
Basic Mechanism Involved In The Process Of Inflammation And Repair
Inflammation: Inflammation is the complex biological response of vascular tissues to harmful stimuli, such as pathogens, damaged cells, or irritants. Avascular tissues such as cornea, articular cartilage, intervertebral disc, etc. do not show inflammatory response.
- The inflammatory response is a protective attempt by the organism to remove the injurious stimuli as well as initiate the healing process. Inflammation is not a synonym for infection. Even in cases where inflammation is caused by infection, the two are not synonymous: Infection is caused by an exogenous pathogen, while inflammation is the response of the organism to the pathogen.
- Inflammation can be classified as either acute or chronic. Acute inflammation is the initial response of the body to harmful stimuli and is achieved by the increased movement of plasma and leukocytes (initially neutrophils) from the blood into the injured tissues.
- A cascade of biochemical events propagates and matures the inflammatory response, involving the local vascular system, the immune system, and various cells within the injured tissue. It comes to an end within a few hours or days.
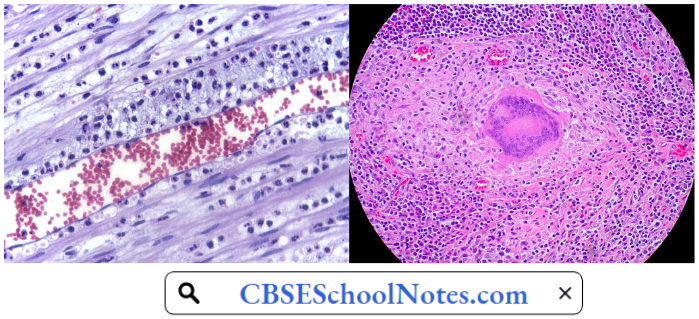
- Prolonged inflammation persisting for weeks or months is known as chronic inflammation. Whereas, neutrophil accumulation in the lesion is a hallmark of acute inflammation, chronic inflammatory lesion is characterized by the presence of lymphocytes, monocytes, macrophages, and plasma cells.
Read and Learn More Pathophysiology
Another hallmark of chronic inflammation is the simultaneous processes of tissue destruction and healing resulting in the formation of scar tissue. Inflammation may result from two sets of causes: Exogenous and endogenous:
- Inflammation Exogenous Factors
- Mechanical injury (traumatic injury),
- Physical injury (extremely low or high temperature, ionizing irradiation, microwaves)
- Chemical injury (caustic agents, poisons, venoms, etc.)
- Biological injury (viruses, microorganisms, protozoan and metazoan parasites).
- Ischaemic injury
- Inflammation Endogenous Factors
- The immunopathological responses such as allergic inflammations and autoimmune inflammatory disorders
- Endogenous products of tissue metabolism such as gout.
Acute Inflammation
Acute Inflammation Cardinal Signs: Acute inflammation is a short-term process/ usually appearing in a few minutes or hours and ceasing once the injurious stimulus has been removed. It is characterized by five cardinal signs
- Redness
- Warmth
- Swelling
- Pain
- Loss of function
The first four (classical signs) were described by Celsus about 2000 years ago, while loss of function was added to the list later by Virchow in 1870.
- Redness and warmth are due to increased blood flow at body core temperature to the areas such as skin, which normally are at a lower temperature; swelling is caused by the accumulation of fluid and plasma proteins in the extravascular spaces; pain is due to the release of chemicals that stimulate pain nerve endings or sensitize them to other stimuli.
- Loss of function has multiple causes, chiefly pain, and local edema.
- These five signs appear when acute inflammation occurs on the body’s surface. In the case of acute inflammation of internal organs, all five signs may not be apparent.
Acute Inflammatory Response: The acute inflammatory response may be discussed under two headings:
- The vascular response and
- The cellular response.
1. The Vascular Response: Alterations in the microvasculature (arterioles, capillaries, and venules) of the injured tissue are the earliest response to the injury. It consists of hemodynamic changes and changes in vascular permeability.
