
Basic Principles Of Cell Injury And Adaptation
Cell Injury And Adaptation Definitions: Aetiology is the origin of a disease, including the underlying causes and modifying factors.
- Pathogenesis refers to the steps in the development of disease. It describes how aetiologic factors trigger cellular and molecular changes that give rise to the specific functional and structural abnormalities of the disease. Whereas etiology refers to why a disease arises, pathogenesis describes how a disease develops.
- Pathology describes the structural changes observed in a diseased tissue or an organ.
- Pathophysiology describes the biochemical, and functional changes that occur in cells, tissues, and organs in response to injury.
- Morphology describes changes in the gross (naked eye) or microscopic appearance of a tissue or an organ.
Read and Learn More Pathophysiology
Cell Injury And Adaptation Symptoms And Signs: A symptom is a subjective feeling of a departure from normal function that is apparent to a patient, reflecting the presence of an unusual state, or of a disease. A symptom can be subjective (felt by the patient) or objective (seen by the patient).
Tiredness is a subjective symptom, whereas cough or fever are objective symptoms. In contrast to a symptom, a sign is a clue to a disease elicited by an examiner or a doctor. For example, edema feet is a sign of congestive heart failure or liver failure.
Homeostasis Physiology
The mammalian cells are very sensitive. The cell’s survival and function is dependent on the maintenance of the internal environment. The composition of the internal environment may be disturbed by a variety of external or internal factors. Examples of external factors that may disturb the internal environment include exposure to extremes of heat or cold, absence of food, deficiency of oxygen, etc.
- Examples of internal factors that may disturb the internal environment include infections, blood loss, increased utilization of glucose, and production of excess lactic acid by vigorously contracting muscles during severe exercise, etc.
- In nil such conditions, various organs of the body maintain homeostasis, that is, act in a harmonious fashion and prevent marked changes in the physical and chemical composition of extracellular fluid. Failure of the homeostatic mechanism results in disturbed body function known as disease.
Homeostatic Mechanisms: Various physiological or pathological processes tend to disturb one or more components of the internal environment. The disturbance sets into motion a series of physiological responses that eliminate the disturbing factor and normalize the composition of extracellular fluid. The homeostatic mechanisms allow an organism to function effectively in a broad range of environmental conditions.
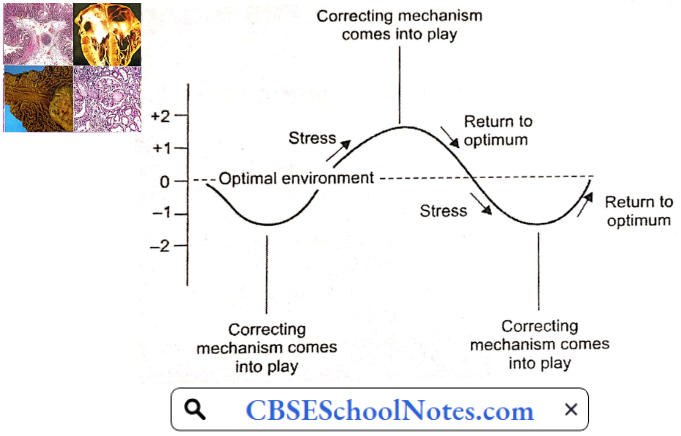
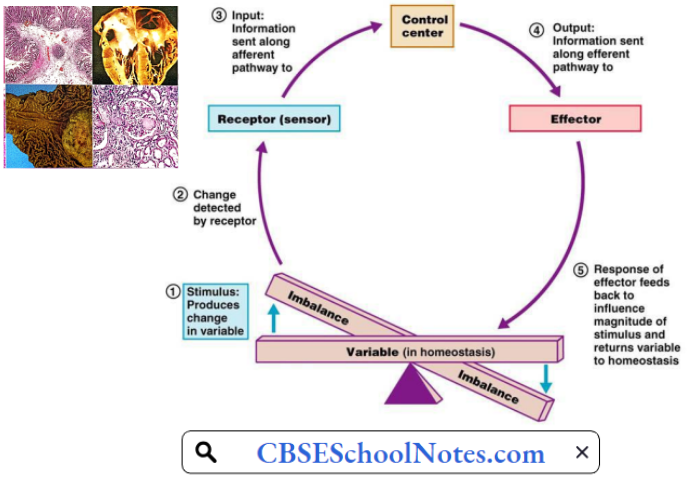
All homeostatic mechanisms have at least three components:
- Receptor that detects a change in the internal environment and sends information to the control center.
- The control center is the structure that evaluates the disturbance and activates the correcting mechanisms.
- The effector is the structure that carries out the corrective responses as directed by the control center.
For example, exposure to cold tends to lower the body temperature. The change in body temperature is detected by cold thermal receptors (receptors). The information is communicated to the temperature-regulating areas of the hypothalamus in the brain (center). The body responds by involuntary contractions of skeletal muscle called shivering (effector).
- Shivering generates heat and prevents a fall in body temperature. Exposure to hot environment tends to raise body temperature. The change in body temperature is detected by warmth thermal receptors (receptors).
- The information is communicated to the temperature-regulating areas of the hypothalamus in the brain (center). The body responds by sweating which results in heat loss by evaporation (effector). This is an example of body temperature homeostasis.
Homeostasis Physiological Control Systems
Our body consists of many organ systems, and each organ system consists of more than one organ. Therefore, central control mechanisms are required so as to allow coordination of activity of different organs of an organ system and coordination between different organ systems. Our body has two major control systems.
- Neural Control: It is chiefly exerted on skeletal muscles and exocrine glands. The response occurs in milliseconds.
- Endocrine Control: It is chiefly exerted on metabolic reactions. The response may take seconds, hours, or even days.
Open-Loop And Closed-Loop Processes (Systems): Physiological processes may be governed by an open-loop system or a closed-loop system. In an open-loop system, the output product (signal) has no control over the process.
The entire process is controlled by the input signals. In a closed-loop control, the product in the system (output signal) has an effect on the input signal. This is called a feedback phenomenon. Feedback control may be a negative feedback or a positive feedback system.
1. Open-Loop System: The presence of food in the intestine results in the secretion of enzymes from the pancreas. however, the concentration of pancreatic enzymes in the intestine has no effect on the secretion of pancreatic acini. This is an example of an open-loop system.

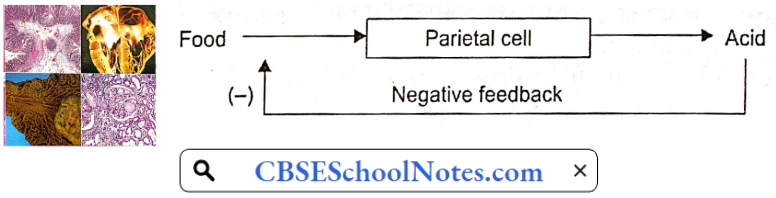
2. Negative Feedback Control: In the negative feedback control system, the output signal has an inhibitory effect on the input signal. For example, ingestion of food results in the secretion of gastric juice that contains hydrochloric acid (secreted by parietal cells of gastric glands).
