
Liver
The liver is an accessory digestive gland. It develops as an outgrowth of the entodermal epithelium of the duodenum. The connection between the duodenum and liver develops as a bile duct. The liver is the largest gland in the body weighing about 1500 g.
It has a double blood supply, i.e., the arterial blood from hepatic arteries and venous blood from the veins of digestive tubes and spleen through portal vein.
Blood from both the sources (arterial and venous) passes through liver sinusoids and ultimately drains into hepatic veins that join the inferior vena cava. Thus, the substances absorbed from the intestines first come in contact with the liver cells.
Gross Histological Organization of Liver
The liver is surrounded by a thin connective tissue capsule and is divided into many lobes, i.e., left, right, caudate and quadrate lobes.
- The hepatic artery, bile duct and portal vein enter the liver at the porta (hilus-a short transverse fissure on the inferior surface of the liver). Artery and veins repeatedly branch to supply hepatic lobules.
- Although the bile duct also follows the same course, it carries bile in the opposite direction, i.e., away from liver lobules.
- The connective tissue entering the liver at the porta, along with other structures, branches within the liver to form the partial boundary of liver lobules and to support the branching vessels and ducts.
- In humans, the lobules of the liver are not well defined because their interlobular connective tissue is poorly developed. The interlobular connective tissue is also called interlobular septa.
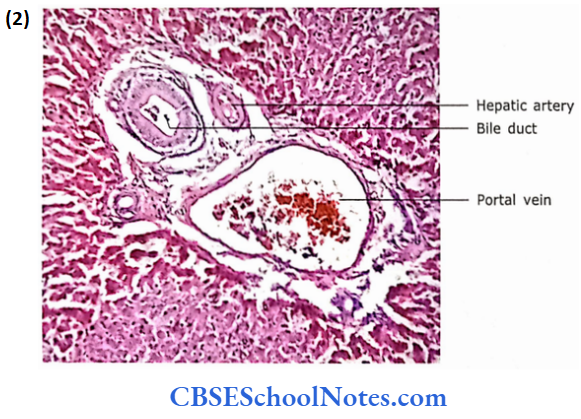
- The branches of the portal vein, hepatic artery and bile duet course together in the connective tissue interlobular septa as a triad, called as a portal triad.
Microscopic Organization of Liver
1. Liver Lobule
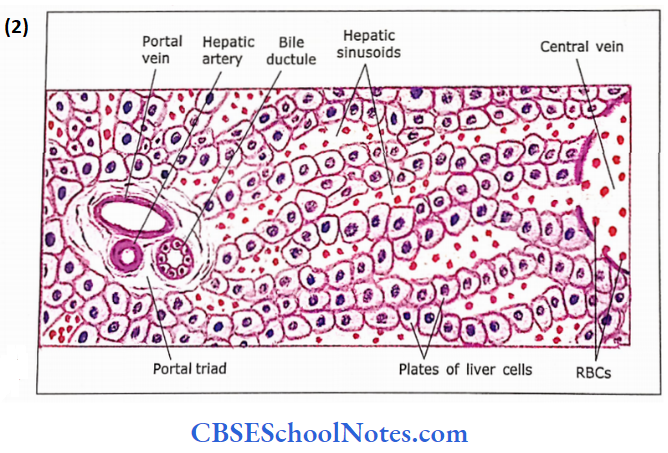
The substance of the liver is made up of liver lobules that form the structural and functional unit of the organ. In cross¬section, the shape of a liver lobule is somewhat similar to a hexagon.
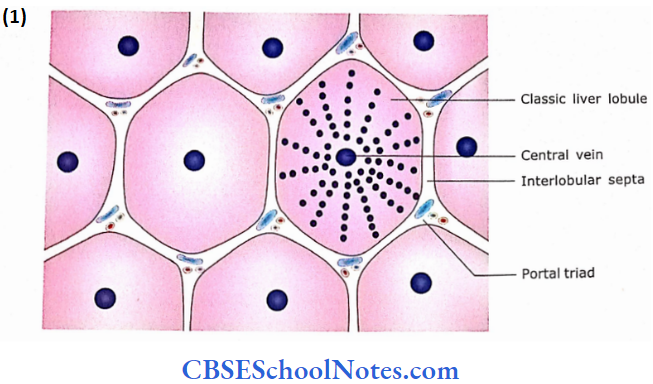
In the human liver, the connective tissue between adjacent lobules is scanty. Hence, no well-defined separation between adjacent lobules is seen. Therefore, the liver tissue of one lobule merges with that of adjacent lobules
At the corners (angles) of the hexagon (lobule) there are small triangular areas of the connective tissue that contain portal triads (branches of the portal vein, hepatic artery and an interlobular bile duct. Thus around the periphery of each lobule, there are several portal triads.
