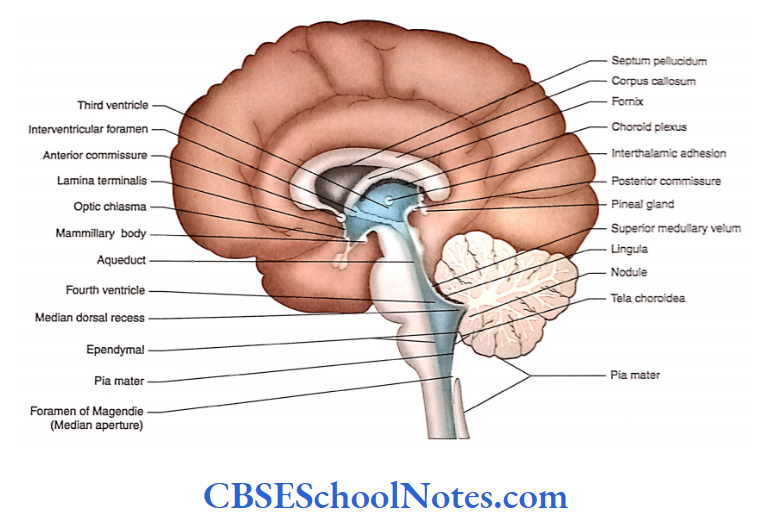
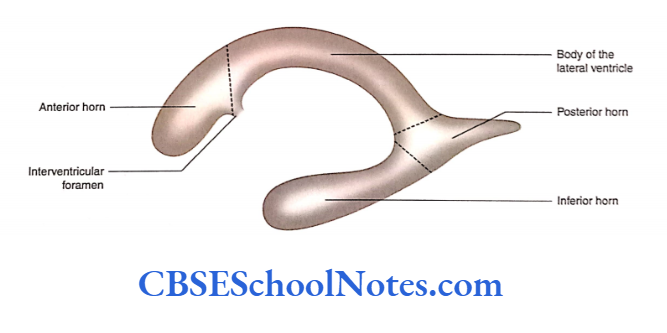
Inferior Horn
The inferior horn begins at the posterior end of the body ofthe lateral ventricle at the level ofthe splenium of the corpus callosum.
The inferior horn at first passes backwards and laterally and then passes downwards behind the thalamus into the temporal lobe.
In the temporal lobe, it takes a turn forward and ends in uncus. The inferior horn has a roof and a floor.
Roof: Above by stria terminalis and tail of caudate nucleus; below and laterally by tapetum. The amygdaloid nucleus lies in its anteriormost part of the roof.
Floor: Medially, it is formed by the hippocampus and laterally by collateral eminence.
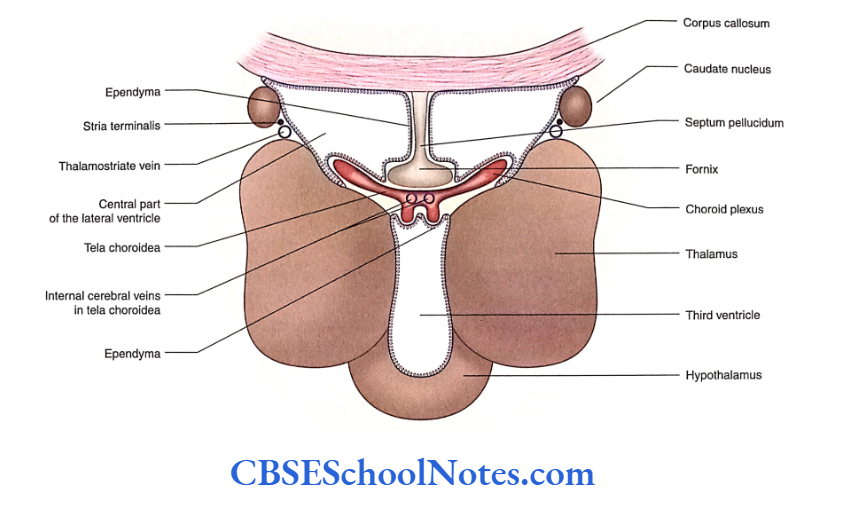
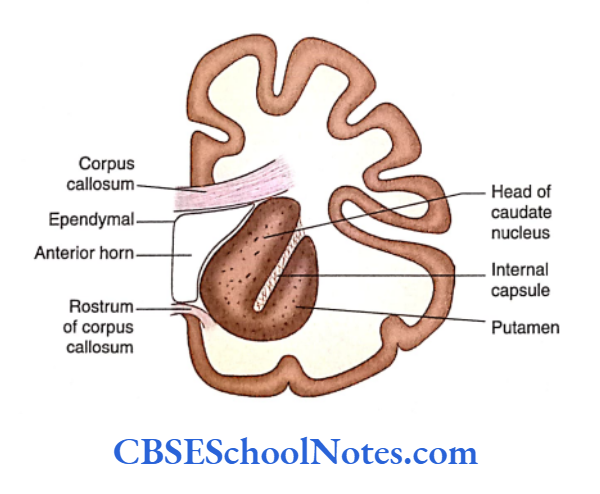
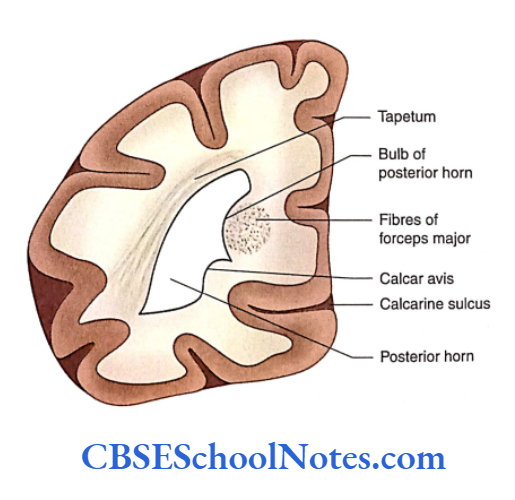
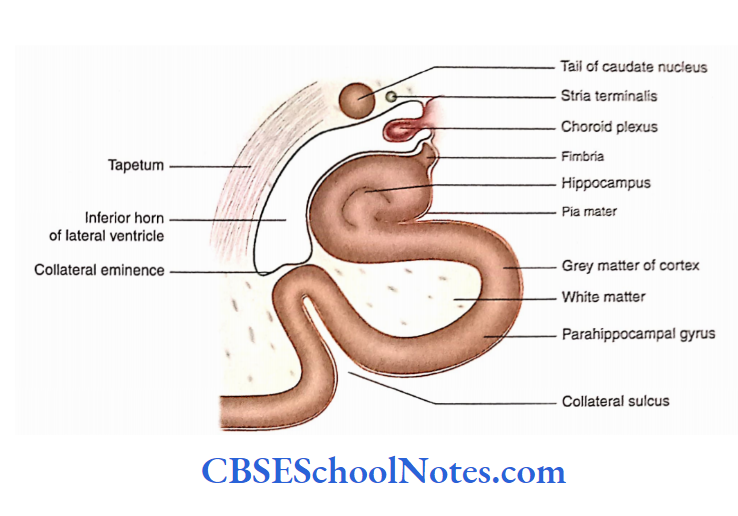