- Hemodynamic Changes: Transient vasoconstriction of the arterioles and reduced blood flow is the immediate response irrespective of the type of injury. It usually lasts only a few seconds but may be prolonged up to five minutes if the injury is very severe. It is followed by:
- Persistent and progressive vasodilatation begins in the arterioles and spreads to the capillaries and venules as well. This change becomes prominent within an hour of injury. Vasodilatation results in increased blood flow to the microvasculature and accounts for tire clinical signs of redness and warmth.
- Vasodilatation is brought about by the release of vasodilator mediators by the injured tissue cells as well as by the blood cells attracted by the injury.
- Transudation of fluid into the extracellular space (edema) is another consequence of vasodilatation. Starling forces, chiefly capillary hydrostatic pressure and plasma protein oncotic pressure govern the tissue fluid exchange across the capillary wall.
- It involves tissue fluid formation at the proximal segment of the capillary followed by reabsorption in the distal segment. Vasodilatation, by increasing the capillary hydrostatic pressure shifts the balance of the Starling forces in favor of greater exudation and decreased reabsorption. Thus, local edema results.
- Stasis. Loss of fluid from the capillaries leads to increased viscosity of blood flowing through the capillaries, with resultant stasis due to the increase in the concentration of the cells within blood. Stasis allows leukocytes to marginate along die endothelium, a process critical to their recruitment into the tissues.
- Normal flowing blood prevents this, as the shearing force along the periphery of die vessels moves blood cells into the middle of the vessel. Nutritional supply to die issue may be so compromised that it may become ischemic, even necrotic.
- Persistent and progressive vasodilatation begins in the arterioles and spreads to the capillaries and venules as well. This change becomes prominent within an hour of injury. Vasodilatation results in increased blood flow to the microvasculature and accounts for tire clinical signs of redness and warmth.
- Increased Vascular Permeability: All the blood vessels are lined by a continuous layer of endothelial cells, which provide a passive diffusion barrier. It permits the free diffusion of water and solutes but restricts the movement of larger molecules such as plasma proteins and cellular components of blood.
- The endothelial cells are joined together by tight junctions. In inflammatory conditions, the excessive fluid transferred into extracellular space consists not only of usual water and solutes (called transudate) but also contains a high concentration of plasma proteins.
- Such a tiuid is called an exudate. The exudate is formed because of markedly increased vascular permeability. The causes of increased vascular permeability include the following
- Opening of endothelial inter-cellular tight junctions, particularly in the postcapillary venules due to contraction of endothelial cells. It is mediated by the release of histamine, bradykinin, and other chemical mediators of inflammation. This response begins immediately after injury and usually lasts for a short duration (15-30 minutes).
- Direct injury to endothelial cells results in necrosis and the appearance of physical gaps at the site of detached endothelial cells. This type of increased permeability lasts for hours or even days.
- Endothelial injury is also mediated by leukocytes. Margination followed by leukocyte adhesion may result in the activation of leukocytes. The activated leucocytes release proteolytic enzymes and toxic free radicals which cause endothelial injury and increased vascular leakiness.
- The capillaries, newly formed during the process of repair, are excessively leaky.
- The endothelial cells are joined together by tight junctions. In inflammatory conditions, the excessive fluid transferred into extracellular space consists not only of usual water and solutes (called transudate) but also contains a high concentration of plasma proteins.
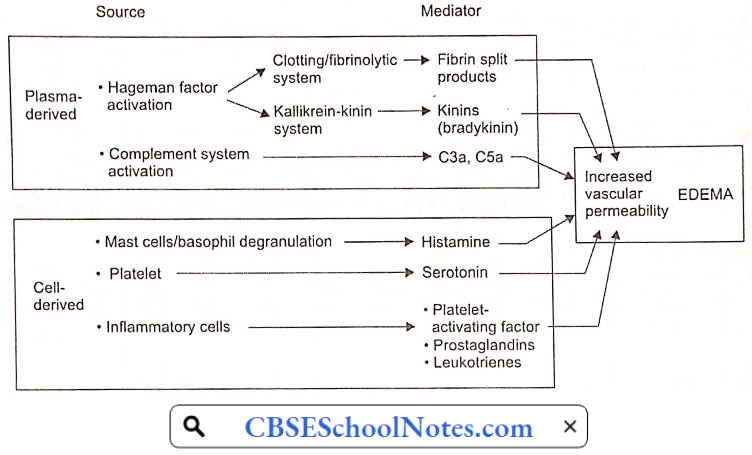
Mediators Of Increased Vascular Permeability: The primary source of vasoactive mediators of increased permeability during an inflammatory process is derived from injured tissue cells as well as plasma
2. The Cellular Response: Inflammatory response, which lasts more than a few hours, is characterized by the accumulation of white blood cells within the area of injury. In bacterial infections, physical or thermal injury, polymorphonuclear neutrophils are first to arrive (“first line of defense”).