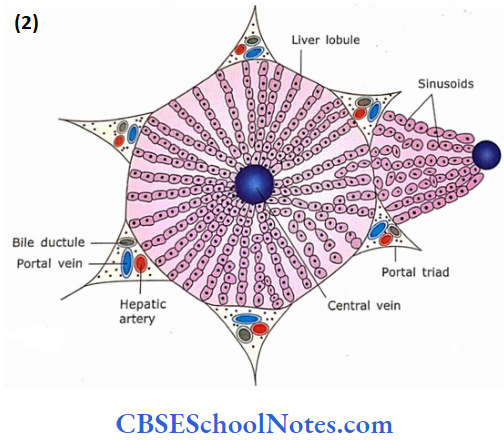
As the boundaries of hexagonal lobules are touching each other, every portal triad forms a partial boundary for more than one lobule. In the centre of each hepatic lobule is a central vein The central vein drains blood from lobules into hepatic veins. Radiating from the central vein are hepatic cells (hepatocytes), which are arranged in plates (laminae) that are usually one cell thick. These plates anastomose to form a three-dimensional network.
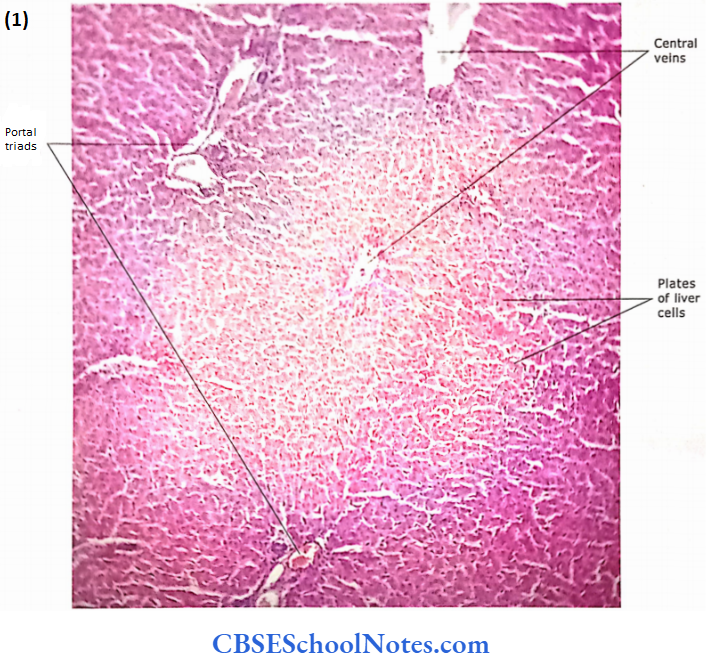
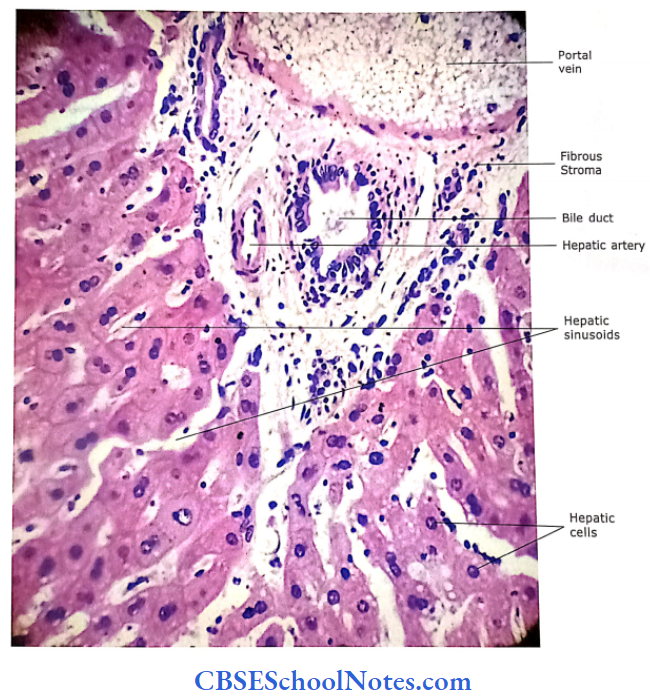
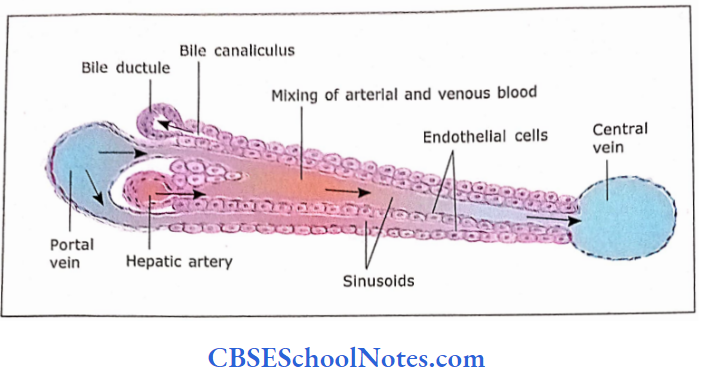
Between the plates (laminae) are blood passageways called sinusoids. The lateral branches of the small hepatic artery and portal venules, which arise from the portal triads, join to form the hepatic sinusoids. The flow of blood in sinusoids is from the periphery of the lobule to toward the central vein.

The bile canaliculus is a small channel, which occurs at the interphase between an adjacent pair of liver cells in a plate. The walls of the canaliculus are formed by the plasma membrane of the opposite hepatocytes. These canaliculi drain bile, produced by hepatocytes, toward the bile duct at the periphery of the lobule, in the portal triad.
A polygonal hepatic cell is thus exposed on its two or three sides to which blood flows toward the central vein. The same hepatic cell also forms bile canaliculi on its 3 or 4 remaining sides.
Liver Remember:
The structural and functional unit of the liver is the “hepatic lobule” which looks somewhat similar to a hexagon. There is no well-defined separation between adjacent lobules and at the corners (angles) of the hexagon (lobule) there are small triangular areas that contain “portal triads.” In the centre of each hepatic lobule is a central vein.
