
Female Reproductive System
The female reproductive system comprises the external genitalia and internal organs. The external genitalia consists of labia majora, labia minora, vestibule and clitoris. As the functions of mammary glands are closely associated with the reproductive system, it is considered an accessory reproductive organ.
The internal reproductive organs are listed below :
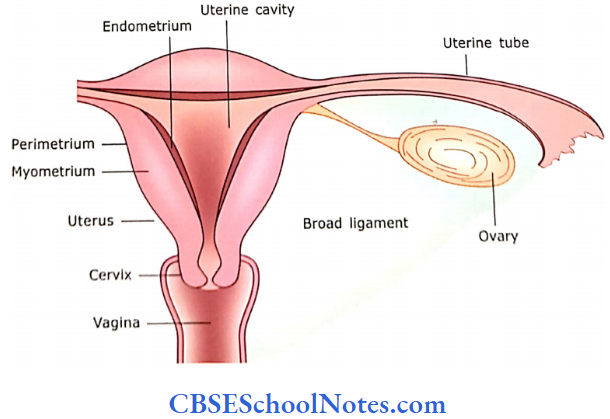
- Ovaries: These are exocrine organs. They produce maturing ova (secondary oocytes), which are discharged and passed into the uterine tubes where they may be fertilized. The ovaries are also endocrine organs because they produce hormones like progesterone and estrogen.
- Uterine Tubes: The uterine tubes or oviducts transport secondary oocytes where they may be fertilized. The fertilized or unfertilized ova are then transported to the uterus.
- The Uterus: The development of embryo and fetus occurs in the uterine cavity.
- Vagina: It is a fibromuscular organ, which gives passage to the fetus at the time of birth.
- Placenta and Umbilical Cord: These are accessory reproductive organs through which a mother can nurture a fetus until the time of parturition. Placenta is also a major endocrine organ, which produces hormones, i.e… chorionic gonadotrophin and progesterone.
- Mammary Glands: These are also considered to be part of the accessory female reproductive system.
Female reproductive organs Remember:
The female reproductive organs, under the influence of hormones, undergo regular cyclic changes from puberty to menopause.
Ovary
The ovaries are almond-shaped paired structures, each attached to a broad ligament on either side of the uterus. Each ovary measures about 3 cm in length, 1.5 cm in width, and 1 cm in thickness.
Each ovary consists of the following parts:
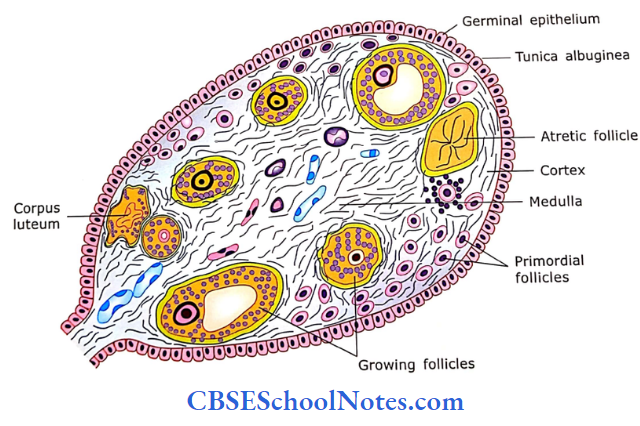
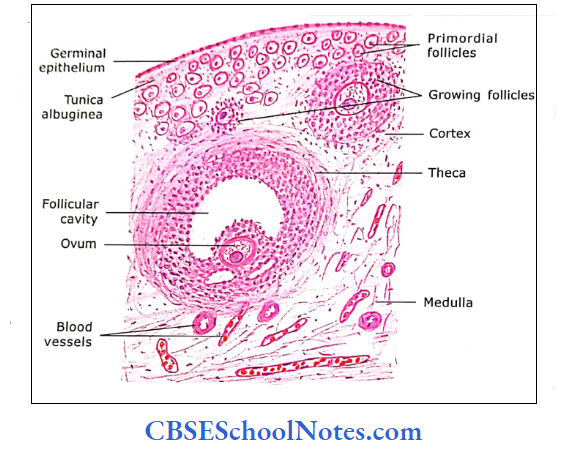
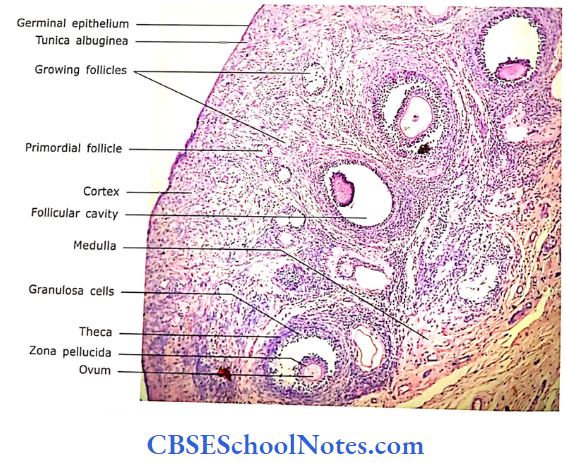
- Germinal epithelium: The surface of the ovary is covered with a single layer of low cuboidal or squamous epithelium that is called germinal epithelium. The term germinal epithelium is a misnomer because it does not give rise to germ cells (ova).
- Tunica albuginea: A connective tissue layer lies beneath the germinal epithelium, i.e., the tunica albuginea. A cross¬section of the ovary shows an outer cortex and inner medulla
- Cortex: It is the peripheral portion of the ovary, which lies beneath the tunica albuginea. It contains germ cells (oocytes) in ovarian follicles.
- The ovarian follicles arc in various stages of development in highly cellular connective tissue (stroma).
- The connective tissue cells are known as stromal (interstitial) cells.
- Their structure is like fibroblasts. The primordial follicles are found in large numbers deep into tunica albuginea.
- The growing follicles (primary and secondary follicles) show stratified follicular cells. Few mature follicles with follicular fluid are also present in the cortex.
- Theca externa and theca interna surround large-sized follicles.
- At certain places in the cortex, atretic follicles and corpus luteum can be seen.
- Medulla: It is present deep in the cortex and consists of loose fibroblastic connective tissue, lymphocytes, blood vessels, and nerves. The demarcation between cortex and medulla is indistinct.
Ovary Remember:
The ovary, deep to tunica albuginea, shows an outer cortex and inner medulla. The cortex contains highly cellular connective tissue (stroma) and germ cells (oocytes) in ovarian follicles. The ovarian follicles are in various stages of development.