Twenty-four to forty-eight hours later, a large number of macrophages can be seen in the inflamed area. In allergic inflammation, eosinophils and mast cells predominate. In viral infections, lymphocytes are the first to arrive.
Polymorphonuclear Neutrophils And Monocyte-Macrophages: The accumulation of neutrophils and monocyte macrophages at the site of inflammation is due to the presence of locally generated chemical mediators called chemotactic factors.
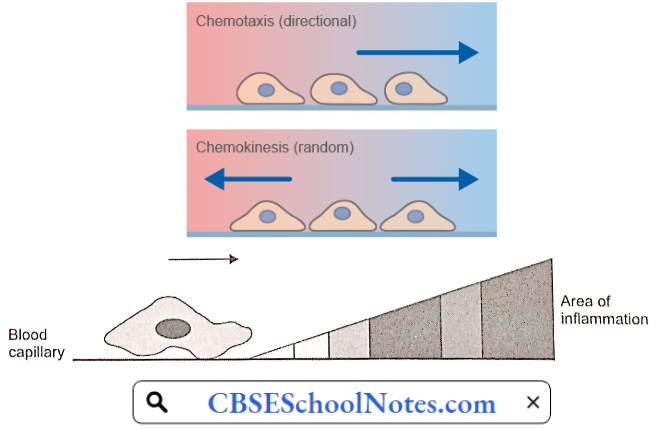
- Chemotaxis: The chemotactic-mediated transmigration of leukocytes involves the initial crossing of several barriers (endothelial basement membrane and matrix), followed by transport in the interstitial fluid to the inflamed area. The process is called chemotaxis.
- The chemical agents that act as potent chemotactic agents include leukotrienes, platelet factor, components of the complement system (C5a in particular), cytokines (IL-8 in particular), soluble bacterial products, monocyte chemo-attractant protein and eotaxin factor (for eosinophils).
- There is an increasing concentration gradient of chemotactic agents between an adjacent blood capillary the site of inflammation and leukocyte migration follows the gradient.
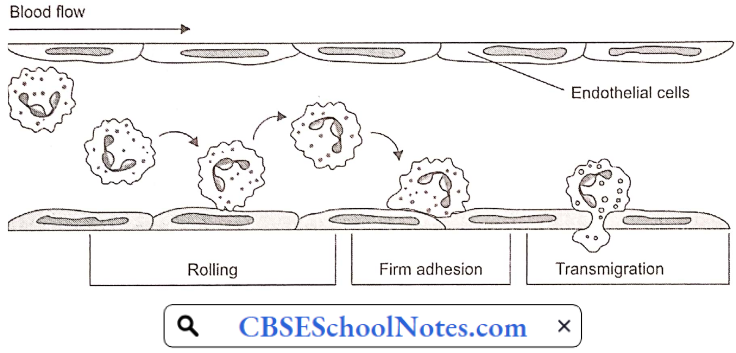
- Margination: This is the first step towards the transmigration of leukocytes out of the blood capillaries. Normal blood flow is characterized by an axial stream of red cells, leukocytes, and platelets and a peripheral cell—a free layer of plasma close to the vessel wall.
- Due to the slowing of blood flow and stasis, the central stream of cells widens and blood cells including leukocytes come closer to the vessel wall. This phenomenon is known as margination.