Three Different Types of Liver Lobules
The following three kinds of structural and functional lobules are described in
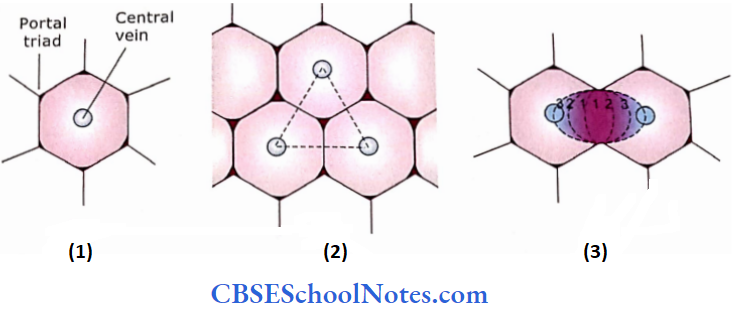
- Classical liver lobule:
- It has a central vein located in the centre of the lobule and portal triads at the edges of the cross-sectioned lobule.
- The blood flows from the periphery to cen¬tre and secretion (bile) from the centre toward the periphery (portal triad).
- Portal lobule:
- It is a triangular area of the liver parenchyma around each portal triad. It includes the portions of three neighbouring classical lobules. In this kind of lobule, the portal triad is in the central position and central vein at the edges of the cross-sectioned lobule.
- This lobule indicates that blood supply to liver parenchyma goes from the centre to the periphery and bile secretion drains into the central duct.
- Liver acinus:
- This is the most commonly accepted structural and functional lobule. Liver acinus is elliptical and includes portions of two neighbouring classical lobules.
- In the centre of the acinus are terminal branches of the hepatic arteriole and portal venule extending laterally from the portal triad, and the central vein at each pole of the cross-sectional structure.
- It is considered that an acinus has three zones, i.e., zones 1, 2 and 3.
- Zone 1 is close to blood vessels and zone 3 is close to a central vein.
- Thus, zone 1 is supplied with blood that is most oxygenated and rich in nutrients and zone 3 gets the least.