Third Ventricle
The third ventricle is a slit-like narrow space of diencephalon. It is situated between two thalami.
The cavity of the third ventricle communicates with the right and left lateral ventricles through the interventricular foramen. Posteriorly, the cavity communicates with the fourth ventricle through the cerebral aqueduct.
As the cavity is situated in the midline, it has two lateral walls. It also consists of an anterior wall, posterior wall, roof and floor.
Anterior Wall
The anterior wall is formed by the lamina terminalis, anterior commissure and anterior column of the fornix.
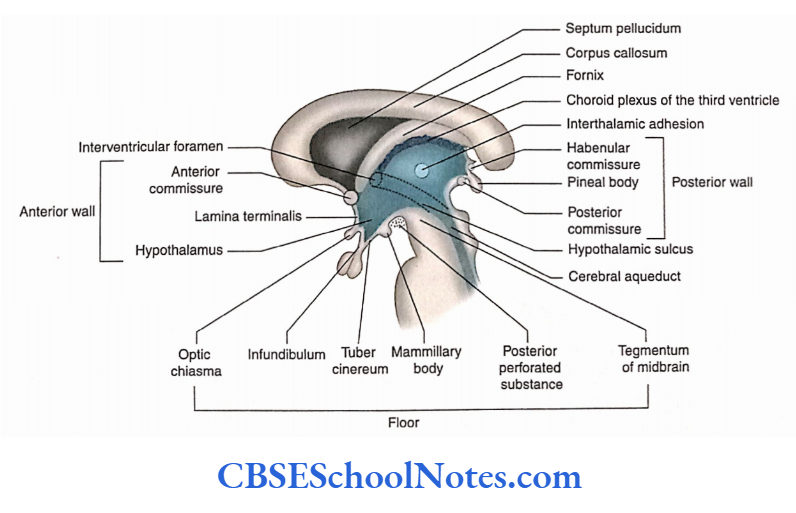
Lateral Wall
The lateral wall is large and is divided by the hypothalamic sulcus into an upper thalamic part and a lower hypothalamic part.
Two thalamines are usually connected by interthalamic adhesion.
