
Lymphatic System
The lymphatic system is also sometimes called as immune system. (Readers are advised to refer to the functions of the immune system from a textbook of physiology.)
Lymphatic System system consists of the following structures:
- Lymphatic vessels: The thin-walled vessels collect the tissue fluid (lymph) and drain it into veins.
- Specific lymphatic organs: These are made up of accumulation of lymphatic tissue and are surrounded by capsule, e.g., lymph node, spleen and thymus
- Lymphatic tissue found within the tissues of other organs: Examples of this are lymphatic tissue found within the bone marrow, GI tract (tonsils, Peyer’s patches, appendix), urinary tract, respiratory tract, etc. These lymphatic tissues are not surrounded by a capsule
Question 1. What is lymph?
Answer:
The tissue fluid drained by lymphatic vessels is called as lymph. It consists of tissue fluid, large molecules of proteins, fat droplets and particulate matters
Question 2. What is lymphatic tissue?
Answer:
It is a specialized form of connective tissue. The supporting framework of lymphatic tissue is a meshwork formed by reticular cells and reticular fibres. The spaces within the meshwork are occupied by a large number of lymphocytes. The other cells present in lymphatic tissue are plasma cells and macrophages. (In the thymus, the supporting framework is not formed by reticular cells and fibres, but by star-shaped epithelial cells called as epithelioreticular cells
Question 3. What are the General Functions of the Lymphatic Tissue?
Answer:
Defence of body. This is achieved by lymphocytes and macrophages, which protect the body from foreign cells (bacteria, viruses and cancer cells). Lymphocytes are capable of identifying foreign entities (antigens) at the molecular level and responding to them immuno-logically. Phagocytosis of foreign cells such as bacteria, viruses and cancer cells by macrophages. Lymphatic tissues are also involved in the production of lymphocytes and plasma cells.
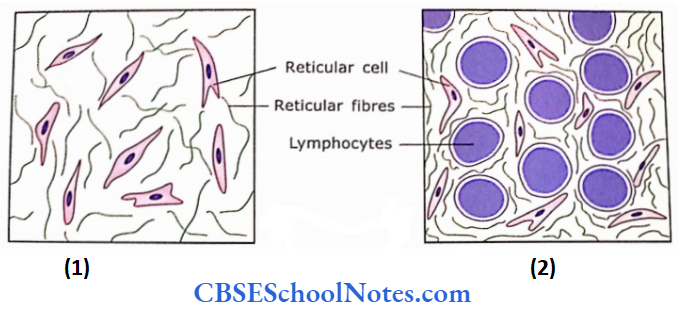
Question 4. What are diffuse lymphatic tissue and lymphatic nodules?
Answer:
The accumulation of lymphatic tissue is seen in the mucous membrane of the gastrointestinal, respiratory, urinary and reproductive tracts. Here, lymphocytes are disposed of randomly beneath the epithelium. This kind of lymphatic tissue is called diffuse lymphatic tissue. These kinds of lymphatic tissues are also known as mucosa-associated lymphatic tissue (MALT). These collections of lymphatic tissues are located in areas where they come in direct contact with antigens and may initiate the immune response
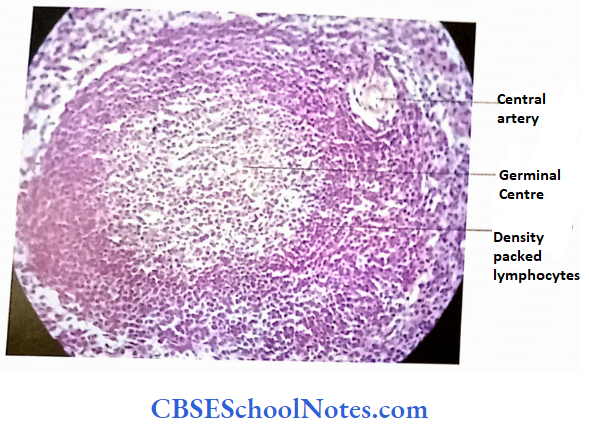
A lymphatic nodule is a circumscribed concentration of lymphatic tissue (lymphocytes and related cells) that is not surrounded by a capsule ). The lymphatic nodules are found both in scattered lymphoid tissue infiltration ofthe connective tissues (as in lamina proper of appendix, tonsil, etc) as well as in the encapsulated lymphoid organs such as spleen and lymph nodes.
The lymphatic nodule may show a lighter stained area in the centre (germinal centre) surrounded by a darkly stained zone of densely packed small lymphocytes. The lighter staining of the germinal centre is because it contains large euchromatic lymphoblasts and plasmoblasts, which are involved in the production of lymphocytes and plasma cells. In a lymphatic nodule, the germinal centre develops only when a nodule is exposed to an antigen (for example, Infection, or foreign cells).
Lymphocytes Remember:
Lymphatic nodules are a circumscribed collection of lymphocytes within the meshwork of reticular cells. This kind of collection of lymphatic tissue is seen In the mucous membrane of gastrointestinal, respiratory, urinary and reproductive tracts
The Lymphatic System Acts as the Immune System:
It should be noted that various lymphatic organs and lymphatic tissues constitute the immune system. The cells of the immune system consist of lymphocytes and various supporting cells.
Classification of Lymphocytes:
Three different functional types of lymphocytes are found in the body, i.e., B lymphocytes, T lymphocytes and natural killer(NK) lymphocytes
- T Lymphocytes (T cells)
- These lymphocytes although originate in the bone marrow, get differentiated in the thymus gland, hence called as T lymphocytes
- T lymphocytes constitute about 60-80% of total blood lymphocytes.