- The cell degeneration as seen in toxic damage to the liver is first observed in the central part (zone 1) as it is exposed to toxin before zone 3, while degeneration secondary to hypoxia is first observed in zone 3.
Lobules liver Remember:
Three different types of lobules are described in the liver, i.e., classical lobule, portal lobule and hepatic acinus. The classical hepatic lobule is a roughly hexagonal mass of tissue. The portal lobule connects three central veins and surrounds a portal triad. The liver acinus is the smallest functional unit of hepatic parenchyma.
Hepatic Sinusoids:
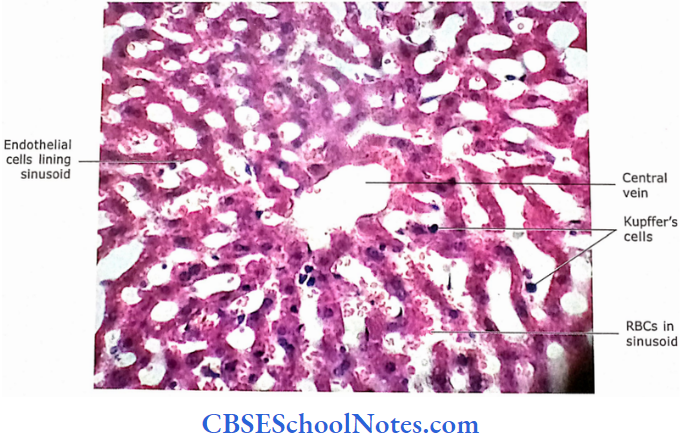
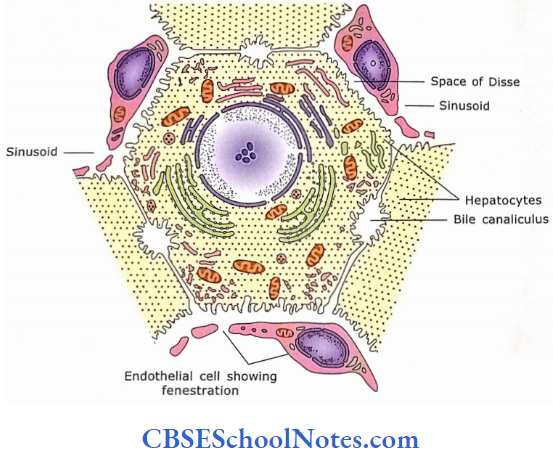
The sinusoids are between the hepatic laminae (plates) and follow their branching and anastomoses Their calibre is larger than capillaries (9-12 pm). Sinusoids are lined by two kinds of cells, i.e., endothelial cells and phagocytic (Kupffer) cells.
- The lining of endothelial cells is not continuous; gaps are seen between neighbouring endothelial cells. The endothelial cells have fenestrations that are not covered by the diaphragm.
- The basal lamina surrounding the sinusoids is either incomplete or absent. The sinusoidal epithelium is separated from the underlying hepatocytes by a small space, called the space of Disse (perisinusoidal space).
- The particulate matter less than 0.5 m in diameter may pass through the lumen of the sinusoid into space of the Disse
The phagocytic Kupffer cells lie by the side of endothelial cells and send cytoplasmic processes (filopodia) between adjacent endothelial cells. They do not form junctions with the neighbouring endothelial cells. Kupffer cells may send their cytoplasmic processes in the space of Disse through fenestrations or the gap between two endothelial cells.
Many microvilli project in the space of Disse from the basal surface of the hepatocytes. They increase the sur¬face area for the exchange of material between blood and liver cells. Blood plasma freely enters the Space of Disse and directly bathes the surface of the hepatic cells.
Ito cells (hepatic stellate cells):
Ito cells (hepatic stellate cells are another type of cells found in perisinusoidal spaces. These cells are involved in the storage of vitamin A and lipids. In chronic inflammation or cirrhosis, they differentiate into cells with characteristics of myofibroblasts, which produce collagen fibres resulting in liver fibrosis.

Hepatic Sinusoids Remember:
Hepatic sinusoids are vascular channels between the plates of hepatocytes. Sinusoids are lined by endothelial and phagocytic (Kupffer) cells. Gaps are seen between neighbouring endothelial cells. The endothelial cells have fenestrations that are not covered by the diaphragm. Perisinusoidal space (space of Disse) is seen between sinusoidal endothelium and hepatocytes.