- Adhesion: Marginated leukocytes tend to stick briefly to the endothelial cells or roll over them. Injury leads to neutralization of the normal charge on the leukocytes and endothelial cells, resulting in a loose transient adhesion of leukocytes to the endothelial cells.
- Transmigration (Diapedesis): During chemotactic response, there is a characteristic change in the morphological orientation of the leukocyte (neutrophil or monocyte). It loses its classical rounded appearance and becomes wedge-shaped. At first, the leading edge passes into the space between two adjacent endothelial cells, damaging the basement membrane, and passes out of the vessel wall.
- By amoeboid movements, the rear part of the cell contains lysosomal granules, and lastly, the nucleus leaves the blood vessel.
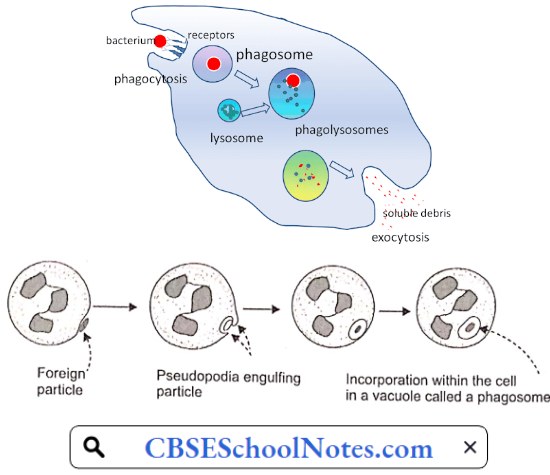
- Phagocytosis: Neutrophils and macrophages have an inherent capacity to recognize and engulf foreign particles. Coating of the bacteria by plasma proteins containing IgG and/or complement (opsonization) renders them more liable to phagocytosis.
- When a neutrophil or a macrophage becomes bound to a bacterium (or a foreign particle), there is a localized contraction of the cell under the point of contact, resulting in the formation of a cup-shaped invagination.
- Through the pseudopodia thrown out at the margins of the cups, the bacterium, enclosed in a vacuole, is internalized into the phagocyte and called a phagosome. Movement of the phagosome towards the granule-rich areas of the cytoplasm results in the fusion of the phagosome to an adjacent lysosome.
- Next, the lysosomal granules are discharged into the phagosome.
- This phenomenon is known as degranulation. The lysosomal membrane is incorporated into the vacuole membrane.
- The resulting structure is called a phagolysosome. Generally, the release of lysosomal granules is restricted to the phagolysosome.
- However, when the phagosome formation occurs in a granule-rich area or the phagocyte attempts to engulf too large a particle, lysosomal granules may be discharged into extracellular space causing damage to the host tissue cells in the vicinity.
- Bacterial Killing And Digestion: This is the ultimate objective of phagocytosis. Anti-microbial agents act by the following two mechanisms
- Oxygen-Dependent Bactericidal Mechanisms: Degranulation is accompanied by the activation of two enzymes present in the leukocyte granules, namely NADPH oxidase and myeloperoxidase.
- Activation of NADPH-oxidase is associated with a sharp increase in oxygen consumption in the leukocyte (the respiratory burst) leading to the generation of highly toxic superoxide (O–2) and hydrogen peroxide (H2O2). Myeloperoxidase catalyzes the formation of highly toxic hypochlorous acid (HCIO).
- Oxygen-Independent Bactericidal Mechanisms: Lysosomal granules contain a number of agents that do not require oxygen for their bactericidal activity. These agents include lysosomal hydrolases, permeability-increasing factors, defensins, lysozyme, and cationic protein.
- Oxygen-Dependent Bactericidal Mechanisms: Degranulation is accompanied by the activation of two enzymes present in the leukocyte granules, namely NADPH oxidase and myeloperoxidase.
Mast Cells/Basophils: Mast cells and basophils play a central role in inflammatory and immediate allergic reactions. They are able to release potent inflammatory mediators, such as histamine, proteases, chemotactic factors, cytokines, and metabolites of arachidonic acid that act on the blood capillaries, smooth muscle, connective tissue, mucous glands, and inflammatory cells.