Posterior Wall
From above downwards, it is formed by supraspinal recess, habenular commissure, pineal recess in the stalk of the pineal gland and posterior commissure.
Roof
The roof is formed by the ependyma stretching between two thalamis. From the roof two choroid plexuses protrude, one on either side of the median plane.
Floor
The floor is formed by the following structures as traced anteroposteriorly: optic chiasma, infundibulum, tuber cinereum, mammillary bodies, posterior perforated substance and tegmentum of midbrain Two recesses are seen in the floor.
These are the optic recess (above) and the optic chiasma) and infundibular recess (above the infundibular stalk).
Fourth Ventricle
The fourth ventricle is found in the hindbrain. Above, it communicates through the cerebral aqueduct with the third ventricle and below it communicates with the central canal of the closed part of the medulla oblongata.
The fourth ventricle lies in front of the cerebellum and behind the lower part of the pons and upper part medulla.
The cerebellum forms the roof of the fourth ventricle and its floor is formed by the pons and upper part of the medulla. The cavity of the fourth ventricle consists of a floor, roof
and lateral wall.
Floor
In the anatomical position, the floor of the fourth ventricle is the anterior wall of the ventricle. The shape of the floor is diamond shaped and hence sometimes called rhomboid fossa.
The floor is divided into upper and lower triangular parts by bundles of transversely running fibres (striaemedullaris)
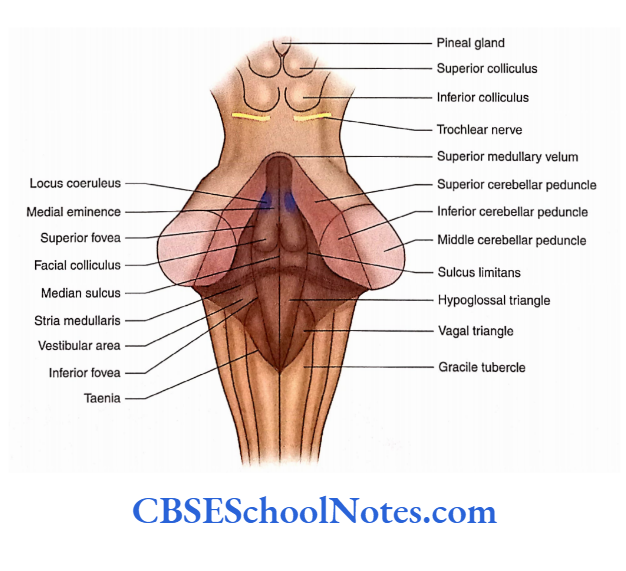
The upper triangular part is formed by the posterior surface of pons while the lower triangular part is formed by the posterior surface of the upper medulla.
Right and Left Halves
The floor of the ventricle is also divided into right and left halves by a median sulcus. On either side of the median sulcus, a longitudinal elevation is known as the median
or medial eminence.
Upper Part
- Immediately above the striae medullaris, on either side, the medial eminence shows a slight swelling known as facial colliculus. This swelling is produced due to fibres of facial nerve looping around the abducent nerve nucleus.
- At the upper level of the facial colliculus, there is a triangular depression—the superior fovea.
- Just above the superior fovea, the sulcus limitans ends in an area which is bluish and is called locus coeruleus.
- The bluish colouration is due to the presence of the melanin pigment present in the noradrenergic neurons of the nucleus coeruleus.
Lower Part
- The lower part of the floor, below the striae medullaris, shows the presence of two small triangles on either side of the median sulcus.
- These triangles are known as hypoglossal and vagal triangles.
- The vagal triangle is situated lateral to the hypoglossal triangle. The dorsal nucleus of the vagus and solitary nuclei lie deep in the vagal triangle.
- The hypoglossal nerve nucleus lies deep in the hypoglossal triangle.
- The lower part of the sulcus limitans close to the apex of the vagal triangle presents a depression—the inferior fovea.
Roof
The roof of the fourth ventricle is tent-shaped and projects posteriorly towards the cerebellum.
Upper Part
The upper part of the roof is formed on each side by superior cerebellar peduncles. The interval between these peduncles is bridged by a thin sheet of white matter—the superior medullary velum.
Lower Part
The lower part of the roof is formed, in small part, by the inferior medullary velum and in large part by tela choroidea.
- The right and left inferior medullary vela are present on each side of the nodule of the cerebellum. The inferior medullary velum is made up of a thin sheet of white matter and merges posteriorly in the white matter of the cerebellum.
- The inner surface of the inferior medullary velum is covered by ependyma while its outer surface is covered by pia mater.