- Secretion of acid has a negative feedback effect on parietal cells—when the concentration of acid in gastric juice reaches a certain level (pH 2), the acidity has an inhibitory effect on parietal cells and thus further acid secretion stops.
- As a result, gastric acidity cannot increase beyond a certain predetermined degree. Negative feedback control mechanisms are most often used in the maintenance of homeostasis. This system prevents deviations from a given set point.
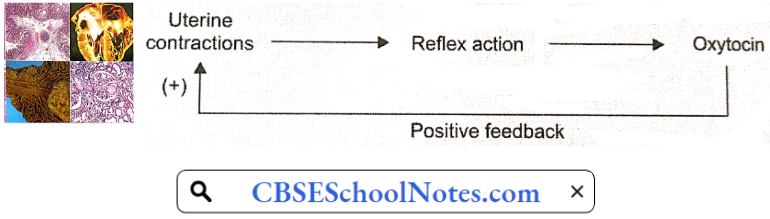
3. Positive Feedback System: In a positive feedback system, the output signal accentuates the input signal. As a result, the output deviates more and more from the initial output. The positive feedback system is not involved in homeostasis. It is used to accelerate or reinforce a reaction.
- For example, during delivery, at about 40 weeks of pregnancy, uterine contractions start that are weak to begin with. Mild uterine contractions cause pressure of the head of the baby on the cervix and dilate it. Dilatation of the cervix reflexly causes the release of the hormone oxytocin by the pituitary gland.
- Oxytocin causes stronger uterine contractions that cause further dilation of the cervix and still greater of oxytocin. In this way, by a positive feedback mechanism, uterine contractions gradually become so strong that the baby is expelled out of the uterus.
4. Feedforward System: This system allows the human body to foresee a change in the environment and prepares the body for the change. The information is sent ahead of time to the control system. The effector system is modified before any change has taken place, i.e. by anticipating change in the environment.
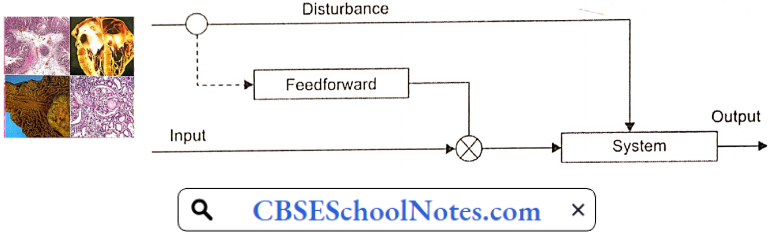
A Feedforward control system is advantageous in fast reactions. For example, during a cricket match, when a fielder tries to catch the ball, he has to anticipate the trajectory of the ball by visual input and run to an appropriate place. In most of the voluntary movements, both feedforward and negative feedback systems operate simultaneously.
Cellular Response To Pathological Stress Or Noxious Stimuli
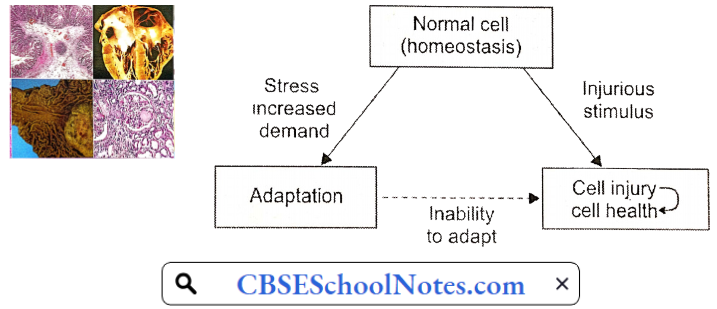
Cells or tissues encounter pathological stresses or stimuli, in the form of hypoxia, ischemia, infections, and physical or chemical insults. The cells can respond to such stimuli by undergoing two fundamental processes:
- Adaptation, modifying themselves to a new steady state and preserving viability and function. The principal adaptive responses are hypertrophy, hyperplasia, atrophy, and metaplasia.
- Cell Injury: If the stressful stimulus exceeds the adaptive capability, cell injury results. Depending on the strength of noxious stimulus, cell injury may be
- Reversible And Subsequently Normal Cellular Function Is Restored, Or
- Irreversible, Resulting In Death Of The Cells Or Tissues
Cellular Adaptations To Stress
Adaptations are reversible changes in the number, size, or metabolic activity of cells in response to changes in their environment.
- Physiologic adaptations usually represent responses of cells to normal stimulation by hormones or endogenous chemical mediators (for example, the hormone-induced enlargement of the breast and uterus during pregnancy).
- Pathologic adaptations are responses to stress that allow cells to modulate their structure and function and thus escape injury. Such adaptations can take several distinct forms, namely hypertrophy, hyperplasia, atrophy, and metaplasia.
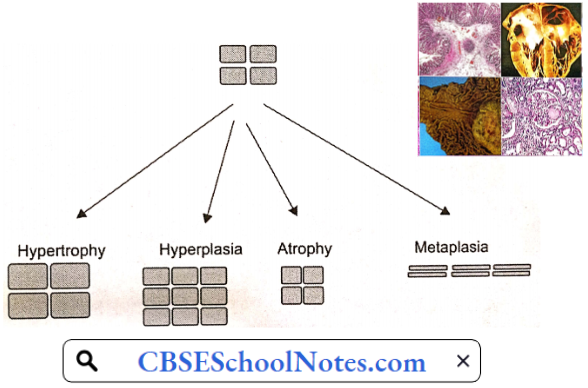
Hypertrophy Heart : Hypertrophy is an increase in the size of cells resulting in increase in the size of the organ. In pure hypertrophy, there are no new cells, just bigger cells containing increased amounts of structural proteins and organelles. Hypertrophy occurs when cells have a limited capacity to divide.
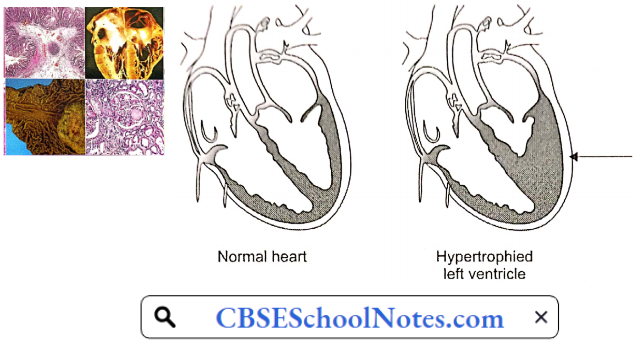
Hypertrophy can be physiologic or pathologic and is caused either by increased functional demand or by growth factor or hormonal stimulation. An example of physiologic hypertrophy is the enlarged muscle of the weightlifter. Thickening of ventricular muscle in response to the narrowing of the outlet valve is an example of pathologic hypertrophy.
