CBSE Class 12 Physics Chapter 9 Ray Optics And Optical Instruments Multiple Choice Questions And Answers
Question 1. For a thin convex lens when the height of the object is double its image, its object distance is equal to ________.
- f
- 2f
- 3f
- 4f
Answer: 3. 3f
⇒ \(m=\frac{f}{f-u}\)
⇒ \(-\frac{1}{2}=\frac{f}{f-(-u)}\)
⇒ -f-u = 2f
∴ |u| = 3f
Read and Learn More Important Questions for Class 12 Physics with Answers
Question 2. Which of the following is responsible for the glittering of diamonds?
- Interference
- Diffraction
- Total internal reflection
- Refraction
Answer: 3. Total internal reflection
Question 3. The focal length of a thin lens made from the material of a refractive index of 1.5 is 20 cm. When it is placed in a liquid of refractive index 4/3 its focal length will be _________ cm.
- 80.00
- 60.25
- 45.48
- 78.23
Answer: 4. 45.48
⇒ \(\frac{f_1}{f_a}=\left(\frac{_a \mu_g-1}{_l \mu_z-1}\right)\)
⇒ \(\frac{f_l}{20}=\frac{(1.5-1)}{\left(\begin{array}{l}
1.5 \\
1.33
\end{array}\right)}\)
∴ fl = 78.23 cm
Question 4. The radii of curvature of both sides of a convex lens are 15 cm and if the refractive index of the material of the lens is 1.5. Then the focal length of the lens in air is _________ cm.
- 10
- 15
- 20
- 30
Answer: 2. 15
⇒ \(\frac{1}{f_a}=\left(_a\mu_g-1\right)\left(\frac{1}{R_1}-\frac{1}{R_2}\right)\)
⇒ \(\frac{1}{f_a}=\frac{1}{2}\left(\frac{1}{15}-\frac{1}{-15}\right)\)
⇒ \(\frac{1}{f_a}=\frac{1}{2} \times \frac{2}{15}\)
∴ fa = 15 cm
Question 5. If the tube length of the astronomical telescope is 105 cm and the magnifying power is 20 for a normal setting, then the focal length of the objective is ________ cm.
- 10
- 20
- 25
- 100
Answer: 4. 100
Question 6. An object is placed at a distance of 25 cm on the axis of a concave mirror having a focal length of 20 cm. What will be the lateral magnification of an image?
- 4
- 2
- -4
- -2
Answer: 3. -4
⇒ \(m=\frac{f}{f-u}\)
⇒ \(\frac{-20}{-20-(-25)}=\frac{-20}{5}\)
∴ m = -4
Question 7. The depth of a filled well is II m and the refractive index of water is 1.33. If viewed normally from the top, by how much height would the bottom of the well appear to be shifted up?
- 2.73 m
- 11 m
- 4.13 m
- 1.37 m
Answer: 1. 2.73 m
⇒ \(h=\frac{H}{\mu}=\frac{11}{4} \times 3=\frac{33}{4}\)
Vertical shifted
⇒ \(H-h=11-\frac{33}{4}\)
∴ \(\frac{44-33}{4}=\frac{11}{4}=2.73 \mathrm{~m}\)
Question 8. In an optical fibre, the refractive index of the material of the core is _______ that of the cladding.
- Less than
- Higher than
- Equal to
- Half
Answer: 2. Higher than
Question 9. The lower half of the concave mirror’s reflecting surface is covered with an opaque (non – reflective) material. The intensity of the image of an object placed in front of the mirror becomes ________.
- Four times
- Half
- One fourth
- Double
Answer: 2. Half
Question 10. If the focal length of the converging lens is 0.25 m then the power of this lens is _____ dioptre.
- +2
- -4
- +4
- -2
Answer: 3. +4
∴ \(P=\frac{1}{f}=\frac{1}{0.25}=4 D\)
CBSE Class 12 Physics Chapter 9 Assertion And Reason
For question numbers 1 to 6 two statements are given-one labelled Assertion (A) and the other labelled Reason (R). Select the correct answer to these questions from the codes (1), (2), (3) and (4) as given below.
- Both A and R are true and R is the correct explanation of A
- Both A and R are true but R is NOT the correct explanation of A
- A is true but R is false
- A is false and R is also false
Question 1. Assertion: Critical angle is minimum for violet colour.
Reason: Because critical angle \(\theta_c=\sin ^{-1}\left(\frac{1}{\mu}\right) \text { and } \mu \propto \frac{1}{\lambda} \)
Answer: 1. Both A and R are true and R is the correct explanation of A
Question 2. Assertion: Within a glass slab a double convex air bubble is formed. This air bubble behaves like a converging lens.
Reason: The refractive index of air is more than the refractive index of glass.
Answer: 4. A is false and R is also false
Question 3. Assertion: A beam of white light gives a spectrum on passing through a hollow prism.
Reason: The speed of light outside the prism is different from the speed of light inside the hollow prism.
Answer: 4. A is false and R is also false
Question 4. Assertion: The microscope magnifies the image.
Reason: Angular magnification for images is more than one in the microscope.
Answer: 1. Both A and R are true and R is the correct explanation of A
Question 5. Assertion: Spherical aberration occurs in lenses of larger aperture.
Reason: The two types of rays, paraxial and marginal rays focus at different points.
Answer: 1. Both A and R are true and R is the correct explanation of A
Question 6. Assertion: The angle of minimum deviation for a prism is lesser for red light than that for blue light.
Reason: The refractive index of the material of a prism for blue light is greater than that for red light.
Answer: 1. Both A and R are true and R is the correct explanation of A
CBSE Class 12 Physics Chapter 9 Short Question And Answers
Question 1. Light from a point source in the air falls on a convex spherical glass surface with a refractive index of 1.5 and a radius of curvature of 20 cm. The distance of the light source from the glass surface is 100 cm. At what position is the image formed?
Answer:
Given: 1 = 1, 2 = 1.5, R = 20cm. u = -100 cm
Form \(\frac{\mu_2}{v}-\frac{\mu_1}{u}=\frac{\mu_2-\mu_1}{R} \Rightarrow \frac{1.5}{v}-\frac{1}{-100}=\frac{0.5}{20}\)
⇒ \(\frac{1.5}{v}=\frac{5}{200}-\frac{1}{100}=\frac{3}{200} \text { or } v=100 \mathrm{~cm}\)
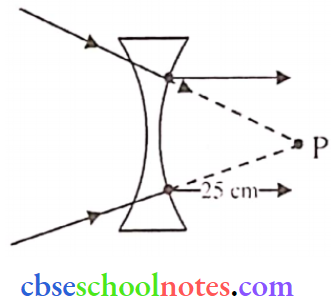
Question 2. A beam of light converges at a point P. A lens is placed in the path of the beam at a distance of 25 cm from P. The final image is formed at infinity. Calculate the power of the lens.
Answer:
So, u = 25 cm, v = ∞
⇒ \(\mathrm{f}=-25 \mathrm{~cm}=-\frac{25}{100} \mathrm{~m}=-\frac{1}{4} \mathrm{~m}\)
∴ \(P=\frac{l}{f}=-4 D\)
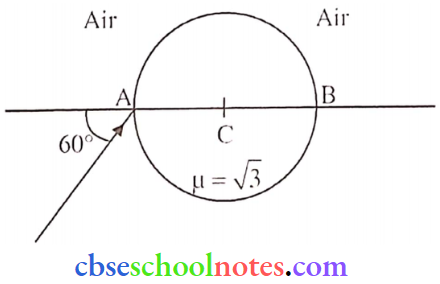
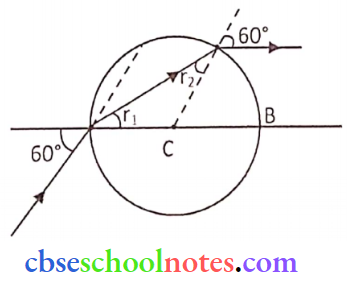
Question 3. A ray of light falls on a transparent sphere of μ = √3 at an angle of incidence 60° with the diameter AB of the sphere having centre C. The ray emerges from the sphere parallel to the line AB. Find the angle of emergence.
Answer:
⇒ \(\mu=\frac{\sin i}{\sin r_1}\)
⇒ \(\sqrt{3}=\frac{\sin 60^{\circ}}{\sin r_1}\)
⇒ \(\sin r_1=\frac{\sqrt{3}}{2} \times \frac{1}{\sqrt{3}}\)
r1 = 30°
i.e. r1 = r2 = 30° so, e = 60° [angle of emergence]
Question 4.
- Explain briefly how the focal length of a convex lens changes with an increase in the wavelength of incident light.
- Explain briefly how the focal length of a convex lens changes when it is immersed in water. The refractive index of the material of the lens is greater than that of water.
Answer:
1. From \(\mu=\frac{\mathrm{c}}{\mathrm{v}}=\frac{\mathrm{c}}{\mathrm{v \lambda}}\)
Here, refractive index \(\mu \propto \frac{1}{\lambda}\)
So, (.t of a lens increases with the decrease in wavelength of the incident light.
From \(\frac{1}{f}=(\mu-1)\left(\frac{1}{R_1}-\frac{1}{R_2}\right)\)
We can say focal length will increase with the increase in wavelength and vice versa.
2. From, \(\frac{1}{f}=\left(\frac{\mu_2}{\mu_1}-1\right)\left[\frac{1}{R_1}-\frac{1}{R_2}\right]\) 2 (lens) = 1.5, 1 (Water) = 1.33
⇒ \(\frac{1}{f}=\left(\frac{1.5}{1.33}-1\right)\left[\frac{1}{R_1}-\frac{1}{R_2}\right]\) When lens placed in water
Clearly \(\left(\frac{\mu_2}{\mu_1}\right)\) decreases which means focal length increases.