Ovarian Follicles
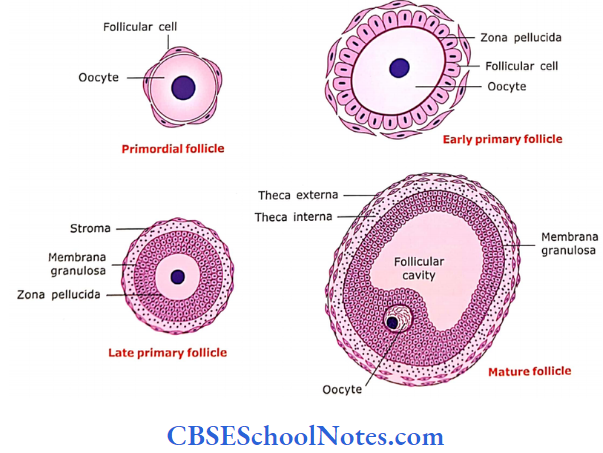
A section passing through the cortex of the ovary shows the ovarian follicles in different stages of development. An ovarian follicle consists of centrally placed oocyte and peripherally placed surrounding cells. When an oocyte is surrounded by a single layer of cells, these cells are called as follicular cells. When these cells multiply to form several layers, they are called granulosa cells. The following developmental stages of ovarian follicles are seen in the ovarian cortex of an adult reproductive female.
1. Primordial Follicle:
The primordial follicle consists of a developing ovum (primary oocyte) surrounded by a single layer of flattened epi-thelium (follicular cells). A large number of primordial follicles are found in the stroma of the cortex just beneath the tunica albuginea. The oocyte measures about 25-30 m in size and its plasma membrane is in close contact with follicular cells.
2. Primary Follicle:
After puberty, a few primordial follicles start to grow during each menstrual cycle. The oocyte enlarges and measures about 50 to 80 m.
- The surrounding single layer of lint-tened cells changes to low cuboidal.
- Oocyte and follicle cells now secrete a gel-like glycoprotein layer surrounding the oocyte.
- This is called zona pellucida.
- These single-layer cuboidal-shaped follicular cells divide rapidly to form six to seven layers of cuboidal cells called granulosa cells.
- The outermost cells rest on a well-defined basement membrane, which is separated from the ovarian stroma.
The surrounding stroma now differentiates into two layers:
- Theca interna, a highly vascular layer of secretory cells and
- Theca externa is the outer layer of connective tissue cells. It mainly contains smooth muscle cells and collagen fibers.
The follicle is now called as primary follicle
3. Secondary Follicle:
The granulosa cells begin to secrete follicular fluid, thus few small fluid-filled spaces appear between follicular cells. Now diameter of the follicle measures about 0.2 mm and the oocyte measures 125 m. These spaces now coalesce into a single large space (antrum) surrounded by follicular cells. The antrum is filled with a fluid. The follicle is now called a secondary follicle.
4. Graafian Follicle (Mature Follicle):
The follicle now increases in size and its antrum also enlarges. It measures about 10 mm or more. The primary oocyte completes its first meiotic division and becomes a secondary oocyte. The secondary oocyte starts its second meiotic division and reaches the metaphase stage at about the time when the follicle bursts and releases its secondary oocyte. This process is called ovulation. The theca interna further develops and produces estrogen. Similarly, granulosa cells are also involved in the production of ovarian hormones.
The follicle in which the above events are taking place is called as Graafian follicle or mature follicle.

Primordial follicle Remember:
A primordial follicle consists of a developing ovum (pri¬mary oocyte) surrounded by a single layer of flattened epithelium (follicular cells).
- In the development of primary follicles, follicular cells divide rapidly to form 6-7 layers of cuboidal cells called granulosa cells.
- The surrounding stroma now differentiates into two layers, i.e., theca interna and theca externa.
- In the secondary follicle, there occurs the accumula¬tion of liquor folliculi among the granulose cells.
- A mature follicle or Graafian follicle is formed by the continued proliferation of granulosa cells and continued formation of liquor follicle until its size just before ovulation reaches about 1 cm or more. This follicle contains the secondary oocyte.
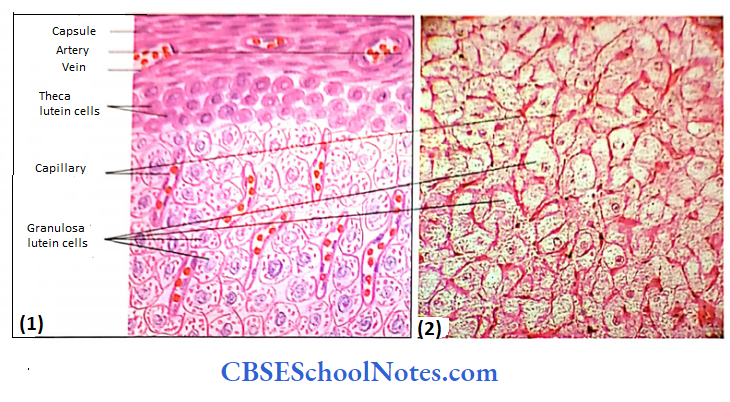
Corpus Luteum
After ovulation, the wall of the follicle collapses and becomes infolded. The blood vessels and stromal cells now invade the granulosa cells. The granulosa cells and theca interna cells enlarge, accumulate lipids,s and become pale-staining luteal cells. The structure is now called as corpus luteum, which is now a spherical body.
Two kinds of lutein cells are seen in the corpus luteum:
- Those arising from granulosa cells are called granulosa lutein cells and they form the bulk of corpus luteum and form progesterone.
- Those arising from theca interna cells are called theca lutein cells.
They are much smaller, less in number, and deeply staining and are found at the periphery. They secrete estradiol. Cells of theca externa form a capsule. If fertilization takes place then the corpus luteum will survive for the next few months. But if fertilization does not take place then corpus luteum will last for only 9 days.
When the corpus luteum degenerates, the lutein cell becomes swollen, thin, and pyknotic and a scar of connective tissue replaces the dead lutein cells. This white scar is called corpus albicans. The corpus albicans persist in the cortex for several months.
Atretic Follicles
For each menstrual cycle usually only one follicle reaches maturity and ovulates. The other maturing follicles, in various stages of development, start to degenerate. This process of regression and ultimate degeneration and disappearance of follicles is called follicular atresia.
After ovulation, the wall of the collapsed follicle undergoes reorganization to form the corpus luteum.
Two kinds of lutein cells are seen in the corpus luteum, i.e.,
- Granulosa lutein cells (they form progesterone) and
- Theca lutein cells (they form estradiol).
If fertilization takes place then the corpus luteum will survive for the next few months.