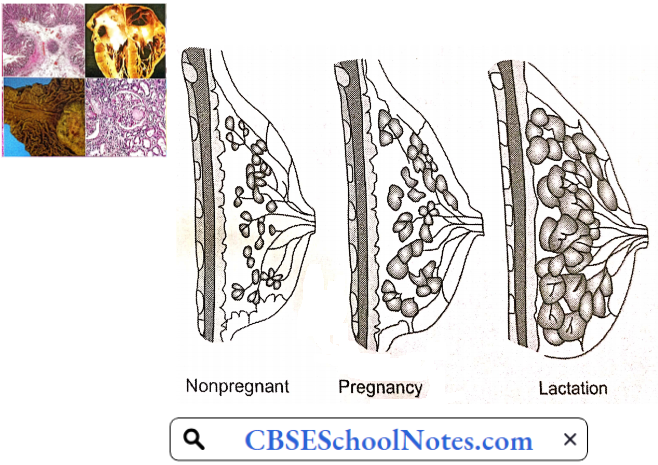
Hyperplasia Uterus : Hyperplasia is characterized by an increase in the size of an organ due to an increase in cell number. It results from a proliferation of tissue cells. Hyperplasia takes place if the tissue contains cell populations capable of replication; it may occur concurrently with hypertrophy and often in response to the same stimuli. Hyperplasia can be physiologic or pathologic.
- An example of physiologic hyperplasia is the enlargement of the mammary gland by the proliferation of the glandular tissue during pregnancy and lactation. Benign prostatic hyperplasia leading to enlargement of the prostate gland is an example of pathological hyperplasia.
- An important point is that in all of these situations, the hyperplastic process remains controlled; if the signals that initiate it disappear, the hyperplasia disappears. It is this responsiveness to normal regulatory control mechanisms that distinguishes pathologic hyperplasia from cancer, in which the growth control mechanisms become dysregulated or ineffective.
- Hypertrophy and hyperplasia can occur simultaneously. The massive physiologic enlargement of the uterus during pregnancy occurs as a consequence of estrogen-stimulated smooth muscle hypertrophy and smooth muscle hyperplasia.
Atrophy: Shrinkage in the size of the cell by the loss of cell substance is known as atrophy. When a sufficient number of cells are involved, the entire tissue or organ diminishes in size, becoming atrophic.
- Although atrophic cells may have diminished function, they are not dead. Causes of atrophy include a decreased workload (for example immobilization of a limb to permit healing of a fracture), loss of innervation, diminished blood supply, inadequate nutrition, loss of endocrine stimulation, and aging (senile atrophy).
- Although some of these stimuli are physiologic (for example the loss of hormone stimulation in menopause) and others pathologic (for example denervation). Cellular atrophy represents a retreat by the cell to a smaller size at which survival is still possible; a new equilibrium is achieved between cell size and diminished blood supply or nutrition.

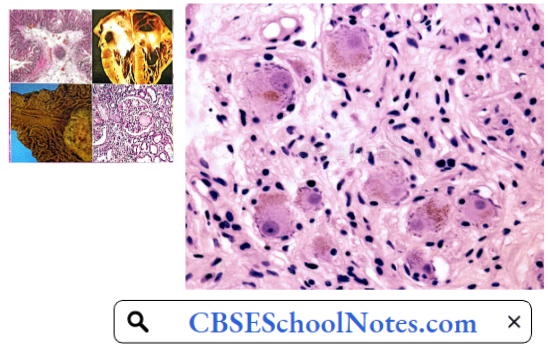
Metaplasia: Metaplasia is a reversible change in which one cell type (epithelial or mesenchymal) is replaced by another cell type. In this type of cellular adaptation, a cell type sensitive to a particular stress is replaced by another cell type that is better able to withstand the adverse environment.
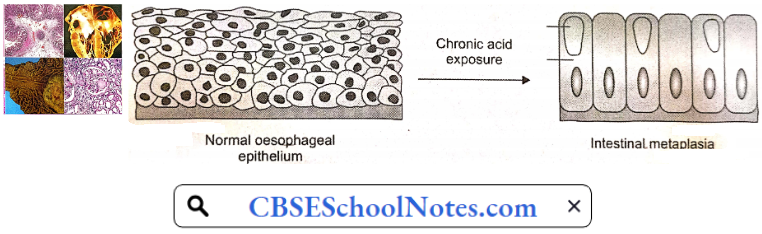
- Epithelial metaplasia is exemplified by the change of normal stratified squamous epithelium of the lower end of the esophagus to the intestinal columnar epithelium in patients of gastro-oesophageal reflux disease (GERD).
- In GERD, weak functioning of the lower oesophageal sphincter leads to the reflux of gastric acid into the esophagus. Chronic acid exposure converts stratified squamous epithelium to columnar epithelium. The columnar epithelium is more resistant to acid.
- Another example is the metaplasia seen in the respiratory mucosa in chronic smokers. In this case the normal delicate ciliated columnar epithelial cells of the trachea and bronchi a tv locally replaced by more rugged stratified squamous epithelial cells. however. the influences that induce metaplastic change, if persistent, may predispose to malignant transformation of the epithelium.
Cell Injury
Cell injury results when cells are stressed so severely that they are no longer able to adapt or when cells are exposed to inherently damaging agents or suffer from intrinsic abnormalities (for example in DNA or proteins). Different injurious stimuli affect many metabolic pathways and cellular organelles. Injury may progress through a reversible stage and culminate in irreversible change, i.e. cell death.
Reversible Cell Injury: In early stages or mild forms of injury, the functional and morphologic changes are reversible if the damaging stimulus is removed. At this stage, although there may be significant structural and functional abnormalities, the injury has typically not progressed to severe membrane damage and nuclear dissolution.
Irreversible Cell Injury (Cell Death): Cell death may occur in the form of
- Necrosis, or
- Apoptosis
- Necrosis: With continuing damage, the injury becomes irreversible, at which time the cell cannot recover and it dies. When damage to membranes is severe, enzymes leak out of lysosomes, enter the cytoplasm, and digest the cell, resulting in necrosis. Cellular contents also leak through the damaged plasma membrane into the extracellular space, where they elicit a host reaction (inflammation).
- Necrosis is the major pathway of cell death in many commonly encountered injuries, such as those resulting from ischemia, exposure to toxins, various infections, and trauma.
- Apoptosis: When a cell is deprived of growth factors, or the cell’s DNA or proteins are damaged beyond repair, the cell kills itself by another type of death, called apoptosis, which is characterized by nuclear dissolution without complete loss of membrane integrity.
- Whereas necrosis is always a pathologic process, apoptosis serves many normal-time ions amt is not necessarily associated with pathologic cell injury.
Furthermore, in keeping with its role in certain physiologic processes, apoptosis does not elicit an inflammatory response.