- Three different types of lymphocytes are known, i.e., helper T, cytotoxic T and memory T cells
- The T lymphocytes are involved in cell-mediated immunity in which, cytotoxic T lymphocytes bind to the surface of parasites and virally infected cells and kill them
- B Lymphocytes (B Cells)
- These cells originate and mature in the bone marrow.
- B lymphocytes constitute about 20-30% of total circulating lymphocytes.
- They are responsible for the production of various antibodies.
- B lymphocytes are of two types, i.e., plasma cells (which produce antibodies) and B memory cells.
- B lymphocytes are responsible for humoral immune response in which B lymphocyte produces antibodies, which combine with antigens to form antigen-antibody complexes.
- These are removed by macrophages and neutrophils
- B cells also express major histocompatibility complex 2 (MHCH) on their surface.
- NK Cells
- These cells also originate in the bone marrow.
- They are genetically programmed to recognize those cells, which are viral Infected or tumour cells. Alter recogni¬ tion they kills these cells.
- NK cells constitute about 5- 10% of circulating lymphocytes
Question 5. How different types of lymphocytes are identified
Answer:
Various types of lymphocytes are similar in appearance, hence, cannot lie differentiated morphologically even under an electron microscope. However, both B and T lymphocytes are distinguished by immunocytochemical methods.
Different types of lymphocytes possess different types of unique molecules on the surface of their cell membrane. These molecules arc culled cluster ol’dilTcrenliation (CD) molecules. These CD molecules can be visualized by immuno-histochemical methods using monoclonal antibodies. This method has helped to identify various subtypes of lymphocytes. These CD markers are designated as numbers according to an international system
T cells express CD2, CD3, CD4, CD7 and CD8 markers. T cells expressing CD4 markers are called helper T cells. While T cells expressing CD8 markers are also known as cytotoxic T lymphocytes. B cells express CD9, CD19 CD20 and CD24 markers. Similarly, CD markers for NK cells are CD16, CD56 and CD94.
Supporting Cells of the Immune System:
The supporting cells of the immune system consist of reticular cells, macrophages, follicular dendritic cells, Langerhans cells and epithelioreticular cells
Lymphocytes Clinical Application
Acquired Immunodeficiency Syndrome (AIDS) The disease is caused due to infection of the human Immunodeficiency virus (HIV). The infection destroys the defence system (immune system) of the body. The virus binds to CD4 molecules of T helper lymphocytes and destroys their capability to fight infection, not only with HIV but also infections due to other viruses and bacteria.
The HIV multiply rapidly within the T lymphocytes and infects other lymphocytes so that their number is reduced significantly. As a result, the infected person ultimately becomes incapable of fighting against any bacteria or virus. Death usually occurs due to secondary infections.
Lymphatic Vessels
In addition to the blood vascular system, there exists a lymphatic system to assist in draining tissue fluid to the blood circulation. The lymphatic system consists of lymph vessels and lymph nodes. The tissue fluid leaves the blood capillaries at its arteriolar end and re-enters at its venule end The excess of tissue fluid, containing particulate matter colloidal material, is absorbed through lymphatic capillaries because these capillaries are more permeable than blood capillaries
Lymphatic vessels begin as a network of blind capillaries in the tissues of the body. The lymphatic capillaries unite to form progressively larger lymph vessels. The largest of these vessels are known as the thoracic duct and right lymphatic duct.
These vessels pour their lymph into venous blood at the root ofthe neck. While the lymph is travelling through lymphatic vessels, it passes through lymph nodes where it gets filtered. The foreign substances (antigens) being conveyed by the lymph are exposed to lymphocytes of lymph nodes, which ultimately leads to an immune response
Histology of Lymph Vessels
1. Lymph Capillaries:
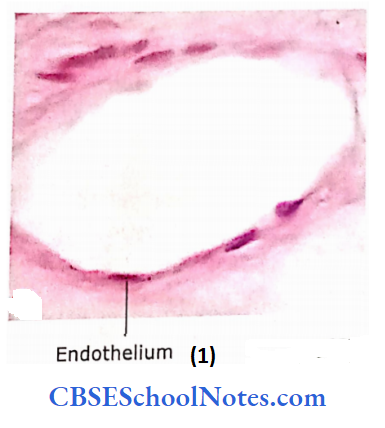
The lymphatic capillary networks accompany the networks of blood capillaries. The histological structure of lymph capillaries is similar to blood capillaries. However, lymph capillaries are more dilated and irregular in cross-section compared to blood capillaries and lack a continuous basal lamina
Lymph Capillaries Remember:
In the lymph capillaries, endothelial cells overlap and act as a one-way valve, which permits only the passage of tissue fluid into lymphatic capillaries but prevents its escape.