- However, if fertilization does not take place then corpus luteum will last for only 9 days.
- In the process of follicular atresia, the vascular connective tissue from theca invades the membrane granulosa and antrum, the granulosa cells and oocyte degenerate, and wrinkled zona pellucida remains for some time.
- The base membrane under the membrane granulosa and cells of the theca interna enlarge.
- The basement membrane becomes a distinct glossy membrane and theca cells look like theca lutein cells.
- The follicle eventually disappears as the ovarian stroma invades the degenerating follicle.
The primary oocyte is arrested for 12-50 years in the prophase stage of the first meiotic Division. Just before ovulation, the secondary oocyte is also arrested at metaphase in the second meiotic division which is completed only if the oocyte is penetrated by a spermatozoon.
Ovary Clinical Application
- Polycystic Ovary:
- In this condition, both the ovaries consist of fluid-filled follicular cysts and atrophic secondary follicles that lie beneath the thick tunica albuginea.
- This condition may result due to excessive production of estrogens; failure of ovulation; and absence of progesterone production due to failure of the follicle to transform into corpus luteum.
- Females suffering from polycystic ovaries are infertile and have scanty menstruation. These patients can be treated by hormones.
Uterine Tube (Fallopian Tube)
Passing from the open end to the uterine cavity, there are four different regions of the uterine tube: the infundibulum, ampulla, isthmus, and interstitial portion in the wall of the uterus. These regions differ according to the size of their lumina and the relative thickness of their wall. The ovum is received by the uterine tube for fertilization in its ampullary part. From here, it is transported to the uterine cavity.
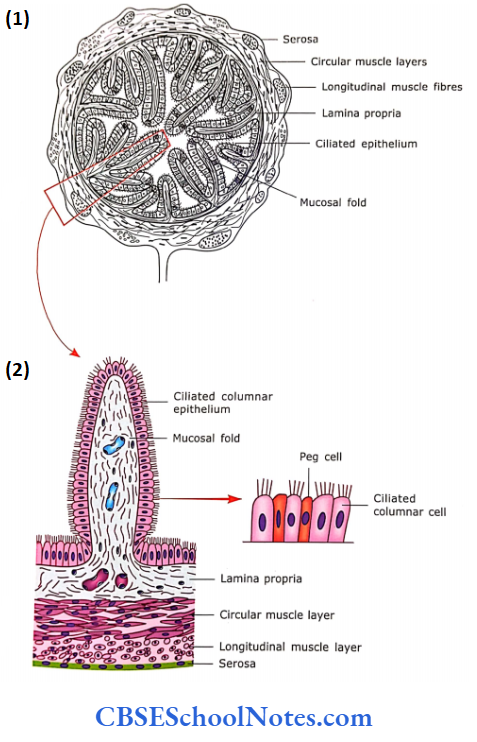
The uterine tube consists of the following layers :
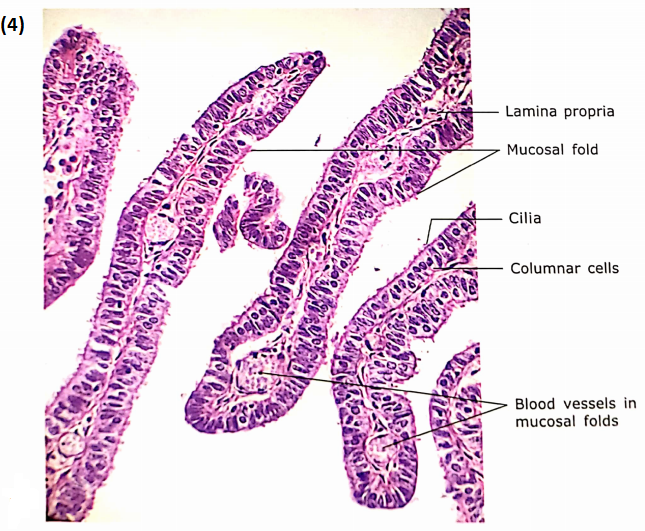
1. Mucosa
The mucosa of all regions is lined by simple ciliated colum¬nar epithelium and peg-shaped noil-ciliated secretory’ cells. The size and activity of these two types of cells vary depending on the level of estrogen and progesterone (stage of the menstrual cycle).
- The lamina propria is made up of richly vascularized loose connective tissue. Peg cells have secretion functions.
- Their secretion provides nutrition and a protective environment for spermatogonia. The secretion also helps incapacitation of spermatozoa. a process by which spermatozoa become fully mature and capable of fertilizing the ovum.
- It also provides nutrition to fertilize the egg as it travels through the uterine tube, and the cilia of columnar ciliated cells beat towards Lucius. This helps in the movement of the zygote toward the uterus.
- Because of the presence of branching mucosal folds (leaf-like structure). the lumen of the uterine tube is highly irregular. The mucosal foldings are maximum in the ampullary nan and minimal in the interstitial part of the tube.
2. Muscle layer:
This is present in two distinct layers, i.e., inner circular and outer longitudinal. The thickness of the muscle coat increases from the lateral end to the medial end of the tube (from the infundibulum to the interstitial portion).
3. Serosa: It is the peritoneal covering of the broad ligament.
Uterine tube Remember:
The wall of the uterine tube consists of three layers, i.e., mucosa, muscle coat, and serosa. The mucosa is lined by simple ciliated columnar epithelium and peg-shaped non-ciliated secretory cells.
Uterus
The uterus is a pear-shaped organ divided into three parts, i.e.. fundus, body, and cervix. The nulliparous uterus measures 7.5 cm in length, 5 cm in width, and 2.5 cm in thickness. During pregnancy, it increases tremendously in size. The uterine wall of the fundus and body consists of three layers, i.e., perimetrium, myometrium, and endometrium . The histology of the cervical part of the uterus is different and will be described separately.
1. Perimetrium:
This consists of two layers a mesothelial lining and a connective tissue layer rich in blood vessels and elastic fibers. This is the continuation of the peritoneum of the broad ligament.
2. Myometrium: It is the thickest layer of the uterus. It consists of compactly arranged smooth muscle bundles, which are arranged in three ill-defined layers.
- The inner and outer layers of muscle fibers are arranged longitudinally.
- The middle layer is a thick layer of circularly or spirally arranged muscle fibers. This layer contains large blood vessels and interstitial connect-live (issue.
- The myometrium undergoes considerable enlargement of during pregnancy.
- This is due to the hypertrophy of existing muscle lilacs and the addition of new smooth muscle fibers.
- New smooth muscle fibers are produced by the division of existing muscle cells and differentiation of mesenchymal cells.
- These changes occur under the influence of estrogen.