Both mast cells and basophils contain special cytoplasmic granules which store mediators of inflammation. The extracellular release of the mediators from the mast cells (degranulation) may be induced by:
- Physical destruction, such as high temperature, mechanical trauma, ionizing irradiation, etc.;
- Chemical substances, such as toxins, venoms, proteases;
- Endogenous mediators, including tissue proteases, cationic proteins derived from eosinophils and neutrophils;
- Immune mechanisms which may be IgE-dependent or IgE-independent
The increase in the number of mast cells and basophils, and the enhanced secretion at sites of inflammation, can accelerate the elimination of the cause of tissue injury or, paradoxically, may lead to a chronic inflammatory response. Thus, manipulating mast cell and basophil adhesion may be an important strategy for controlling the outcome of allergic and inflammatory responses.
Eosinophils: Eosinophils is a leukocyte that resides predominantly in submucosal tissue and is recruited to sites of specific immune reactions, including allergic diseases. The large specific granules contain four distinct cationic proteins which exert a range of biological effects on host cells and microbial targets: Major basic protein (MBP), eosinophil cationic protein (ECP), eosinophil-derived neurotoxin (EDN), and eosinophil peroxidase (EPO).
- In addition, histaminase and a variety of hydrolytic lysosomal enzymes are also present in the large specific granules. These proteins have major effects not only on the potential role of eosinophils in host defense against helminthic parasites but also in contributing to tissue dysfunction and damage in eosinophil-related inflammatory and allergic diseases.
- Compared to neutrophils, eosinophils have limited phagocytic activity which is mainly aimed at killing multicellular parasites. Another possible beneficial function of eosinophils is the inactivation of mediators of anaphylaxis.
Systemic Effects Of Acute Inflammation: Fever is due to the release of interleukin 1 (a cytokine), prostaglandins, or tumor necrosis factor from the inflammatory tissues, either of which can disturb tire hypothalamic temperature regulating center. Fever may also be induced by certain constituents in the cell wall of dead bacteria called pyrogens.
- Leucocytosis is a feature of infections or even non-infectious inflammations. Typically, the total leukocyte count is between 15,000 and 20,000 IpL. Usually, in bacterial infections, leucocytosis is due to neutrophilia; in viral infections due to lymphocytosis; and in allergic conditions due to eosinophilia. Some infections, e.g. typhoid fever, however, are associated with leucopenia (neutropenia with relative lymphocytosis).
- Lymphangitis: lymphadenitis in the lymph vessels and lymph nodes draining the area of inflammation is commonly seen. These responses represent either a non-specific reaction to chemical mediators released by the inflamed tissues or an immunological response to foreign antigens.
- Acute phase proteins: Acute inflammation is commonly accompanied by increased concentrations of several plasma proteins such as C-reactive protein, alpha-2 macroglobulin, and fibrinogen (collectively called acute phase proteins).
- The precise function of these proteins in inflammation is largely unclear. However, when measured in the laboratory, they can serve as useful markers of inflammation.
- These proteins also increase the erythrocyte sedimentation rate (ESR), a nonspecific indicator of inflammation. Finally, prolonged or widespread inflammation can deplete complement leading to decreased levels of certain components of complement in the serum.
- Other symptoms such as decreased appetite, lactacidosis, negative nitrogen balance, and increased slow-wave sleep are commonly seen in acute infections. Most of these seem to be produced by interleukin 1.
- Shock may develop in severe acute inflammatory conditions. Tumor necrosis factor (TNF-α), a cytokine, is one of the mediators of acute inflammation. Bacteraemia/septicemia may result in the release of a massive amount of TNF-α leading to widespread vasodilatation and increased vascular permeability.
- These changes lead to intravascular volume loss, hypotension, and circulatory shock. Microthrombi may be formed throughout the body which may lead to disseminated intravascular coagulation (DIC), bleeding, and death.
Outcomes Of Acute Inflammation: The acute inflammatory response may have one of the following four outcomes depending on whether or not injury results in significant tissue loss or the inflammatory stimulus is rapidly removed:
- Resolution
- Healing,
- Suppuration, or
- Chronic inflammation.
