
Disorders Of the Respiratory System
Obstructive Lung Disease
Obstructive lung diseases are the second (after cardiovascular diseases) leading cause of death in the adult population in India. Obstructive lung disease refers to a group of diseases that share a common feature—difficulty in expelling air from the lungs.
- Asthma
- Chronic bronchitis
- Emphysema
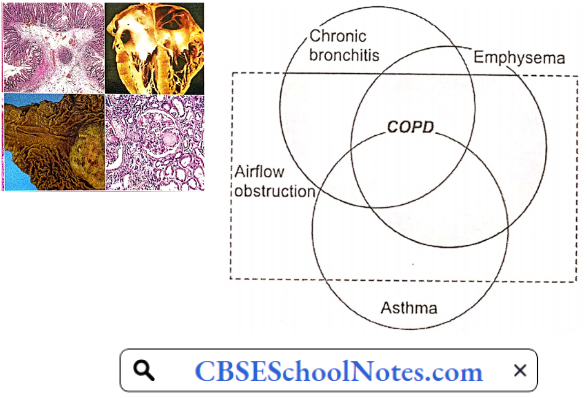
All three disorders have an increased airway resistance, but, are caused by a different mechanism in each case. However, often there is an overlap. In old cases of bronchial asthma, some element of emphysema develops. In chronic bronchitis, some elements of bronchospasm are commonly present.
Chronic bronchitis and emphysema are considered a spectrum of chronic obstructive pulmonary disease (COPD) with some patients showing dominantly bronchitis, while others show dominantly emphysema.
Read and Learn More Pathophysiology
In bronchial asthma, chronic bronchitis, and emphysema, the common factor is increased airway resistance. Pathogenesis and pathophysiology of obstructive lung disease can be explained only if the reader is familiar with the role of mucociliary clearance in respiratory mucosa and the physiology of airway resistance.
Mucociliary Clearance: From the trachea down to the terminal bronchioles, the respiratory mucosa is characterized by the presence of cilia, goblet cells, and submucosal mucous glands. The cilia are covered with a blanket of mucus, which traps any incoming particle greater than 5 p in size.
The ciliary movement of adjacent cells is so coordinated that it produces waves of ciliary motions from the distal to the proximal parts of the tracheobronchial tree. As a result, mucus blanket on the top of cilia laden with dust particles or bacteria is propelled upwards till it readies the oropharynx, where it is swallowed or expectorated.
Mucodliary clearance is a critical factor in the protection of the upper respiratory tract.
Airway Resistance
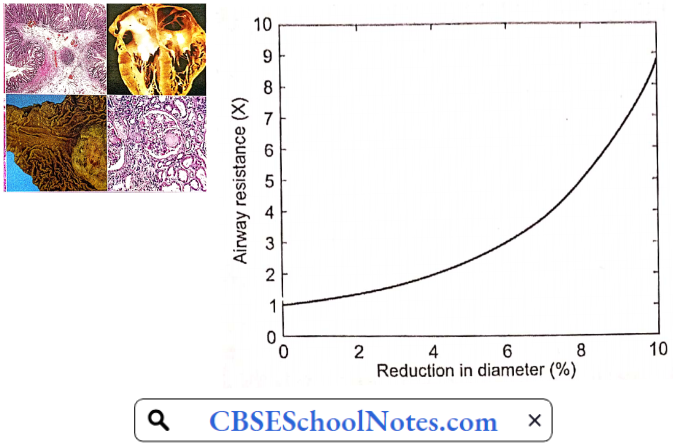
Resistance in the airways (RaW) is basically determined by the same factors that determine vascular resistance:
R = \(\frac{8 n L}{\pi r 4}\)
n = gas viscosity; L = airway length; r = radius
In the airways, the variable factor is the radius of the airways. A given reduction in the radius of bronchi results in a fourfold increase in airway resistance. Even a 4% reduction in airway diameter doubles the airway resistance.