Histologic Signs Of Reversible Cell Injury
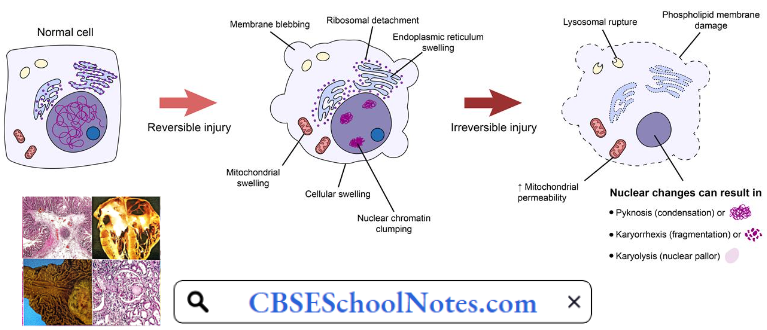
- Cellular Swelling: The first sign of almost all forms of injury to cells, is a reversible alteration called cellular swelling. Microscopic examination may reveal small, clear vacuoles within the cytoplasm; these represent distended and pinched-off segments of the endoplasmic reticulum (ER). This pattern of nonlethal injury is sometimes called vacuolar degeneration. The intracellular changes associated with reversible injury include:
- Plasma membrane alterations such as blunting, or distortion of microvilli, and loosening of intercellular attachments;
- Mitochondrial swelling
- Dilation of the er with detachment of ribosomes and
- Minimal nuclear alterations (clumping of chromatin).
- Cellular swelling is the result of the failure of energy-dependent ion pumps in the plasma membrane, leading to an inability to maintain ionic and fluid homeostasis.
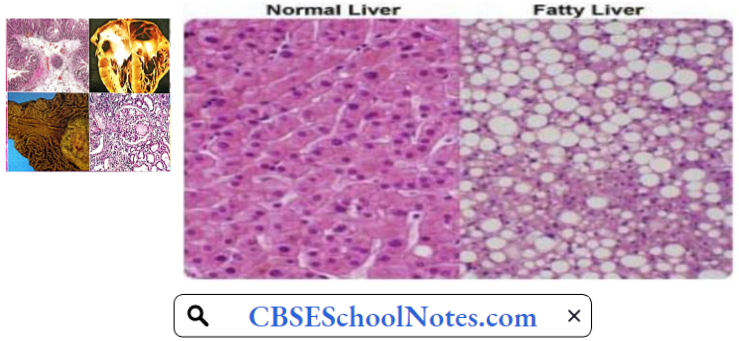
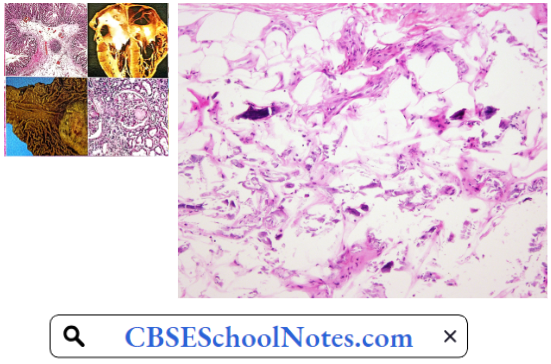
- Fatty Change: Fatty change occurs in hypoxic injury and in various forms of toxic or metabolic injury. It is manifested by the appearance of small or large lipid vacuoles in the cytoplasm. It is principally encountered in cells participating in fat metabolism (for example hepatocytes). Like cellular swelling, fatty change is also the reversible stage of tissue injury.
Histologic Signs Of Necrosis: Necrosis is the type of cell death that is associated with loss of membrane integrity and leakage of cellular contents culminating in the dissolution of cells, largely resulting from the degradative action of enzymes on lethally injured cells.
- The leaked cellular contents often elicit a local host reaction, called inflammation, that attempts to eliminate the dead cells and start the subsequent repair process.
- The enzymes responsible for the digestion of the cell may be derived from the lysosomes of the dying cells themselves and from the lysosomes of leukocytes that are recruited as part of the inflammatory reaction to the dead cells
Necrosis is characterized by changes in the cytoplasm and nuclei of the injured cells
- Cytoplasmic Changes: Increased eosinophilia (deep pink staining in slides stained with H and E). It is attributable in part to the increased binding of eosin to denatured cytoplasmic proteins and in part to the loss of the basophilia that is normally imparted by the ribonucleic acid (RNA) in the cytoplasm.
- Compared with viable cells, the cell may have a more glassy, homogeneous appearance, mostly because of the loss of glycogen particles.
- When enzymes have digested cytoplasmic organelles, the cytoplasm becomes vacuolated and appears “moth-eaten.”
- By electron microscopy, necrotic cells are characterized by discontinuities in plasma and organelle membranes, marked dilation of mitochondria with the appearance of large amorphous densities, and disruption of lysosomes.
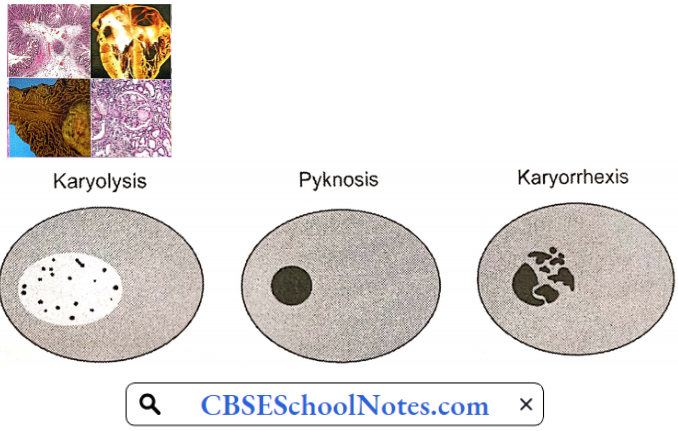
- Nuclear Changes: Nuclear changes assume one of three patterns, all due to the breakdown of DNA and chromatin.
- Karyolysis, in which basophilia of the chromatin may fade presumably secondary to deoxyribonuclease (DNase) activity.
- Pyknosis is characterized by nuclear shrinkage and increased basophilia; the DNA condenses into a solid shrunken mass.
- Karyorrhexis, the pyknotic nucleus undergoes fragmentation.
Fates Of Necrotic Cells
- Necrotic cells may persist for some time or maybe digested by enzymes and disappear.
- Dead cells may be phagocytosed by other cells
- Dead cells ultimately become calcified.
Mechanisms Of Cell Injury: Cell injury results from functional and biochemical abnormalities in one or more of several essential cellular components. The principal targets and biochemical mechanisms of cell injury are
- Mitochondria and their ability to generate ATP and ROS under pathologic conditions
- Disturbance in calcium homeostasis
- Damage to cellular (plasma and lysosomal) membranes
- Damage to DNA.