2. Hepatocytes (Liver Cells)
Each liver cell is polygonal in shape possessing a relatively large nucleus (may be binucleated) and a single nucleolus. Hepatocytes have granular acidophilic cytoplasm but also contain basophilic bodies.
- Hepatocytes constitute about 80% of liver volume. Their life span is of about 5 months and are capable of regeneration.
- The polyhedral liver cells may have 5-12 sides and are about 20-30 cm in width. These cells form hepatic cords, which may branch and anastomose frequently.
- Some sides of the cells are exposed to the sinusoids, and the sides which are not exposed to sinusoids show infolding between adjacent cells to form bile canaliculi. The bile canaliculi form a network within the cell plates.
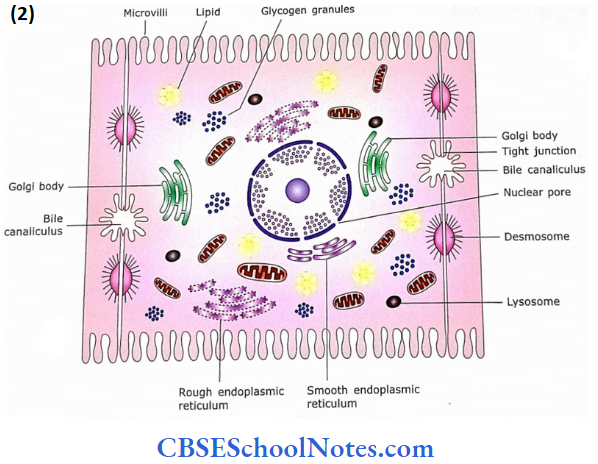
3. Electron Microscopic Structure of Liver Cells
The electron micrograph of liver cells shows the presence of numerous oval mitochondria with leaf-like cristae. Hepatocytes contain rough and smooth endoplasmic reticulum, free ribosomes, and many small Golgi complexes located near the bile canaliculi. There are many lysosomes and peroxisomes. Peroxisomes are involved in the detoxification of alcohol. Glycogen granules and lipid vacuoles are also seen.
4. Blood Circulation
The hepatic artery and portal vein after entering the porta hepatitis divide repeatedly to lie between hepatic lobules.
- The blood vessels present in portal triads are called interlobular vessels.
- The interlobular vessels of portal triads branch into vessels, which lie at the periphery of the lobules (between the lobules).
- These vessels are called distributing vessels.
- The distributing vessels are branches of the portal vein (which brings deoxygenated blood along with J-absorbed products of digestion) and the hepatic artery (which brings arterial blood) rich in oxygen.
- The distributing vessels send branches to liver sinusoids.
- The flow of mixed blood (arterial and venous) in sinusoids is from the periphery toward the central vein. The central veins join to form hepatic veins, which ultimately drain into the inferior vena cava.
Liver Functions
- The liver has several functions, most of which are performed by hepatocytes.
- Liver cells produce not only exocrine secretion bile but also perform many endocrine functions.
- It modifies the structure and functions of many hormones.
- The liver produces most of the circulating plasma proteins.
- It is involved in many metabolic pathways, storage of vitamins and detoxification of toxins.
- The liver has several functions, most of which are performed by hepatocytes.
- Liver cells produce not only exocrine secretion bile but also perform many endocrine functions.
- It modifies the structure and functions of many hormones. The liver produces most of the circulating plasma proteins.
- It is involved in many metabolic pathways, storage of vitamins and detoxification of toxins.
Liver Clinical Application
Cirrhosis of the Liver:
- The function of liver cells is to detoxify drugs and toxic chemicals including alcohol.
- Those people who consume alcohol regularly for many years may develop a disease of the liver called cirrhosis.
- In this disease, there occurs the necrosis (death) of liver cells. These dead cells are replaced by fibrous tissue.
- The patient gradually becomes weak and develops jaundice due to the obstruction in the flow of bile.
- The other agents, which may cause cirrhosis are drugs, chemicals, hepatitis virus and autoimmune liver disease.
- Chronic viral hepatitis [^(B or C type) may also lead to cancer of the liver.
Liver Regeneration
The liver has high regenerative power. It can regenerate after toxic damage and even if a portion of it is excised.
Gallbladder
The gall bladder is a temporary storehouse of bile and concentrates it by water reabsorption.
