Bones Of The Abdominal And Pelvic Regions
The bones of the abdominal region consist of five lumbar vertebrae and intervening intervertebral discs. The bones of the pelvic region consist of two hip bones (right and left), a sacrum, and a coccyx.
The right and left hip bones are joined anteriorly at the pubic symphysis and to the sacrum posteriorly to form a bony pelvis.
We shall first study the lumbar vertebrae, sacrum, and coccyx before studying the bony pelvis. Students are advised to review the features of a typical vertebra (as described in Chapter 4), before studying lumbar vertebrae
Lumbar Vertebrae
The lumbar region of the vertebral column consists of five lumbar vertebrae. The upper four vertebrae are typical while the fifth is atypical.
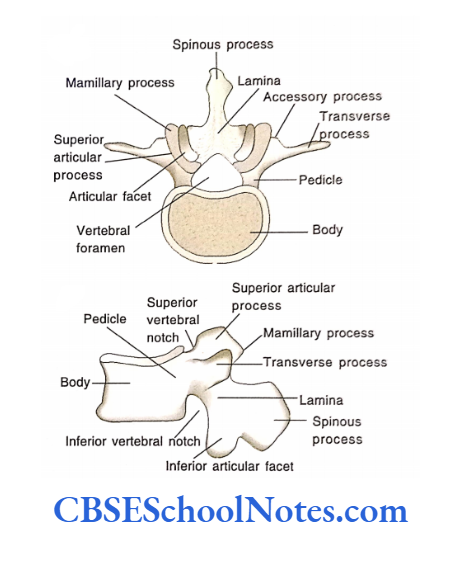
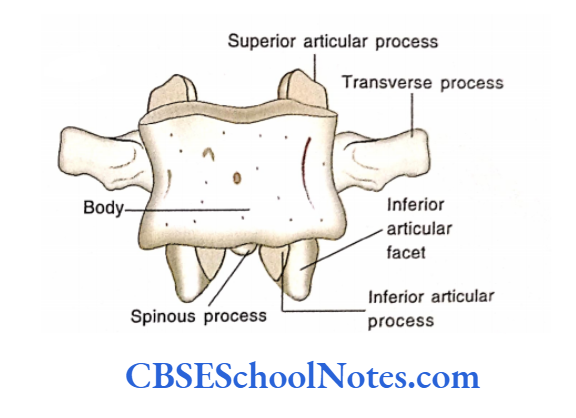
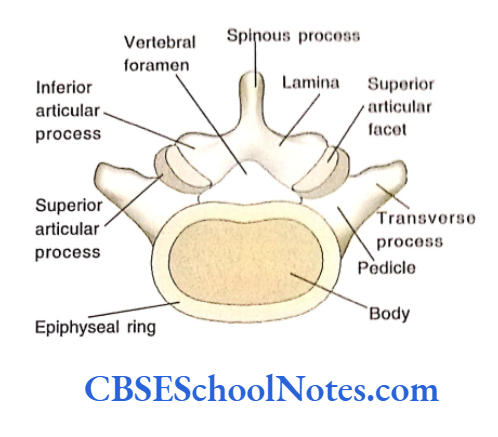
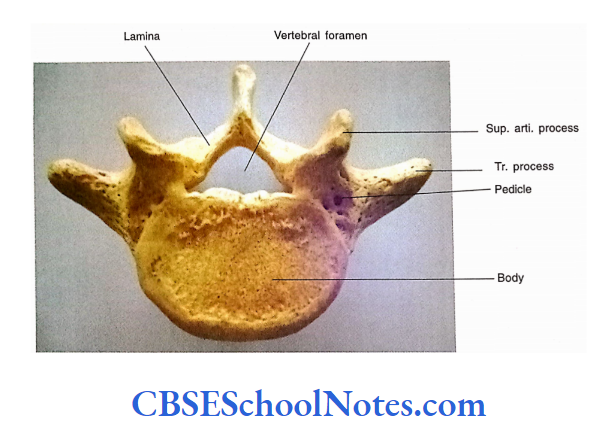
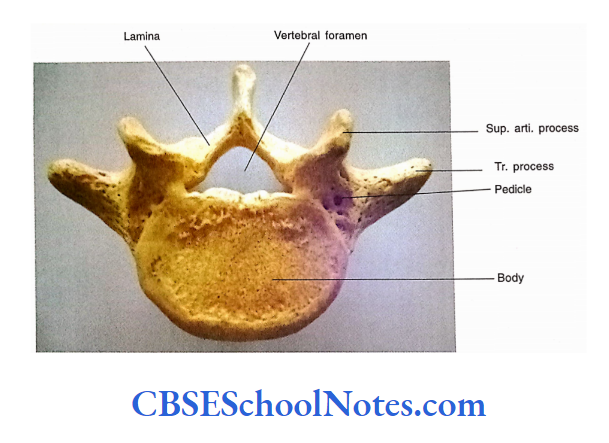
Features Of A Typical Lumbar Vertebra
Body
The bodies of lumbar vertebrae are large and kidney-shaped. The size of the lumbar vertebrae increases from above downwards as they have to bear the increasing weight of the body.
Pedicles
The pedicles are short and strong. They are directed backward and somewhat laterally. The superior vertebral notches are shallow while inferior notches are deep.
Lamina
These are broad and short and do not overlap one another as in the case of thoracic vertebrae.
Vertebral Foramen
The vertebral foramen is large and varies in shape, i.e., oval (LI) to triangular (L4).