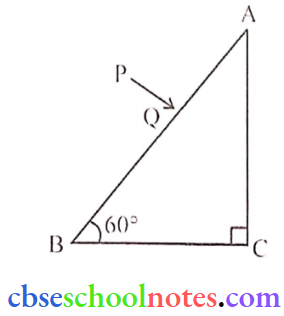
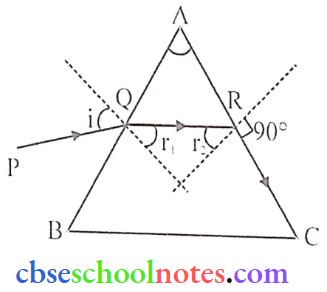
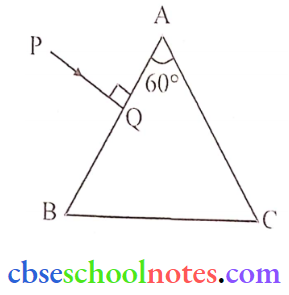
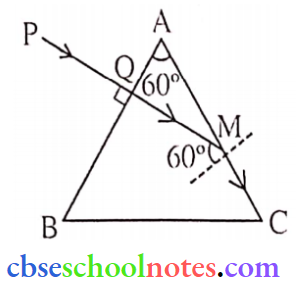
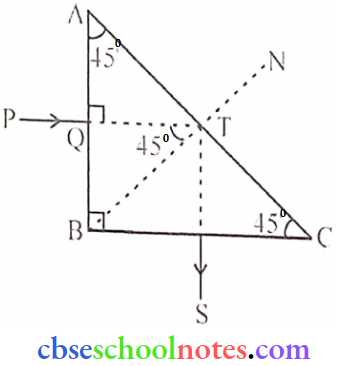
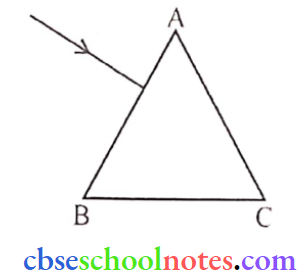
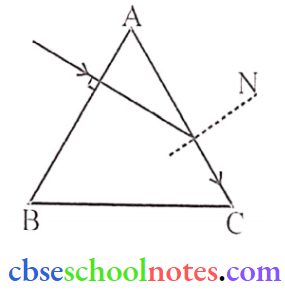
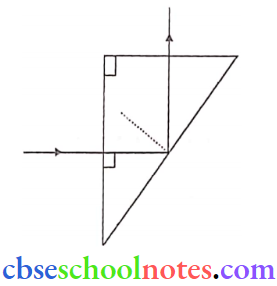
Question 5. A ray PQ incident normally on the refracting face BA is refracted in the prism BCA made of material of refractive index 1.5. Complete the path of the ray through the prism. From which face will the ray emerge?
Answer:
Refractive index (μ) = 1.5 (given)
Ray PQ will go straight in ΔBAC as it falls normally on the surface BA. From the condition of TIR.
⇒ \(\sin \mathrm{i}_C=\frac{1}{\mu}=\frac{1}{1.5}=\frac{2}{3}=0.66\)
or ic = 42° (∵ sin 42° = 0.66)
⇒ \(\frac{\sin i}{\sin r}=\frac{\mu_2}{\mu_1}=\frac{2}{3}\)
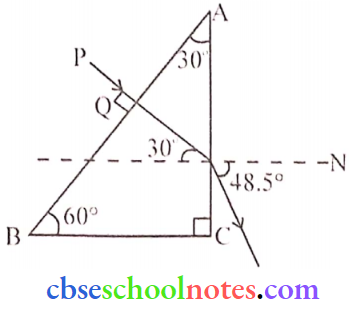
or \(\frac{\sin 30^{\circ}}{\sin r}=\frac{2}{3}\)
or sin r = 0.75
or r = 48.5° (∵ sin 48.5° = 0.75)
So ray PQ will emerge from surface AC at an angle = 48.5°
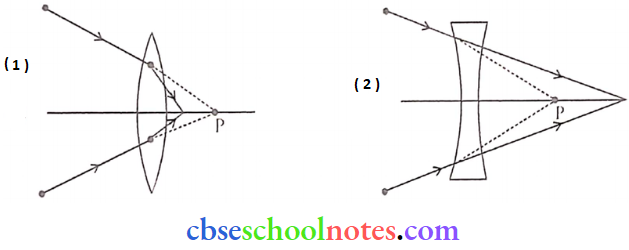
Question 6. A beam of light converges at a point P. Draw ray diagrams to show where the beam will converge if
- A convex lens, and
- A concave lens is kept in the path of the beam.
Answer:
Question 7. A coin is placed inside a denser medium. Why does it appear to be raised? Obtain an expression for the height through which the object appears to be raised in terms of the refractive index of the medium and real depth.
Answer:
Because of Refraction, it appears to be raised.
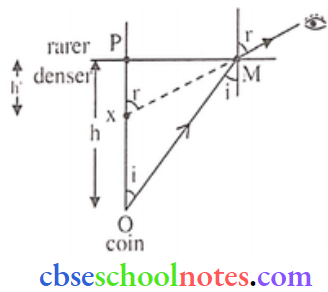
⇒ \(\Delta \mathrm{OMP} \rightarrow \sin i=\frac{\mathrm{MP}}{\mathrm{OM}}\)
⇒ \(\Delta \mathrm{XMP} \rightarrow \sin r=\frac{\mathrm{MP}}{\mathrm{XM}}\)
So, \(\text { So, }{ }_d \mu_r=\frac{\sin i}{\sin r}=\frac{X M}{O M}\)
If M and P are closer, then XM ≅ XP = h’ (Apparent depth), OM = OP = H (Actual Depthdepth)
⇒ \({ }_d \mu_r=\frac{h^{\prime}}{h}\)
⇒ \(\frac{1}{{ }_r \mu_d}=\frac{h^{\prime}}{h}\)
∴ \(h^{\prime}=\frac{h}{\mu}\) (\(\left[d \mu_r=\frac{1}{\mu_d}=\frac{1}{_r\mu_1}\right]\))
Thus the height (vertical shift) through which, the object appears to be raised
∴ \(\Delta=h-h^{\prime}=h\left(1-\frac{1}{\mu}\right)\)
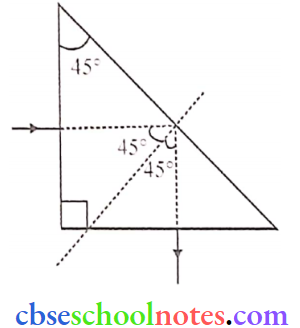
Question 8. Under what conditions does the phenomenon of total internal reflection lake place? Draw a ray diagram showing how a ray of light deviates by 90° after passing through a right-angled isosceles prism.
Answer:
Conditions:
- The light must move from a denser to a rarer medium.
- The angle of incidence must be greater than the critical angle.
Question 9. State, with the help of a ray diagram, the working principle of optical fibres. Write one important use of optical fibres.
Answer:
Working principle of optical fibres: Optical fibres are extensively used for transmitting audio and video signals in the form of light from one end to another based on multiple total internal reflections at the interface of inner and outer layers which are known as core and cladding.
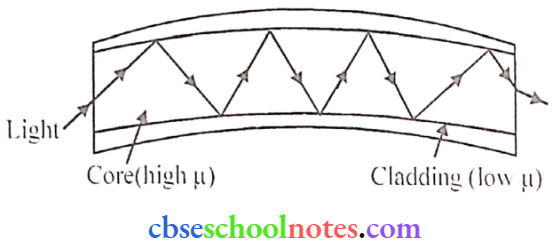
Use: Used in visual examination of Internal organs like the stomach and intestine by the endoscopy in medical Science
Question 10. Which two aberrations do objectives of refracting telescope suffer from? How are these overcome in reflecting telescopes?
Two Aberrations: Spherical aberration & chromatic aberration. Spherical aberration in mirrors is corrected by using parabolic mirrors and in lenses it is corrected by using a lens with a small aperture or one side plane.
Chromatic aberration is reduced by using an achromatic combination of lenses in which materials with differing dispersive properties arc assembled to form a compound lens.
Question 11. A compound microscope consists of an objective lens of focal length 2 cm and an eyepiece of focal length 6.25 cm separated by a distance of 15 cm. How far from the objective should an object be placed to obtain the final image at the least distance of distinct vision (25 cm)? Calculate the magnifying power of the microscope.
Answer:
f0 = 2cm. fe = 6.25 cm. d = 15 cm. D = 25 cm. ve = -25 cm
⇒ \(\frac{1}{f_e}=\frac{1}{v_e}-\frac{1}{u_e} \Rightarrow \frac{1}{6.25}=\frac{1}{-25}-\frac{1}{u_e} \Rightarrow u_e=-5 \mathrm{~cm}\)
So. the image distance for the objective lens
v1 = d – ue = 15 – 5 = 10cm
Now again
⇒ \(\frac{1}{f_0}=\frac{1}{v_0}-\frac{1}{u_0} \Rightarrow \frac{1}{2}=\frac{1}{10}-\frac{1}{u_0} \Rightarrow u_0=-2.5 \mathrm{~cm}\)
Magnifying Power
⇒ \(m=\frac{-v_0}{u_0}\left(1+\frac{D}{f_c}\right)=\frac{10}{2.5}\left(1+\frac{25}{6.25}\right)\)
m = 20
Question 12.
- An object approaches a converging lens with a uniform speed of 5 m/s and slops at the focus. How- will the image move for the lens? Specify its nature.