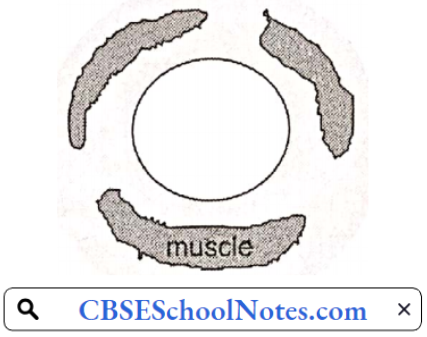
Lower Airway Resistance: The physiological control of airway resistance lies in the medium-sized bronchi (2-4 mm diameter). These airways contain, besides supporting cartilage, large amount of smooth muscle. Smooth muscle contraction can substantially increase airway resistance by reducing airway radius. The lumen of these bronchi can be altered by the following factors
- Bronchomotor muscle tone
- Radial traction by lung parenchyma
- Transmural pressure
- Luminal mucus
Bronchial Muscle Tone: Bronchial muscle tone is the chief factor that determines bronchial lumen size. It is chiefly regulated by parasympathetic neural discharge. In allergic asthma, a large number of local chemical mediators, such as histamine, prostaglandins, leukotrienes, kinins, etc. are released. All these mediators produce varying degrees of bronchial muscle spasm.
In chronic bronchitis also, there is some degree of bronchospasm. Circulating epinephrine can produce bronchodilation by acting on β2 receptors present on the bronchial smooth muscle. β2 agonists are used in the treatment of bronchial asthma.
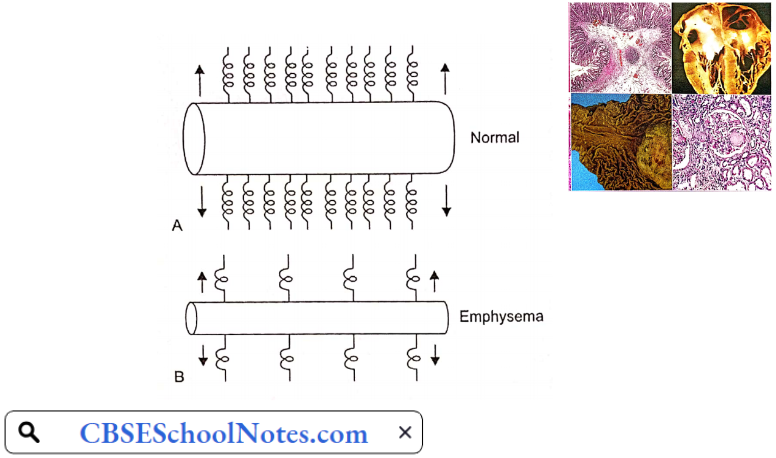
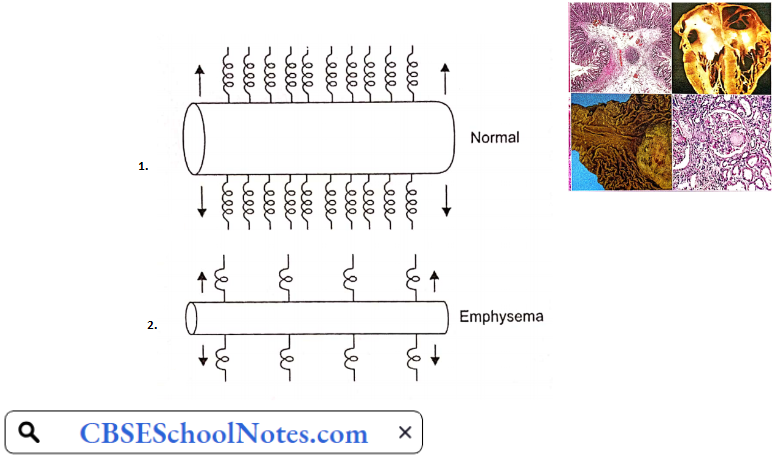
Radial Traction By Lung Parenchyma: Bronchi and bronchioles are surrounded by lung parenchyma, whose constant pull helps the patency of the airways. This supportive action is called radial traction. Parenchymal destructive diseases, such as emphysema, cause loss of radial traction. As a result, small airways collapse. That is the chief mechanism of bronchial narrowing in emphysema.