Read and Learn More Human Osteology Notes
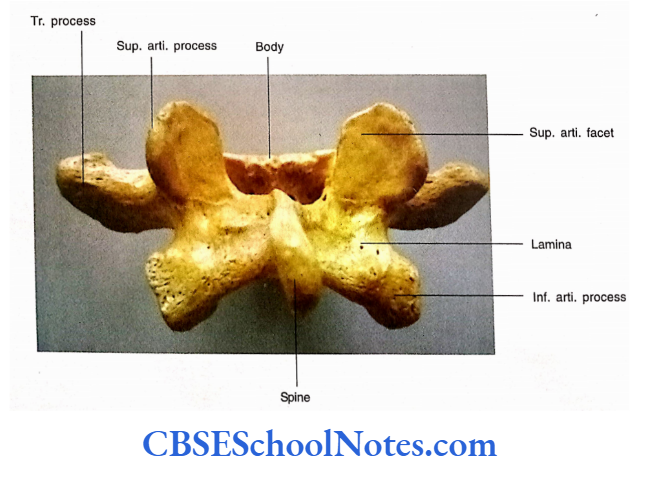
Transverse Processes
These are thin, long, and often have tapering ends. The posteroinferior aspect of the root of each transverse process bears a small projection called an accessory process.
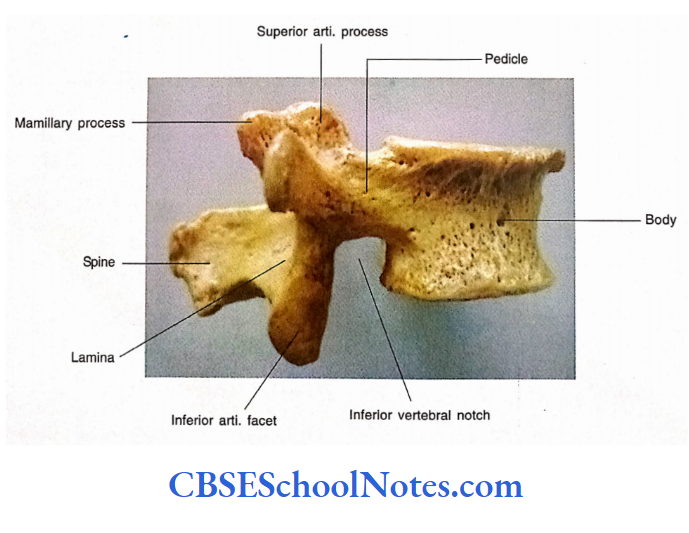
Superior Articular Processes
These are vertical curved processes and bear concave articular facets facing backward and medially. There is the presence of a nonarticular rough projection on the posterior border of the superior articular process called as mammillary process.
Inferior Articular Processes
These are also vertical processes. They bear a convex articular facet, which is directed forward and laterally.
Spinous Process
The spinous process of a typical vertebra is large, thick, horizontal, and quadrilateral in shape. It presents thickened posterior and inferior borders.
Features of Fifth Lumbar Vertebra
- The fifth lumbar vertebra is the largest of all the vertebrae. The body and transverse processes of L5 are very massive as they carry the weight of the whole upper body.
- The vertical height of the anterior surface of the body is higher as compared of the posterior surface.
- This fact is responsible for a prominent sacrovertebral angle (angle between the long axis of the lumbar column and the long axis of the sacrum).
- The transverse processes of L5 are very large and thick. They have a wide origin, i.e., they arise from the lateral aspect of the pedicle and also encroach on the side of the body.
- The transverse processes of L5 are massive because they are involved in the transmission of load from the body of L5 to the ilium (through the ilio-lumbar ligament) and to the sacrum (through the lumbo-sacral ligament).
- The spinous process of the L5 vertebra is short and directed backward and somewhat downwards.
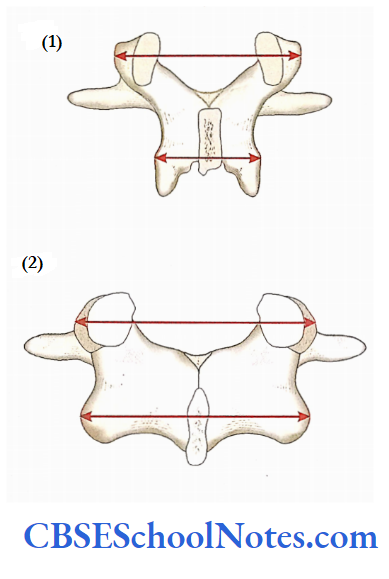
- The distance between two superior articular processes is almost equal to the distance between two inferior articular processes.
- (In the case of a typical lumbar vertebra the distance between two superior articular processes is more as compared to the distance between two inferior processes.
Clinical application
Lumbar Spinal Stenosis
- In this condition, there occurs the narrowing of the lumbar part of the vertebral canal.
- The condition may result due to bulging (prolapse) of the intervertebral disc, arthritic proliferation, or ligamentous degeneration.
- Sometimes stenosis may be congenital also. The stenosis causes compression of the spinal nerve roots of the cauda equina.
- The condition is usually treated surgically by laminectomy (excision of vertebral laminae) or by removing the entire vertebral arch.
Low Back Pain
- The neural arch at L4 and L5 levels is involved in the transmission of a considerable magnitude of load. This fact indicates that the joints between the articular facets may be the site for low back pain.
- Probably, the pain is due to stretching of the joint capsule (or transmission of load across it), which contains a nociceptive type IV receptor system (Pal and Routal, 1987).
Instability of Spine Following Laminectomy
About 20% of the load in the lumbar region passes through the laminae of lumbar vertebrae. Thus the laminectomy leads to instability of the lumbar column. Pal and Routal (1987) strongly recommended the preservation of the integrity of the articular facet joints in laminectomy.
Prolapsed or Herniated Disc
A prolapsed disc occurs when the nucleus pulposus pushes outward, distorting the shape of the disc.
