
Disorders Of the Gastrointestinal System
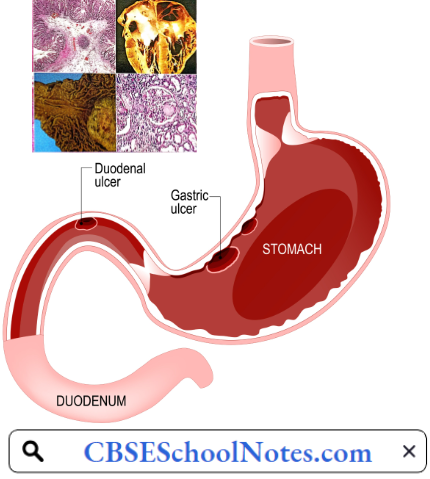
Peptic Ulcer
Peptic ulcer disease presents as a duodenal ulcer or gastric ulcer. During the last few decades, the incidence of peptic ulcer disease has decreased in India. In one study, the prevalence of duodenal ulcers was 12% in 1988, but it declined to 3 % in 2008. During the same period, gastric ulcer prevalence declined from 4.5% to 2.7%.
Peptic Ulcer Symptoms
- Burning stomach pain. The most common symptom of a duodenal ulcer is waking at night with upper abdominal pain that improves with eating. With a gastric ulcer, the pain may worsen with eating. The pain is often described as a burning or dull ache.
- The feeling of fullness, bloating, or belching
- Fatty food intolerance
- Heartburn
- Nausea
Read and Learn More Pathophysiology
Causes Of Peptic Ulcer
- H. pylori infection
- NSAIDs
- Alcohol
- Cigarette smoking
- Psychogenic stress
Peptic Ulcer Pathogenesis: It is a physiological marvel that gastric juice can easily digest the swallowed pieces of meat but normally, it has no corrosive action on the gastric mucosa itself. Several factors seem to be involved in the protection of gastric mucosa from autodigestion. These factors, collectively known as the gastric mucosal barrier, include:
- Mucus secreted by surface epithelial cells and mucus neck glands which forms a water insoluble visco-elastic gel with poor diffusion coefficient for H+.
- Bicarbonate is secreted by surface epithelial cells into the boundary zone between the epithelial cells and the mucus layer. The secretion of mucus and bicarbonate is believed to be mediated through prostaglandins.
- Tight Junctions between the adjacent cells of gastric surface epithelium.
- Rapid Turnover of surface epithelial cells, and rich blood supply.
- Prostaglandins: Endogenous prostaglandins stimulate the secretion of gastric mucus as well as gastric and duodenal mucosal bicarbonate. Prostaglandins also participate in the maintenance of gastric mucosal blood flow and integrity of the mucosal barrier and promote epithelial cell renewal in response to mucosal injury.
Under normal conditions, a physiologic balance exists between peptic acid secretion and gastro-duodenal mucosal defense. Mucosal injury may lead to peptic ulcer when the balance between the aggressive factors and the defensive mechanisms is disrupted.
- Aggressive factors, such as H. pylori, NSAIDs, alcohol, cigarette smoking, and psychogenic stress can alter the mucosal defense and allow back diffusion of hydrogen ions and subsequent epithelial cell injury.
- Mechanisms of injury differ distinctly between duodenal and gastric ulcers. Duodenal ulcer is essentially an H. pylori-related disease and is caused mainly by an increase in acid and pepsin load, and gastric metaplasia in the duodenal cap.
- Gastric ulcer is most commonly associated with NSAID ingestion, although H. pylori infection might also be present. Chronic, superficial, and atrophic gastritis predominate in patients with gastric ulcers when even normal acid levels can be associated with mucosal ulceration.
- Role Of Helicobacter Pylori: Helicobacter pylori is a bacillus responsible for one of the most common infections found in humans worldwide. H. pylori inhabit the mucus- adjacent to the gastric mucosa. Helicobacter pylori bacteria colonize the stomach and induce chronic gastritis.