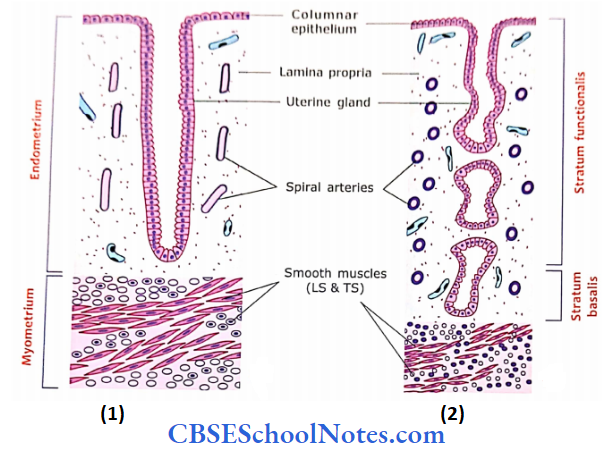
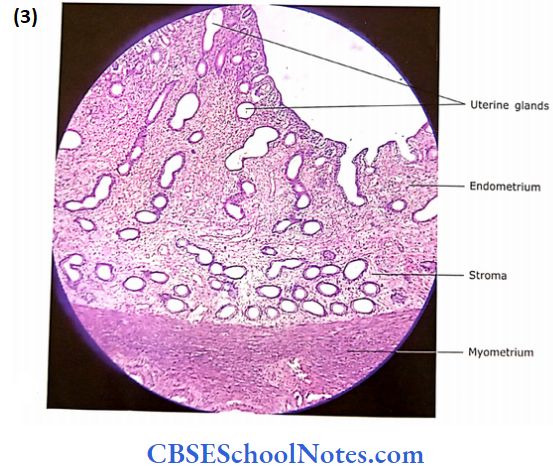
3. Endometrium:
- This is the mucosal lining of the uterine cavity.
- It consists of simple columnar secretory epithelium overlying thick lamina propria.
- Simple tubular glands are present in lamina propria, which open directly to the surface.
- These glands are usually coiled in deep portions. Hence, many cross-sections of glands are seen in the deep part (near the myometrium).
- Coiled (spiral) arteries are present in between the glands.
The endometrium can be divided into two zones:
A narrow 1/3 deep layer is called as basal stratum (stratum basalis) and a wide 2/3 superficial layer called as functional stratum (stratum functionalis).
Uterus Remember:
The uterine wall of the fundus and body consists of three layers, i.e., perimetrium, myometrium, and endometrium. The endometrium is the mucosal lining of the uterus.
- It consists of two layers: A narrow 1/3 deep layer is called stratum basalis and a wide 2/3 superficial layer is called stratum functionalis. The stratum functionals of endometrium proliferate and then degenerate during each menstrual cycle
Cyclic Changes in Endometrium:
The endometrium undergoes monthly cyclic changes in its thickness and histological appearance. These changes are under the control of ovarian hormones. The cyclic changes of the endometrium are divided into three phases.
- Follicular Phase (Proliferative Phase): It coincides with the secretion of estrogen from developing follicles in the ovary. It extends from day 4 to day 14 of menstrual cycle. It is also known as the pre-ovulatory phase as ovulation occurs on day 14 of the menstrual cycle.
- Secretory Phase: It coincides with the secretion of progesterone by corpus luteum. It correlates with day 15 to day 28 of the menstrual cycle.
- Menstrual Phase (Menses): If the ovum is not fertilized the shedding of the superficial endometrium (functional stratum) occurs along with loss of blood.
- The stratum basale remains intact.
- This phase occurs because of the cessation of the selection of progesterone by corpus lutcum.
- This phase lasts for roughly the first 5 days of the cycle. The first day of menstruation is considered the first day of a new cycle.
Histological Structure of Endometrium in Different Phases
1. The Endometrium of the Proliferative Phase:
This phase begins at the end of the menstrual phase (on about 511 days of the cycle). In this phase, there occurs the repair of damaged endometrium by the proliferation of cells in the stratum basale. There appear new surface epithelium and stroma, and blood vessels and glands begin to grow by numerous mitotic divisions.
At the end of this phase:
- The thickness of the endometrium is about 3-4 mm.
- The stroma is abundant and highly cellular. It consists of fibroblast cells, a few collagen fibers, and a network of reticular fibers.
- The endometrial glands are straight and have narrow lumen with a slightly wavy’ appearance.
- Spiral arteries are now long reaching up to the middle of the endometrium. They are slightly coiled.
2. The Endometrium of the Secretory Phase:
The endometrium now comes under the influence of progesterone secreted by the corpus luteum. The endometrium becomes thicker and measures about 6-7 mm. The increase in thickness is due to the collection of fluid (edema) in the stroma.
- The endometrial glands show increased secretory activities and because of this they become more tortuous and acquire lateral sacculation.
- Thus, in a section, the lumen of glands is dilated because of the accumulation of large quantities of secretory products.
- The spiral arteries are highly coiled and now extend throughout the endometrium, i.e., up to the superficial part.
- The above changes are seen in stratum functionale. Very little change takes place in the stratum basale.
3. The Endometrium of the Menstrual Phase
This phase results because of necrosis of the endometrium secondary to constriction of coiled arteries. These changes occur due to a decline in the ovarian secretion of estrogen and progesterone.
- The epithelium and underlying tissue are lost.
- The fragments of necrotic stroma, spiral arteries, and glands are sloughed off.
- The eroded surface is covered with blood clots.
- The vaginal discharge consists of blood, uterine fluid, and fragments of necrotic endometrial tissue of stratum functional,
Cortex
The cervix is the narrow lower part of the uterus. ‘The lumen of the cervix is narrow and known as a cervical canal. The upper end of the canal communicates with the cavity of the body of the uterus and the lower end with the vagina. The upper and lower openings are referred to as internal and external os, respectively. The lower portion cervix projects into the vagina and is called as portion vaginalis.
The histology of the cervix is different than the fundus and the body of the uterus. The cervix is not lined by endometrium, hence does not show cyclic changes similar to endometrium. The surface epithelium of cervical mucosa is mucus-secreting and lamina propria contains a large branched gland.
There are no spiral arteries in the cervical mucosa.
- The cervical canal is lined by tall columnar mucus-secreting epithelium.
- This type of epithelium also lines the branched tubular cervical glands in lamina propria. They secrete mucus, which is rich in the enzyme lysozyme.
- The secretion of mucus increases many folds during mid-cycle (at the time of ovulation), which helps in the migration of sperms into the uterus.
- The secretion of mucus is under cyclic control of ovarian hormones.