- In a simple microscope, a convex lens of focal length 5 cm is used. Calculate the magnifying power when the object is placed at the focus of the lens.
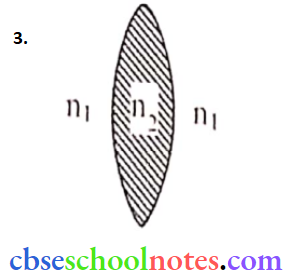
- What is the power of a biconvex lens of refractive index n2 dipped in a liquid of refractive index n1? where n1 < n2?
Answer:
1. Moves away from the lens with a non-uniform speed.
For example: If f = 20 m,
u = -50m. -45m, -40m. -34m
v = 33.3m, 36m. 40m, 46.7m [by using lens formula]
2. \(m=\frac{D}{f}=\frac{25}{5}=5\)
The lens behaves as a convex lens
⇒ \(\mathrm{P}=\frac{1}{\mathrm{f}}=\left(_1\mathrm{n}_2-1\right)\left(\frac{1}{\mathrm{R_1}}-\frac{1}{\mathrm{R}_2}\right)\)
⇒ \(P=\left(\frac{n_2}{n_1}-1\right)\left(\frac{1}{R_1}-\frac{1}{R_2}\right)\)
1n2 < an2 (∵ n1 can not be less than 1 )
So. Focal length will increase. power will decrease.
Question 13. Draw a labelled ray diagram of a refracting telescope. Deduce an expression of magnifying power of it. Write two main limitations of a refracting-type telescope or a reflecting-type telescope.
Answer:
Refracting Telescope:
Refracting type telescope consists of an objective lens of large aperture and large focal length whereas an eyepiece is of small aperture and small focal length.
Magnifying Power:
It is the ratio of visual angle substandard by the final image at the eye to the visual angle subtended by an object.
⇒ \(M=\frac{\beta}{\alpha} \quad\left\{\begin{array}{l}
\text { if } \alpha \text { and } \beta \text { are very small } \\
\alpha \approx \tan \alpha \text { and } \beta \approx \tan \beta
\end{array}\right.\)
⇒ \(M=\frac{\tan \beta}{{tan} \alpha} \Rightarrow M=\frac{\left(\frac{A^{\prime} B^{\prime}}{O_2 B^{\prime}}\right)}{\left(\frac{A^{\prime} B^{\prime}}{O_1 B^{\prime}}\right)} ⇒ M=\frac{O_1 B^{\prime}}{O_2 B^{\prime}}=\frac{-f_0}{u_e}\)
⇒ \(M=\frac{-f_0}{u_e}\) (1)
1. When the final image is formed at least a distance of distinct Vision (Ve = D)
Applying lens formula for eyepiece:
⇒ \(\frac{1}{f_e}=\frac{1}{v_e}-\frac{1}{u_e} \quad\left\{\begin{array}{l}
\text { applying sign convention } \\
v_e=-D . \quad u_e=-u_e
\end{array}\right.\)
⇒ \(\frac{1}{f_e}=-\frac{1}{D}+\frac{1}{u_e} \Rightarrow \frac{1}{u_e}=\frac{1}{f_e}+\frac{1}{D} \Rightarrow \frac{f_0}{u_e}=f_0\left(\frac{1}{f_e}+\frac{1}{D}\right) \Rightarrow \frac{f_0}{u_e}=\frac{f_0}{f_e}\left(1+\frac{f_e}{D}\right)\)
Hence magnifying power from eq (1)
∴ \(M=-f_0\left[\frac{1}{f_e}+\frac{1}{D}\right]\)
2. When the final image is formed at infinity (ue = fe )
From eq. (i)
∴ \(M=\frac{-\mathrm{f}_0}{\mathrm{f}_e}\)
Drawbacks of refracting telescope:
- A defect of chromatic aberration occurs in refracting-type telescopes.
- It has a small resolving power
Question 14.
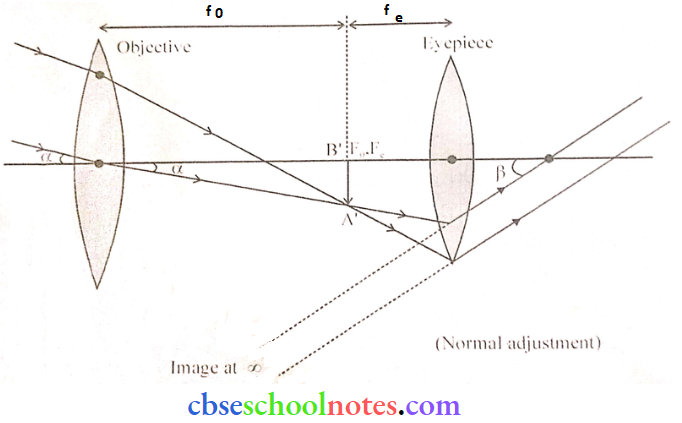
- Draw a ray diagram depicting the formation of the image by an astronomical telescope in normal adjustment.
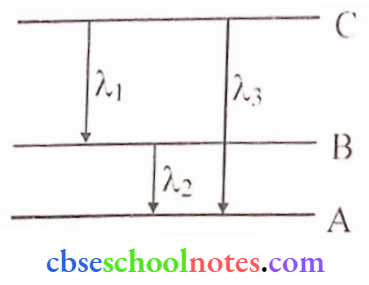
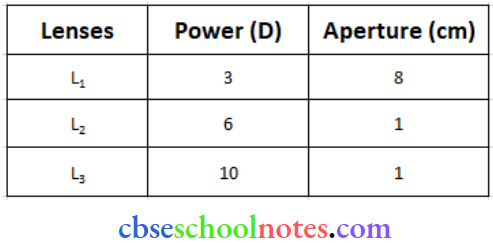
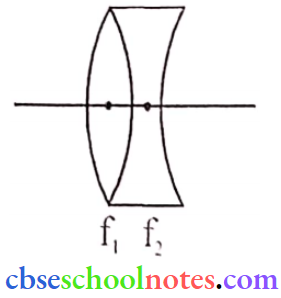
- You are given the following three lenses. Which two lenses will you use as an eyepiece and as an objective to construct an astronomical telescope? give reason.
Answer:
2. ‘L1‘ is used for an objective as it has the largest focal length which is needed, \(M_0=\frac{f_0}{f_e}\) for better-magnifying power. ‘L3‘ is Used for an eyepiece to get better angular magnification, as from \(M_{0}=\frac{f_{0}}{f_e}\) least fe is needed.
Question 15.
- A convex lens of focal length 30 cm is in contact with a concave lens of focal length 20 cm. Find out if the system is converging or diverging.
- Obtain the expression for the angle of incidence of a ray of light, which is incident on the face of a prism of refracting angle A so that it suffers total internal reflection at the other face. (Given, the refractive index of the glass of the prism is μ.)
Answer:
1. Focal length of convex lens f1 = 30 cm
the focal length of the concave lens f2 = -20 cm
Equivalent focal length of combination
⇒ \(\frac{1}{f}=\frac{1}{f_1}+\frac{1}{f_2} \Rightarrow \frac{1}{f}=\frac{1}{30}-\frac{1}{20} \Rightarrow \frac{1}{f}=-\frac{1}{60} \Rightarrow f =-60 \mathrm{~cm}\)
The system is diverging.
2. For total internal reflection.
⇒ \(\sin i_c=\frac{1}{\mu}\)
For Prism we know that
r1 + r2 = A and r2 = ic
∴ r1 = A -ic
Applying Snell’s law at point ‘Q’
∴ \(\frac{\sin i}{\sin f_i}=\mu\)
sin i = μ sin r1 ⇒ sin i = μ sin (A- ic)
i = sin-1 |μ sin-(A-ic)|
Question 16.
- Name the phenomenon on which the working of an optical fibre is based.
- Draw a labelled diagram of an optical fibre and show how light propagates through the optical fibre using this phenomenon.
Answer:
1. Total internal reflection (TIR)
Question 17.
- A screen is placed at a distance of 100 cm from an object. The image of the object is formed on the screen by a convex lens for two different locations of the lens separated by 20 cm. Calculate the focal length of the lens used.
- A converging lens is kept coaxially in contact with a diverging lens with equal focal length. What is the focal length of the combination?
Answer:
1. For the first position of the lens, we have
∴ \(\frac{1}{f}=\frac{1}{y}-\frac{1}{(-x)}\) → (1)
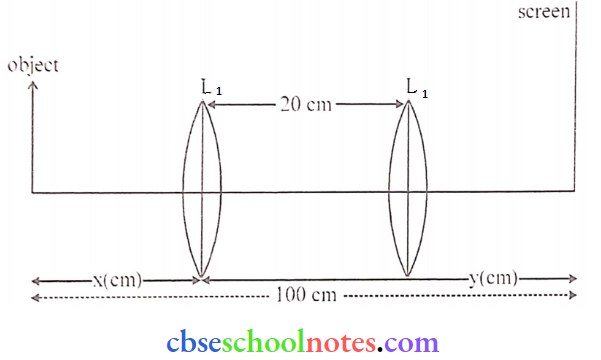
For the second position of the lens, we have (2)
⇒ \(\frac{1}{f}=\frac{1}{y-20}-\frac{1}{[-(x+20)]}\) →(2)
From (1) and (2)
⇒ \(\frac{1}{y}+\frac{1}{x}=\frac{1}{(y-20)}+\frac{1}{(x+20)} \Rightarrow \frac{x+y}{x y}=\frac{(x+20)+(y-20)}{(y-20)(x+20)}\)
∴ xy = (y – 20) (x + 20) = xy – 20 x + 20 y- 400
∴ x – y = -20
Also, x + y = 100
x= 40 cm and y = 60 cm
∴ \(\frac{1}{f}=\frac{1}{60}-\frac{1}{-40}=\frac{2+3}{120}=\frac{5}{120}\)
∴ f = 24 cm
or
Distance between the image (screen) and the object, D = 100 cm.