- H. pylori is able to survive the highly acidic environment of the stomach because it protects itself by release of an enzyme urease, that splits blood urea and produces ammonia. The type of ulcer that develops depends on the location of chronic gastritis, which occurs at the site of H. pylori colonization.
- In those with duodenal ulcers, H. pylori colonizes the antrum. The inflammatory response to the bacteria causes destruction of somatostatin-producing D cells in the pylorus. Consequently, the G cells in the antrum secrete more of the hormone gastrin, which travels through the bloodstream to the fundus and body of the stomach.
- Gastrin stimulates the parietal cells to secrete more acid into the stomach lumen. Chronically increased gastrin levels eventually cause the number of parietal cells to also increase, further escalating the amount of acid secreted. The increased acid load damages the duodenum, and ulceration may eventually result.
- In contrast, in gastric ulcers, H. pylori colonizes the corpus of the stomach, where the acid-secreting parietal cells are located. However, chronic inflammation induced by the bacteria leads to a reduction of acid production, and eventually atrophy of the stomach lining. Gastric atrophy may lead to gastric ulcers and increase the risk of stomach cancer.
- Non-Steroidal Anti-Inflammatory Drugs: Non-steroidal anti-inflammatory drugs (NSAIDs) including low-dose aspirin are some of the most commonly used medicines. They are associated with gastrointestinal mucosal injury.
- Endoscopic studies have shown a prevalence rate of 14-25% of gastric and duodenal ulcers in NSAID users, NSAID acts as anti-inflammatory agents by inhibition of prostaglandin (PG) synthesis. As discussed earlier, prostaglandins are an important component of the gastric mucosal barrier. Inhibition of PG synthesis breaks the gastric mucosal barrier leading to peptic ulcers.
- Smoking: Cigarette smoking appears to be a risk factor for the development, maintenance, and recurrence of peptic ulcer disease. Smokers are about two times as likely to develop ulcer disease as non-smokers. Smoking predisposes to peptic ulcer by
- Acceleration of gastric emptying of liquids,
- Promotion of duodenal-gastric reflux,
- Reduction in mucosal blood flow, and
- Inhibition of mucosal prostaglandin production. Cigarette smoking not only causes ulcer formation but also increases the risk of ulcer complications such as ulcer bleeding, stomach obstruction, and perforation.
- Since cessation of smoking is associated with the prompt recovery of the respective functions, smokers will benefit immediately by stopping or reducing cigarette consumption.
- Cigarette smoking is also a leading cause of failure of medicinal treatment of peptic ulcers.
- Role Of Stress: The development of acute gastric ulcers as a result of severe stress after major surgery or extensive bums is well known. Reduced gastric blood flow coupled with raised plasma cortisol levels seem to be primarily responsible for such ulcers.
- Till the 1980s, psychological stress was considered the chief cause of the duodenal ulcers.
- The high-stung type “A” individuals were considered special candidates for the development of duodenal ulcers. In the 1990s, after the discovery of H. pylori, it began to be believed that psychogenic factors play no role in the development of chronic peptic ulcer disease.
- Over the years, it is now been appreciated that psychogenic stress acts as a co-factor with H. pylori in the production of hyperacidity leading to duodenal ulcers.
Peptic Ulcer Risk Factors
- Alcohol
- Spicy food
Alone, these factors do not cause ulcers, but they can make them worse and more difficult to heal.