If the annulus fibrosus of the disc ruptures (usually on the posterolateral aspect and most commonly at L4/L5 or L5/S1 levels) then the nucleus pulposus is herniated through the rupture.
Both in prolapsed or herniated disc surrounding tissue become inflamed and swollen. The tissue of the disc may press on the nerve or spinal cord, causing pain e.g. sciatica.
The Sacrum
The sacrum is composed of five fused sacral vertebrae in adults. It is a large, triangular wedge-shaped bone.
It is wedged between two hip bones and forms the posterior part of the bony pelvis. It transmits the weight of the upper body received through L5 to the pelvic girdle through sacroiliac joints.
The sacrum is triangular because there is a portion below the sacroiliac joint) is not involved in weight bearing hence its size diminishes rapidly.
The triangular sacrum presents an upper end or base. The base is formed by the superior surface of the SI vertebra.
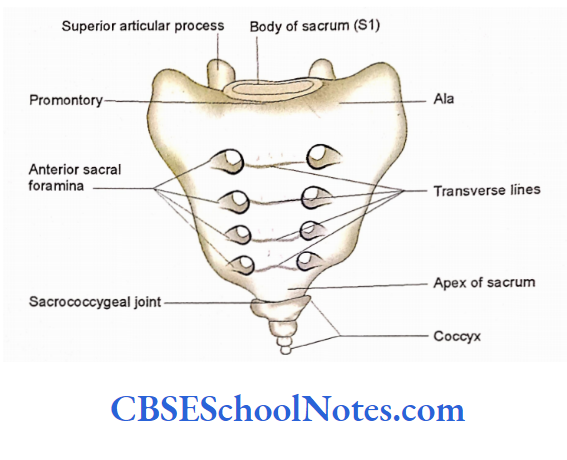
It articulates with the fifth lumbar vertebra at the lumbosacral joint. The lower end of the sacrum is tapering also known as apex. It articulates with the coccyx.
The sacrum presents an anterior (or pelvic) concave surface and a dorsal (or posterior) convex surface. The pelvic surface shows the presence of four pairs of anterior sacral foramina.
Similarly, the posterior surface also shows four pairs of posterior sacral foramina the sacrum also presents the right and left lateral sacrum also presents the right and left lateral of the right and left hip bones to form sacroiliac joints The Mcra( cam, the continuation of the vertebral canal in the sacrum The canal Bes posterior to the median part of the sacrum formed by fused bodies.
The sacral canal communicates with the anterior and posterior sacral foramina through which passes the ventral and dorsal rami of sacral nerves.
Anatomical Position
Hold the bone in such a way that the pelvic (anterior) surface is directed forward and downwards. In this situation, the base of the sacrum will look forward and upwards.
General Features
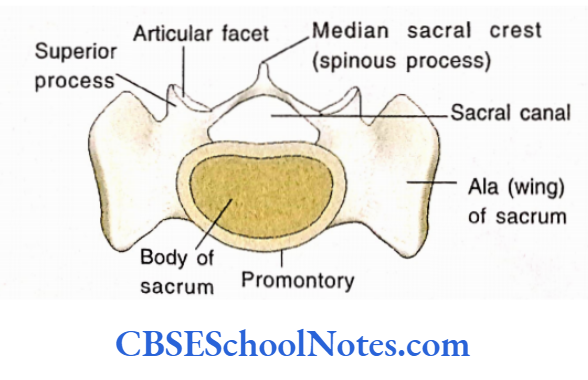
The base of the Sacrum
It is formed by the upper surface of the first sacral vertebra. The base consists of a centrally placed oval body and the upper surface of the right and left ala (lateral mass) on each side of the body.
Posterior to the body there is the presence of a triangular sacral canal bounded by thick pedicles and laminae.
The superior articular facets project upwards from the junction of the pedicles and laminae.
The superior articular facets of the sacrum articulate with the inferior articular facets of the 5th lumbar vertebra.
Posteriorly, there is a resence of a tubercle at the meeting point of two laminae. This tubercle represents the rudimentary spinous process.
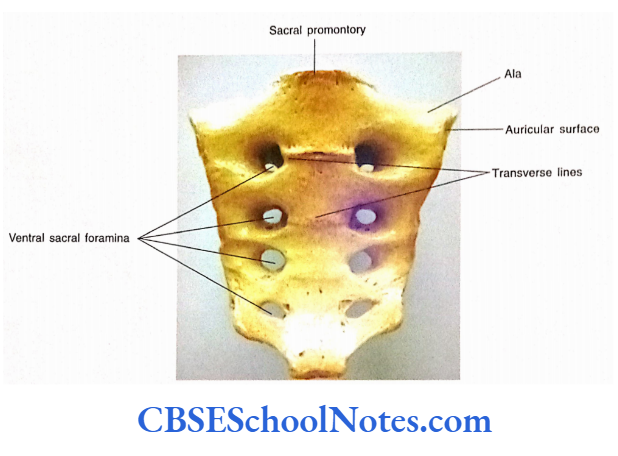
The body of the first sacral vertebra is large and much wider. Its anterior border is projecting and called the sacral promontory The lateral portion of the base (ala of the sacrum) is smooth and like a wing.
The ala of the sacrum is strong as it has to transmit the load from the lumbosacral joint to the sacroiliac joint.
Pelvic (Anterior) Surface
This surface is smooth, concave, and faces downwards and forwards. This surface presents four transverse lines indicating the site of fusion of 5 sacral vertebrae.
At the ends of these transverse lines, there are four pairs of sacral foramina on this surface. These foramina communicate with the sacral canal through intervertebral foramina.