Distance between two locations of the convex lens, d = 20cm
Focal length (f) = \(=\frac{D^2-d^2}{4 D}=\frac{(100)^2-(20)^2}{4 \times 100}\)
f = 24 cm.
2. \(\frac{1}{f}=\frac{1}{f_1}+\frac{1}{\left(-f_2\right)}=\frac{1}{f_1}-\frac{1}{f_2}\)
⇒ [/altex]\frac{1}{f}=\frac{f_2-f_1}{f2 f_1}[/latex]
∴ \(f=\frac{f_2 f_1}{f_2-f_1}\)
Question 18.
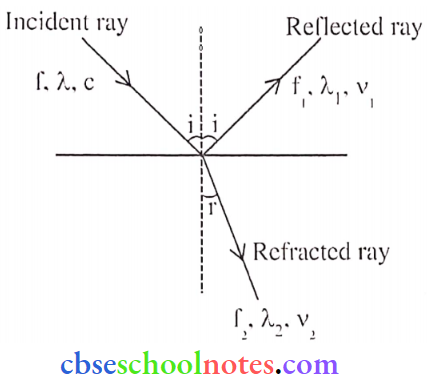
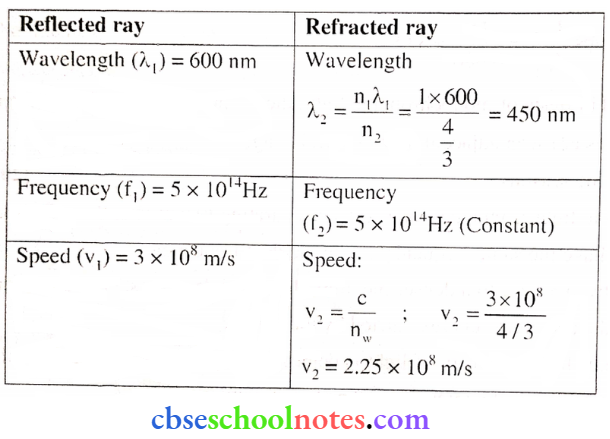
- Monochromatic light of wavelength 589 nm is incident from air on a water surface. If μ for water is 1.33, find the refracted light’s wavelength, frequency and speed.
- A double convex lens is made of glass with a refractive index of 1.55, with both faces of the same radius of curvature. Find the radius of curvature required, if the focal length is 20 cm.
Answer:
1. \(\lambda_{\text {air }}=589 \mathrm{~nm}, \mu_{\text {water }}=1.33\) (Given)
For water, \(\lambda_{w a t e r}, \frac{\mu_n}{\mu_a}=\frac{\lambda_a}{\lambda_n} \Rightarrow \lambda_w=\frac{589}{1.33}\)
∴ w = 442.8nm
Frequency of light remains constant.
Velocity, \(v=\frac{c}{\mu}=\frac{3 \times 10^8}{1.33}=2.25 \times 10^8 \mathrm{~m} / \mathrm{s}\)
2. From \(\frac{1}{f}=\left(\mu_{21}-1\right)\left[\frac{1}{R_1}-\frac{1}{R_2}\right] \quad\left\{\begin{array}{l}
\text { Using sign Convention } \\
R_1=+R \quad \text { for equi convex lens } \\
R_2=-R
\end{array}\right.\)
⇒ \(\frac{1}{f}=(1.55-1)\left[\frac{1}{R}-\left(-\frac{1}{R}\right)\right]\)
∴ \(\frac{1}{r}=(.55)\left[\frac{2}{R}\right]=\frac{1.1}{R} \Rightarrow \frac{1}{20}=\frac{1.1}{R} \Rightarrow R=1.1 \times 20=22 \mathrm{~cm}\)
Question 19.
- A triangular prism with a refracting angle of 60° is made of a transparent material of refractive index 2/√3.
- A ray of light is incident normally on the face AB as shown in the figure. Trace the path of the ray as it passes through the prism and calculate the angle of emergence and angle of deviation.
Answer:
Given: ∠A = 60°, ∠i = 0°
At M: \(\sin \mathrm{i}_{\mathrm{C}}=\frac{1}{\mu}=\frac{\sqrt{3}}{2}=\sin 60^{\circ}\)
∴ ic = 60°
So the ray PQ after refraction from the face AC grazes along AC.
∴ ∠e = 90°
From ∠i = ∠e = ∠A + ∠δ
or 0° + 90° = 60° + ∠δ
∴ δ = 90° – 60° = 30°
Question 20.
- What is total internal reflection? Under what conditions does it occur?
- Find a relation between critical angle and refractive index.
- Name one phenomenon which is based on total internal reflection
Answer:
The complete reflection of a light ray at the boundary of two media, when the ray is going from a denser to a rarer medium is called TIR.
Condition:
- Light rays must pass from a denser to a rarer medium
- the angle of incidence must be greater than the critical angle, (i > ic).
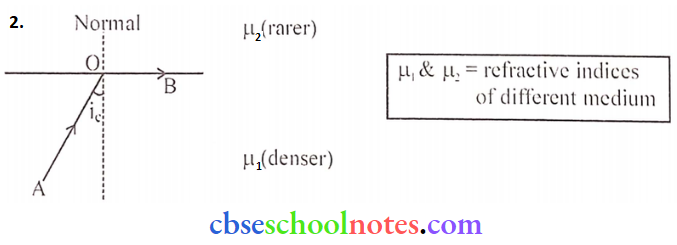
In the above Ray Ao goes from denser (say water) to rarer (say air) medium, So using Snell’s law, \(\frac{\sin i}{\sin r}=\frac{\mu_2}{\mu_1}\)
or \(\frac{\sin i_c}{\sin 90^{\circ}}=\frac{\mu_2}{\mu_1}\) [Here, angle of incidence = ic and angle of refraction = 90°]
If refractive index of rarer medium = 1 (i.e. 2 = 1)
or \(\sin i_c=\frac{1}{\mu_1}=\frac{1}{\mu}\) = (∵ \(\))
3. Mirage or Brilliance of diamond.
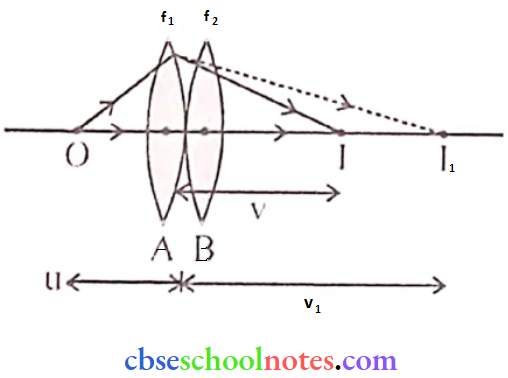
Question 21. In the following diagram, an object ‘O’ is placed 15 cm in front of a convex lens L1 of focal length 20 cm and the final image is formed at ‘I’ at a distance of 80 cm from the second lens L2. Find the focal length of the lens L2.
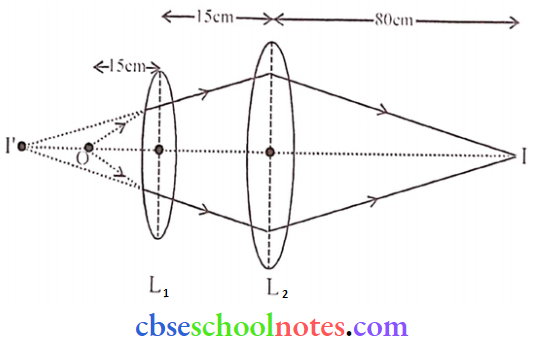
Answer:
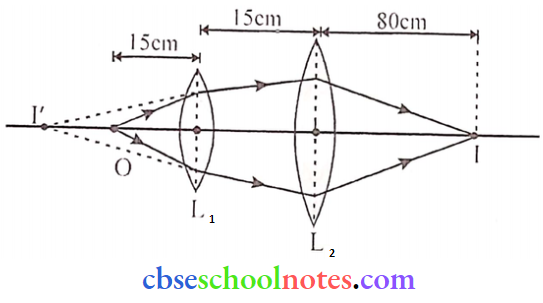
For Lens L1: \(\frac{1}{v_1}-\frac{1}{u_1}=\frac{1}{f_1} \Rightarrow \frac{1}{v_1}=\frac{1}{f_1}+\frac{1}{u_1}\)
⇒ \(\frac{1}{v_1}=\frac{1}{20}+\frac{1}{-15}\)
v1 – 60 cm
Now image formed (v1) acts as an object for L2.
For lens L2: \(\frac{1}{v_2}-\frac{1}{u_2}=\frac{1}{f_2} \Rightarrow \frac{1}{80}+\frac{1}{75}=\frac{1}{f_2} \Rightarrow \frac{1}{f_2}=\frac{31}{1200}\)
∴ \(\mathrm{f}_2=\frac{1200}{31} 38.71 \simeq 39 \mathrm{~cm}\)
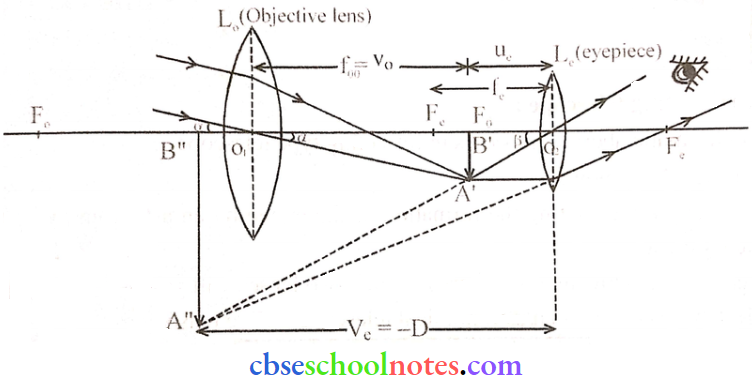
Question 22. Describe the construction of a compound microscope. Derive an expression for its total magnification. Draw a ray diagram for the formation of an image by a compound microscope.