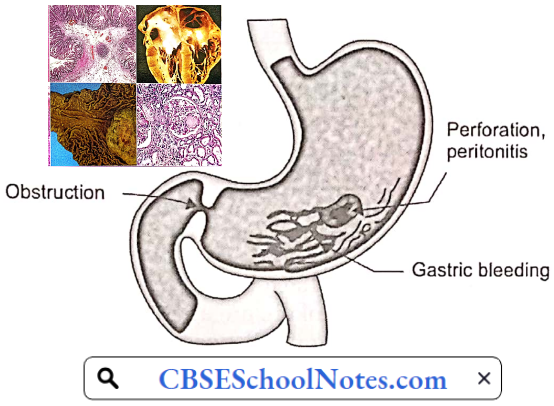
Peptic Ulcer Complications: Left untreated, peptic ulcers can result in serious complications:
- Internal Bleeding: Bleeding can occur as slow blood loss that leads to anemia or as severe blood loss that may require hospitalization or a blood transfusion. Severe blood loss may cause black or bloody vomit or black or bloody stools. s
- Infection: Peptic ulcers can perforate the wall of the stomach putting at risk of a serious infection called peritonitis.
- Obstruction to the passage of food.
Hepatitis
Hepatitis is an inflammation of the liver. The condition can be self-limiting or can progress to fibrosis (scarring), cirrhosis, or liver cancer. Hepatitis viruses are the most common cause of hepatitis in the world but other infections, toxic substances (for example, alcohol, and certain drugs), and autoimmune diseases can also cause hepatitis.
Viral Hepatitis: Viral hepatitis is one of the major public health concerns around the world. Every year 1.4 million people die from viral hepatitis-related cirrhosis and liver cancer. Viral hepatitis is a cause for major healthcare burden in India as well.
There are 5 main hepatitis viruses, referred to as types A, B, C, D, and E. Viral hepatitis A, B, and E is an acute disorder. Types B and C lead to chronic hepatitis in hundreds of millions of people and, together, are the most common cause of liver cirrhosis and cancer.
- Hepatitis A virus (HAV) is present in the feces of infected persons and is most often transmitted through consumption of contaminated water or food. Most people in areas of the world with poor sanitation have been infected with this virus.
- Hepatitis B virus (HBV) is transmitted through exposure to infective blood, semen, and other body fluids. Transmission occurs through transfusions of HBV-contaminated blood and blood products, contaminated injections during medical procedures, and through injection drug use.
- HBV also poses a risk to healthcare workers who sustain accidental needle stick injuries while caring for infected HBV patients.
- Hepatitis C Virus (HCV) is mostly transmitted through exposure to infective blood. This may happen through transfusions of HCV-contaminated blood and blood products, contaminated injections during medical procedures, and through injection drug use. Sexual transmission is also possible but is much less common.
- Hepatitis D Virus (HDV) infections occur only in those who are infected with HBV. The dual infection of HDV and HBV can result in a more serious disease and worse outcome.
- Hepatitis E virus (HEV) is mostly transmitted through consumption of contaminated water or food. HEV is a common cause of hepatitis outbreaks in developing parts of the world and is increasingly recognized as an important cause of disease in developed countries.
Symptoms And Signs Of Hepatitis A
- Fatigue
- Sudden nausea and vomiting
- Abdominal pain or discomfort, especially on the upper right side beneath the lower ribs (site of the liver)
- Clay-colored stools
- Loss of appetite
- Low-grade fever
- Jaundice
- Dark urine
- Joint pain
- Intense itching
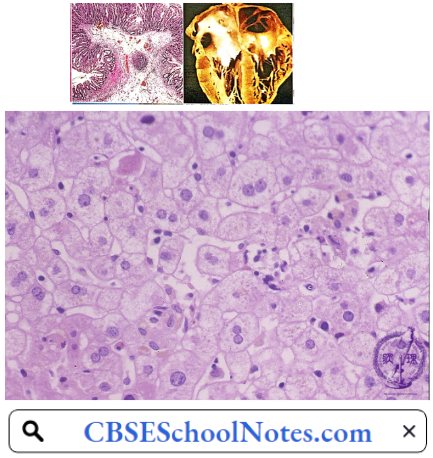
Pathology of Acute Hepatitis: The characteristic histopathological features of acute hepatitis include
- Ballooning degeneration
- Spotty necrosis
- Predominantly sinusoidal and lobular mononuclear cell infiltrate
- Kupffer cell hyperplasia
- Scattered apoptotic bodies
- Hepatocellular regeneration
Complications of Acute Hepatitis: Hepatic failure
Complications Of Chronic Hepatitis
- Hepatic failure
- Liver cirrhosis
- Hepatic cancer
Jaundice
Jaundice is a yellow discoloration of the skin, mucous membranes, and the whites of the eyes caused by increased amounts of bilirubin in the blood. Serum bilirubin level is normally below 1.0 mg/ dL, and levels over 2-3 mg/dL typically result in jaundice.