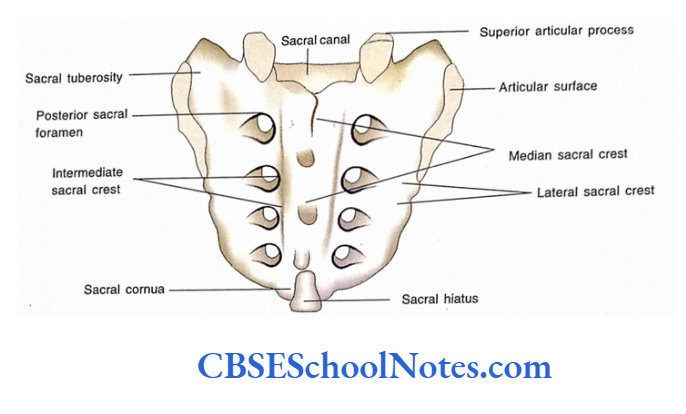
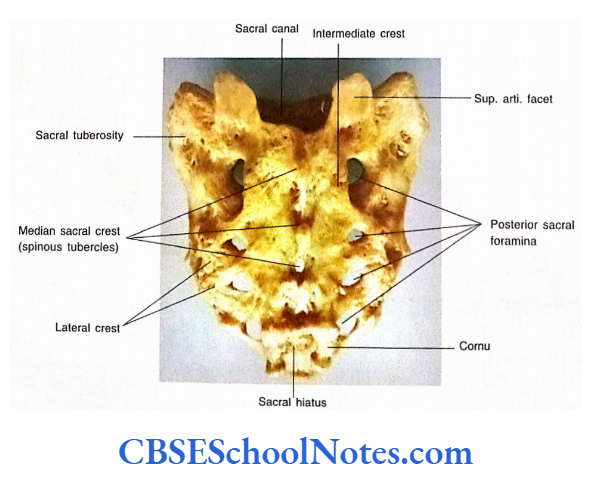
Posterior (Dorsal) Surface
The dorsal surface of the sacrum is rough and convex.
- In the midline, there is the presence of a longitudinal ridge called as median sacral crest, which is formed by the fused spinous processes of the upper four sacral vertebrae The dorsal surface presents four pairs of dorsal sacral foramina, which communicate with the sacral canal and transmit dorsal rami of upper four sacral spinous nerves.
- An area between the right and left foramina is formed by the fusion of laminae of the upper four sacral vertebrae.
- The laminae Body of S1 of the fifth sacral vertebra (and sometimes the fourth also) fails to fuse in the midline and presents an inverted U or V-shaped gap called a sacral hiatus.
- On either side of the sacral hiatus are the sacral cornua, which represent the inferior articular processes of the fifth sacral vertebra.
- The sacral hiatus contains fatty connective tissue, filum-terminale, the S5 nerve and the coccygeal nerve. The sacral cornua can be easily palpated in a living person and are useful guide to locate the hiatus for the injection of anesthetic agents.
- On the medial side of dorsal sacral foramina is a vertical crest consisting of four small tubercles. These tubercles represent the fused articular processes of fused sacral vertebrae. This crest is called intermediate crest.
- On the lateral side of the dorsal sacral foramina there is the presence of lateral sacral crest. This crest is formed by the fusion of transverse processes.
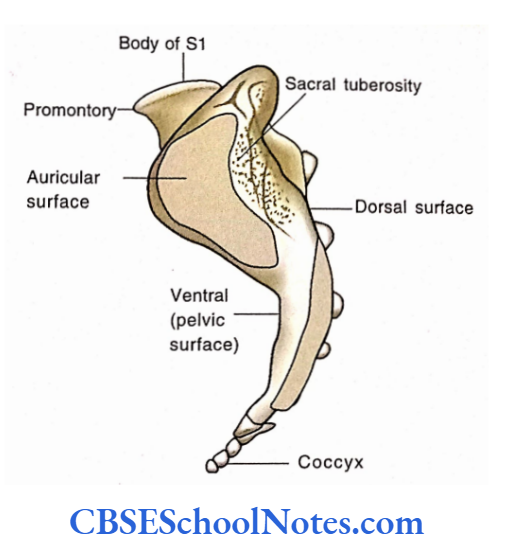
Lateral Surface of the Sacrum
On both the lateral surfaces of the sacrum, there is the presence of a large ear-shaped auricular surface that articulates with the ilium of each hip bone to form a sacroiliac joint.
Posterior to the auricular surface is a rough area, the sacral tuberosity for attachment of strong interosseous sacroiliac ligament.
Apex of the Sacrum
It has an oval facet for articulation with the coccyx.
The Coccyx
It is a small triangular bone formed by the fusion of four rudimentary vertebrae. It has an upper end (base), lower end, and pelvic and dorsal surfaces.
The base is formed by the first coccygeal vertebra, which has an oval facet for articulation with the apex of the sacrum.
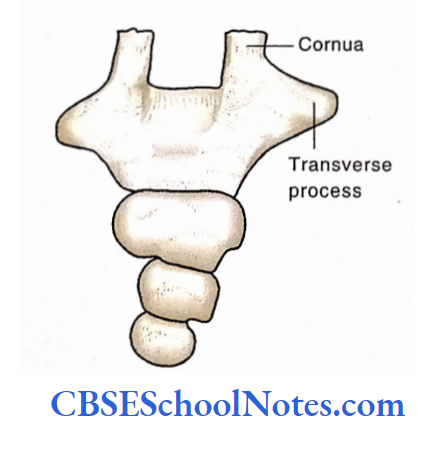
- The first coccygeal vertebra also has transverse processes and cornua.
- The cornua project upwards from the base of the coccyx and are connected with the cornua of the sacrum through ligaments.
- The remaining coccygeal vertebrae are featureless and represented by the nodules of bone.