- ATP Depletion: The major causes of ATP depletion are reduced supply of oxygen and nutrients, as well as mitochondrial damage. ATP is required for virtually all synthetic and degradative processes within the cell, including membrane transport, protein synthesis, lipogenesis, etc. Deficiency of ATP leads to
- Reduced activity of Na-K-ATPase pump resulting in intracellular accumulation of sodium and efflux of potassium. The net gain of solute is accompanied by the gain of water, causing cell swelling and dilation of the endoplasmic reticulum.
- A compensatory increase in anaerobic glycolysis in an attempt to maintain the cell’s energy sources. As a consequence, intracellular glycogen stores are rapidly depleted, and lactic acid accumulates, leading to decreased intracellular pH and decreased activity of many cellular enzymes.
- Influx Of Calcium: Ischaemia and certain toxins cause an increase in cytosolic calcium concentration, initially because of the release of Ca2+ from the intracellular stores, and later resulting from the increased influx of Ca2+ across the plasma membrane due to failure of ATP-dependent Ca2+ pumps. Increased cytosolic Ca2+ activates a number of enzymes, with potentially deleterious cellular effects.
- There is structural disruption of the protein synthetic apparatus, manifested as the detachment of ribosomes from the rough endoplasmic reticulum. Thus, there is a reduction in protein synthesis. Ultimately, there is irreversible damage to mitochondrial and lysosomal membranes, and the cell undergoes necrosis.
- Defects In Membrane Permeability: Increased membrane permeability leading ultimately to overt membrane damage is a consistent feature of most forms of cell injury that culminate in necrosis. The most important sites of membrane damage during cell injury are the mitochondrial membrane, the plasma membrane, and the membranes of lysosomes.
- Mitochondrial membrane damage. Damage to mitochondrial membranes leads to a further reduction in the production of ATP culminating in necrosis.
- Plasma membrane damage. Plasma membrane damage leads to loss of osmotic balance and influx of fluids and ions, as well as loss of cellular contents.
- Injury to lysosomal membranes results in leakage of their enzymes into the cytoplasm and activation of the acid hydrolases in the acidic intracellular pH of the injured (for example ischaemic) cell. Lysosomes contain ribonucleases (RNAses), DNAses, proteases, glucosidases, and other enzymes. Activation of these enzymes leads to enzymatic digestion of cell components, and the cells die by necrosis.
- Damage To DNA: Cells have mechanisms that repair damage to DNA, but if this damage is too severe to be corrected, the cell initiates its suicide program and dies by apoptosis.
Apoptosis Pathway
Apoptosis is a pathway of cell death in which cells activate enzymes that degrade the cells’ own nuclear DNA and nuclear and cytoplasmic proteins. Fragments of the apoptotic cells then break off, giving the appearance that is responsible for the name (apoptosis, “falling off”). The plasma membrane of the apoptotic cell remains intact, but the membrane is altered in such a way that the cell and its fragments become targets for phagocytes.
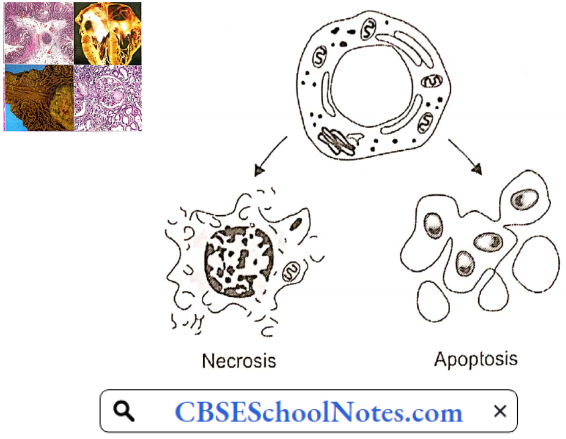
The dead cell and its fragments are rapidly cleared before cellular contents have leaked out, so apoptotic cell death does not elicit an inflammatory reaction in the host. Apoptosis differs in this respect from necrosis, which is characterized by loss of membrane integrity, enzymatic digestion of cells, leakage of cellular contents, and frequently a host reaction. However, apoptosis and necrosis sometimes coexist, and apoptosis induced by some pathologic stimuli may progress to necrosis.
Causes Of Apoptosis: Apoptosis occurs in many normal situations and serves to eliminate potentially harmful cells and cells that have outlived their usefulness. It also occurs as a pathologic event when cells are damaged beyond repair, especially when the damage affects the cell’s DNA; in these situations, the irreparably damaged cell is eliminated by apoptosis.
Physiological Apoptosis
- Involution of hormone-dependent tissues upon hormone deprivation, such as endometrial cell breakdown during the menstrual cycle, and regression of the lactating breast after weaning.
- Cell loss in proliferating cell populations, such as intestinal crypt epithelia, in order to maintain a constant number.
- Elimination of cells that have served their useful purpose, such as neutrophils in an acute inflammatory response.
Pathologic Apoptosis
- Damaged DNA
- Apoptosis eliminates cells that are genetically altered or injured beyond repair and does so without eliciting a severe host reaction, thereby keeping the extent of tissue damage to a minimum. Death by apoptosis is responsible for the loss of cells in a variety of pathologic states that damage the DNA of cells.
- Cell injury in certain infections, particularly viral infections, in which loss of infected cells is largely due to apoptotic death that may be induced by the virus.
Intracellular Accumulations
Intracellular accumulations of various substances and extracellular deposition of calcium, both of which are often associated with cell injury.
Fat: fatty change refers to any abnormal accumulation of triglycerides within parenchymal cells. It is most often seen in the liver since this is the major organ involved in fat metabolism, but it may also occur in the heart, skeletal muscle, kidney, and other organs.
Steatosis may be caused by toxins, protein malnutrition, diabetes mellitus, obesity, or anoxia. Alcohol abuse and diabetes associated with obesity are the most common causes of fatty change in the liver (fatty liver).
Cholesterol And Cholesteryl Esters: Cellular cholesterol metabolism is tightly regulated to ensure normal cell membrane synthesis without significant intracellular accumulation. However; phagocytic cells may become overloaded with lipids (triglycerides, cholesterol, and cholesteryl esters) in several different pathologic processes. Of these, atherosclerosis is the most important.
Glycogen: Excessive intracellular deposits of glycogen are associated with abnormalities in the metabolism of either glucose or glycogen. In poorly controlled diabetes mellitus, the prime example of abnormal glucose metabolism, is glycogen accumulates in renal tubular epithelium, cardiac myocytes, and p cells of the islets of Langerhans.
Lipofuscin: It is an insoluble brownish-yellow granular intracellular material that accumulates in a variety of tissues (particularly the heart, liver, and brain) as a result of age or atrophy.
Calcium: Pathologic calcification is a common process in a wide variety of disease states; it implies the abnormal deposition of calcium salts. When the deposition occurs in dead or dying tissues, it is called dystrophic calcification; it occurs in the absence of derangements in calcium metabolism, i.e. with normal serum levels of calcium. In contrast, the deposition of calcium salts in normal tissues is known as metastatic calcification and is almost always secondary to hypercalcemia.