- At the free margin of the inferior medullary velum, the ependyma and pia mater come close to each other and form the tela choroidea of the fourth ventricle. Thus, the lowest part of the roof of the fourth ventricle is membranous.
- Laterally, on either side, this membrane fuses with the inferior cerebellar peduncle.
- The lower part of this membrane presents a large median aperture (foramen of Magendie) through which the fourth ventricle communicates with the cerebellomedullary cistern.
- The roof also presents two lateral apertures through which the ventricle communicates with the subarachnoid space.
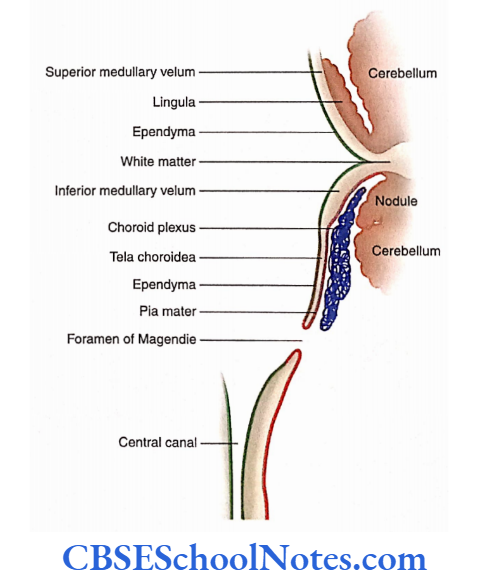
Lateral Walls
The upper part of the fourth ventricle is bounded laterally by the right and left superior cerebellar peduncles.
The lower part is bounded laterally by the right and left inferior cerebellar peduncles and gracile and cuneate tubercles.
Cavity of the Fourth Ventricle
The cavity of the fourth ventricle is somewhat diamond-shaped and lined by ependyma. It has superior, inferior and two lateral angles. The cavity communicates above with the third ventricle through the cerebral aqueduct.
Openings
- The fourth ventricle communicates below (at its inferior angle) with the central canal of the medulla oblongata.
- It has three openings in the roof—one median and two lateral through which it communicates with the subarachnoid space.
- Two lateral openings (foramina of Luschka), one on each side, lie in the lateral angle of the ventricle between the inferior cerebellar peduncle and the flocculus.
- Through this opening, the CSF escapes into the subarachnoid space. The choroid plexus of the fourth ventricle also protrudes through this opening.
Recesses
The cavity has many pouch-like protrusions which are known as recesses. It has a pair of lateral recesses, a single median dorsal recess and a pair of lateral dorsal recesses.
Summary
- Ventricles are CSF-filled cavities of the brain. These cavities are lined with ependyma.
- Each cerebral hemisphere contains a large C-shaped cavity known as a lateral ventricle.
Each lateral ventricle consists of a body and three horns:
- Anterior, Posterior and Inferior.
- The anterior horn extends into the frontal lobe, the posterior horn in the occipital lobe and the inferior horn in the temporal lobe.
- The third ventricle is situated in the midline and has two lateral walls, anterior wall, roof, floor and posterior wall. The cavity of the third ventricle communicates with the right and left lateral ventricles through the interventricular foramen. Below, it also communicates with the fourth ventricle through the cerebral aqueduct.
- The fourth ventricle is located between the brainstem and the cerebellum. It communicates below with the central canal.
- The floor of the fourth ventricle is diamond-shaped; hence, sometimes it is called rhomboid fossa. The fourth ventricle has three openings in the roof—one median and two lateral.
Multiple Choice Questions
Question 1. Following are parts of the lateral ventricle except
- The central part of the body
- Anterior horn
- Posterior horn
- Superior horn
- Inferior horn
Answer: 4. Superior horn
Question 2. Which of the following facts regarding the central part of the lateral ventricle is false?
- It extends between the interventricular foramen and the splenium
- It has three walls—roof, floor and medial wall
- The medial wall is formed by septum pellucidum
- The floor is formed by the thalamus and caudate nucleus
- None of the above
Answer: 5. None of the above
Question 3. Which of the following facts regarding the third ventricle is false?
- It is a slit-like narrow space of diencephalon
- It communicates with the lateral ventricle through the interventricular foramen.
- It communicates with the fourth ventricle through the central canal
- It has two lateral walls
Answer: 3. It communicates with the fourth ventricle through the central canal
Question 4. Which of the following structures is not seen in the floor of the fourth ventricle?
- Stria terminalis
- Median sulcus
- Median eminence
- Sulcus limitans
- Vestibular area
Answer: 1. Stria terminalis
Question 5. Which of the following structures are present in the roof of the fourth ventricle?
- Superior cerebellar peduncles
- Superior medullary velum
- Inferior medullary velum
- Tela choroidea
- All of the above
Answer: 5. All of the above