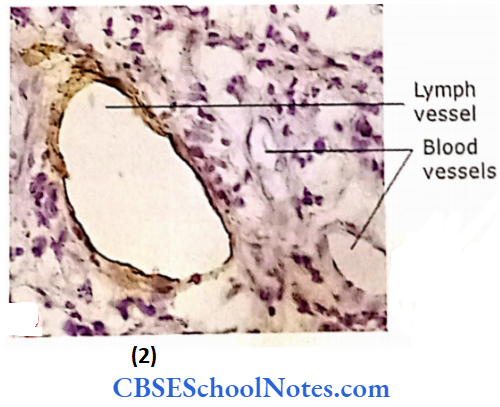
2. Small size Lymph Vessels
Their histological structure is almost similar to lymph capillaries. but they are more dilated than capillaries A lymph vessel can be differentiated from a blood vessel by staining it with an immuno-histochemical method (using D2-40 as a marker). This stains only lymphatic endothelial lining
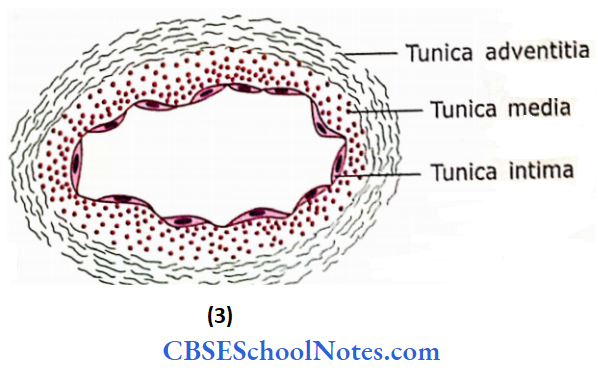
3. Medium Size Lymph Vessels
These vessels consist of three layers. In tunica intima. the endothelial cells rest on the basal lamina. In subendothelia! layer, connective tissue fibres are arranged longitudinally. In tunica media, the connective tissue and muscle fibres are circularly disposed. The tunica externa of lymph vessels is similar to that of veins.
4. Large Size Lymph Vessels:
Although the histological structure of large size lymph vessels resembles that of comparable size veins, it differs in two characteristics: the muscle tissue is more abundant than in veins and their tunicae are more difficult to distinguish. In the thoracic duct, muscle is arranged longitudinally
Lymphatic Organs
Lymphatic organs are made up of an accumulation of lymphatic tissue and are surrounded by capsules, i.e.,
- Lymph nodes
- Spleen and
- Thymus
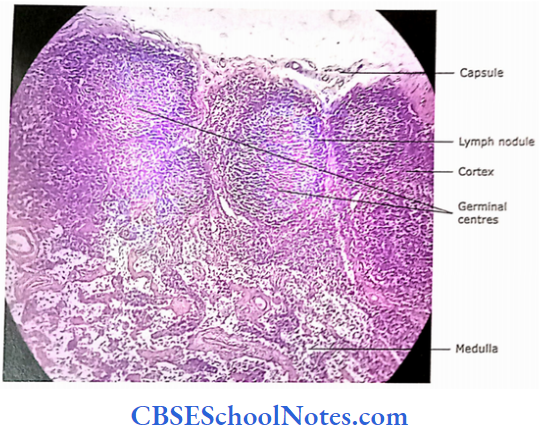
1. Lymph nodes
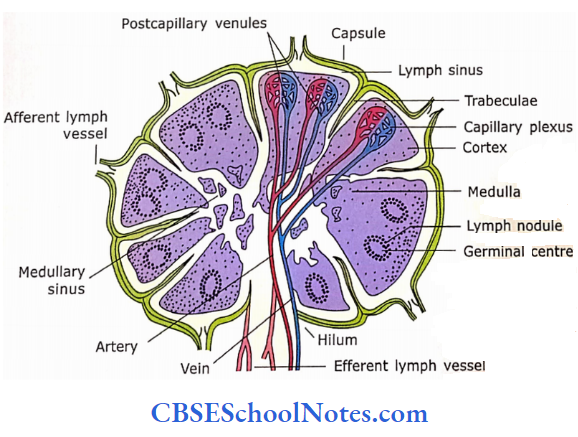
Lymph nodes are kidney-shaped structures measuring from a millimetre to one or two centimetres. Lymph nodes serve as filter of lymph and hence are placed in the pathway of lymphatic vessels. Several afferent lymphatic vessels enter the lymph node at its convex surface and a single lymph vessel leaves through the hilus as an efferent lymphatic vessel
The hilus also serves for the entry and exit of blood vessels and nerves A section through the lymph node shows an outer darkly stained zone cortex and an inner medulla. The dark staining is due to densely packed lymphocytes in the cortex while the medulla is lightly stained because it contains fewer lymphocytes. The cortex has several lymph nodules, which may show a germinal centre (see above).
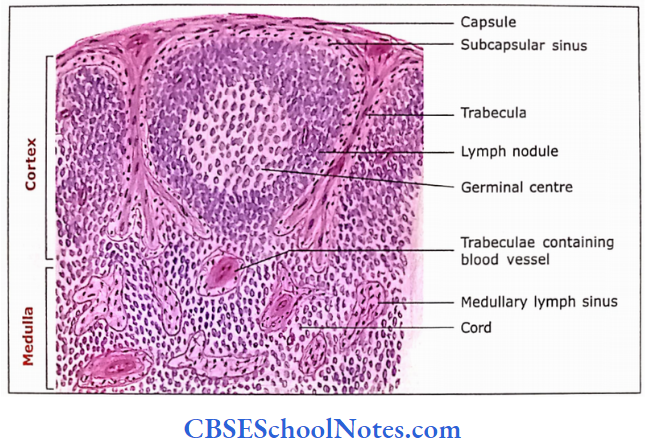
The Supporting Elements of Lymph Node:
- The connective tissue capsule surrounds the bean-shaped lymph node. It is made up of dense connective tissue (collagenous, elastic and a few reticular fibres).
- The trabeculae extend from the capsule into the substance ofthe lymph node
- Besides the capsule and trabeculae, the supporting elements in the organ are formed by reticular cells and reticular fibres, which form a meshwork throughout the cortex and medulla.
- Reticular cells synthesize reticular fibres (type 1 collagen) and ground substance. These cells also produce substance which attracts T and B lymphocytes and dendritic cells
- Dendritic cells, which are present in the parenchyma of lymph nodes are of bone marrow origin and they present the antigen t0 specific T cells
- This meshwork is not seen, in a histological section, as the spaces within this meshwork are occupied by densely packed iymph0cytes.