- Resolution: Such an outcome follows the complete removal of the agent or microorganism that triggered the inflammatory response. The process includes the removal of any injured (necrotic) host cells. This is the ideal outcome for acute inflammation. It is more likely if cellular damage has been minimal, for example, the resolution of lobar pneumonia.
- Healing May Involve Two Processes:
- Regeneration: The replacement of damaged or lost tissue by normal tissue of a similar type. It occurs only in tissues that contain cells capable of dividing (for example, epithelial tissues such as the epidermis of the skin).
- Repair: Scar formation, fibrosis. It involves the replacement of damaged or lost tissue by collagen fibers (scar tissue). This is the healing mechanism for those tissues that cannot regenerate (dermis, nerve, muscle, etc.).
- Suppuration And Abscess Formation: If there has been a large amount of cellular necrosis, or if there is a great deal of bacterial contamination, exudates and dead leukocytes (pus) can accumulate forming an abscess. In time, connective tissue walls of the abscess and limits its spread. Resolution and healing cannot take place until adequate drainage of the abscess has been provided.
- Chronic Inflammation: Normally, the acute inflammatory response to cellular injury has subsided by the time tissue healing begins. If tissue destruction is prolonged, inflammation and attempts at healing occur at the same time. This produces a picture of chronic inflammation.
Mechanism Of Final Resolution Of Acute Inflammation: Acute inflammation normally resolves by mechanisms that have remained somewhat elusive. Emerging evidence now suggests that an active, coordinated program of resolution is initiated in the first few hours after an inflammatory response begins. After entering tissues, granulocytes promote the switch of arachidonic acid—derived prostaglandins and leukotrienes to lipoxins, which initiate the termination sequence.
Neutrophil recruitment thus ceases and programmed death by apoptosis is engaged. Consequently, apoptotic neutrophils undergo phagocytosis by macrophages, leading to neutrophil clearance and release of anti-inflammatory and reparative cytokines such as transforming growth factor-β1. The anti-inflammatory program ends with the departure of macrophages through the lymphatics.
Allergic Inflammation: An allergic reaction is the result of an inappropriate immune response triggering inflammation. A common example is hay fever, which is caused by a hypersensitive response by skin mast cells to allergens.
Pre-sensitized mast cells respond by degranulation, releasing vasoactive chemicals such as histamine. These chemicals propagate an excessive inflammatory response characterized by blood vessel dilation, production of pro-inflammatory molecules, cytokine release, and recruitment of leukocytes. A severe inflammatory response may mature into a systemic response known as anaphylaxis.
Chronic Inflammation
Chronic inflammation occurs when the damaging stimulus persists and the process of continuing tissue necrosis, organization, and repair all occur concurrently. In addition to acute inflammation, the specific defenses of the immune system are activated around the area of damage, and tissues are infiltrated by activated lymphoid cells.
The Chronic Inflammatory Tissue Shows:
- Necrotic cell debris
- Acute inflammatory exudate
- Vascular and fibrous granulation tissue
- Lymphoid cells
- Macrophages
- Collagenous scar
Chronic inflammation may be caused by one of the following three mechanisms:
- Chronic Inflammation Following An Acute Inflammation: When tissue destruction is extensive or bacteria survive and persist at the site of inflammation, for example, osteomyelitis or pneumonia leading to a lung abscess.
- Recurrent Attacks Of Acute Inflammation: Repeated attacks of acute inflammation may culminate in chronicity of the disease process, for example, pyelonephritis resulting from recurrent attacks of urinary tract infection, or repeated attacks of acute cholecystitis culminating in chronic cholecystitis.
- Chronic Inflammation Starting De Novo: In such cases, the inflammatory agent produces a chronic inflammatory response to begin with.
General Features Of Chronic Inflammation: Ordinarily, agents that produce an acute inflammatory response are removed by the neutrophils and macrophages by phagocytosis and digestion. However, certain agents cannot be removed by an acute inflammatory response, for example, Mycobacterium tuberculosis, fungus, or a suture.