Transmural Pressure: During inspiration, intrapleural pressure is negative with respect to intrapulmonary pressure which helps to keep airways open. A similar situation exists during tidal expiration also. However, during forced expiration, intrapleural pressure becomes strongly positive, which tends to cause dynamic airway collapse.
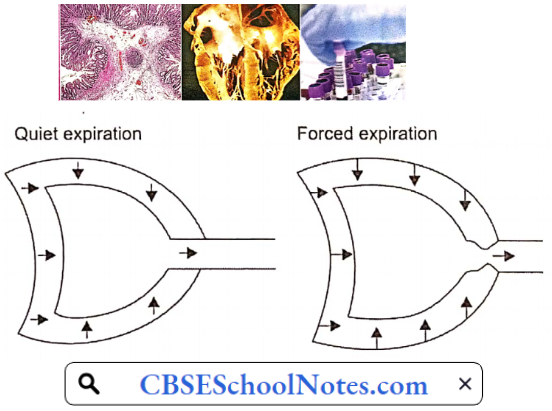
In emphysema, as explained later, expiration is brought about by the active contraction of expiratory muscles. The dynamic airway collapse causes expiratory flow limitations, i.e. beyond a point, increased expiratory effort does not produce further increase in air outflow. The problem is worsened in emphysema due to loss of radial traction, as well.
Mucus In Airways: The presence of mucus or other extraneous material in the airway lumen increases airway resistance. Cigarette smoking or respiratory infections enhance the secretion of submucosal mucous glands as well as mucosal goblet cells in the respiratory tract.
Bronchial Asthma
It is a disease characterized by recurrent attacks of breathlessness and wheezing, which vary in severity and frequency from person to person. Between the attacks, the patient’s breathing is normal. Worldwide, around 250,000 people die every year as a result of asthma.
Bronchial Asthma Symptoms
- Wheezing (a whistling sound arising from the lung during breathing)
- Tightness in the chest
- Shortness of breath
- Trouble sleeping caused by shortness of breath, coughing or wheezing
- Coughing or wheezing attacks that are worsened by a respiratory virus, such as a cold or the flu
Asthma Triggers: Exposure to various irritants and substances that trigger allergies (allergens) can trigger signs and symptoms of asthma. Asthma triggers are different from person to person and can include
- Airborne substances, such as pollen, dust mites, mold spores, pet dander, or particles of cockroach waste
- Respiratory infections, such as the common cold
- Physical activity (exercise-induced asthma)
- Cold air
- Air pollutants and irritants, such as smoke
Pathogenesis: The pathology of bronchial asthma consists of reversible bronchial narrowing associated with a spasm of smooth muscle in the wall of the airways (bronchi). The airway hyper-responsiveness is a fundamental disorder. The airway smooth muscle shows an exaggerated response to a variety of triggers such as seasonal outdoor allergens (pollens) or allergens derived from house dust, mites present in carpets, beds, or domestic animals or cockroaches.
- There is a genetic predisposition to bronchial asthma. A substantial percentage of asthmatic patients have elevated IgE levels (a sign of allergic predisposition) and a history of additional allergic disorders.