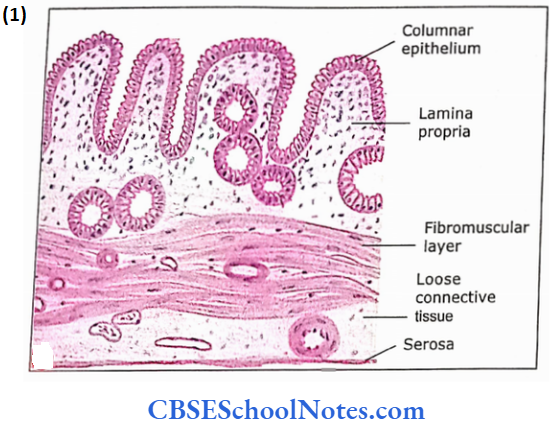
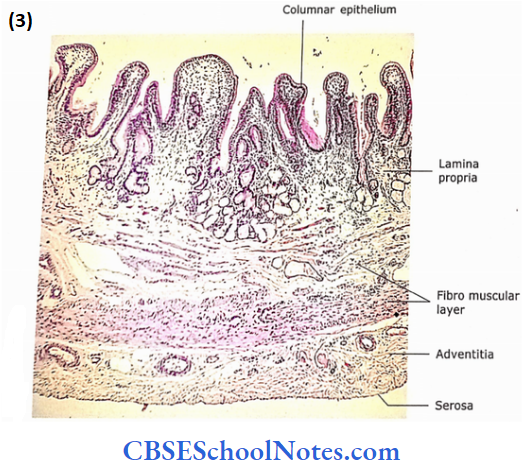
It consists of the following layers:
- Mucosa
- Fibromuscular layer
- Adventitia/Serosa
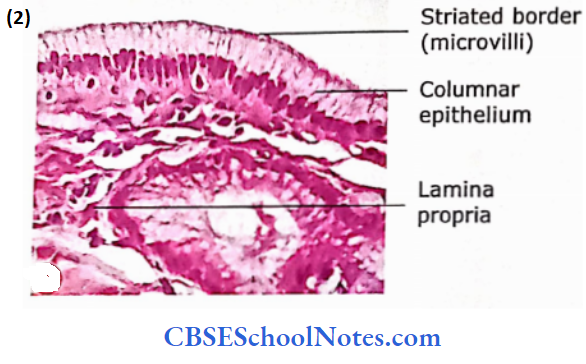
1. Mucosa:
It consists of simple tall columnar epithelium and lamina propria of loose connective tissue.
- The mucosal glands and muscularis mucosae are absent.
- The mucosa is thrown into small folds when the gall blad¬der is empty. The gall bladder epithelial cells have a basally placed ovoid nucleus and faintly stained eosinophilic cytoplasm.
- These cells have many small microvilli on their apical surface.
- These cells are highly involved in the absorption of water from stored bile. Lamina propria is present but submucosa is absent.
2. Fibromuscular Layer:
- This layer is composed of randomly arranged smooth muscle fibres.
- In between muscle fibres is dense connective tissue that is rich in elastic fibres.
3. Adventitia/Serosa:
- There is a layer of dense connective tissue outside the muscle layer, which contains blood vessels, nerves and lymphatics.
- This layer is called adventitia. On its inferior surface gall bladder is covered by se-rosa, rest of it is covered by adventitia.
Gall bladder Remember:
The muscularis mucosae and submucosa are absent in the wall of the gall bladder. The release of bile from the gall bladder is controlled by cholecystokinin and vagal stimulation.
Gallbladder Clinical Application
Gallstones and Jaundice:
- Sometimes due to the presence of a higher concentration of bile acids in bile, there may occur the formation of stones in the gall bladder.
- If a gallstone obstructs the bile duct, it causes jaundice.
- Jaundice is a disease where there is the presence of an increased amount of bile pigments in the blood.
Pancreas
The pancreas is an accessory gland of digestion. This lies wholly outside the alimentary tract and is connected to it (duodenum) by an excretory’ duct(s). The pancreas is a mixed gland, i.e., it consists of an exocrine and an endocrine portion.
- The exocrine pancreas secretes pancreatic juice that helps in the digestion of carbohydrates, proteins and fats, while the endocrine pancreas secretes hormones, which regulate the metabolism of carbohydrates.