The mechanism of dealing with such indigestible agents is termed chronic or granulomatous inflammation. Chronic inflammation response primarily serves to contain the pathological process, as well as to remove the offending agent, if possible.
Though chronic inflammatory responses may somewhat differ in detail, depending on the offending agent, the following features are common to all chronic inflammations:
- Mononuclear Cell Infiltration
- Tissue Destruction And necrosis
- Proliferative Changes.
- Mononuclear Cell Infiltration
- Macrophages: The macrophages comprise the most important cells in chronic inflammation. These cells are recruited by chemotactic migration from the circulation as well as by local proliferation.
- Activated macrophages release several biologically active substances such as neutral and acid proteases, oxygen-derived reactive metabolites, and cytokines. These agents bring about tissue destruction, neo-vascularization, and fibrosis. Chronic inflammatory lesions usually show some other chronic inflammatory cells:
- Lymphocytes: These cells are a prominent feature of chronic inflammatory lesions. They perform vital functions both in cell-mediated and humoral immune responses. The T-lymphocytes function not only as cytotoxic killer cells but also regulate macrophage recruitment and activation through the secretion of lymphokines (cytokines) and modulate antibody production.
- Plasma Cells: These cells are also usually present in a chronic inflammatory lesion. Plasma cells are immune-activated B-lymphocytes rich in cytoplasmic reticulum. These cells are the primary source of antibodies specific to the antigen present at the site of chronic lesions.
- Macrophages: The macrophages comprise the most important cells in chronic inflammation. These cells are recruited by chemotactic migration from the circulation as well as by local proliferation.
- Tissue Destruction: It is one of the important features of most of the chronic inflammatory responses. As mentioned above, it is brought about by several biologically active substances released by activated macrophages.
- Proliferative Changes: As a result of necrosis, proliferation of small blood vessels is stimulated. Eventually, collagen is laid down and healing by fibrosis occurs.
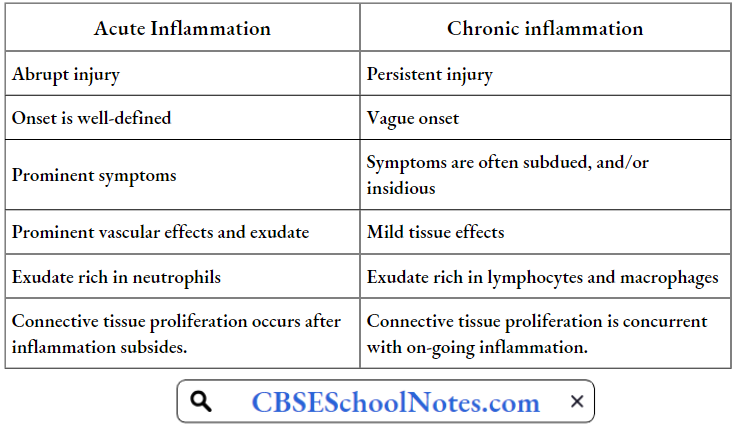
Summary Of Differences Between Acute And Chronic Inflammation
Basic Principles Of Wound Healing
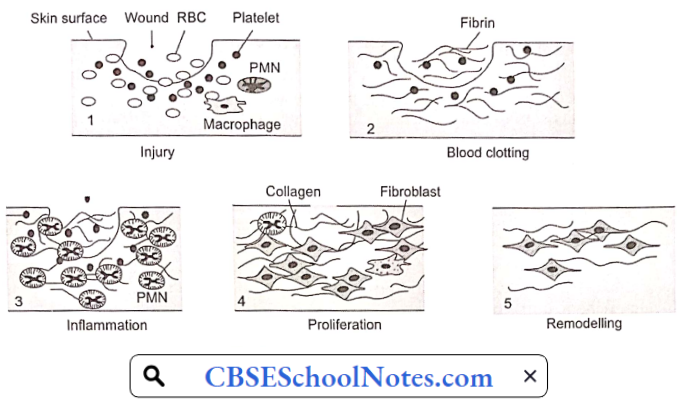
If there is an injury to the skin, under normal circumstances, the wound heals in a few days. The process of wound healing consists of four overlapping phases:
- Hemostasis Phase: Injury to the skin or other tissues results in bleeding. The first step in wound healing involves the stoppage of bleeding (hemostasis). Hemostasis starts when blood leaks out of the body. The circulating platelets collect at the site of injury, stick together, form a platelet plug, and seal the break in the wall of the blood vessel. This step is known as primary hemostasis.