- The lamina propria is made up of loose connective tissue where cells predominate.
- Deep to lamina propria is a muscle layer consisting of smooth muscle and intervening connective tissue.
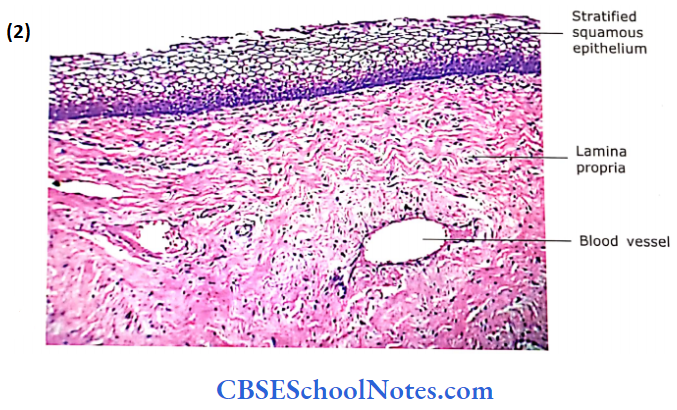
- The portion of the cervix, which projects in the vagina, is lined by stratified squamous epithelium. At the externals, there is a sudden change from columnar to stratified squamous epithelium.
Cervical canal Remember:
The cervical canal is lined by tall columnar mucous-secreting epithelium. The branched tubular cervical glands are present in lamina propria, which also secrete mucus. At the external os, there is a sudden change from columnar to stratified squamous epithelium.
Cervical and Vaginal Smear Clinical Applications
Examination of Cervical and Vaginal Smear (Pap Smears or Papanicolaou Test)
- As the epithelial cells of the vagina and cervix are constantly shed off. the cervical and vaginal smear is examined to study the characteristics of these cells (cytology).
- This examination gives information of clinical importance. The pap smear can tell us whether the lady is in the first or second half of the menstrual cycle (estrogen or progesterone phase).
- The pap smear is also useful in the detection of early cervical cancer (carcinoma in situ).
- The cancer of cervical (cervical carcinoma) is the most common in males. It is derived from the stratified squamous epithelium of the cervix.
Vagina
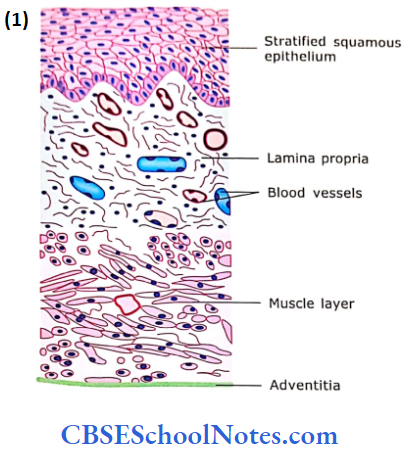
The vagina is a fibromuscular tube. It has the following layers
- Mucosa
- Muscular Layer
- Adventitia
1. Mucosa:
The lining epithelium is stratified squamous, which is non-keratinized. although some of the superficial cells may contain keratohyaline.
- The epithelium accumulates glycogen under the influence of estrogen (follicular phase) but diminishes later in the cycle.
- Bacteria act on glycogen to produce lactic acid, which lowers the pH of the vagina and helps in controlling the infection.
- The surface cells are continuously shed off. The vagina has no glands but is kept moist by the secretion of cervical glands.
- The lamina propria is broad and contains many elastic fibers in moderately dense connective tissue.
- Large numbers of small vessels are present throughout the lamina propria.
2. Muscular Layer:
It is made up predominantly of longitudinally and obliquely arranged bundles of smooth muscle fibers. In between the muscle bundles are connective tissue and blood vessels.
3. Adventitia: This layer is made up of connective tissue and contains blood vessels.
Placenta
Readers are advised to read the embryological development of the placenta before reading
The following description of the placenta:
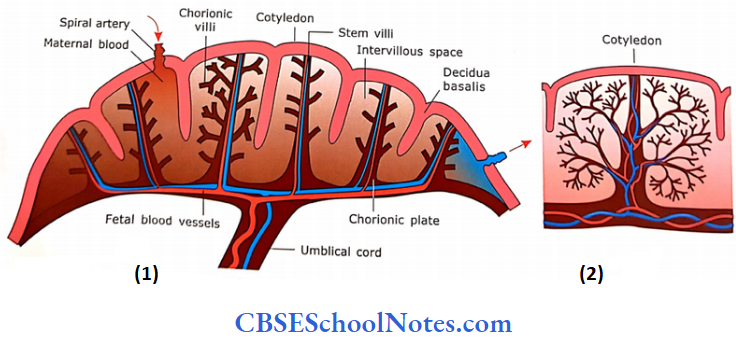
- The placenta is involved in providing the nutrition, hormones, and oxygen to the fetus and removes the metabolic wastes of the fetus. The placenta is formed by both fetal and maternal tissue. The fetal part of the placenta is formed by chorion and the maternal by decidua basalis. is a diagrammatic representation of various parts of a fully formed placenta.
- From the chorionic plate, there are many stem villi, which branch repeatedly. The core of these villi contains fetal blood vessels and capillaries. The other side of the placenta has a decidual plate. It sends incomplete septa toward the chorionic plate, which divides the placenta into 15- 20 cotyledons.
- The maternal blood comes to intervillous space from the spiral arteries of decidua. It bathes the chorionic villi. The exchange of gases and metabolic products occurs between the blood flowing in the capillaries of the villi and the maternal blood, which bathes these villi.
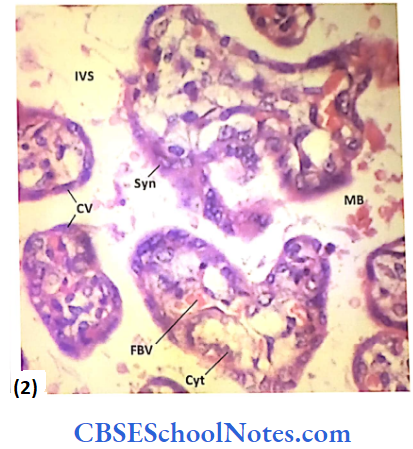
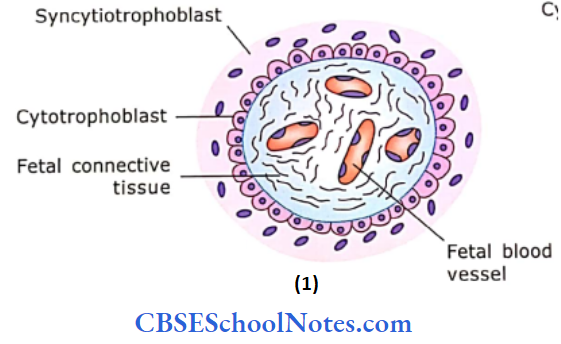
- A slide of the placenta will show the cross-section of many villi. A villus is lined with the inner layer of cytotrophoblasts and the outer layer of syncytiotrophoblasts. The cytotrophoblasts are cuboidal in shape and lie on the basement membrane.