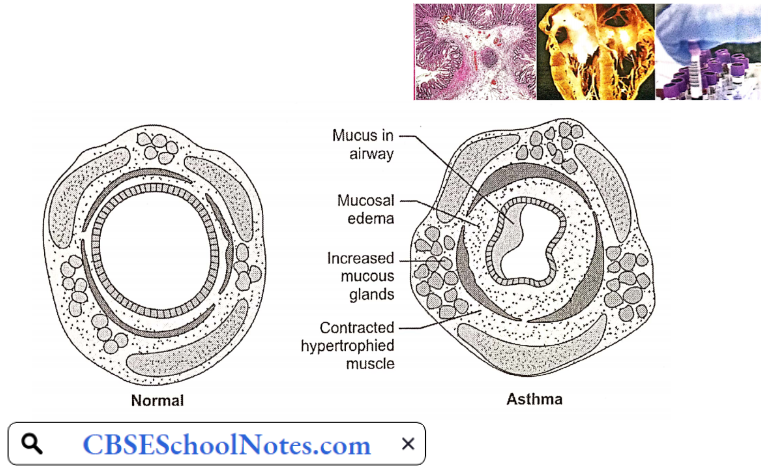
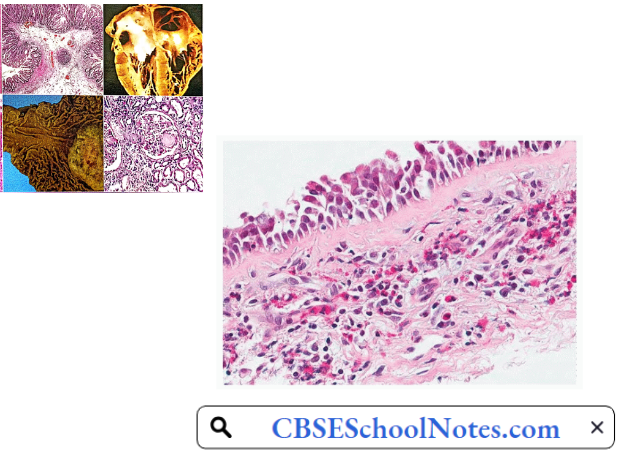
- Histological examination of small bronchi reveals epithelial damage, hypertrophy, and hyperplasia of bronchial smooth muscle, enlargement of mucous glands, increased number of goblet cells, and infiltration of the bronchial wall with eosinophils and lymphocytes.
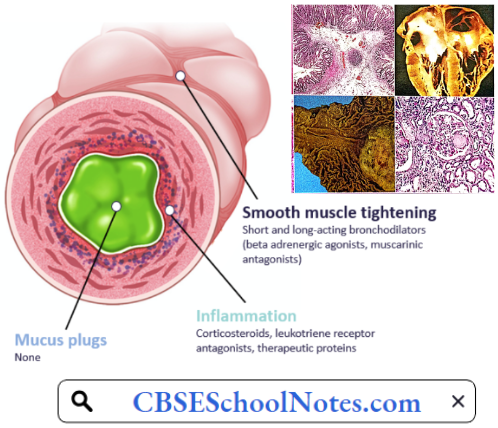
- The inflamed tissues respond to any of the triggers by release of mediators such as histamine and bradykinin by the mast cells and eosinophils in the bronchial mucosa. These mediators produce bronchospasm and increased mucus secretion.
The combined effect of bronchoconstriction and increased mucus secretion produces a critical narrowing of airways and increased airway resistance, especially during the expiratory phase. During an asthmatic attack, though breathing difficulty is felt during inspiratory phases, it becomes worse during expiratory phases of respiratory cycles.
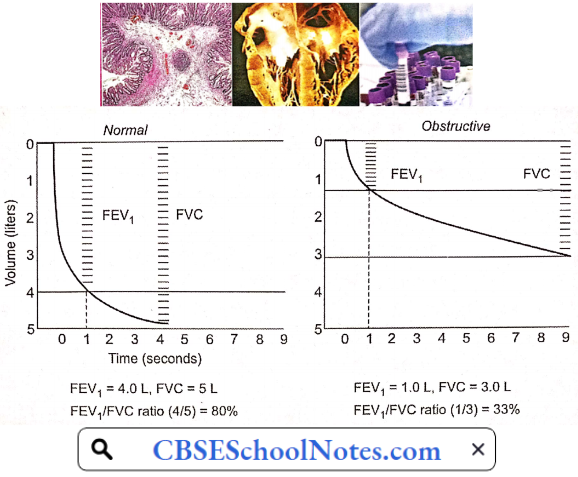
Confirmatory Pulmonary Function Tests
- Forced vital capacity (FVC) is decreased
- Forced expiratory volume 1st second/vital capacity ratio (FEV1/FVC ratio) is decreased.
- Peak expiratory flow rate (PEFR) decreased.