- The exocrine pancreas shows a similar structural organization as that of salivary glands.
- The secretory units of acini of the exocrine pancreas are tubuloacinar in shape and resemble a bunch of grapes where stems are comparable to the duct system and secretory acini are comparable to grapes.
- The endocrine units are called the islets of Langerhans. These are clusters of pale staining cells situated between the exocrine acini.
Pancreas Remember:
The pancreas is a mixed gland, i.e., exocrine and endocrine. The exocrine pancreas produces serous digestive juices and the endocrine pancreas produces hormones.
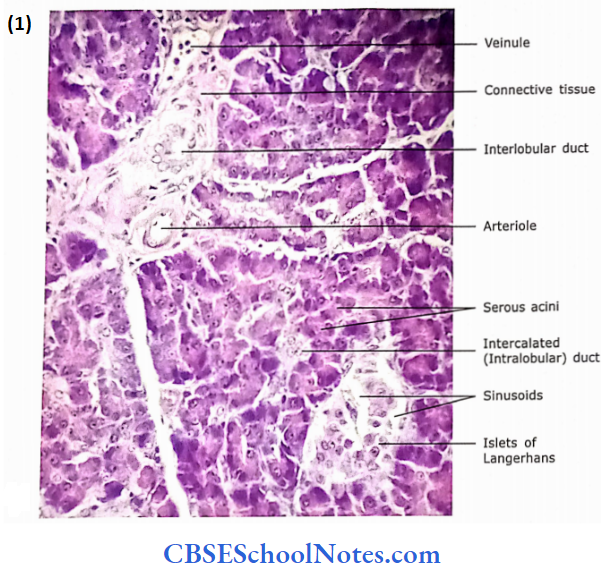
Histology of Exocrine Pancreas
The pancreas is covered with a very thin layer of loose con¬nective tissue capsule. Thin septa arise from this to divide the gland into many small lobules. These lobules are not very distinct. The interlobular connective tissue contains large ducts, blood vessels, and nerve fibres. The interlobular loose connective tissue surrounds the acini, small ducts and islets of Langerhans
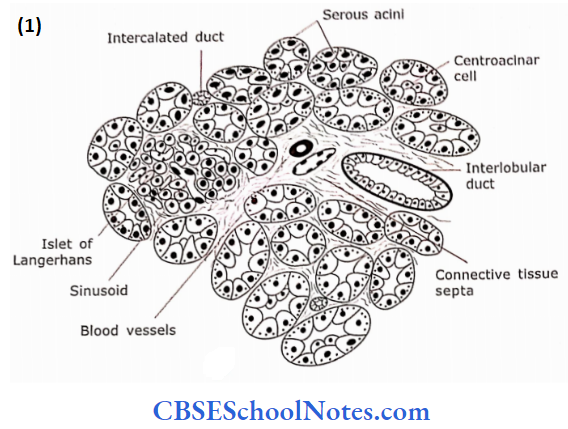
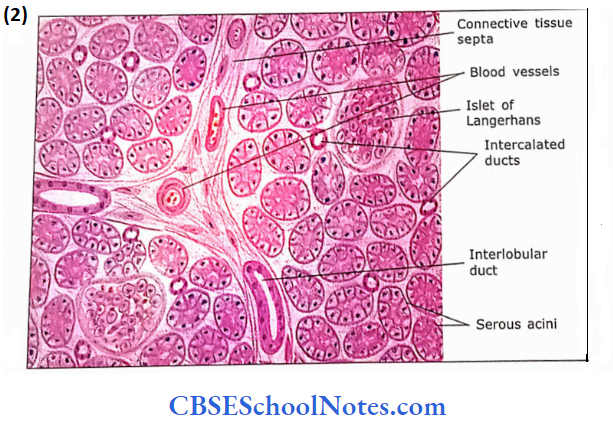
1. Pancreatic Acini
The pancreatic acini are serous. Their shape is either round or slightly elongated.
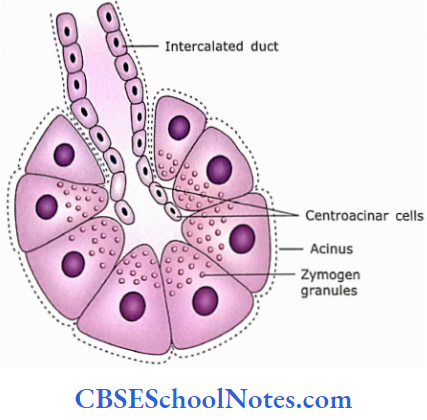
- These acini are lined by pyramidal cells and have small lumen. The intercalated duct begins within the acini (see below).