Bilirubin Metabolism
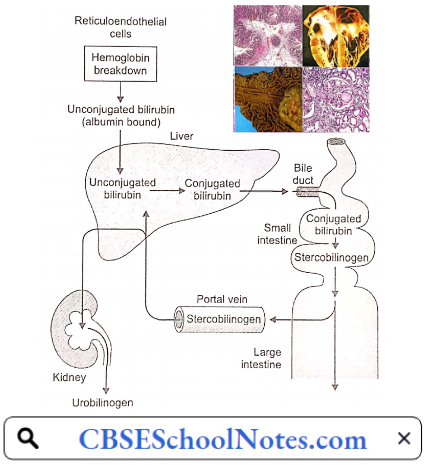
Destruction of senescent red blood cells in the tissue macrophages (in the spleen, liver, bone marrow, etc.) results in the catabolism of hemoglobin to haeme (and globin) and subsequently to bilirubin. Bilirubin released from the tissue macrophages is called unconjugated bilirubin.
- It is a lipid-soluble pigment transported in blood tightly bound to albumin. In the liver, the hepatocytes take up unconjugated bilirubin from the blood, convert it into water-soluble compounds called conjugated bilirubin (bilirubin mono- and di-glucuronide), and excrete it into bile canaliculi. The bile duct excretes conjugated bilirubin into the small intestine.
- Conjugated bilirubin cannot be absorbed in the intestines. In the large gut, bacterial degradation converts it to stercobilinogen (= urobilinogen), a water-soluble colorless product. Some of the urobilinogen is absorbed into the portal blood to reach the systemic circulation.
- Being water soluble, it is excreted into the urine by the kidneys. The remaining stercobilinogen is excreted in the feces. On exposure to air, stercobilinogen is oxidized to stercobilin which gives a brown color to the faeces.
- In obstructive jaundice, since bilirubin does not reach the intestines, stercobilinogen and urobilinogen excretion in the feces and urine is very low. That accounts for the pale chalky color of the stools of such patients.
Conjugated bilirubin is water-soluble; if present in the blood, it is excreted by the kidneys into the urine (bilirubinuria). Bilirubin imparts a dark brown color to the urine, an important clinical sign of conjugated hyperbilirubinemias (hepatic and post-hepatic jaundice). Classification of jaundice based on the pathophysiology of bilirubin metabolism is given below
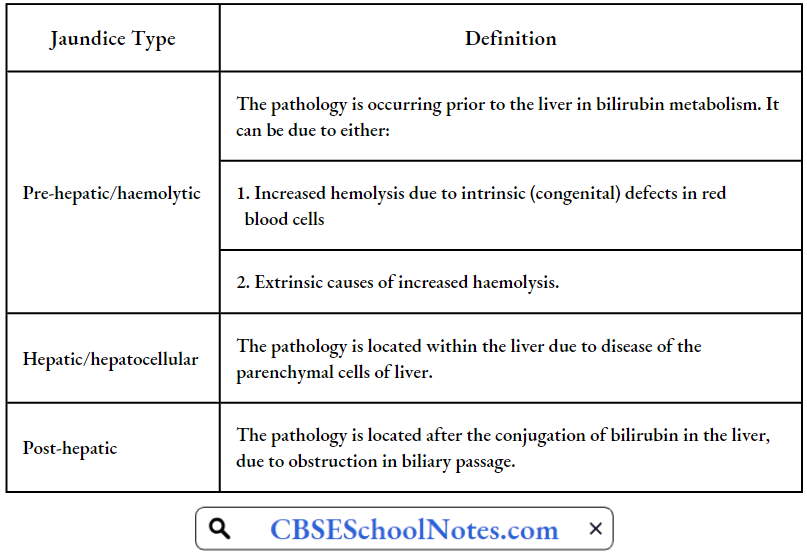
Pre-Hepatic Jaundice: Pre-hepatic jaundice is caused by an increased rate of hemolysis due to a congenital (sickle cell anemia, spherocytosis, thalassemia) or an acquired defect in the structure of red cells. The increased breakdown of red blood cells leads to an increase in the production of unconjugated bilirubin.