Answer:
Compound Microscope: Figure shows a ray diagram of a compound microscope. It consists of two convex lenses one nearer to the object is known as the objective and the other closest to the eye is the eyepiece lens. Here objective lens is of small focal length (f0) and small aperture whereas the eyepiece is also of small focal length but larger than the objective lens and relatively large aperture
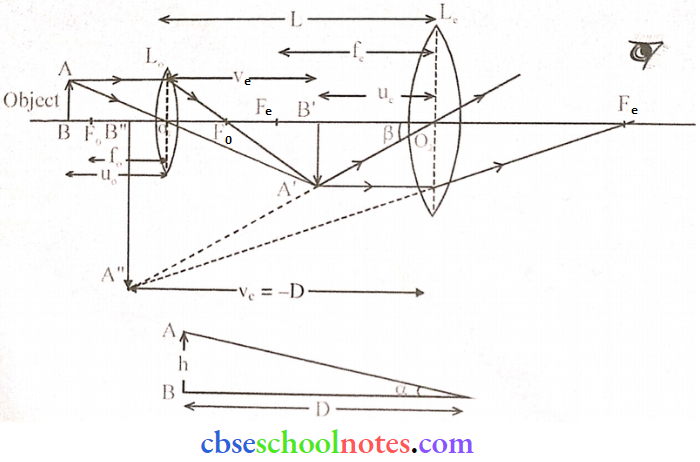
The image A’ is formed by the objective lens L0 of object AB and the final image is A “B’.
Magnifying power (M) = \(\frac{\text { Angle subtended by the final image at eye }}{\text { Angle subtended by the object when it is placed at the least distance of distinct vision at eye }}\)
⇒ \(M=\frac{\beta}{\alpha} \quad\left\{\begin{array}{l}
\text { if } \alpha \text { and } \beta \text { are very smill. then } \\
\alpha=\tan \alpha \text { and } \beta=\tan \beta
\end{array}\right.\)
⇒ \(M=\frac{\tan \beta}{\tan \alpha}\)
∴ \(M=\frac{\left(\frac{A^{\prime \prime} B^{\prime \prime}}{D}\right)}{\left(\frac{A B}{D}\right)}\) = \(M=\frac{A^{\prime \prime} B^{\prime \prime}}{A B}\)
⇒ \(M=\frac{A^{\prime \prime} B^{\prime \prime}}{A^{\prime} B^{\prime}} \times \frac{A^{\prime} B^{\prime}}{A B} \Rightarrow M=m_e \times m_o \quad\left\{\begin{array}{l}
m_0=\frac{-v_0}{u_0} \\
m_c=\frac{v_e}{u_e}
\end{array}\right.\)
⇒ \(\mathrm{M}=\frac{-\mathrm{v}_{\mathrm{o}}}{\mathrm{u}_{\mathrm{o}}} \times \frac{\mathrm{v}_{\mathrm{c}}}{\mathrm{u}_{\mathrm{c}}}\) (1)
Applying lens Formula for eyepiece \(\)
⇒ \(\frac{1}{f_e}=\frac{1}{v_e}-\frac{1}{u_e} \quad\left\{\begin{array}{l}
v_e=-D \\
u_e=-u_e
\end{array}\right.\)
∴ \(\frac{1}{f_e}=-\frac{1}{D}+\frac{1}{u_e} \Rightarrow \frac{D}{f_e}=-1+\frac{D}{u_e}\) = \(\frac{\mathrm{D}}{\mathrm{u}_{\mathrm{e}}}=1+\frac{\mathrm{D}}{\mathrm{f}_{\mathrm{e}}}\) (2)
1. When the final image is formed at least the distance of district vision (Ve = -D)
⇒ \(M=\frac{-V_0}{u_0} \times \frac{D}{U_e}\)
∴ \(M=\frac{-V_0}{u_0}\left(1+\frac{D}{f_e}\right)\) → (3)
2. When the final image is formed at infinity (ue = fe)
∴ \(M=\frac{{-v_0}}{u_0} \times \frac{D}{1}\) (4)
Question 23.
- For a glass prism (μ = √3) the angle of minimum deviation is equal to the angle of the prism. Calculate the angle of the prism.
- Draw a ray diagram when the incident ray falls normally on one of the two equal sides of a right-angled isosceles prism having refractive index μ = √3.
Answer:
Given. δm = A
From \(\mu=\frac{\sin \left(\frac{A+\delta_m}{2}\right)}{\sin (A / 2)}\) = \(\frac{\sqrt{3}}{1}=\frac{\sin \left(\frac{A+A}{2}\right)}{\sin (A / 2)}=\frac{\sin A}{\sin (A / 2)}\)
⇒ \(\sqrt{3}=\frac{2 \sin (A / 2) \cos (A / 2)}{\sin (A / 2)}\) = \(\frac{\sqrt{3}}{2}=\cos \mathrm{A} / 2\)
⇒ \(\cos 30^{\circ}=\cos (\mathrm{A} / 2) \Rightarrow 30^{\circ}=\mathrm{A} / 2\)
∴ A = 60°
2. Given μ = √3 (Prism)
For total internal reflection, angle of incidence (i) > critical angle (ic)
i.e. i > ic
or sin i > sin ic
or \(\sin i>\frac{1}{\mu}\)
or \(\sin 45^{\circ}>\frac{1}{\mu}\)
or μ > 2
Hence, ray PQ suffers TIR and goes along path TS.
Question 24.
- Draw a schematic diagram of a reflecting telescope
- Slate the advantages of reflecting telescope over refracting telescope.
Answer:
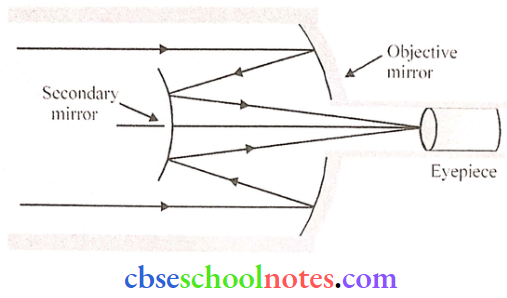
Schematic diagram of a reflecting telescope (Cassegrain).
- Reflecting telescopes do not suffer from chromatic aberration.
- The intensity of light is higher in the case of a reflecting telescope.
- Reflecting telescope’s mirrors arc easier to mount.
- Manufacturing of mirrors is cheaper compared to lenses.
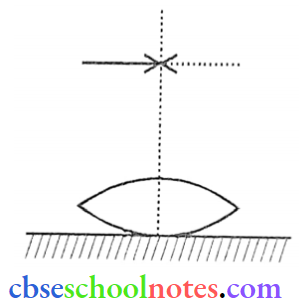
Question 25. A symmetric biconvex lens of radius of curvature R and made of glass of refractive index 1.5, is placed on a layer of liquid placed on top of a plane mirror as shown in the figure. An optical needle with its lip on the principal axis of the lens is moved along the axis until its real, inverted image coincides with the needle itself. The distance of the needle itself. The distance of the needle from the lens is measured to be x. On removing the liquid layer and repeating the experiment, the distance is found to be y. Obtain the expression for the refractive index of the liquid in terms of x and y.
Answer:
Let μ1 denote the refractive index of the liquid. When the image of the needle coincides with the needle itself; its distance from the lens, equals the relevant focal length.
With a liquid layer present, the given set-up is equivalent to a combination of the given (convex) lens and a concave plane or piano concave ‘liquid ‘lens’.
We have \(\frac{1}{f}=(\mu-1)\left(\frac{1}{R_1}-\frac{1}{R_2}\right)\)
and \(\frac{1}{f}=\frac{1}{f_1}+\frac{1}{f_2}\)
⇒ \(\frac{1}{x}=\frac{1}{f_l}+\frac{1}{y}\)
as per the given data, we then have
⇒ \(\frac{1}{r_2}=\frac{1}{y}=(1.5-1)\left[\frac{1}{R}-\left(-\frac{1}{R}\right)\right]=\frac{1}{R} = \left\{\begin{array}{l}
\frac{1}{y}=\frac{1}{R}=\frac{1}{f_2} \\
f=x
\end{array}\right\}\)
∴ \(\frac{1}{x}=\left(\mu_1-1\right)\left(-\frac{1}{R}\right)+\frac{1}{y}=\frac{-\mu_1}{y}+\frac{2}{y}\)
∴ \(\frac{\mu_1}{y}=\frac{2}{y}-\frac{1}{x}=\left(\frac{2 x-y}{x y}\right) \text { or } \mu_1=\left(\frac{2 x-y}{x}\right)\)
Question 26. The figure shows a ray of light falling normally on the face AB of an equilateral glass prism having refractive index \(\frac{3}{2}\), placed in water of refractive index \(\frac{4}{3}\) Will this ray suffer total internal reflection on striking the face AC?