- The acinar cells show all the features of a serous-secreting cell. These cells have centrally placed round nuclei.
- The intranuclear region is intensely basophilic (stains with haematoxylin) because it contains a rough endoplasmic reticulum and many free ribosomes.
- The supranuclear region is filled with secretory granules called zymogen granules The apical portion takes eosinophilic staining or may stain light basophilic. These secretory granules contain the precursors of several digestive enzymes.
- These enzymes are amylase, lipase, ribonuclease, deoxyribonuclease, trypsinogen, chemo-trypsinogen, etc. The release of these enzymes is controlled by cholecystokinin and acetylcholine.
- The cholecystokinin is liberated by the small intestine (mostly duodenum), which acts on the receptors of pancreatic acinar cells.
- Similarly, stimulation of parasympathetic nerves secrete acetylcholine, which facilitates the secretion of enzymes from pancreatic acini.
 ‘
‘
- Islets of Langerhans
- Pancreatic acini
- Pancreatic lobule
- Blood vessels
- Interlobular duct
Islets of Langerhans Present Acini And Intrabular Ducts:

Pancreatic Remember:
The pancreatic acini are lined by pyramidal cells and have small lumen. They are serious in nature and manufacture and release digestive enzymes. Pancreatic exocrine secretion is controlled by hormones (cholecystokinin) and nervous system (acetylcholine).
2. Ducts
The pancreas, like salivary glands, has an extensive duct system, i.e., intralobular (intercalated), interlobular and main duct.
- The intralobular ducts are very small in diameter and lined by squamous to very low simple cuboidal epithelium.
- An intercalated duct commonly begins within the acinus. Therefore, the ends of intercalated ducts are surrounded by acinar cells.
- Cells of intercalated ducts add bicar¬bonate and water to the exocrine secretion. The acinar lumen may show pale staining cells of the intercalated duct. These cells are called centroacinar cells. There are no striated ducts in the pancreas.
- The intercalated ducts are short and open into ’ intralobular collecting ducts’, which are lined by cuboidal or low columnar epithelium.
- The interlobular ducts are lined with simple columnar epithelium and lie in connective tissue septa.
- The main duct is lined with tall columnar cells with occasional goblet cells.
Duct Remember:
The centroacinar cells are part of the intercalated duct. Cells of intercalated ducts add bicarbonate and water to the exocrine secretion.
Histology of Endocrine Pancreas
The endocrine component of the pancreas is in the form of small groups of cells (“islands”), which are scattered among the acini of the exocrine pancreas. These small groups of cells are called “islets of Langerhans.”
- The islets are lightly stained with H&E and thus can be easily differentiated from acini, which are darkly stained.
- The cells of islets are arranged as anastomosing plates or cords and permeated by a rich network of fenestrated capillaries. They pour their secretions directly into blood capillaries.
- The islets contain mainly four kinds of cells, which can be distinguished by special stains, but not by H&E.
These cells are designated as:
- α (alpha) cells: These are 20% of the total population of islet cells and secrete glucagon. Glucagon acts antagonistically to insulin.
- β (beta) cells: These are 70% of the total population and secrete insulin, which promotes the uptake of glucose.
- δ (delta) cells: These are 5% and secrete somatostatin, which suppresses the release of insulin and glucagon.
- PP cells: These cells secrete pancreatic polypeptides, which regulate acinar cell secretion (PP = protein polypeptide).
Pancreas Clinical Application
- Diabetes: Diabetes is caused by to impaired function of beta cells of islets of Langerhans. In this condition, these cells are unable to produce the required amount of insulin.
- A person suffering from diabetes has high blood levels of glucose. The glucose may also get excreted through urine. The disease if remains untreated may lead to atherosclerosis and partial blindness from degenerative changes in the retina.
- Diabetes occurs in two forms, i.e., type 1 and type 2:
- In type 1 the f3 cell of islets are destroyed before the age of 15 years. These patients are dependent on the injection of insulin as no insulin is produced by islets.
- Type 2 (non-insulin-dependent diabetes) usually occurs after 40 years of age and in.