Particular Features of the Sacrum and Coccyx
Attachments of the Muscles on the Sacrum and Coccyx
- lilacs and piriformis muscles are attached on the pelvic surface of the sacrum.
- The coccygeus muscle is inserted on the pelvic surface of the 5th sacral vertebra and coccyx.
- The levator ani is inserted on the tip of the coccyx.
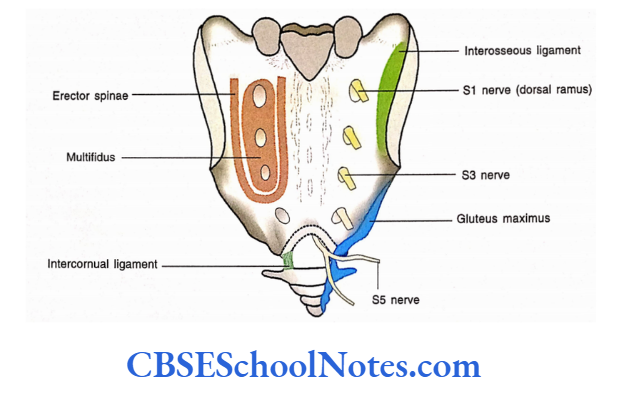
- Note the origin of gluteus maximus from the sacrum and coccyx from their dorsal surfaces.
- The dorsal surface also gives origin to the erector spinae and multifidus.
Attachment of Ligaments
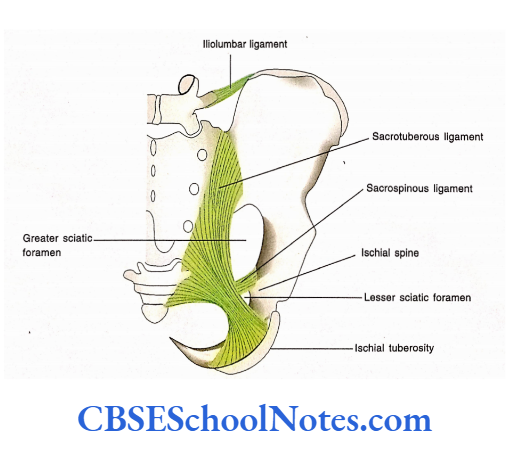
- The sacrotuberous ligament is attached to the lower part of the dorsal surface of the sacrum.
- The lateral margin of the lower part of the sacrum and the lateral margin of the coccyx gives attachment to the sacrospinous ligament.
- The interosseous ligament of the sacrospin¬ ous joint is attached to the rough area on the lateral surface posterior to the auricular surface.
- The iliolumbar ligament is attached to the lateral margin of the ala and iliac crest.
- Nerves and Blood Vessels about the Pelvic and Dorsal Surface of the Sacrum
- The median sacral artery is related to the midline.
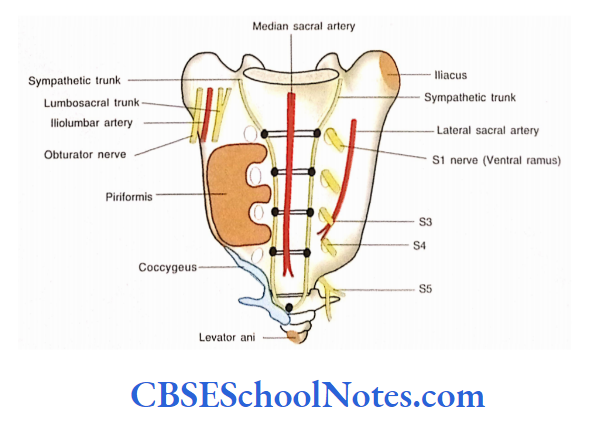
- The lateral sacral artery is related lateral to the ventral sacral foramina.
- The right and left sympathetic trunks are related medial to the ventral sacral foramina.
- The superior rectal artery is related to the left side of the midline.
- The dorsal and ventral sacral foramina give passage to the dorsal and ventral spinal rami respectively.
- The sacral canal contains the cauda equina.
- The subdural and subarachnoid spaces end at the middle of the sacrum.
- Each ala of the sacrum is related to the following structures medial to the lateral-sympathetic trunk, lumbosacral trunk, iliolumbar artery, and obturator nerve.
Clinical Importance
Caudal Epidural Anesthesia
As the subdural and subarachnoid spaces end at the level of the middle of the sacrum, the sacral canal contains extradural or epidural space filled with fibro-fatty tissue. In this space, there are spinal nerves of cauda equina covered by dura.
In epidural anesthesia (caudal analgesia) a local anesthetic agent is injected in the sacral canal through the sacral hiatus. The sacral hiatus is located by palpating the sacral cornua and lower end of the median sacral crest.
The anesthetic agent when injected in the sacral hiatus acts on the spinal nerves in the cauda equina (usually S2 to coccygeal nerves).
This procedure is usually used to relax the perineal musculature for painless childbirth.
Abnormal Fusion of Lumbar and Sacral Vertebrae Sometimes (in about 5% of people) L5 vertebra is partly or completely fused with the sacrum.
The condition is called sacralization of the L5 vertebra. In some cases, the S1 vertebra is separated from the sacrum and may be partly or completely separated from the sacrum.
This condition is called lumbarization of the S1 vertebra. Both the above conditions may produce painful symptoms in persons having abnormal fusion of the vertebra.
Bony Pelvis
The bones of the pelvic region consist of two hip bones (right and left), a sacrum, and a coccyx. The right and left hip bones are joined anteriorly at the pubic symphysis and to the sacrum and coccyx posteriorly to form a pelvic girdle or bony pelvis.
Above it articulates with the lumbar part of the vertebral column at the lumbosacral joint. Below it is attached to the lower limbs (femora) at hip joints.