- This meshwork can be demonstrated by special staining
Passage of Lymph Through Lymph Node:
- Afferent lymphatic vessels pour their lymph into the subcapsular sinus, which is placed just under the capsule between the capsule and cortical lymphocytes.
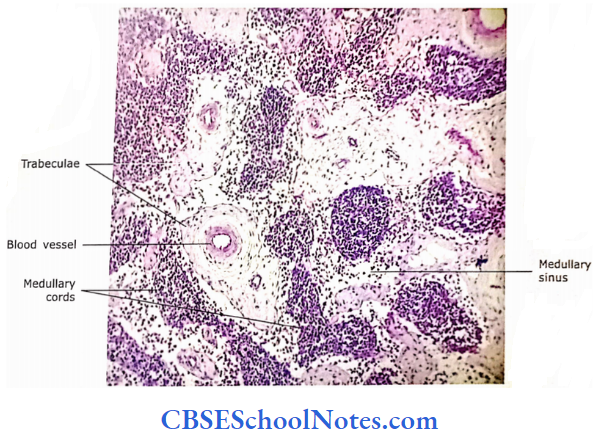
- From here the lymph flows deep inside the cortex in the secular sinuses and reaches the medullary sinuses.
- The sinuses within the medulla are in the form of
- Interanastomosing channels between cords of lymphocytes.
- The medullary sinuses then drain into an efferent lymphatic vessel at the hilum through which lymph passes through the lymph node.
- The sinuses are lined by endothelium, but their wall allows passage of lymphocytes into and out of sinuses
The Parenchyma of Lymph Node:
The parenchyma of the lymph node is present in the form of the cortex and medulla. The cortex is darkly staining the outer portion of the node deep to the capsule. The cortex is further divided into the outer and deep cortex. Lymphocytes are the most numerous cells of parenchyma.
These lymphocytes’ outer cortex are organized in the form of nodules, which may be in the form of primary nodules (nodules is made up of small lymphocytes with heterochromatic nuclei with very little cytoplasm and thus is deeply stained) or secondary nodules (nodules possessing germinal centre,
Germinal centre stains lightly because there are few dark staining small lymphocytes, but there are more light staining large lymphocytes (lymphoblasts, with euchromatic nucleus and clear rim of cytoplasm), macrophages and young plasma cells.
The lymphocytes in the deep cortex are not organized in the form of nodules, but they are diffusely arranged. B lymphocytes are predominantly present in the outer cortex but T lymphocytes are present in the deep cortex
Cortex Medulla Remember:
The cortex of the medulla is rich in B lymphocytes, while the cortico-medullary junction of the lymph node is rich in T cells.
The medulla is the inner part ofthe node and consists of lymphocytic tissue arranged in the cords called as medullary cords.
Besides lymphocytes both the cortex and medulla also contain the following types of cells:
- Reticular cells: These cells along with reticular fibres serve as the framework of the lymph node.
- Plasma cells: B lymphocytes mature into antibody-producing plasma cells. These cells are mainly present in medullary cords
- Macrophages: These cells are mainly present in the medulla but are also common in the germinal centres. These cells are phagocytic, which hold and present antigens to lymphocytes to aid the immune response
- The antigen-presenting cells (APCs) like dendritic and follicular dendritic cells are also present in the lymph node.
- The Parenchyma of the cortex and medulla is traversed by blood vessels and lymph sinus both of which are lined by endothelial cells.
Functions of Lymph Node:
It serves as filter of lymph. Filtration occurs in two different ways, i.e., the reticular meshwork (meshwork formed by reticular fibres and reticular cells) obstructs The foreign bodies (antigens), while these foreign bodies are phagocytosed by macrophages.
The foreign bodies are presented to lymphocytes by reticular cells and macrophages, which aid in immunological reactions.
- Both B and T lymphocytes are produced by lymph nodes. Thus, both humoral and cellular immune functions oc¬ cur here.
- B lymphocytes mature to form plasma cells in lymph nodes, which produce antibodies.
- Re-circulation of B and T lymphocytes takes place here through lymph nodes, i.e., the circulating B and T lymphocytes may enter the lymph node through postcapillary venule and may pass in lymph via the efferent lymphatics, draining to the thoracic duct
Lymph node Remember:
The lymph node is an important site where foreign bodies are phagocytosed by macrophages. The immune response is initiated when foreign bodies are presented to lympho¬ cytes by reticular cells and macrophages.
The Circulation of Lymphocytes Through Lymph Node:
In addition to lymph, lymphocytes also circulate through the lymph node. The lymphocytes enter the lymph node from two different sources.
Few lymphocytes enter the lymph node through afferent lymphatic vessels and reach into the network of lym¬ phatic sinuses. From the sinus, they enter into the cortex of the lymph node where they engage in immunosurveillance. This lymphocyte now comes back to the sinuses and migrates out of the lymph node through efferent lymph vessels.
- Many lymphocytes enter the deep cortex lymph node through the wall of postcapillary venules.
- Postcapillary venules are specialized blood vessels because they are lined by cuboidal or columnar endothelial cells, hence, also called as high endothelial venules. These endothelial cells have receptors to identify specific types of lymphocytes.
- They signal lymphocytes to leave the postcapillary venule (by passing between endothelial cells) and migrate into the deep cortex of lymph node.
From here lymphocytes migrate in the entire cortex and after performing their function of immunosurveillance they mi¬grate in lymph sinuses to come out of the lymph node through efferent lymph vessels.
Lymph node Clinical Applications
Lymphadenitis (Enlargement of Lymph Nodes) Lymph nodes are located along the path of lymph ves¬ sels. Lymph flows from one node to the next. Lymphad¬ enitis is the name given to the enlargement of lymph nodes, which is usually secondary to the infection in the area of drainage of lymph.