- The syncytiotrophoblast layer is the layer of multinucleated cytoplasm with indistinct cell margins. The core of the villi contains umbilical blood capillaries.
Placenta Remember:
The placenta is involved in providing the nutrition, hormones, and oxygen to the fetus and removes the metabolic wastes of the fetus. In the third trimester of. pregnancy, the placental barrier is formed by thin syncytiotrophoblastic cells, the basement membrane of the fetal capillary’ and the endothelial cell of the fetal capillary.
Embedded in a thin layer of legal conned tissue. The cross-sections of villi nix’ are surrounded by maternal blood (RBCs)
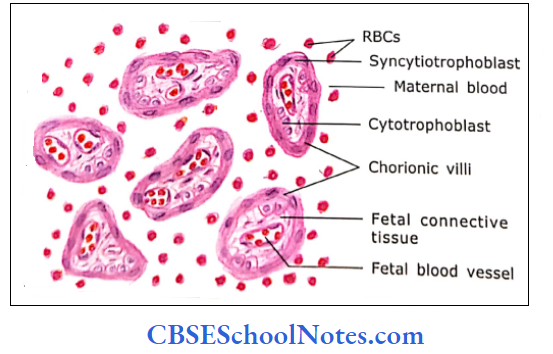
In earlier stages of pregnancy (3-5 months), the placental barrier between fetal blood (in fetal capillaries) and maternal blood (in intervillous space) consists of:
- Endothelium of fetal capillaries. The endothelium is non-fenestrated.
- The basal lamina of fetal capillaries.
- Fetal connective tissue
- The basal lamina of cytotrophoblasts
- Cvtotrophoblast
- Syncytial trophoblast
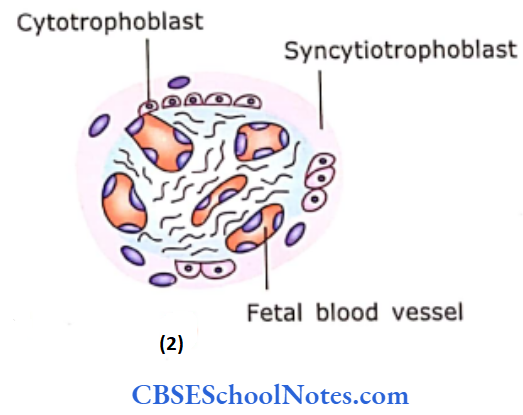
As the placenta becomes older, the chorionic villi at full term show the disappearance of the cytotrophoblastic layer. The syncytial trophoblast becomes thin, and fetal capillaries increase in number and abut closely to the syncytial trophoblast. The thickness of the placental barrier reduces from 0.025 mm at the beginning to 0.002 mm at full term.
Now it has the following layers:
- Thin syncytiotrophoblastic cells
- The basement membrane of the fetal capillary
- The endothelial cell of the fetal capillary
The syncytial Imphobliisl produces progesterone, estrogen, human chorionic gonadotrophin, and other hormones.
Umbilical Cord
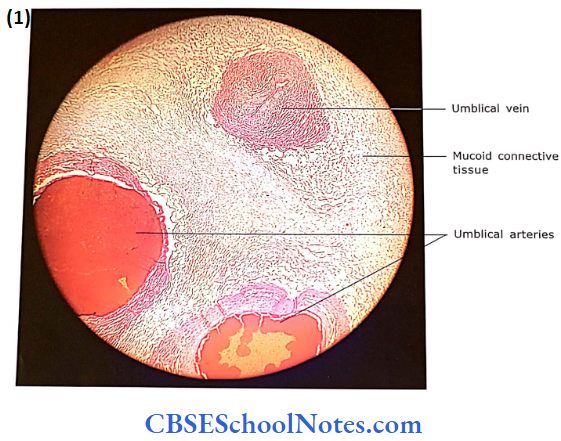
The umbilical cord extends between the placenta and the fetus. It brings the oxygenated blood from the placenta to the fetus through a single umbilical vein and carries deoxygenated blood to the placenta through two umbilical arteries. A cross-section of the umbilical cord shows the following structures
- The amniotic membrane covers the umbilical cord. Thus, the cord is lined by flattened amniotic epithelial cells.
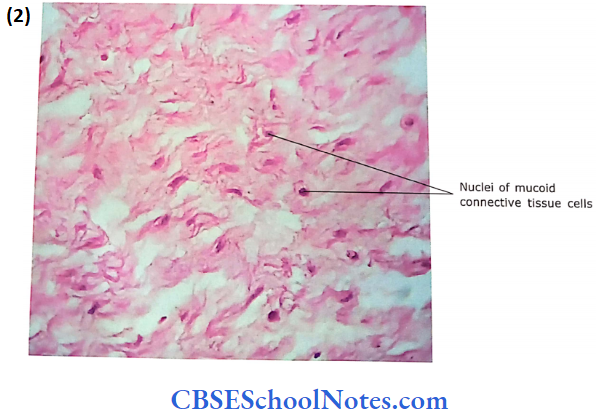
- Deep to epithelial lining umbilical cord contains mucoid connective tissue (Wharton’s jelly).
- Wharton’s jelly consists of highly branched fibroblasts, collagen fibers, and ground substance.
- The fibroblasts are widely separated from each other because of the ground substance.
- In the connective tissue, there is the presence of two umbili¬cal arteries and one umbilical vein. The umbilical arteries are thick-walled and show wavy internal elastic lamina and narrow lumen. The vein is thin-walled with a wide lumen.
Mammary Glands (Breast)
Two mammary glands are modified sweat glands of the skin that have evolved in mammals to produce milk to nourish the offspring. Breast starts developing in females at puberty under the influence of hormones.
- They reach their greatest development at about age 20. The striking changes in size and functional activity occur during pregnancy and lactation. Atrophic changes start at the age of 40 and increase after menopause.