Functions of the Bony Pelvis
- The bony pelvis is the basin-shaped ring of bones, which protects the distal part of the intestine, urinary bladder, and internal genital organs.
- The main function of the bony pelvis is to transmit the weight of the upper body from the vertebral column to the lower limbs.
- It transmits the thrust between the vertebral column and lower limbs.
- Provides attachment to the powerful muscles.
- It gives passage to the fetus at the time of birth.
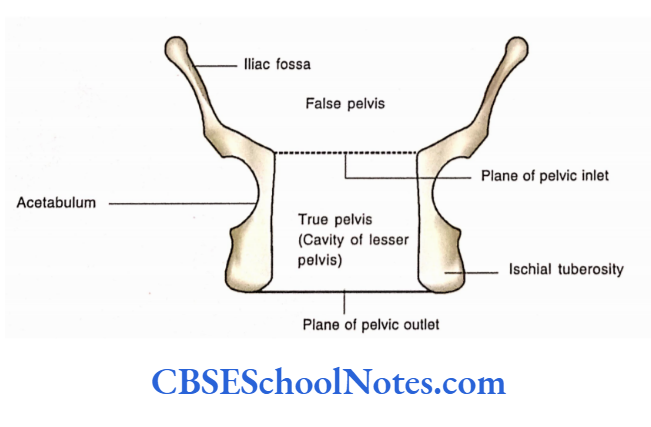
The bony pelvis is divided into greater and lesser pelvis. The greater pelvis is also called a false pelvis.
The lesser pelvis is called as true pelvis. The greater and lesser pelves are separated from each other by an imaginary plane, i.e., the plane of the pelvic inlet or pelvic brim).
Greater Pelvis
The walls of the greater or false pelvis are formed by the iliac fossa of the hip bones and posteriorly by the ala of the sacrum. Anteriorly, the greater pelvis presents no bony wall.
Lesser Pelvis
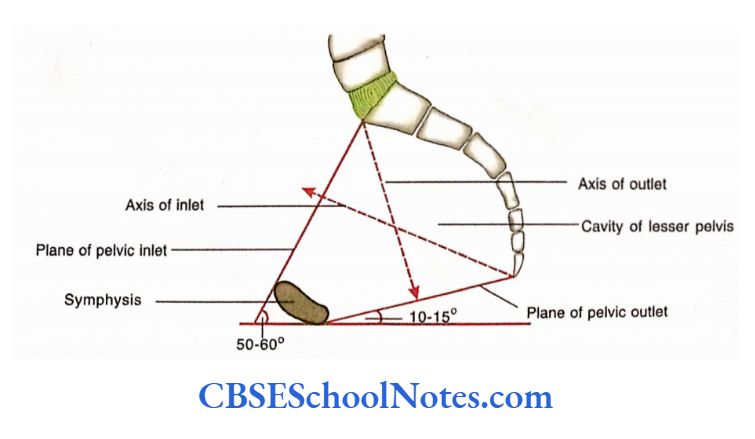
The lesser or true pelvis presents an inlet (superior pelvic aperture), a pelvic cavity, and an outlet (inferior pelvic aperture). The Pelvic Inlet The plane of the pelvic inlet slopes obliquely downwards and forward.
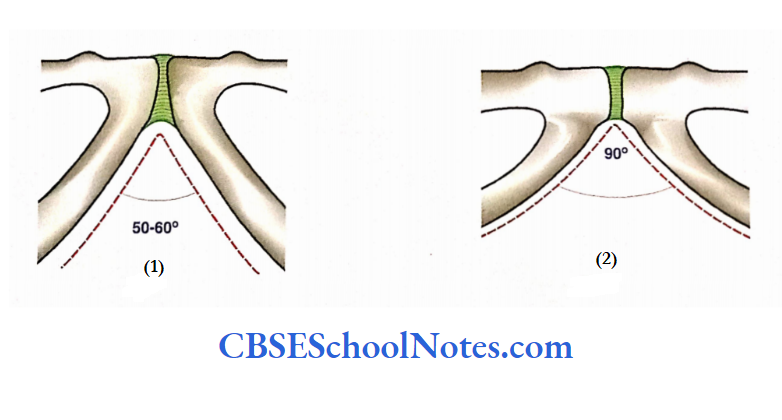
The axis of the inlet is determined by a line drawn perpendicular through the center of the plane. The plane of the pelvic inlet makes an angle of 50 to 60 with the horizontal plane.
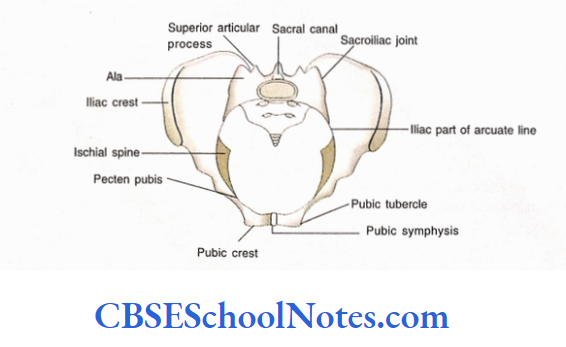
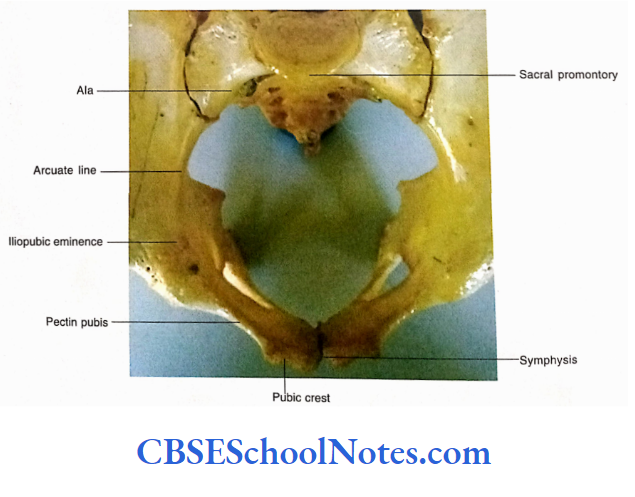
The boundary of the pelvic inlet on each side is formed behind by the sacral promontory, the anterior margin of the ala of the sacrum, the linea terminalis, and the upper end of the symphysis pubis.