The most common infection causing lymphadenitis is due to streptococcal and staphylococcal bacteria. Common symptoms of acute lymphadenitis are swollen and tender nodes, fever and gen¬ eral weakness. Lymph nodes are also enlarged secondary to cancer (malignancy) in the region of drainage
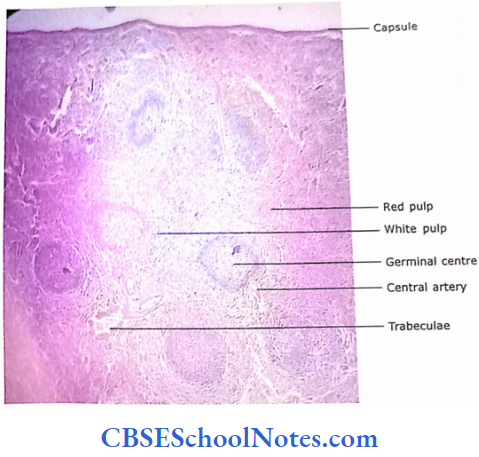
2. Spleen
The spleen, similar to the lymph node, is an encapsulated lymphatic organ. Lymph nodes filter the lymph while blood is filtered through the spleen (thus blood is monitored immunologically by the spleen). In humans, the spleen is a single large organ present in the upper abdomen and covered by the peritoneum.
A cut section through the spleen shows the substance of the spleen arranged in the form of limited pulp and red pulp. In a fresh section of the spleen (unstained), the white pulp is seen as circular grey areas scattered randomly throughout the substance of the spleen.
The white pulp is surrounded by red pulp. In the hematoxylin-stained section, the white pulp appears as basophilic due to the presence of small lymphocytes with heterochromatic nuclei. The red pulp appears red because it contains many blood sinuses filled with RBCs.
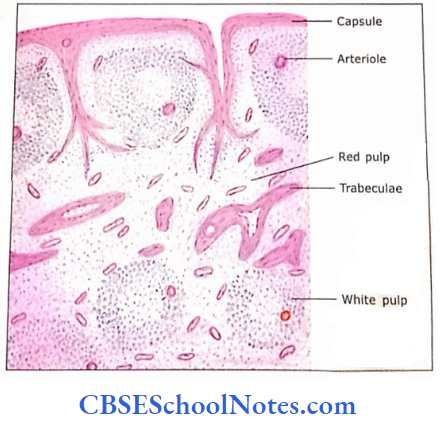
The Supporting Elements of Spleen:
The spleen is covered by a capsule made up of dense connective tissue. The capsule contains elastic fibres. From the capsule, trabeculae extend into the substance ofthe organ where they repeatedly divide to form a network. Small spaces within the trabecular network are occupied by the delicate meshwork formed by reticular cells and reticular fibres.
- Macrophages are also present in this delicate meshwork. The spaces of this meshwork are filled by lymphocytes, macrophages and blood cells.
- In red pulp, these cells are arranged in the form of cords, which itself forms a network
- These cords are called splenic cords. Spaces between cords are occupied by blood sinusoids.
- The hilus of the organ gives passage to the splenic artery, vein, nerves and efferent lymphatic vessels.
- The spleen has no afferent lymphatic vessels and efferent vessels originate in the white pulp through which lymphocytes go out of the spleen
Circulation of blood Through the Spleen:
- The splenic artery enters at hilum and its branches travel in the trabeculae.
- After repeated branching within trabeculae, the final branch enters the pulp where it is covered by the aggre¬ gation oflymphocytes.
- This peri-arteriolar lymphatic sheath is called the white pulp. At the centre of the white pulp is the central artery. The central artery then enters red pulp and terminates by branching into straight vessels that are called penicillin.
- Penicilli shows localized thickening called as an ellipsoid. Penicillin continues as arterial capillaries. The mode of flow of blood between arterial capillaries and splenic sinuses is yet not clear. Two different theories (open and closed circulation theories) have been proposed.
- According to the ‘closed circulation theory,’ arterial capillaries open directly into splenic sinuses that drain into tributaries of splenic veins that are present in trabeculae.
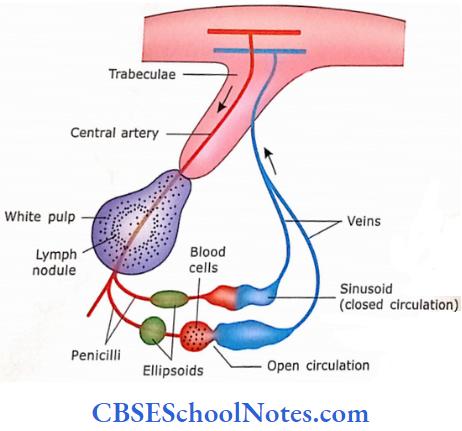
The splenic vein thus formed comes out from the hilus of the spleen.
According to the “open circulation theory,” the arterial capillaries open and pour their blood into splenic cords of pulp,
The blood cells from here (splenic cords) then enter the blood sinuses by passing between endothelial cells lining the wall of the sinus.