Answer:
The angle of incidence, of the ray, on striking the face AC is i = 60° (as in figure)
Also. the relative refractive index of glass, concerning the surrounding water, is \(\mu_{\mathrm{r}}=\frac{3 / 2}{4 / 3}=\frac{9}{8}\)
Also \(\sin \mathrm{i}=\sin 60^{\circ}=\frac{\sqrt{3}}{2}=\frac{1.732}{2}=0.866\)
For total internal reflection, the required critical angle, in this case, is given by.
⇒\(sin \mathrm{i}_{\mathrm{C}}=\frac{1}{\mu}=\frac{8}{9} \simeq 0.89\)
∴ i < ic
Hence the ray would not suffer total internal reflection on striking the face AC.
[The student may just write the two conditions needed for total internal reflection without analysis of the given case]
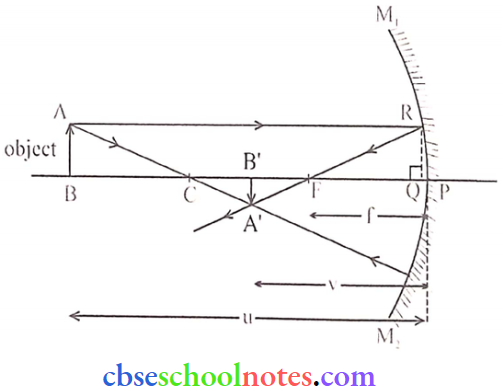
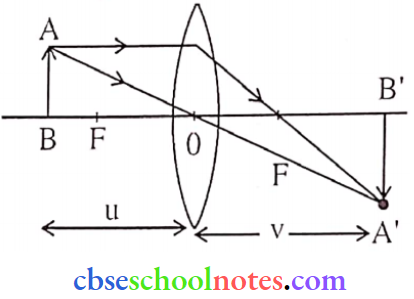
Question 27. Establish a relation between focal length, distance of object and distance of image in concave mirror.
Answer:
u ⇒ distance between pole and object
v ⇒ distance between pole and image
f ⇒ focal length
In ΔA’FB’ and ΔRFQ
∠QFR = ∠A’FB’ and ∠A’B’ F = ∠RQF = 90°
∴ ΔA’FB’- ΔRFQ. so
\(\frac{A^{\prime} B^{\prime}}{Q R}=\frac{F B^{\prime}}{Q F} \Rightarrow \frac{A^{\prime} B^{\prime}}{A B}=\frac{F B^{\prime}}{Q F}\) (1) (from QR = AB)
Similarly ΔABC ∼ ΔA’B’c, hence
⇒ \(\frac{A^{\prime} B^{\prime}}{A B}=\frac{B^{\prime} C}{B C}\) → (2)
From eq (1) and(2)
∴ \(\frac{\mathrm{FB}^{\prime}}{\mathrm{QF}}=\frac{\mathrm{B}^{\prime} \mathrm{C}}{\mathrm{BC}}\)
Point Q is very close to P, Hence ⇒ QF ≈PF
⇒ \(\frac{P B^{\prime}-P F}{P F}=\frac{P C-P B^{\prime}}{P B-P C}\)
Applying sign convention, PB’ = -v, PF = -f, PC = -2f and PB = -u-0
⇒ \(\frac{-v-(-f)}{-f}=\frac{-2 f-(-v)}{u-(-2 f)}\)
On solving, uv – uf = vf
divide by uvf
∴ \(\frac{1}{\mathrm{f}}=\frac{1}{\mathrm{u}}+\frac{\mathrm{l}}{\mathrm{v}}\) (This is mirror’s equation)
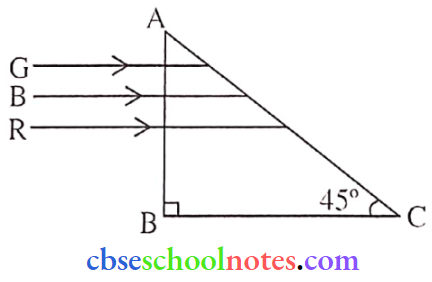
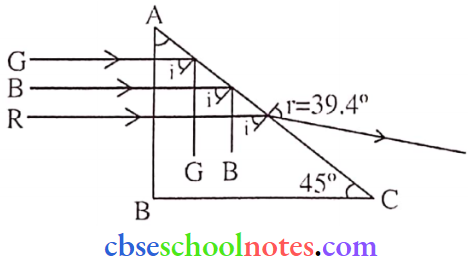
Question 28. Refractive indices of the given prism material for Red, Blue and Green colours arc 1 .39. 1 .48 and 1 .42 respectively. Trace the path of rays through the prism.
Answer:
For TIR
i > ic
sin i > sin ic
⇒ \(\sin i>\frac{1}{\mu}\)
cosec i < μ
(μR = 1 .39, μG = 1 .42, μB = 1 .48
Now → cosec 45° = √2 = 1 .414
So, μR < cosec i [Red colour will refract]
μB > cosec i [Blue colour will be internally reflected]
μG > cosec i [Green colour will be internally reflected]
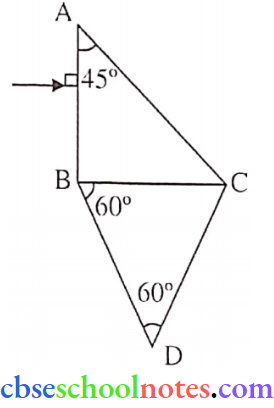
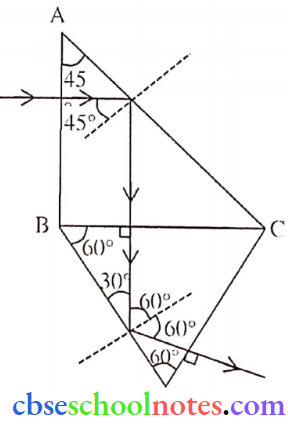
Question 29. Two prisms ABC and DBC are arranged as shown in the figure
The Ctritical angles for the two prisms concerning air are 41.1 and 45 respectively. Trace the path of the ray through the combination.
Answer:
Question 30.
- An object is placed in front of a converging lens. Obtain the conditions under which the magnification produced by the lens is
- Negative and
- Positive.
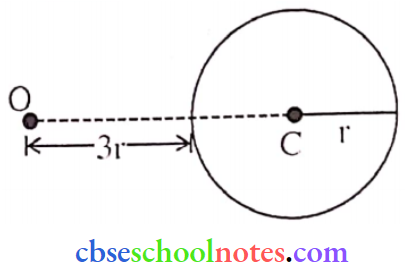
- A point object is placed at 0 in front of a glass sphere. Show the formation of the image by the sphere.
Answer:
1. (1). For negative magnification object is placed beyond the focus:
⇒ \(m=\frac{v}{u}\)
using sign convention
∴ \(\mathrm{m}=-\frac{\mathrm{v}}{\mathrm{u}}\)
(2). For positive magnification object is placed between the focus and the optical centre.
⇒ \(m=\frac{v}{u}\)
Using sign convention \(\mathrm{m}=\frac{-\mathrm{v}}{-\mathrm{u}}\)
∴ \(m=\frac{v}{u}\)
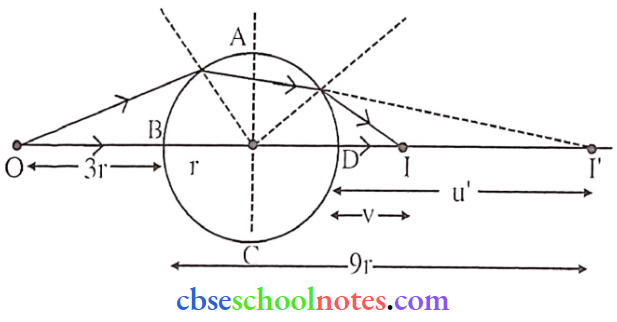
Refraction through spherical surface ABC
⇒ \(\frac{\mathrm{n}_2}{\mathrm{v}^{\prime}}-\frac{\mathrm{n}_1}{\mathrm{u}}=\frac{\mathrm{n}_2-\mathrm{n}_1}{\mathrm{R}} \quad\left\{\begin{array}{l}
\text { Refractive index of glass }=3 / 2 \\
\mathrm{u}=-3 \mathrm{r}
\end{array}\right.\)
⇒ \(\frac{\frac{3}{2}}{v^{\prime}}-\frac{1}{\left(-3 r\right)}=\frac{\left(\frac{3}{2}-1\right)}{r} = \frac{3}{2 v^{\prime}}=\frac{1}{2 r}-\frac{1}{3 r} = v^{\prime}=9 r\)
Refractive through spherical surface ADC
For refracting surface ADC, the image I’ acts as a virtual object and 1 is the final image
⇒ \(\frac{\mathrm{n}_2}{\mathrm{v}}-\frac{\mathrm{n}_1}{\mathrm{u}^{\prime}}=\frac{\mathrm{n}_2-\mathrm{n}_1}{\mathrm{R}} = \frac{1}{\mathrm{v}}-\frac{1.5}{\mathrm{u}^{\prime}}=\frac{1-1.5}{-\mathrm{r}}\) (u’ = 9r – 2r = 7r)
∴ \(\frac{1}{v}-\frac{1.5}{7 r}=\frac{0.5}{r} = \frac{1}{v}=\frac{1}{2 r}+\frac{1.5}{7 r} = \frac{1}{v}=\frac{1.5}{7 r}+\frac{0.5}{r}=\frac{1.5+3.5}{7 r} = v =\frac{7 r}{5}\)
Distance of final image from ‘B’
∴ \(\frac{7 r}{5}+2 r=\frac{17 r}{5}=3.4 \mathrm{r}\)
CBSE Class 12 Physics Chapter 9 Long Questions And Answers
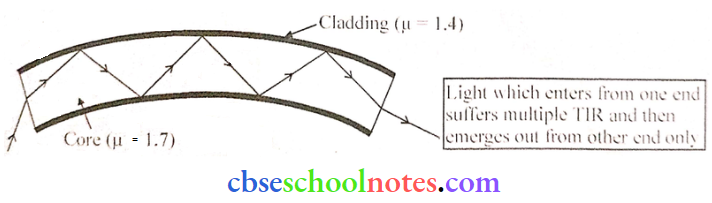
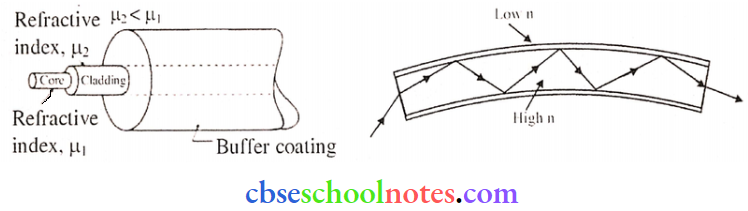
Question 1. Optical fibres Nowadays optical fibres are extensively used for transmitting audio and video signals through long distances. Optical fibres too make use of the phenomenon of total internal reflection. Optical fibre arc fabricated with high-quality composite glass or quartz fibres.