- The presence of excess of unconjugated bilirubin in blood causes its deposition into various tissues causing jaundice. Increased production of unconjugated bilirubin leads to increased production and increased excretion of stercobilinogen and urobilinogen in stools and urine respectively.
- Bilirubin is not found in the urine because unconjugated bilirubin is not water-soluble.
Pre-hepatic jaundice Laboratory Findings Include:
- Urine: Excess of urobilinogen, absent bilirubin.
- Serum: Increased unconjugated bilirubin.
Hepatic Jaundice: Hepatocellular (hepatic) jaundice results from an acute or chronic injury to hepatocytes (viral hepatitis, cirrhosis, alcoholic liver disease). Cell necrosis reduces the liver’s ability to take up, conjugate and excrete bilirubin. Therefore, the level of both unconjugated and conjugated types of bilirubin rises in the blood. The conjugated type of bilirubin, when present in the blood is excreted in the urine.
Hepatic Jaundice Laboratory Findings Include:
- Urine: Bilirubin present.
- Serum: contains excess of both conjugated and unconjugated bilirubin.
- Elevated levels of certain enzymes in the blood are indicative of hepatocellular injury.
Post-Hepatic Jaundice: Post-hepatic jaundice, also called obstructive jaundice, is caused by an interruption to the drainage of bile, containing conjugated bilirubin, in the biliary system.
- The most common causes are gallstones in the common bile duct, and cancer in the head of the pancreas, through which the bile duct passes. The back pressure on bile causes regurgitation of conjugated bilirubin and bile salts into blood circulation.
- In complete obstruction of the bile duct, bile does not reach the intestine, and stercobilinogen and urobilinogen are not found in the feces and urine, restively. Hence faeces have a pale chalky appearance.
Post-Hepatic Jaundice Laboratory Findings Include:
- Urine: Bilirubin present, urobilinogen absent
- Serum: contains excess of conjugated bilirubin.
Alcohol Liver Disease
Alcohol consumption is on the rise in India. Between 2010 and 2017, alcohol consumption in India increased by 38 per cent. In some parts of India, the prevalence of current alcohol use varies between 33% and 50%, with a higher prevalence among the lesser educated and the poor. In India, 15 people die every day from the effects of drinking alcohol.
Chronic Heavy Drinking May Lead To:
- Alcoholic fatty liver
- Alcoholic hepatitis
- Alcoholic cirrhosis (Laennec’s cirrhosis)
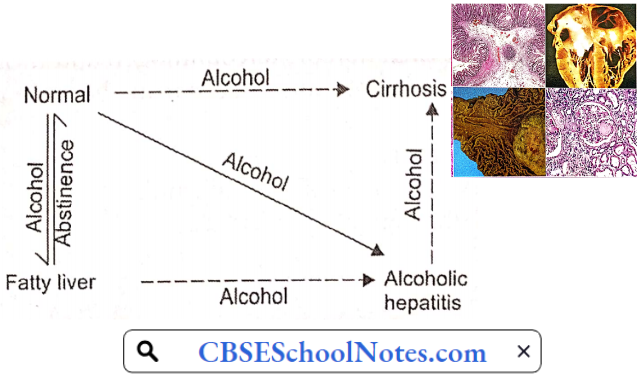
Between 10 and 20 percent of heavy drinkers will develop cirrhosis. Alcohol liver disease starts as an alcoholic fatty liver. It then progresses to alcoholic hepatitis, and then to alcoholic cirrhosis. Alcoholic liver cirrhosis is the most advanced form of liver disease that is related to drinking alcohol. Liver cirrhosis ends up as liver failure.