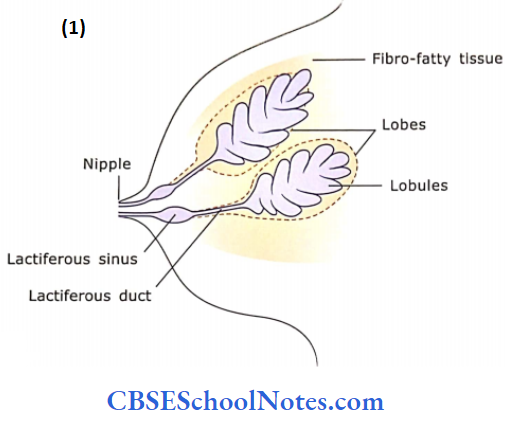
- Each breast consists of 15-20 individual, radially arranged mammary glands called lobes. A single large lactiferous duct drains each lobe. Therefore, 15-20 large lactiferous ducts converge upon the nipple to open as milk pores.
- Each lobe (in a breast) is surrounded by a dense fi¬brous connective tissue capsule. The capsule in turn is surrounded by abundant adipose tissue. Each lobe consists of several smaller compartments called lobules.
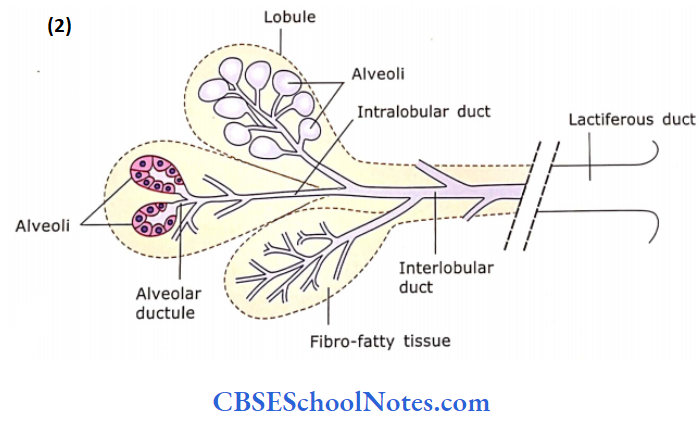
- Each lobule is composed of grapelike clusters of milk-secreting glands termed alveoli, which are embedded in connective tissue.
From alveoli, ducts may be traced as follows:
- Alveolus to Alveolar Ductule: The ductule drains an alveolus and is lined by low cuboidal epithelium.
- Intralobular Duct: Many ductules join to form this duct, which is lined by cuboidal epithelium. Both alveolar ductules and intralobu¬lar ducts are present within lobule, in between alveoli.
- Interlobular Ducts: These are lined by cuboidal to low columnar epithelium and are present in connective tissue septa between lobules.
Lactiferous (Lobar Duct):
It is a large duct with columnar epithelium, terminating at the nipple. The lobar ducts ha ve a dilatation. the lactiferous sinus, under the areola, which may be lined by two layers of cuboidal or pseudostratified columnar epithelium.
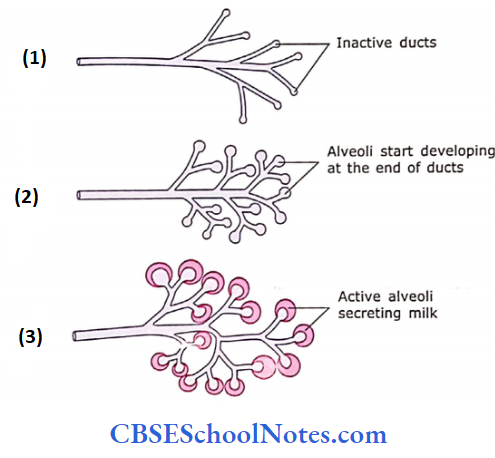
Histology of Inactive (Non-lactating) Gland
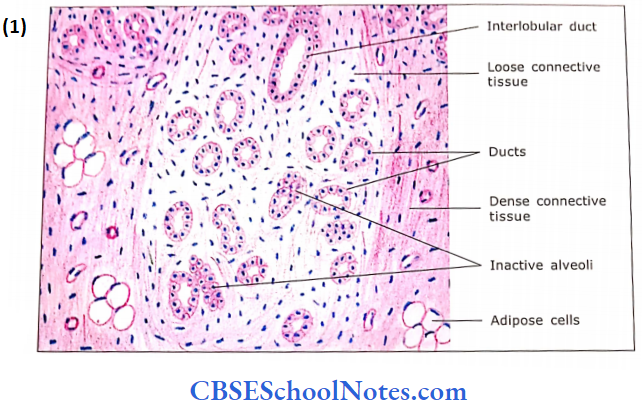
The inactive mammary gland consists mainly of duets and their branches embedded in connective tissue stroma and fat cells.
- The stroma of the gland is lobulated, although lobules in an inactive mammary gland are poorly defined. Each lobule consists of intralobular ducts and inactive alveoli in the form of solid epithelial spherical masses or cords. The intralobular connective tissue consists of loose vascular connective tissue with numerous fibroblasts.
- Lobules are surrounded by interlobular connective tissue, which is made up of dense collagen fibers, adipose tissue, blood vessels, and interlobular ducts.
- The glandular elements (alveoli) are minimal or absent. The glandular elements may be present in the form of small spherical masses of epithelial cells.
- These masses are present at the terminal end of the smallest branches of the duct system.
- These solid masses of cells do not have a lumen, but under the influence of hormones may develop into functional acini.
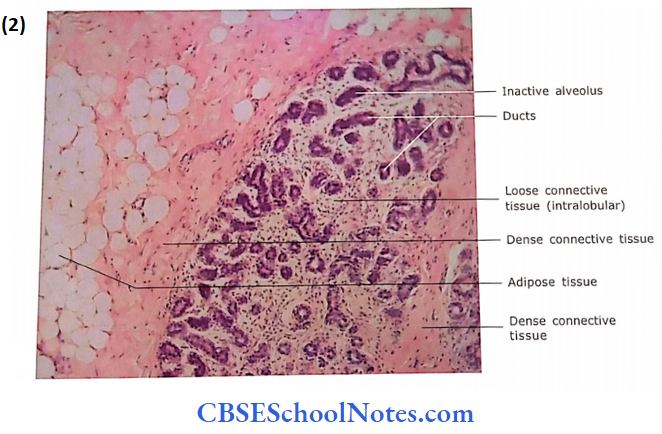
Mammary gland Remember:
In an inactive mammary gland, there is the absence of alveoli, and only ducts and their branches are embedded in connective tissue stroma.