- However, the platelet is soft and temporary. In the next step known as secondary hemostasis, the blood collected at the site of injury clots. Clotting of blood seals the leak in blood vessels permanently.
- The blood clot reinforces the platelet plug with threads of fibrin which are like a molecular binding agent. The hemostasis stage of wound healing happens within a few minutes.
- Inflammatory Phase: Inflammation is the second stage of wound healing and begins right after the injury when the injured blood vessels lose blood. Inflammation both controls bleeding and prevents infection. During the inflammatory phase, damaged cells are removed from the wound area. Swelling, heat, pain, and redness commonly seen during this stage of wound healing are signs of acute inflammation.
- If some bacteria get into the wound, blood macrophages remove the pathogens. Inflammation is a natural part of the wound healing process and is only problematic if prolonged or excessive if infection cannot be controlled.
- Proliferative Phase: The proliferative phase features three distinct stages:
- Filling the wound
- Contraction of the wound margins
- Covering the wound by epithelialization
- The gap in the skin is filled by newly built tissue consisting of collagen fibers and extracellular matrix. In addition, a new network of blood vessels grows into the wound bed forming shiny, deep red granulation tissue. When tissues are injured, fibroblasts around the injured region differentiate into myofibroblasts, a type of highly contractile cells that produce abundant extracellular matrix proteins.
- It has become clear that both fibroblasts and myofibroblasts play a critical role in the wound healing process. Fibroblast cells lay down collagen fibers. Myofibroblasts cause the wound to contract by gripping the wound edges and pulling them together.
- In healthy stages of wound healing, granulation tissue is pink or red and uneven in texture. Moreover, healthy granulation tissue does not bleed easily. Dark granulation tissue can be a sign of infection, ischemia, or poor perfusion. In the final phase of the proliferative stage of wound healing, epithelial cells resurface the injury. It is important to remember that epithelialization happens faster when wounds are kept moist and hydrated.
- Maturation Phase: When collagen is laid down during the proliferative phase, it is disorganized and the wound is thick. During the maturation phase, collagen is aligned along tension lines and water is reabsorbed so the collagen fibers can lie closer together and cross-link. Cross-linking of collagen reduces scar thickness and also makes the skin area of the wound stronger.
- When the wound fully closes, the cells that had been used to repair the wound but which are no longer needed are removed by apoptosis. Generally remodelling begins about 21 days after an injury and can continue for a year or more.
- The stages of wound healing are a complex and fragile process. Failure to progress in the stages of wound healing can lead to chronic wounds. Factors that lead to chronic wounds include venous disease, infection, diabetes, poor nutrition, old age, etc.
Scar: A scar is an area of fibrous tissue that replaces normal skin after an injury. Scars result from the biological process of wound repair in the skin, as well as in other organs and tissues of the body. Thus, scarring is a natural part of the healing process.

With the exception of very minor lesions, every wound (for example an accident, disease, or surgery) results in some degree of scarring.
- Hypertrophic Scars occur when the body overproduces collagen, which causes the scar to be raised above the surrounding skin. Hypertrophic scars take the form of a red raised lump on the skin. They usually occur within 4 to 8 weeks following wound infection or wound closure with excess tension and/or other traumatic skin injuries.
- Keloid Scars are a more serious form of excessive scarring because they can grow indefinitely into large, itchy tumorous masses. Keloids differ from normal mature scars in type of collagen and size. Some people are prone to keloid formation and may develop them in several places.
- Atrophic Scars take the form of a sunken recess in the skin, which has a pitted appearance. These are caused when underlying structures supporting the skin, such as fat or muscle, are lost. This type of scarring is often associated with acne or chickenpox.