Alcohol Liver Disease Symptoms And Signs
- Alcoholic Fatty Liver
- Usually no symptoms
- Discomfort in the right upper abdomen (liver region)
- Fatigue
- Alcoholic Hepatitis
- Jaundice
- Fatigue
- Loss of appetite
- Low-grade fever
- Alcoholic Cirrhosis
- Fatigue
- Loss of appetite
- Nausea
- Ankles edema
- Nausea
- Vomiting
- Tenderness in the right upper abdomen
- Weight loss
- Jaundice
- Ascites
Pathogenesis Of Alcohol Liver Disease: In alcoholic liver disease, the total amount and duration of ethanol ingested rather than the type of alcoholic drink ingested determines the results. For example, 360 ml of beer (5% alcohol) and 45 ml of whisky contain the same amount of ethanol.
- Women appear to develop alcohol-induced liver injury at lesser levels of consumption than men. Malnutrition seems to augment the detrimental effects of alcohol. The cause of malnutrition in alcoholics is not merely economic. Even when economic problems is not present, alcoholism tends to produce malnutrition.
- In chronic alcoholics, alcohol itself may provide over 50% of total caloric requirements, which otherwise would have been provided by food containing proteins, vitamins, and minerals. The liver is the main site of alcohol metabolism.
- In the hepatocytes, alcohol is first oxidized to acetaldehyde, which is further oxidized to acetate. Both of these reactions increase the concentration of NADH which inhibits the operation of the citric acid cycle. Therefore, rather than undergoing further oxidation to CO2 and water, acetate is diverted to fatty acid synthesis.

Alcohol causes inhibition of fatty acid oxidation as well. Excessive concentration of acetaldehyde seems to inhibit biosynthesis and secretion of lipoproteins, the form in which fatty acids can be exported from the liver. Therefore, triglycerides accumulate in the hepatocytes, producing a “fatty liver”.
- Fatty liver may develop in any alcoholic after a bout of heavy drinking, but it is a reversible process. This condition presents clinically as a tender hepatomegaly with many non-specific symptoms such as malaise, weakness, anorexia, nausea, and abdominal discomfort.
- Elevated levels of hepatic enzymes may be the only laboratory finding. Jaundice is present in 15% of patients admitted to the hospital because of these symptoms of fatty infiltration of the liver.
- With total abstinence, the condition can return to normal within 2-4 weeks. However, continued alcohol consumption may result in more advanced forms of liver disease, either alcoholic hepatitis or cirrhosis.
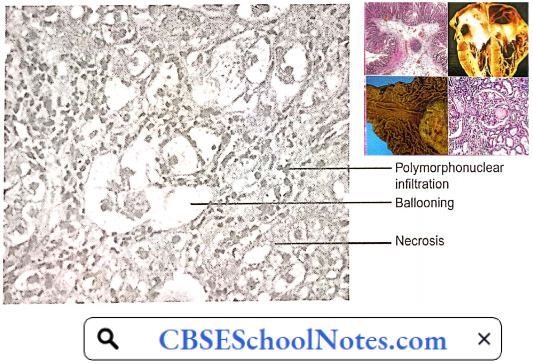
Alcoholic Hepatitis: Some 10-15% of chronic alcoholics develop alcoholic hepatitis. Alcoholic hepatitis is characterized by hepatocyte ballooning, hepatocyte necrosis, and polymorphonuclear infiltration.
Deposition of collagen fibers around the central vein and in the perisinusoidal area sets the stage for progression to cirrhosis. A cardinal sign of alcoholic hepatitis is the rapid onset of jaundice. Other common features include fever and ascites.