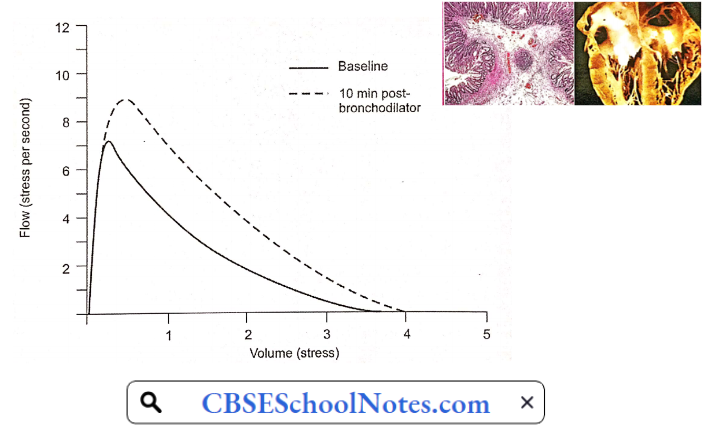
- Increase in FEV1/VC ratio and PEFR when tested after inhalation of a bronchodilator drug.
Bronchial Asthma Risk Factors
- Family history.
- Viral respiratory infections during infancy and childhood.
- Other Allergies: Having an allergic condition, such as eczema or allergic rhinitis is a risk factor for developing asthma.
- Smoking.
- Air pollution.
- Obesity.
Bronchial Asthma Complications
- Frequent attacks of bronchial asthma interfere with day-to-day life.
- Acute severe asthma may progress to a life-threatening condition known as status asthmaticus.
- COPD (emphysema) in later life.
Pathophysiological Basis Of Treatment: An attack of bronchial asthma terminated by administration of a bronchodilator drug.
Chronic Obstructive Pulmonary Disease (COPD)
COPD is defined as a chronic, slowly progressive disorder characterized by airflow obstruction which continues over several months. Bronchial asthma, though involves airflow obstruction, is excluded by this definition. COPD starts as chronic bronchitis, which over the years develops into emphysema.
Chronic Obstructive Pulmonary Disease Symptoms And Signs: Signs and symptoms of COPD may include
- Cough and copious sputum
- Shortness of breath, especially during physical activities
- Wheezing
- Chest tightness
- Blueness of the lips or fingernail beds (cyanosis) (later stages)
- Frequent respiratory infections
- Swelling in ankles, and feet (later stages)
Aetiology
- Cigarette Smoking: Cigarette smoking is considered to be the most important cause of COPD. Cigarette smoke contributes to the development of COPD through a number of mechanisms
- Inhibits ciliary clearance function in bronchial mucosa
- Inhibits function of alveolar macrophages
- Causes hypertrophy of goblet cells and mucous glands
- Provokes release of elastase from polymorphonuclear neutrophils
- Causes destruction of alveolar parenchyma by inhibiting antitrypsin
- Increases airway resistance by stimulating irritant receptors
- Air Pollutants: Almost 3 billion people worldwide use biomass and coal as their main source of energy for cooking, heating, and other household needs. In these communities, indoor air pollution is responsible for a greater fraction of COPD risk than smoking or outdoor air pollution.
- Biomass fuels used by women for cooking account for the high prevalence of COPD among nonsmoking women in parts of the Middle East, Africa, and Asia. Indoor air pollution resulting from the burning of wood and other biomass fuels is estimated to kill two million women and children each year.
- Frequent lower respiratory infections during childhood.
- Congenital alpha-1 antitrypsin deficiency.
- Occupational dust and chemicals (such as vapors, irritants, and fumes)
Pathophysiology
COPD with Predominant Bronchitis: In such patients, the major pathology is increased activity of hypertrophic and hyperplastic mucus-secreting apparatus (goblet cells and mucous glands) throughout large and small airways. Excessive production of thick and viscid mucus results in characteristic cough and copious purulent sputum.
- The airway obstruction is primarily due to these changes in tire terminal bronchioles. Besides intraluminal secretions, some degree of bronchospasm, or thickening of the airway wall by edema, inflammation, or fibrosis contributes to the increased airway resistance.