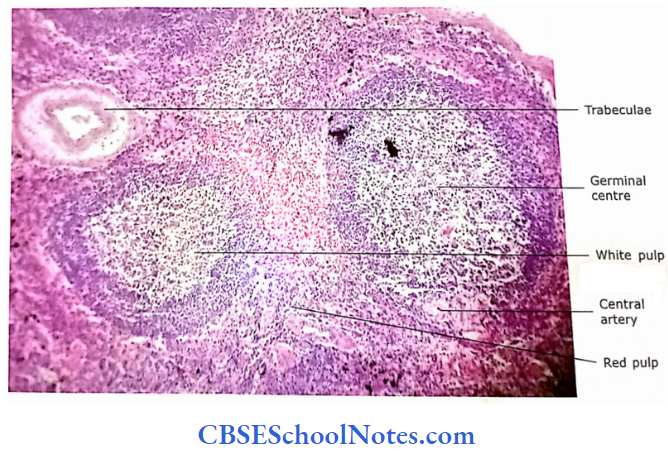
Pulps of Spleen:
The substance of the spleen consists of two different types of 2 1 pulp, i.e., white pulp and red pulp S The white pulp is the lymphatic tissue sheath that surrounds * the central artery. It contains lymphocytes and macrophages P in a reticular connective tissue meshwork.
This peri-area rial lymphatic tissue sheath may also contain lymphatic nodules with germinal centres. These nodules are called splenic & nodules or Malpighian corpuscles. Most of the lymphocytes in while pulp are T lymphocytes while nodules predominantly contain B lymphocytes.
The red pulp consists of a network of inter-anastomosing splenic cords. The splenic cords are made up of reticular cells and reticular fibres containing B and T lymphocytes, macrophages, plasma cells, RBCs and granulocytes. These splenic cords are also called “cords of Billroth.” In between the splenic cords, spaces are filled with branch¬ ing venous sinuses.
The macrophages and lymphocytes come in contact with the antigens present in circulating blood. This leads to the initiation of an immune response against blood-borne antigens
Spleen Remember:
The periarterial lymphatic sheath of white pulp contains T cells, while the lymphoid nodule of white pulp contains B cells. The red pulp of the spleen consists of blood sinuses and splenic cords
Spleen Functions
- Filtration of blood.
- Immune response against antigens circulating in the blood. Site for production of B and T lymphocytes.
- Aged and abnormal RBCs are detained and destroyed in the red pulp by the macrophages of the splenic cord.
- Macrophages also remove bacteria by phagocytosis. Storage of blood.
- Formation of blood cells during fetal life.
- The spleen may enlarge secondary to malaria and leukaemias.
- The spleen is not an essential organ and can be surgically removed if required (as in the case of profuse bleeding alter injury to the spleen).
Spleen Clinical Application
Rupture of Spleen:
The spleen is a fragile organ and presents relatively superficial in the abdomen, therefore trauma to the spleen may lead to its rupture. As it is a highly vascular organ, rupture leads to rapid and massive bleeding, which may result in the death of a person soon after injury. In some cases, the spleen can be removed surgically without affecting the life of a person because its function of removal of aged red blood cells is taken over by macrophages present in the liver and bone marrow.
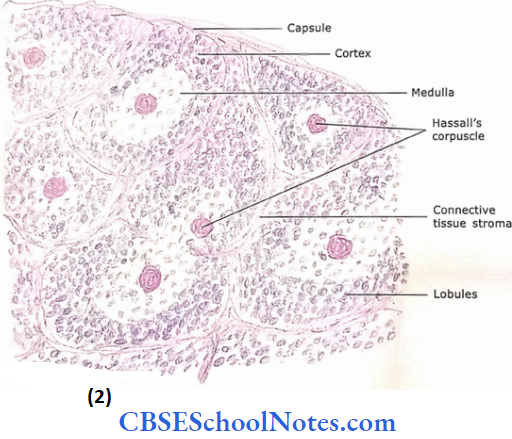
3. Thymus
It is an encapsulated lymphatic organ, which neither filters lymph (like a lymph node) nor blood (like a spleen). This is the only lymphatic organ, which is fully developed at birth, while organs such as lymph nodes, tonsils and spleen are underdeveloped and require the migration of B and T cells for their development.
Supporting Elements of Thymus:
Both the lobes of the thymus are completely covered by a thin layer of connective tissue capsule from which trabeculae extend into the substance of the organ. These trabeculae partially subdivide the lobe of the thymus into thousands of lobules, each of which has a cortical cap over inner medullary tissue.
- The medullary tissues are partly divided by the trabeculae, hence the medullary tissue of adjacent lobules are continuous with each other.
- Thus, the medulla is a continuous branching mass surrounded by the cortex. Through these trabeculae pass the blood vessels, nerves and lymphatics.
- The thymus has only efferent lymphatic
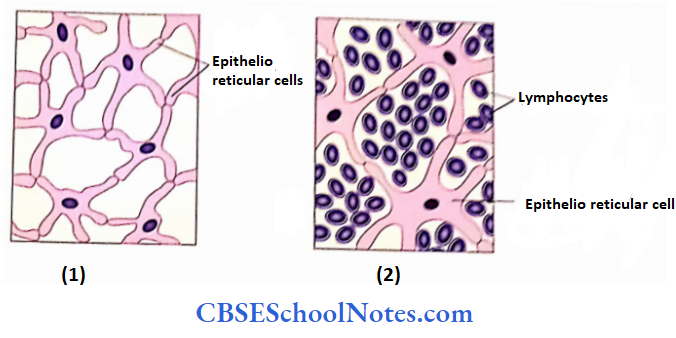
- The delicate supporting stroma of the organ, within a lobule, is formed by epithelial-reticular cells. These cells are stellate in shape and their cytoplasmic processes are joined with the processes of neighbouring cells with the help of desmosomes.
- Thus, epithelioreticular cells form a cytoplasmic reticulum within the thymus. This reticulum is different from the reticulum present in the spleen and lymph nodes.
- In the spleen and lymph node, the reticulum is formed with the help of reticular cells and reticular fibres.