Each fibre consists of a core and cladding. The refractive index of the material of the core is higher than that of the cladding. When a signal in the form of light is directed at one end of the fibre at a suitable angle, it undergoes repeated total internal reflections along the length of the fibre and finally comes out at the other end.
Since light undergoes total internal reflection at each stage, there is no appreciable loss in the intensity of the light signal. Optical fibres are fabricated such that light reflected at one side of the inner surface strikes the other at an angle larger than the critical angle.
Even if the fibre is bent, light can easily travel along its length. Thus, an optical fibre can be used to act as an optical pipe.
(1). Which of the following statements is not true?
- Optical fibre is based on the principle of total internal reflection.
- The refractive index of the material of the core is less than that of the cladding.
- An optical fibre can be used to act as an optical pipe.
- There is no appreciable loss in the intensity of the light signal while propagating through optical fibre.
Answer: 2. The refractive index of the material of the core is less than that of the cladding.
(2). What is the condition for total internal reflection to occur?
- The angle of incidence must be equal to the critical angle.
- The angle of incidence must be less than the critical angle.
- The angle of incidence must be greater than the critical angle.
- None of the above
Answer: 3. Angle of incidence must be greater than the critical angle.
(3). Which of the following is not an application of total internal reflection?
- Mirage
- Sparkling of diamond
- Splitting of white light through a prism.
- Reflects the prism.
Answer: 3. Splitting of white light through a prism.
(4). Optical fibres are used extensively to transmit:
- Optical signal
- Current
- Sound waves
- None of the above
Answer: 1. Optical signal
Question 2. The total internal reflection of the light is used in polishing diamonds to create a sparking brilliance. By polishing the diamond with specific cuts, it adjusted most of the light rays approaching the surface arc incident with an angle of incidence more than the critical angle. Hence, they suffer multiple reflections and ultimately come out of the diamond from the top. This gives the diamond a sparking brilliance.
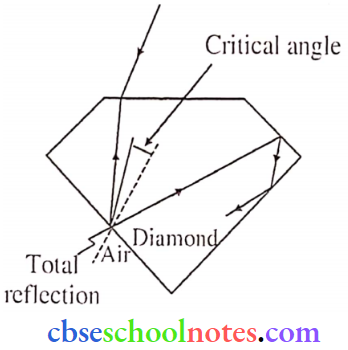
(1). The refractive index for a diamond is
- 1.41
- Same as glass
- 2.42
- 1
Answer: 3. 2.42
(2). The basic reason for the extraordinary sparkle of a suitably cut diamond is that
- It has a low refractive index
- It has high transparency
- It has a high refractive index
- It is very hard
Answer: 3. It has a high refractive index
(3). The extraordinary sparkling of diamond
- Docs do not depend on their shape
- Depends on its shape
- Has no fixed reason
- None
Answer: 4. None
(4). Optical fibre cables work on the principle of
- Dispersion of light
- Refraction of light
- Total internal reflection
- Interference of light
Answer: 3. Total internal reflection
Question 3. A compound microscope consists of two converging lenses. One of them, of a smaller aperture and smaller focal length is called an objective and the other of a slightly larger aperture and slightly larger focal length is called an eye-piece. Both lenses are fitted in a tube with an arrangement to vary the distance between them. A tiny object is placed in front of the objective at a distance slightly greater than its focal length. The objective produces the image of the object which acts as an object for the eye-piece. The eyepiece, in turn, produces the final magnified image.
(1). In a compound microscope the images formed by the objective and the eye-piece are respectively.
- Virtual, real
- Real, virtual
- Virtual, virtual
- Real, real
Answer: 2. Real, virtual
(2). The magnification due to a compound microscope does not depend upon:
- The aperture of the objective and the eye-piece
- The focal length of the objective and the eye-piece
- The length of the tube
- The colour of the light used
Answer: 1. The aperture of the objective and the eye-piece
(3). Which of the following is not correct in the context of a compound microscope?
- Both the lenses are of short Focal lengths.
- The magnifying power increases by decreasing the local lengths of the two lenses.
- The distance between the two lenses is more than (f0 + fc)
- The microscope can be used as a telescope interchanging the two lenses.
Answer: 4. The microscope can be used as a telescope interchanging the two lenses
(4). A compound microscope consists of an objective of 10X and an eye-piece of 20X. the magnification due to the microscope would he:
- 2
- 10
- 30
- 200
Answer: 4. 200
(5). The focal length of the objective and eye-pic of a compound microscope arc is 1.2 cm and 3.0 cm respectively. The object is placed at a distance of 1.25 cm from the objective. If the final image is formed at infinity, the magnifying power of the microscope would be:
- 100
- 150
- 200
- 250
Answer: 3. 200
Question 4.
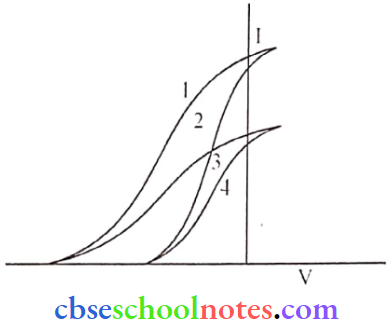
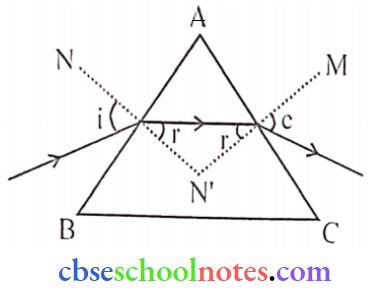
- Plot a graph to show the variation of the angle of deviation as a function of the angle of incidence for light passing through a prism. Derive an expression for the refractive index of the prism in terms of the angle of minimum deviation and the angle of the prism.
- What is the dispersion of light? What is its cause?
- A ray of light incident normally on one face of a right-angled isosceles prism is reflected as shown. What must be the minimum value of the refractive index of glass? Give relevant calculations.
Answer:
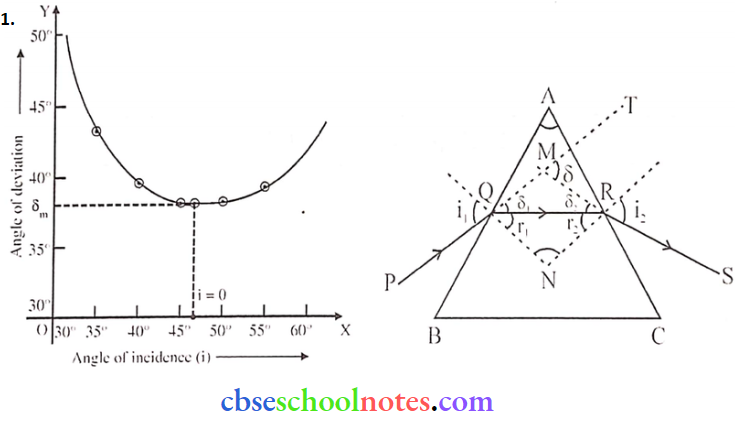
Let PQ and RS be incident and emergent rays. Let the incident ray get deviated by (δ) in a prism.
i.e. ∠TMS = δ
δ1 and δ2 are deviations produced at surfaces AB and AC respectively.
∴ δ = δ1 + δ2
δ = ( i1 – r1 ) + ( i2 – r2 )
δ = ( i1 +i2 )- ( r1 +r2 ) → (1)
In quadrilateral AQNR,
A + ∠QNR = 180° ( ∵ QN, RN are normal)
Also, in ΔQNR, ∠QNR + r1 + r2 = 180°
δ = r1 + r2 → (2)
From eq (1) and (2), we get
δ = ( i1 +i2 )- A →(3)
The angle of deviation produced by the prism varies with the angle of incidence. When the prism is adjusted at an angle of minimum deviation, then
i1 = i2 = i (suppose)
at δ = δm
⇒ r1 = r2 = r (suppose)
From (1) and (2) we have,
δm = 2i – 2r
and 2r = A
⇒ \(i=\frac{A+\delta_{m}}{2}\)
r = A/2
∴ Refractive index of material of prism is \(\mu=\frac{\sin \mathrm{i}}{\sin \mathrm{r}}=\frac{\sin \left(\frac{\mathrm{A}+\delta_{\mathrm{m}}}{2}\right)}{\sin \left(\frac{\mathrm{A}}{2}\right)}\).
2. The splitting of white light into bands of seven different colours (V, I, B, g, Y, O, R) is called dispersion of white light.