Encephalopathy may develop in those with severe hepatitis. Alcoholic hepatitis usually persists and progresses to cirrhosis if heavy alcohol use continues. If alcohol use ceases, alcoholic hepatitis resolves slowly over weeks to months, sometimes without permanent sequelae but often with residual cirrhosis.
Alcoholic Cirrhosis: The pathological hallmark of cirrhosis is the development of scar tissue that replaces normal hepatic parenchyma, blocking the portal flow of blood through the orga ]n and disturbing normal function.
- The fibrous tissue bands (septa) separate hepatocyte nodules; which eventually distort the entire liver architecture, and obstruct the normal hepatic blood flow leading to portal hypertension.
- Alcoholic liver cirrhosis is the most advanced form of liver disease that is related to drinking alcohol. Portal hypertension is responsible for most severe complications of cirrhosis such as edema feet, ascites, and bleeding from esophageal varices.

Complications Of Liver Cirrhosis
- Ascites
- Edema feet
- Bacterial peritonitis
- Bleeding from esophageal varices
- Hepatic encephalopathy
- Liver cancer
Inflammatory Bowel Disease
Inflammatory bowel disease (IBD) is an umbrella term used to describe disorders that involve chronic inflammation of your digestive tract. Types of IBD include
- Ulcerative Colitis: In ulcerative colitis, inflammation begins in the rectum and extends proximally in an uninterrupted fashion to the proximal colon, eventually involving the entire length of the large intestine. The small intestine is never involved.
- The rectum is always involved in ulcerative colitis, and no “skip areas” (i.e. normal areas of the bowel interspersed with diseased areas) are present. Ulcerative colitis primarily involves the mucosa and the submucosa, with the formation of crypt abscesses and mucosal.
- Crohn’s Disease: In Crohn’s disease, the most common location is the ileocecal region, followed by the terminal ileum Diseased segments frequently are separated by intervening normal bowel, leading to the term “skip areas.”
- Inflammation can be transmural (extending through the entire depth of the intestinal wall), often extending through to the serosa, resulting in sinus tracts or fistula formation.
Inflammatory Bowel Disease Signs And Symptoms that are common to both Crohn’s disease and ulcerative colitis include:
- Diarrhea
- Fever and fa li gue
- Abdominal pain and cramping
- Blood in your stool
- Reduced appetite
- Unintended weight loss
Inflammatory Bowel Disease Cause: The exact cause of inflammatory bowel disease remains unknown. One possible cause is an immune system malfunction.
- Age: Most people who develop IBD are diagnosed before they are 30 years old.
- Family History: You are at higher risk if you have a close relative—such as a parent, sibling, or child—with the disease.
- Cigarette Smoking: Cigarette smoking is the most important controllable risk factor for developing Crohn’s disease.
- Nonsteroidal Anti-Inflammatory Medications: These medications may increase the risk of developing IBD or worsen the disease in people who have IBD.
Inflammatory Bowel Disease Complications Colon Cancer: Having IBD increases your risk of colon cancer. General colon cancer screening guidelines for people without IBD call for a colonoscopy every 10 years beginning at age 50. Ask your doctor whether you need to have this test done sooner and more frequently.
- Skin, Eye, And Joint Inflammation: Certain disorders, including arthritis, skin lesions, and eye inflammation (uveitis), may occur during IBD flare-ups.
- Bowel Obstruction: Crohn’s disease affects the full thickness of the intestinal wall. Over time, parts of the bowel can thicken and narrow, which may block the flow of digestive contents. You may require surgery to remove the diseased portion of your bowel.
- Malnutrition: Diarrhea, abdominal pain, and cramping may make it difficult for you to eat or for your intestine to absorb enough nutrients to keep you nourished. It is also common to develop anemia due to low iron or vitamin B12 caused by the disease.
- Ulcers: Chronic inflammation can lead to open sores (ulcers) anywhere in your digestive tract, including your mouth and anus, and in the genital area (perineum).