The epithelioreticular cells envelope the thymic blood capillaries to form a “blood-thymic barrier.”It is believed that the blood-thymic barrier does not allow any antigen to enter the thymus where T lymphocytes are maturing, which otherwise may influence the development of T lymphocytes
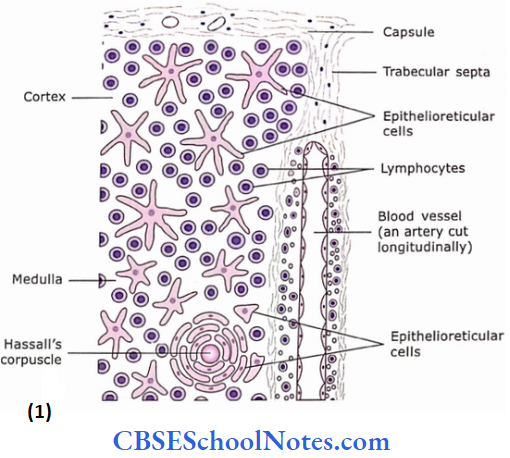
MicroscopicStructure of Thymic Lobule:
Each lobule of the thymus is surrounded by connective tissue stroma and contains an outer cortex and inner medulla
The cortex contains a higher concentration oflympho¬ cytes than the medulla. The cortex is darkly stained because of densely packed small lymphocytes with heterochromatic nuclei.
The outer cortex receives stem cells from bone marrow”‘ which divide repeatedly to form small lymphocytes. These cells form the cellular framework for the entire 1 – These small, maturing lymphocytes then move towards the medulla. The mature lymphocytes leave the thymus via veins and lymphatics.
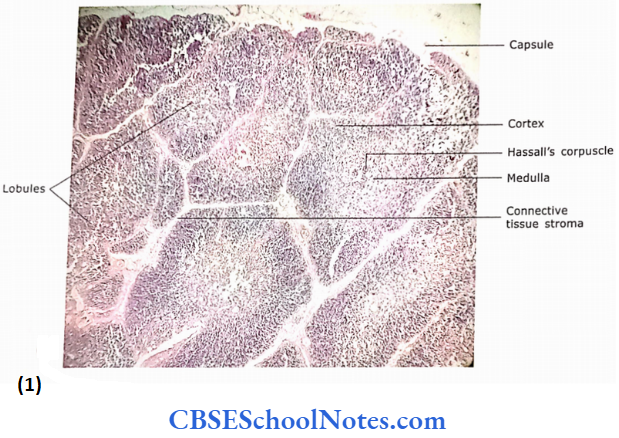
This entire process takes about 24 hrs The medulla stains lightly compared to the cortex because here lymphocytes are less densely packed. Because of this reason, epithelioreticular cells are more obvious. The ta i medulla also contains thymic or Hassall’s corpuscles. !lu; These are masses of concentrically arranged type 6 l epithelioreticular cells around a central degenerated homogeneous mass.
The Hassall’s corpuscles stain pink with acid |u dyes and their number increases with increasing age. The macrophages are found in large numbers both in the cortex and medulla. They engulf antigens and also remove the lymphocytes, which might have been produced in excess.
Thymic Remember:
In the thymic cortex, immunologically incompetent T cells acquire the immunological competency (site of maturation of T lymphocytes), while the medulla consists of all immune-competent T cells.
Thymic Epithelioreticular Cells:
Epithelioreticular cells provide a skeletal framework of the thymus, which is similar to the reticular cells and their associated fibres in the spleen and lymph node
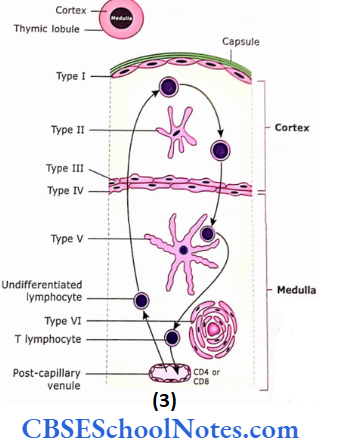
Epithelioreticular cells show some features of epithelial cells such as the presence of intercellular junction and intermediate filaments. The thymus exhibits six different types of epithelioreticular cells, i.e., types 1,2,3,4, V and 6. Out of these six types, types 1,2 and 3 are present in the cortex and the remaining three in the medulla. It is believed that epithelioreticular cells are derived from the endoderm of third and fourth pharyngeal pouches.
The epithelioreticular cells provide an isolated and protective environment to developing (immature) lymphocytes.
The following functions can be attributed to various kinds of reticuloendothelial cells:
- Type 1: They isolate lymphocytes from neighbouring connective tissue (capsule and trabeculae) and blood vessels of the cortex. These cells form occluding junctions with each other, thus isolating the thymic cortex from the remainder of the body
- Type 2: These cells are present in mid cortex and form an isolated compartment for developing T cells
- Types 3 & 4: These cells are present at the cortico-medullary junction. They form a functional barrier between the cortex and medulla
- Type 5: These cells form the cellular framework for entire medulla lymphocytes. and form compartments for various groups of
- Type 6: They form thymic corpuscles. Thymic cor¬ puscles are isolated masses of closely packed concentrically arranged type 6 epithelioreticular cells. They contain flattened nuclei and their number increases with the increase in age.
Though the function of the thymic corpuscle is not known it is believed that type 6 cells are involved in the production of interleukins (IL-4 and IL-7) that help in the differentiation and education of T lymphocytes. Some believe that thymic corpuscles are the site for the death ofT lymphocytes
Thymic (Hassall’s) Corpuscles:
The type 6 epithelioreticular cells form thymic corpuscles. These cells of the thymic corpuscle show keratohyalin granules, intermediate filaments and lipid droplets in their cytoplasm. The centre of the corpuscle shows the keratinization of epithelioreticular cells. Thymic corpuscles are functionally active multicellular components of the medulla that are capable f producing hormones like thymosin and thym opoietin.