Cause: Different colours travel with velocity while passing through a prism so they get separated.
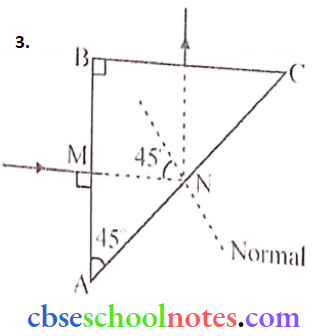
From geometry, the angle of incidence at the surface (AC) is 45°. Now as shown ray MN gets reflected at angle 45, i.e, i > ic
From \(\mu=\frac{1}{\sin i_c}=\frac{1}{\sin 45^{\circ}}=\sqrt{2}\)
Question 5.
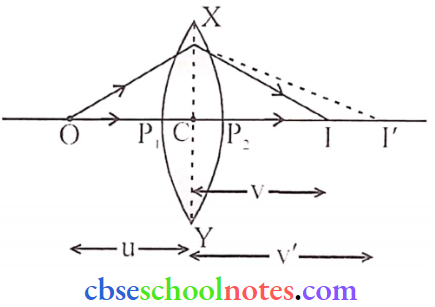
- Draw a ray diagram to show the image formation by a combination of two thin convex lenses in contact. Obtain the expression for the power of this combination in terms of the focal lengths of the lenses.
- A ray of light passing from the air through an equilateral glass prism undergoes minimum deviation when the angle of incidence is \(\left(\frac{3}{4}\right)^{\mathrm{th}}\) of the angle of prism. Calculate the speed of light in the prism.
Answer:
The object is placed at point O. whose image is formed at me, by the first lens. As image I1 is real, it works as a virtual object for second lens B, producing the final image at I.
Since the lenses are thin, assume the optical centres to be coincident. Let this central point be p.
For the image formed by lens A.
\(\frac{1}{v_1}-\frac{1}{u}=\frac{1}{f_1}\) → (1)
Similarly, for the lens B,
\(\frac{1}{v}-\frac{1}{v_1}=\frac{1}{f_2}\) → (2)
Add (1) and (2) we get,
\(\frac{1}{v}-\frac{1}{u}=\frac{1}{f_1}+\frac{1}{f_2}\)
If a lens system is taken as equivalent to a single lens of focal length f, we get.
\(P=\frac{1}{f}=\frac{1}{f_1}+\frac{1}{f_2}\) → (3)
In terms of power, equation (3) can be written as,
P = P1 + P2
Where P is the net power of this combination.
2. Given: (A = angle of prism)
- ABC is an equilateral triangle. [A = 60°]
- \(\angle \mathrm{i}=\frac{3}{4} \mathrm{~A}\)
we know that,
δ =i + c- A
Now in the condition of min. deviation,
i = e, therefore we can write,
δm = i +i- A
or \(\delta_{\mathrm{m}}=2 \mathrm{i}-\mathrm{A} \text { or } \delta_{\mathrm{m}}=2\left(\frac{3 \mathrm{~A}}{4}\right)-\mathrm{A}\)
⇒ \(\delta_{\mathrm{m}}=\frac{3 \mathrm{~A}}{2}-\mathrm{A}=\frac{\mathrm{A}}{2}=30^{\circ}\)
⇒ δm = 30°
Now, \(\mu=\frac{\sin \left(\frac{A+\delta_m}{2}\right)}{\sin \left(\frac{A}{2}\right)}=\frac{\sin \left(\frac{60^{\circ}+30^{\circ}}{2}\right)}{\sin \left(\frac{60^{\circ}}{2}\right)}\)
⇒ \(\mu=\frac{\sin 45^{\circ}}{\sin 30^{\circ}}=\sqrt{2}\)
So, \(v=\frac{c}{\mu}=\frac{3 \times 10^8}{\sqrt{2}}=2.1 \times 10^8 \mathrm{~m} / \mathrm{s}\)
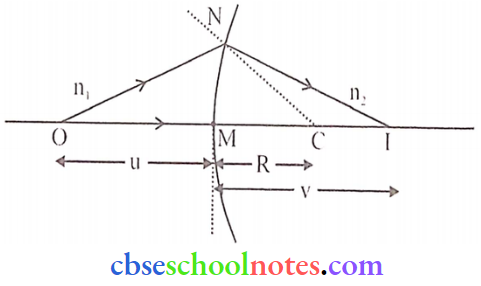
Question 6. A point object O on the principal axis of a spherical surface of radius of curvature R separating two media of refractive indices ni and m forms an image T.
Prove that: \(\frac{n_2}{v}-\frac{n_1}{u}=\frac{n_2-n_1}{R}\)
Answer:
Assumptions:
- The Aperature of the spherical refracting surface is small.
- The object is a point object and lies on the principal axis.
- Incident ray, refracted ray and normal to the spherical surface make small angles with PA.
Let, XPY = Convex spherical refracting surface.
0 = Point object in rarer medium
I = Real image in a denser medium
From ΔAOC, i = α + γ
From ΔAIC, γ = r + β ⇒ r = γ – β
From snell’s law, \(\frac{\sin i}{\sin r}=\frac{n_2}{n_1} ⇒ n_1 \sin i=n_2 \sin r\)
Since the angles are small,
∴ n1 i = n2 r
Substituting for i and r, in the above eqn, we get
⇒ n1 (α + γ) = n2 (γ – β)
or \(n_1\left\{\frac{\mathrm{AM}}{\mathrm{PO}}+\frac{\mathrm{AM}}{\mathrm{MC}}\right\}=\mathrm{n}_2\left\{\frac{\mathrm{AM}}{\mathrm{MC}}-\frac{\mathrm{AM}}{\mathrm{MI}}\right\}\)
Since the aperature is small,
∴ MC = PC, MI = PI
∴ \(\left\{\frac{n_1}{P O}+\frac{n_1}{P C}\right\}=\left\{\frac{n_2}{P C}-\frac{n_2}{P l}\right\}\)
Acc. to sign convention,
PO = -u. PC = R, PI = v
∴ \(\left\{\frac{n_1}{-u}+\frac{n_1}{R}\right\}=\left\{\frac{n_2}{R}-\frac{n_2}{v}\right\}\)
or. \(\frac{n_2}{v}-\frac{n_1}{u}=\frac{n_2-n_1}{R}\)
Question 7.
- Derive lens maker’s formula. Draw the necessary diagram.
- A convex lens is placed over a plane mirror. A pin is now positioned so that there is no parallax between the pin and its image formed by this lens-mirror combination. How will you use this observation to find the focal length of the lens? Explain briefly.
Answer:
1. Lens maker’s formula
∴ \(\frac{1}{f}=(n-1)\left[\frac{1}{R_1}-\frac{1}{R_2}\right]\)
Assumptions:
- The lens is considered a thin lens.
- An object is a point object which is situated on the principal axis.
- The aperture of the lens is small.
- Incident and refracted rays make a small angle with the principal axis.
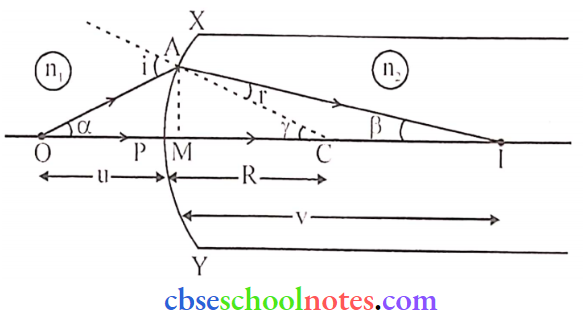
Consider a thin convex lens of absolute refractive index n2 placed in a rarer medium of absolute refractive index n1. Also, R1 and R2 are the radii of curvature of surfaces XP1 Y and XP2 Y respectively.
For refraction at surface XP1 Y:
‘O’ is the object and I’ is its real image.
Using formula,
⇒ \(\frac{n_2}{v}-\frac{n_1}{u}=\frac{n_2-n_1}{R}\) we get,
⇒ \(\frac{n_2}{v^{\prime}}-\frac{n_1}{u}=\frac{n_2-n_1}{R_1}\) → (1)
For refraction at surface XP2 Y:
F is the virtual object &I is its real image (final image).
Using formula
⇒ \(\frac{n_1}{v}-\frac{n_2}{u}=\frac{n_1-n_2}{R}\)
⇒ \(\frac{n_1}{v}-\frac{n_2}{v^{\prime}}=\frac{n_1-n_2}{R_2}\) → (2)
Adding equations (1) and (2). we get
⇒ \(n_1\left(\frac{1}{v}-\frac{1}{u}\right)=\left(n_2-n_1\right)\left[\frac{1}{R_1}-\frac{1}{R_2}\right]\)
⇒ \(\frac{1}{v}-\frac{1}{u}=\frac{n_2-n_1}{n_1}\left[\frac{1}{R_1}-\frac{1}{R_2}\right]\)
or \(\frac{1}{f}=\frac{1}{v}-\frac{1}{u}=\left(\frac{n_2}{n_1}-1\right)\left[\frac{1}{R_1}-\frac{1}{R_2}\right]\)
or \(\frac{1}{f}=(n-1)\left[\frac{1}{R_1}-\frac{1}{R_2}\right]\) (\(\frac{n_2}{n_1}=n_1=n\))
2. The rays must fall normally on the plane mirror so that the image of the pin coincides with itself.
∴ P is the position of the locus of the lens. i.e.
Distance OP = focal length










 the cubes.
the cubes. against the shapes that are cones.
against the shapes that are cones. against the shapes that are cones.
against the shapes that are cones. around the cuboids.
around the cuboids.