Acidosis And Alkalosis
The Concept Of pH: An acid is a chemical species that can donate a proton (H+), and a base is a species that can accept (gain) a proton. Pure water undergoes an extremely small degree of dissociation to yield H+ and OH–.
H2O ⇔ H+ + OH–
The concentration of H+ in water is 10-7 mEq/L. Water is regarded as neutral. Acids are solutions with H+ concentration greater than 10-7 (for example 10-6 or 10-5 mEq/L). Alkalis or bases are solutions with H+ concentration less than 10-7 (for example 10-8 or 10-9 mEq/L). Expression of H+ concentration in the body fluids as described above is cumbersome; hence a symbol pH came to be used:
- Thus pH of pure water is written as 7. The arterial blood has an average pH of 7.4 (normal range 7.35-7.45). A decrease in arterial pH value below 7.35 is known as acidosis, whereas the term alkalosis is used to describe arterial pH values higher than 7.45.
- Arterial pH values below 6.8 or above 8 are not compatible with life. In fact, arterial pH is maintained within a narrow range, transiently with the help of acid-base buffers in the body fluids, and finally by the kidneys and the lungs.
Regulation Of Hydrogen Ion Balance
- Buffer systems response—very rapid (in seconds), incomplete
- Respiratory responses—rapid (in minutes), incomplete
- Renal responses—slow (in hours to days), complete
Under normal circumstances, tremendous amounts of hydrogen ions (H+) are continuously added to the body fluids. Carbon dioxide accounts for the addition of over 12,000 mEq H+ per day. Nonvolatile (fixed) acids account for another 60 mEq/ day.
- Almost all the CO2 is excreted by the lungs, whereas the kidney is responsible for the excretion of non-volatile acid products of protein metabolism. Lactic acid produced during severe exercise or keto acids produced in severe diabetes is also excreted by the kidney.
- Fruits are the main dietary source of the alkali. They contain sodium and potassium salts of weak organic acids, whose metabolism produces NaHCO3 or KHCO3 (and CO2). Normally, the alkali content of the diet is very small and all the normal individuals excrete acidic urine except for transient post-prandial alkaline tide.
Role Of Respiration: In response to changes in blood pH, respiratory responses occur within minutes by stimulation/depression of respiratory centers in the CNS.
In spite of the addition of 12,000 mEq H+ per day to the blood, the pH of arterial blood remains remarkably constant at 7.4. Similarly, pCO2 of the arterial blood is kept constant at 40 mm Hg. This is made possible by two factors:
- In the venous blood, CO2 is converted to H2CO3 and further to H+ and HCO–3. Hydrogen ions are immediately buffered by the blood buffers, chiefly hemoglobin and plasma proteins.
- As the venous blood passes through the lungs, CO2 is regenerated by reversal of the reactions mentioned above 1 and excreted very efficiently. Pulmonary ventilation is so delicately adjusted that it exactly matches the CO2 produced in the body.
- Even during severe exercise, when CO2 production increases 20-fold, CO2 excretion is so efficient that arterial pCO2 does not increase at all. Such a delicate control is made possible by the fact that ventilation is controlled by both CO2 as well as H+ concentration through central and peripheral chemoreceptors.
- Effect Of CO2: CO2 is a highly diffusible gas. It can easily cross the blood-brain and blood-CSF barriers, and stimulate the medullary central chemoreceptors. In contrast, H+ cannot cross these barriers easily. Therefore, central chemoreceptors are most sensitive to changes in arterial pCO2 and less so to changes in H+ concentration.
- Effect Of pH: An increase in H+ concentration of arterial blood also stimulates pulmonary ventilation, chiefly through the peripheral (sino-aortic) chemoreceptors. Therefore, the respiratory system helps in the regulation of the acid-base balance of the body even when the increase in H+ concentration is not due to CO2 but due to non-volatile acids like sulphuric acid, phosphoric acid, or lactic acid.
Role Of Kidneys: The kidneys regulate pH by either acidification or alkalinization of the urine. The renal response occurs over hours/days and is capable of nearly complete restoration of acid-base balance. As mentioned above, about 60 mEq of H+ is added to the blood every day as nonvolatile acids.
- They cannot be excreted by the lungs. They are excreted by the kidneys in an indirect manner. In the kidneys, most of the excretory products are initially filtered into the glomerular filtrate. All that is necessary for their excretion is that renal tubules reabsorb them partially or not all.
- In contrast, the concentration of H+ in the blood is so small, that they cannot be excreted in this manner. Actually, most of the H+ produced in the body does not remain as such. They are immediately buffered by HCO3– and other buffers. The kidney generates new hydrogen ions equivalent to the amount metabolically produced and actively secretes them into the urinary tubules, where they are buffered by phosphate and ammonium ions.
- The generation of H+ in the renal tubules is accompanied by the production of HCO3– which diffuses into the blood circulation and replenishes the amount of HCO3– lost during the initial buffering of the acids. In case an excess of base (NaHCO3) is ingested, it is excreted by the kidney by filtration followed by partial or complete non-reabsorption.
- In primary pulmonary diseases such as emphysema, pulmonary excretion of CO2 is diminished, and therefore arterial pCO2 and H+ concentrations tend to rise (respiratory acidosis). In such circumstances, renal excretion of H+ is the only means of maintaining body pH near normal (renal compensation).
- Similarly in chronic renal failure, renal excretion of H+ is diminished leading to metabolic acidosis. In such a condition, excessive loss of CO2 by hyperventilation is the only means of maintaining body pH near normal (respiratory compensation).
Anion Gap Concept: In the plasma, total cations (Na+, K+, Ca++, Mg++, etc.) are always counterbalanced by total anions (Cl–, HCO3–, PO4–, SO4–, etc). Of these ions, only Na+, K+, Cl–, and HCO3– are routinely measured. Therefore, the concentration of measured anions is always less than the concentration of measured cations. The difference is known as the anion gap
Anion gap = {[Na3] + [K3]} – {[Cl–] + [HCO3–] )
Anion Gap Example: Anion gap = {140 mEq/L + 4 mEq/L } – {100 mEq/L + 28 mEq/L} = 16 mEq/L
- The anion gap concept is useful in the differential diagnosis of metabolic acidosis. In one group of disorders producing metabolic acidosis, the anion gap becomes larger than normal. Such disorders are said to produce high anion gap metabolic acidosis.
- In the other group of disorders, the anion gap remains normal. Such disorders are said to produce normal attire gap metabolic acidosis. Estimation of the anion gap is also a useful tool to assess mixed acid-base disorders.
In clinical practice, since K+ concentration does not vary grossly, the anion gap is usually calculated as follows:
Anion gap = [Na+] – { [Cl–] + [HCO3–,] }
Calculated in this way, the normal anion gap is 12 ± 4 mEq/L.