(The linea terminalis of each hip bone consists of an arcuate line of ilium iliopubic eminence, pectin pubis, and pubic crest).
The Cavity of the Lesser Pelvis
The cavity of the lesser pelvis extends downwards and backward from the pelvic inlet and lies between the inlet and outlet. Anteriorly, the cavity is bounded by the symphysis, the body of the pubis, and two rami of the pubis.
On each side, the wall is formed by ilium and ischium below the arcuate line. Posteriorly it is limited by the concave pelvic surface of the sacrum and coccyx. The posterior wall of the cavity is much longer than the anterior wall.
The Outer or Inferior Pelvic Aperture (Pelvic Outlet)
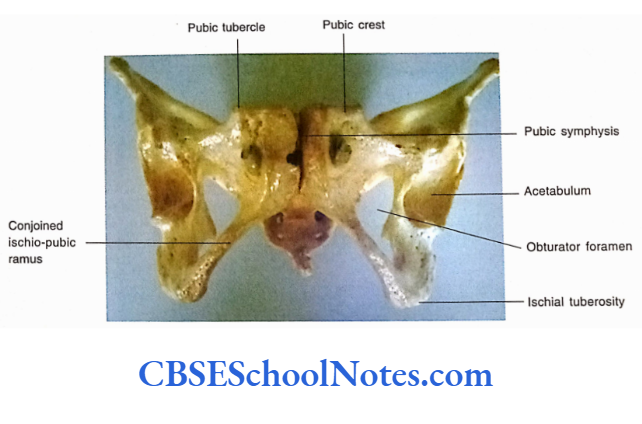
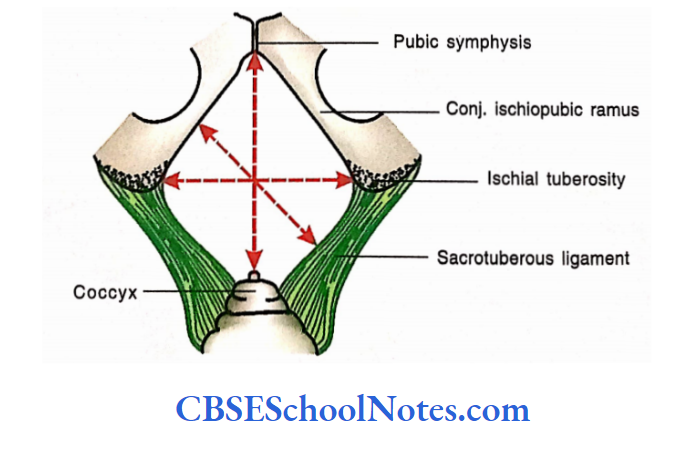
It is bounded anteriorly by the lower margin of the symphysis pubis, anterolaterally by the conjoined ischiopubic rami, laterally by the ischial tuberosities, posterolaterally by sacrotuberous ligaments, and posteriorly by the tip of the coccyx.
Thus the lower pelvic aperture is somewhat diamond-shaped. The plane of the pelvic outlet lies between the lower border of the symphysis pubis and the tip of the coccyx.
A line drawn perpendicular to the center of this plane is known axis of the pelvic outlet. The plane of the pelvic outlet makes an angle of 10 to 15 with the horizontal plane.
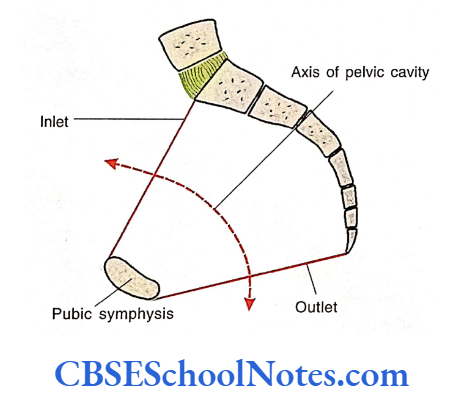
The Axis of Pelvic Cavity
The axis of the pelvic cavity is an imaginary axis passing through the pelvic cavity between the inlet and outlet of the pelvic cavity the axis is concave anteriorly and passes parallel to the sacrococcygeal curve.
The axis of the pelvic cavity is important because this axis passes the head of the fetus during childbirth. Hence, the axis of the pelvic cavity is also called as axis of the birth canal.