Blood-Thymic Barrier:
Further Details The thymic barrier helps to protect the developing immature lymphocytes in the thymus from exposure to the external environment (antigens).
The following are the constituents of blood thymic barrier:
- Capillary endothelium with basal lamina and pericytes
- Perivascular connective tissue space containing macrophages
- TypeI epithelioreticular cells with their basal lamina
Thus, the perivascular connective tissue space is located between the basal laminar capillary endothelium and basal lamina ofepithelioreticular cells. The macrophages present in perivascular connective tissue phagocytose the antigenic molecules that may come out from the capillary lumen. Thus,the layers of the blood-thymus barrier provide necessary protection to the developing immature T lymphocytes and separate them from mature lymphocytes, which are circulating in the bloodstream
Blood Thymic Barrier Remember:
Blood-thymus barrier protects the developing T cells in the cortex form the macromolecules present in the blood
Thymus Functions:
- The thymus receives immunologically incompetent stem cells from bone marrow and provides the environment where they can divide and mature into T lymphocytes.
- The mature T lymphocytes are then carried from thymus, via blood, to the lymph nodes, spleen and other lymphatic tissues.
- T cells are important for both cellular and humoral immunological responses.
- Epithelioreticular cells secrete many factors.
- Thymopoietin induces T cell production and maturation.
- Thymosin supports T cell activities throughout the body.
- Thymus is essential till puberty. After puberty, the other lymphatic tissues ofbody are fully developed; hence, the thymus gets atrophied
Thymus Remember:
The thymus is a primary lymphoid organ where T lymphocytes are immunologically matured.
Thymus Clinical Application:
- Myasthenia Gravis: Myasthenia gravis is a rare autoimmune disorder in which the immune system produces antibodies that attack and slowly destroy the receptors in muscles that receive nerve impulses.
- As a result, the affected muscle fails to respond or responds only weakly to nerve impulses. The muscles of the throat, face and eye are most commonly affected.
- The other muscles may also be affected.
- The cause of the autoimmune disorder is not known, but about 70% of people suffering from this disorder have an abnormality of the thymus gland.
- The most common abnormality of the thymus gland associated with this disorder is thymoma (a noncancerous tumour of the thymus
- DiGeorge’s Syndrome: This syndrome is characterized by the congenital absence of the thymus gland.
- The patient is unable to produce T lymphocytes, thus cell-mediated immune response is not functional.
- Patients may die at a young age due to infection. Since the thymus is absent, the parathyroid gland also fails to develop.
- In the absence of a parathyroid, death may be caused due to tetany.
Lymphatic Tissue In Other Organs
As stated earlier, the mucosa-associated lymphoid tissue (MALT) consists of localized lymphocyte infiltration and lymphoid nodules in the mucosa of GIT (tonsil, Peyer’s patches of intestine, appendix), respiratory (bronchus), re¬ productive and urinary tracts.
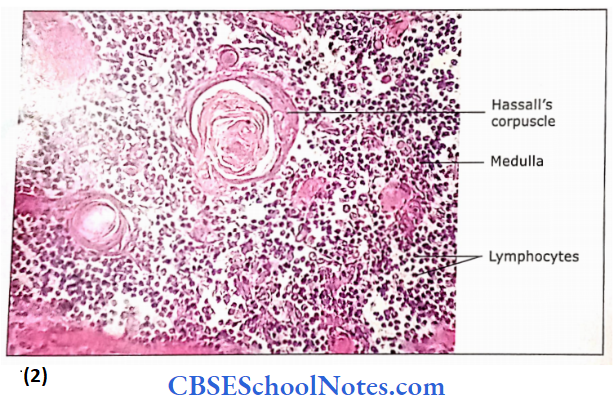
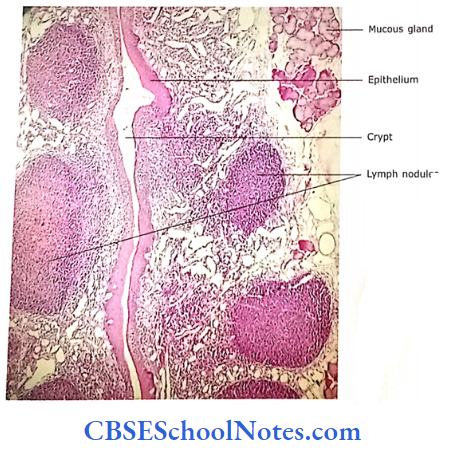
Palatine Tonsil:
- Palatine tonsils are collections of lymphoid tissue in the mucosa of oropharyngeal isthmus.
- Each tonsil consists of an aggregation of lymphatic nodules within the diffused lymphoid tissue
- This lymphoid tissue is present just beneath the stratified
squamous epithelium ofthe oropharynx. - This epithelium at places may go deep into the substance of the tonsil. This invagination epithelium within the lymphoid tissue is called as epithelial crypt.
Tonsil has only efferent lymphatic vessels. Infection of the tonsil is called tonsillitis
Tonsil Functions:
- Production of lymphocytes.
- Immunological responses against the antigens and organisms coming in contact with epithelium
Tonsil Clinical Application
Tonsillitis: The infection of the tonsil may be caused either by virus or by bacteria. The tonsillitis is common in children because their tonsils are exposed to infections for the first time. Tonsils become smaller with increasing age and hence tonsillitis is also less common in adults. Surgical removal of tonsils (tonsillectomy) is performed on children who have recurrent tonsillitis.