Pathophysiology Of Acid Base Disorders
1. Metabolic Acidosis (Ma): The primary abnormality in metabolic acidosis is a decline in plasma HCO3– concentration. This metabolic abnormality may arise because of:
- Increased H+ load on the body in the form of lactic acidosis, ketoacidosis, or ammonium chloride administration.
- Deficient renal H+ excretion.
- Loss of HCO3– from GI tract or kidneys.
Metabolic Acidosis May Be Classified Into Two Major Groups:
- High anion gap MA and
- Normal anion gap (hyperchloraemic) MA.
High Anion Gap MA: There are three prominent causes of high anion gap MA:
- Lactacidosis
- Circulatory shock
- Severe hypoxia
- Ketoacidosis
- Diabetic ketoacidosis
- Alcoholic ketoacidosis
- Starvation
- Renal failure
- Acute or chronic
In the uncompensated stage of such MA, the acid-base picture is:
Acidosis stimulates central and peripheral chemoreceptors causing hyperventilation (respiratory compensation). The renal compensation consists of the excretion of highly acidic urine (↑H+ excretion). Renal compensation is not possible if MA is due to renal failure.
The respiratory compensation decreases the arterial pCO2, whereas renal compensation generates HCO3–, (a side effect of H+ secretion), which partially restores the depleted HCO3–. The acid-base status of a case of compensated MA is as follows:
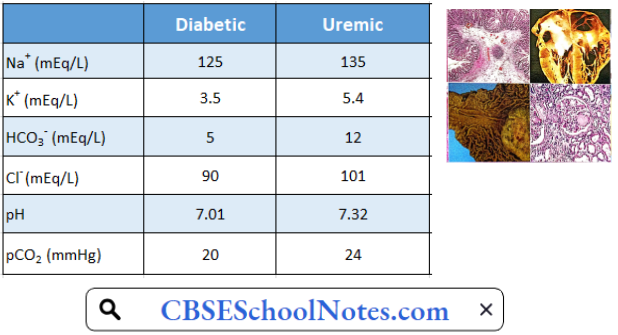
The two most important causes of high anion gap MA in clinical practice are diabetic ketoacidosis and renal failure. The two disorders can be differentiated by the study of serum K+ level, which is elevated in renal failure and subnormal in diabetic ketoacidosis. A typical pattern of acid-base status and electrolyte status of patients of these two types of disorders is given below:
Normal Anion Gap (Hyperchloremic) MA
- Diarrhea
- Renal tubular acidosis
High anion gap MA is characterized by a decrease in plasma HCO3– level, but no significant change in plasma Cl– level. In the hyperchloraemic type of MA, a decrease in plasma HCO3– is accompanied by a significant increase in plasma Cl– hence the name hyperchloraemic.
This type of MA is typically seen in patients suffering from diarrhea or renal tubular acidosis (RTA). In diarrhea, HCO3– is lost from the gut in exchange for Cl–. In RTA, the failure of bicarbonate reabsorption from the renal tubules results in greater reabsorption of Cl–. In either case, the plasma Cl– level is significantly elevated. A typical pattern of acid-base status and electrolyte pattern in the case of RTA is given below
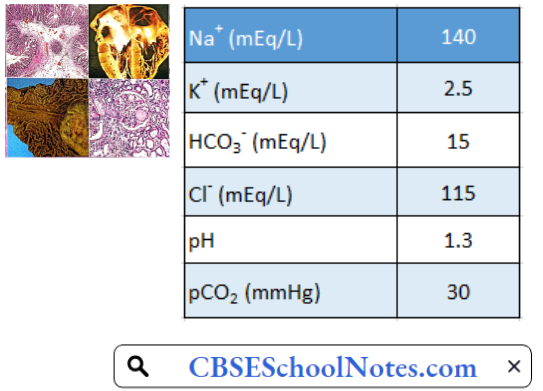
The anion gap in the three cases with MA given above is calculated below:
Anion gap = [Na+] – [(Cl–) 4-(HCO3–)]
Diabetic: 125 – [90 + 5] = 30 mEq/L (high anion gap)
Uremic: 135 – [101 + 12] = 22 mEq/L (high anion gap)
RTA: 140 – 1115 + 15] = 10 mEq/L (normal anion gap)
2. Metabolic Alkalosis
- Excessive sodium bicarbonate ingestion
- Persistent vomiting
Metabolic alkalosis occurs as a result of net gain of bicarbonate (for example ingestion of NaHCO3 for peptic ulcer) or more often due to loss of non-volatile acids (for example HCl in prolonged vomiting). The primary acid-base picture in the uncompensated stage is as follows:
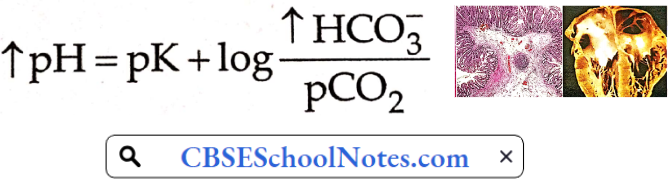
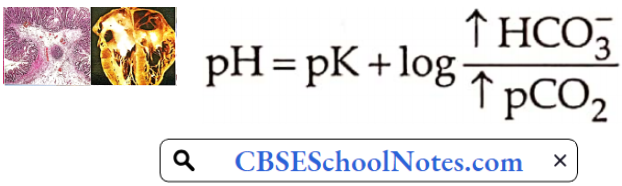
For metabolic alkalosis, there is respiratory as well as renal compensation. Alkalosis inhibits the peripheral chemoreceptors, resulting in hypoventilation and elevation of pCO2 In the kidney, metabolic alkalosis results in decreased secretion of H+ by the renal tubules. Hence filtered bicarbonate is not completely absorbed.
The urinary losses of bicarbonate decrease the extent of elevation of plasma bicarbonate. Hence the change in pH of blood is minimized. The acid-base status of a case of compensated metabolic alkalosis is as follows:
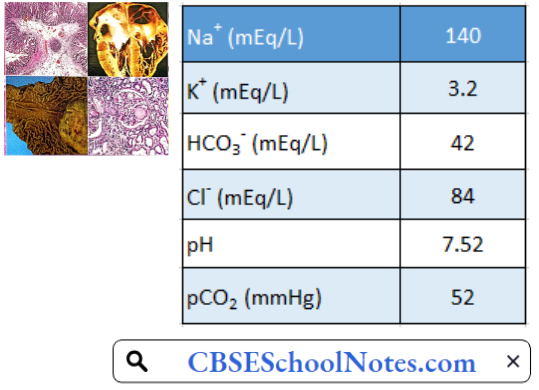
Metabolic alkalosis due to persistent vomiting is accompanied by not only the loss of acid but also fluid from the stomach. The resulting hypovolemia becomes a strong stimulus for sodium reabsorption in the kidneys through Na+ -K+ as well as Na+-H– antiport systems.