Diameters of the Pelvi
The diameter of the pelvic inlet and outlet are important in females due to childbearing
Measurements of the Inlet in Adult Females
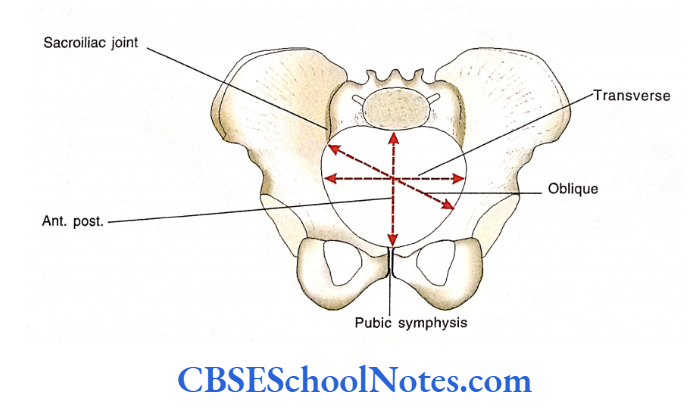
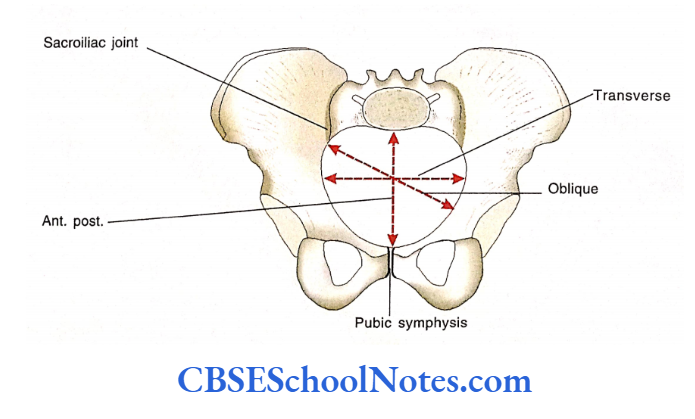
Anteroposterior diameter: It extends between the middle of the sacral promontory to the upper margin of the symphysis pubis. It measures about 105 to 110 mm.
The transverse diameter: Is the widest measurement across the inlet. It measures about 125 to 130 mm.
The oblique diameter: It is measured from the sacroiliac joint of one side to the iliopubic eminence of the other side. It measures about 120 to 125 mm.
Measurements of the Outlets in Adult Females The anteroposterior diameter: Is measured from the lower border of the symphysis pubis to the tip of the coccyx. It is about 125 mm.
The transverse diameter: It is the distance between two ischial tuberosities. It measures about 110 to 118 mm. The oblique diameter: It is the distance between the junction of the ischiopubic ramus of one side and the midpoint of the sacrotuberous ligament of the opposite side.
Anatomical Position of the Pelvis
Hold the articulated pelvis in such a way that the upper end of the pubic symphysis and the anterior superior iliac spines lie in the same vertical plane (place these points against a wall)
In this position, the tip of the coccyx lies almost at the level of the upper margin of the symphysis pubis.
The pelvic inlet faces forward and upwards and the pelvic outlet faces downwards and backwards.
In this position sacrum faces downwards and forwards.
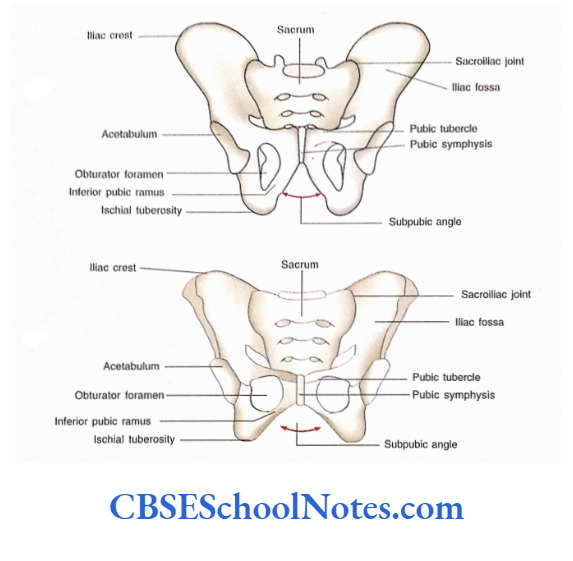
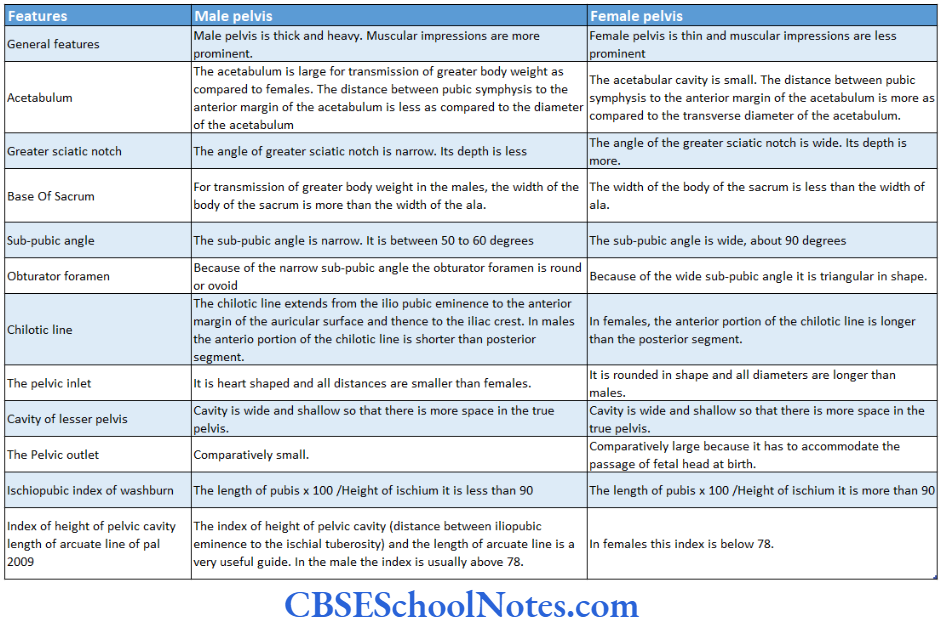
Differences Between Male and Female Pelves
The pelves of males and females differ significantly. These differences are due to childbearing function in females. For identification of sex from human skeletal remains, the pelvis or even a single hip bone is the most useful because here the sexual differences are clearly defined.