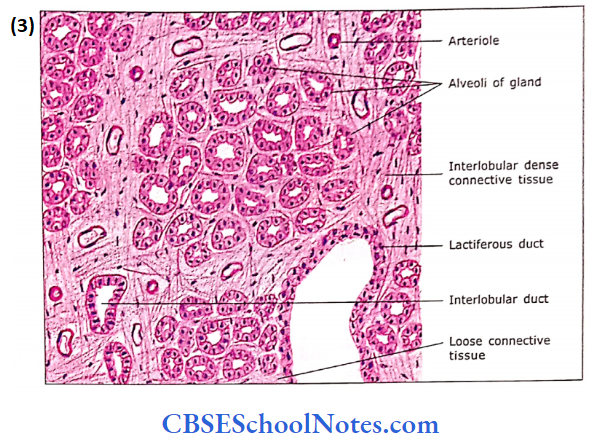
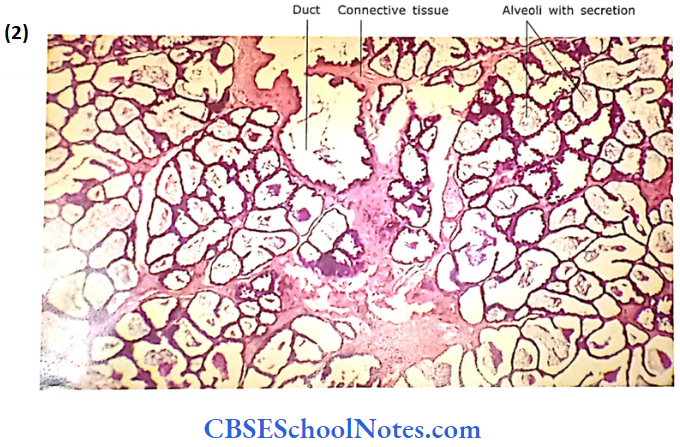
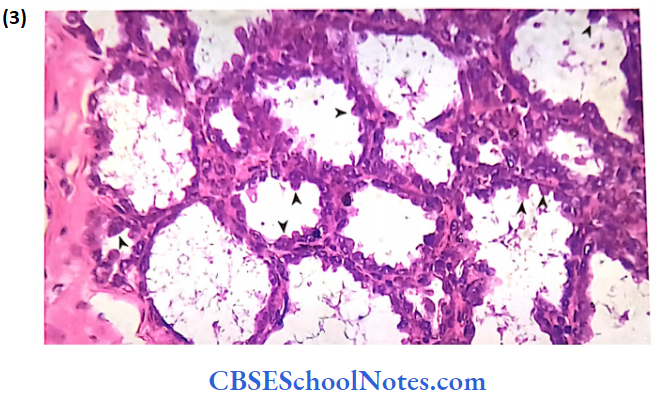
Histology of Active (Lactating) Gland
During pregnancy, the increased level of estrogen and progesterone influences the rapid growth and branching of the duct system. There occurs the formation of new acini (alveoli) at the terminal tip of ducts. The pre-existing sphere and cords of glandular cells start proliferating and form true alveoli
- In a lactating breast, the lobule of the gland is full of acini with a minimal amount of connective tissue.
- There is a marked reduction in adipose tissue. New stroma is infiltrated by lymphocytes, plasma cells, and eosinophils.
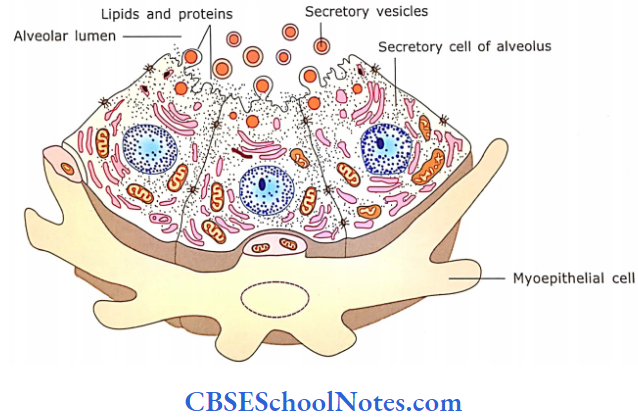
- Plasma cells secrete antibodies in the milk, which may be some degree of passive immunity to the newborn. Many alveoli me lined with low columnar cells with narrow lumen.
- They lake acidophilic slain, Bill also shows some basophilia near the base. The apical pot lion (d cell shows the presence of lipid droplets.
- The lipid droplets are also seen in the lumen of the alveoli. The secretion of lipids is apocrine, while the protein component of the milk is secreted through merocrine secretion.
- Some alveoli may be in the resting phase, i.e… their epithelium is low cuboidal and their wide lumen is filled with lipid droplets (milk).
- Myoepithelial cells are seen between the basement membrane and secretory cells.
- The intralobular ducts are seen, but they are fewer in number compared to several alveoli.
- They can be easily differentiated from alveoli because they take dark stains compared to alveoli.
- The interlobular ducts may also show the presence of milk in their lumen. The bigger ducts now may be lined with stratified columnar cells.
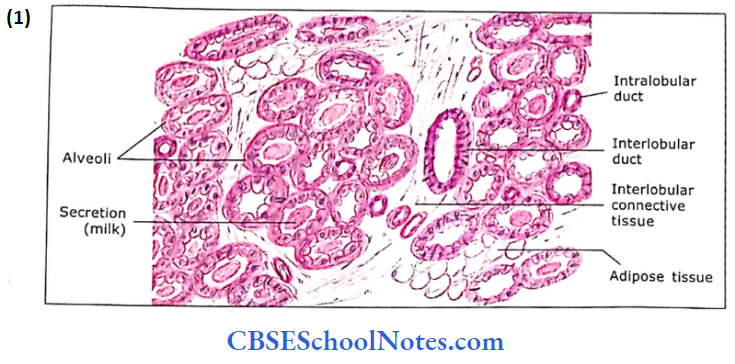
During pregnancy under the influence of hormones, there occurs the rapid growth and branching of the duct system and the development of secretory units known as alveoli. While in a lactating breast, the lobule of the gland is full of alveoli with a minimal amount of connective tissue.
Mammary Gland (Brest) Clinical Application
- Breast Cancer: Breast cancers (carcinomas) arise due to the malignant proliferation of epithelial cells lining lactiferous ducts. The early detection of breast cancer by self-examination may reduce the mortality rate.
- Milk Ejection Reflex: As soon as a child suckles the breast, the sensory receptors in the nipple of the mother get stimulated.
- This results: In the secretion of oxytocin from the posterior pituitary gland.
- This hormone causes the contraction of myoepithelial cells 1 in alveoli and ducts, which results in the ejection of milk.
- The sensory stimulation also inhibits the release of prolactin j inhibiting factor.
- This leads to the release of prolactin from the anterior pituitary resulting in the secretion of milk from the breast.