Therefore, when metabolic alkalosis is accompanied by hypovolemia, the renal response tends to aggravate alkalosis rather than correct it. It leads to hypokalemia as well. A fairly typical pattern of acid-base status and electrolytes in a patient with persistent vomiting is given below:
3. Respiratory Acidosis: The primary abnormality in respiratory acidosis is the elevation of PaCO2 due to alveolar hypoventilation. Alveolar hypoventilation also reduces PaO2. Therefore, hypoxemia always accompanies hypercapnia.
Acute respiratory acidosis is defined as hypercapnia developed in the time prior to renal compensation, i.e. less than 24 hours. In acute respiratory acidosis, the acid-base status is as follows:
Acute Respiratory Acidosis May Be Caused By:
- Acute airway obstruction (severe asthma)
- Central respiratory drive depression
- Dings: Narcotics, benzodiazepines, barbiturates
- Neurologic Disorders: Encephalitis, brainstem disease, trauma, poliomyelitis.
Chronic respiratory acidosis is most commonly present in
- Chronic obstructive pulmonary disease
- Emphysema
- Chronic bronchitis
- Chest wall deformities
- Kyphoscoliosis
The renal compensation involves ↑H+ excretion, as well as increased generation of HCO3– The resultant increase in plasma bicarbonate concentration partially restores the blood pH towards normal:
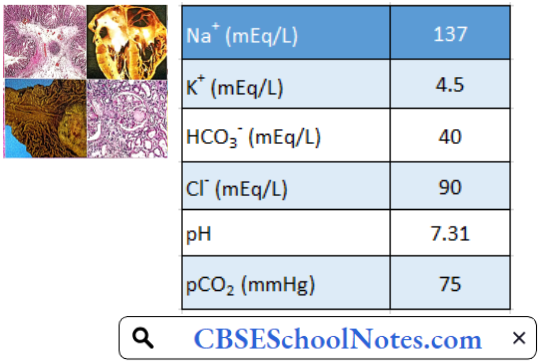
Renal compensation results in the elevation of plasma HCO3– by 3.5 mEq/L for every 10 mmHg increase in pCO2 A fairly typical pattern of acid-base and electrolyte status of a patient with chronic respiratory acidosis is given below:
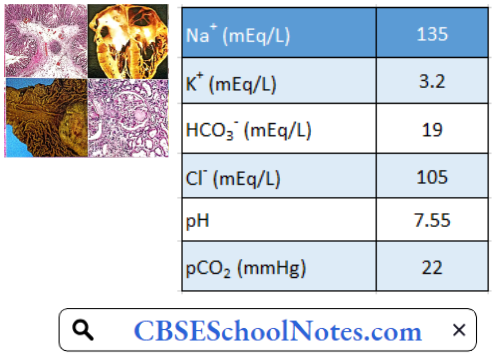
4. Respiratory Alkalosis: Respiratory alkalosis is the most common acid-base disorder in a critically ill patient. It is primarily caused by alveolar hyperventilation leading to decreased paCO2.
Hypoxia due to acute pulmonary disease (for example pneumonia) or chronic pulmonary disease, sepsis, and psychogenic hyperventilation are common causes of respiratory alkalosis.
Renal compensation to decreased arterial pCO2 is decreased renal secretion of H+.
Consequently, bicarbonate is not generated in the kidneys. More importantly, even the filtered bicarbonate is not fully reabsorbed. Hence plasma HCO3– falls markedly which minimizes the change in blood pH:
A fairly typical pattern of acid-base and electrolytes in a patient with respiratory alkalosis is given below
Electrolyte Imbalance
Electrolyte Imbalance is an abnormality in the concentration of electrolytes in the body. Electrolytes play a vital role in maintaining homeostasis within the body. They help to regulate heart and neurological function, fluid balance, oxygen delivery, acid-base balance and much more.
Electrolyte imbalances can develop by consuming too little or too much electrolyte as well as excreting too little or too much electrolyte. The most serious electrolyte disturbances involve abnormalities in the levels of sodium, potassium or calcium.
1. Sodium
- Hypernatraemia: Hypernatraemia means that the concentration of sodium in the blood is too high. An individual is considered to have high sodium at levels above 145 mEq/L of sodium.
- Hypernatraemia Causes
- Inadequate water consumption
- Severe dehydration
- Excessive loss of bodily fluids as a result of prolonged vomiting, diarrhea, sweating, or respiratory illness
- Certain medications, such as diuretics and corticosteroids
- Hypernatraemia Symptoms
- Dehydration
- Nausea
- Vomiting
- Fatigue
- Weakness
- Increases thirst
- Hypernatraemia Causes
- Hyponatremia: Hyponatremia is defined as a concentration lower than 135 mEq/L.
- Hyponatremia Causes
- Excessive fluid loss through the skin from sweating or burns
- Vomiting or diarrhoea
- Overhydration
- Congestive heart, or kidney failure
- Certain medications, including diuretics
- Syndrome of inappropriate secretion of antidiuretic hormone (SIADH)
- Hyponatremia Symptom: The severity of symptoms is directly correlated with the severity of hyponatremia and rapidness of onset.
- Loss of appetite
- Agitation
- Nausea
- Weakness
- Vomiting
- Seizures, coma, and death
- Confusion
- Hyponatremia Causes
2. Potassium
- Hyperkalaemia: Hyperkalaemia means the concentration of potassium in the blood is >5 mEq/L.
- Hyperkalemia Causes:
- Kidney failure
- Severe acidosis, including diabetic ketoacidosis
- Certain medications, including some blood pressure medications and diuretics
- Adrenal insufficiency
- Hyperkalaemia Symptoms
- Nausea
- Vomiting
- Diarrhea
- Muscle cramps
- Numbness
- Tingling
- Absence of reflexes
- Paralysis
- Cardiac arrhythmias can result in death.
- Hyperkalemia Causes:
- Hypokalaemia: Hypokalaemia is defined as the plasma concentration of potassium is <3.5 mEq/L.
- Hypokalaemia Causes
- Severe vomiting or diarrhea
- Dehydration
- Certain medications, including laxatives, diuretics, and corticosteroids
- Hypokalaemia Symptoms
- Muscle weakness
- Cramping
- Cardiac arrhythmias
- Hypokalaemia Causes
3. Calcium
- Hypercalcaemia: Hypercalcaemia is when plasma calcium concentration is above 10.5 mEq/dL.
- Hypercalcemia Causes
- Hyperparathyroidism
- Malignancy
- Hyperthyroidism
- Hypercalcaemia Symptoms
- Abdominal pain
- Constipation
- Kidney stones
- Hypercalcemia Causes
- Hypocalcaemia: Hypocalcaemia is defined as a plasma calcium level less than 9 mg/dL ‘
- Hypercalcemia Causes
- Vitamin D deficiency
- Hypoparathyroidism
- Multiple blood transfusions
- Hypercalcaemia Symptoms
- Muscle cramping or twitching
- Numbness around the mouth and fingers
- Arrhythmias
- Hypercalcemia Causes