- A component of airway hyper-responsiveness may further aggravate bronchial obstruction resulting in what is called asthmatic bronchitis.
- In oxidatively pure chronic bronchitis, pulmonary parenchyma is mostly intact, and oxygen diffusion capacity is near normal. However, the patient shows a more marked decrease in arterial pO2 (45-50 mmHg) as well as moderately elevated pCO2 (50-60 mmHg) and marked polycythemia.
- The abnormalities in blood gases arise chiefly from uneven ventilation/perfusion in different parts of the lungs. Some bronchioles are obstructed by mucus/inflammation/edema causing a marked decrease in ventilation, but fairly well-maintained perfusion. The physiological shunts lead to hypoxia and polycythemia.
- Increased pulmonary vascular resistance is an important feature of chronic bronchitis. It mainly results from chronic hypoxia. Other contributory factors include increased polycythemia, increased pCO2, and acidosis.
Confirmatory Pulmonary Function Tests: Forced vital capacity (FVC) is decreased
- Forced expiratory volume 1st second/vital capacity ratio (FEV1/FVC ratio) is decreased.
- Peak expiratory flow rate (PEFR) decreased.
- There is no significant improvement in FEV1/ FVC ratio and PEFR when tested after inhalation of a bronchodilator drug.
- Total lung capacity (TLC) is normal.
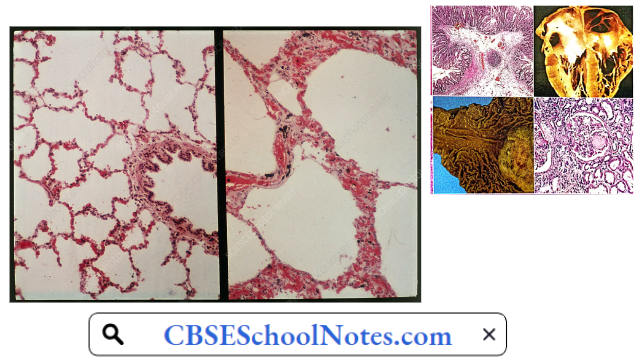
COPD With Prominent Emphysema: In such a patient, the primary problem is the degeneration of alveolar tissue. The destruction of air space walls reduces the surface area available for the exchange of oxygen and carbon dioxide during breathing.
- It also reduces the elasticity of the lung itself, which results in a loss of support for the airways that are embedded in the lung, leading to a decrease in the elastic recoil of the lungs.
- Therefore, the force that normally drives air out of the lungs during expiration decreases. Due to disruption of the alveolar septa, the support that keeps the small airways open due to transmural pressure is lost.
- Due to the loss of elastic fibers, compliance of the lungs increases, and the lungs are inflated to a larger volume for a given degree of increase in intrapulmonary pressure. The total lung capacity increases and the lungs remain permanently inflated. Residual volume and functional residual capacity are both increased.
- The chest becomes barrel-shaped. The diaphragm remains permanently flattened. As a result, diaphragm contraction cannot contribute to inspiratory effort. Inspiration is produced by the contraction of external intercostals only.
Due to the loss of elastic fibers, expiration is produced by the active contraction of expiratory muscles rather than by the passive recoil of elastic fibers. This results in dyspnoea and increased energy cost of work of breathing.
Confirmatory Pulmonary Function Tests
- Forced vital capacity (FVC) is decreased
- Forced expiratory volume 1st second/vital capacity ratio (FEV1/FVC ratio) is decreased.
- Peak expiratory flow rate (PEFR) decreased.
- There is no significant improvement in FEV1/ FVC ratio and PEFR when tested after inhalation of a bronchodilator drug.
- Total lung capacity (TLC) is increased.
Confirmatory Pulmonary Function Tests Complications
- Frequent respiratory infections
- Cyanosis
- Polycythaemia
- Congestive heart failure
- Respiratory failure
Pathophysiological Basis of Treatment
- Cessation of smoking
- Bronchodilators
- Antibiotics
- Oxygen therapy when the patient has cyanosis in the later stages of COPD
- Treatment of congestive heart failure (in later stages)