Cranial Nerves Nuclei And Functional Aspects
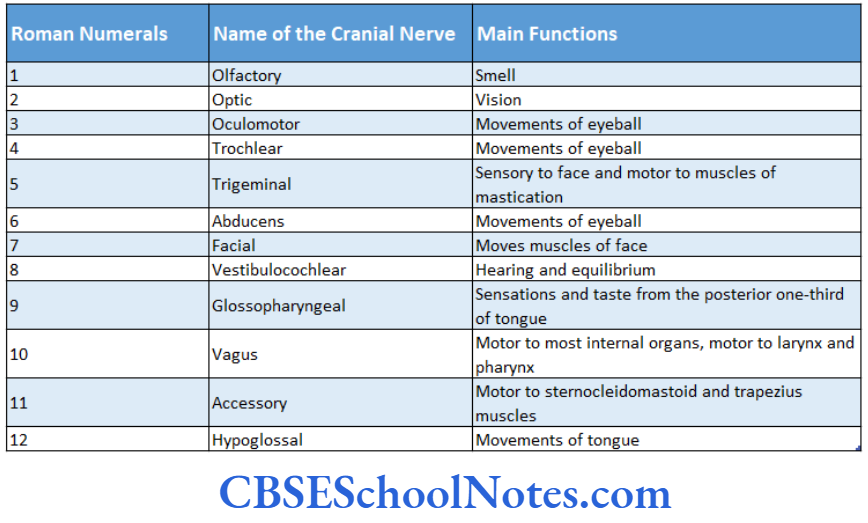
Cranial nerves, like spinal nerves, are a part of the peripheral nervous system (PNS). 12 pairs of cranial nerves are attached to the ventral surface of the brain (except the trochlear nerve which is attached to the dorsal surface of the brain). The first two cranial nerves olfactory and optic, are attached to the forebrain.
While The Rest Of The Cranial nerves are attached to the brainstem. The Cranial nerves are usually designated by Roman numerals.
Cranial nerves 1 and 2 are pure secondary nerves while other nerves are mixed. thus a cranial nerve may contain fibers that take origin from various functional types of nuclei located in the brainstem, i.e. somatic motor, visceral motor, somatic sensory, and j visceral sensory.
Read and Learn More Neuroanatomy
Cranial Nerves Nuclei Developmental Aspects
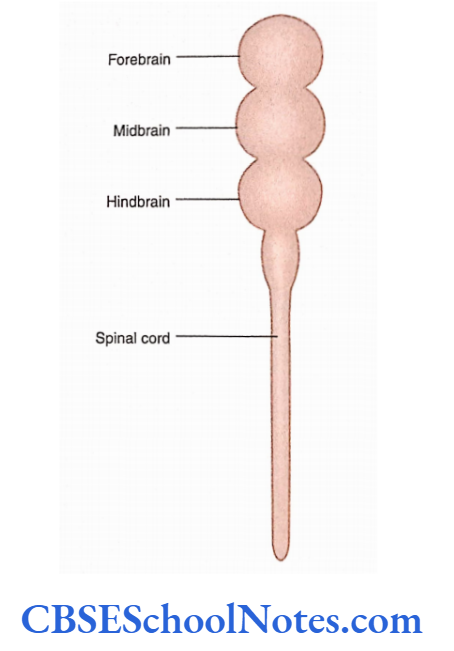
Before discussing the functional columns in the brainstem it is important to understand the development of the brainstem. Tire brainstem and the spinal cord develop from the neural tube that appears in the embryo
Development Of Functional Columns In Spinal Cord And Brainstem
The events that take place during the development of the spinal cord and brainstem are depicted respectively. Students are suggested to read the description of these diagrams carefully before proceeding to learn the following text.
Arrangement of Nuclear Columns
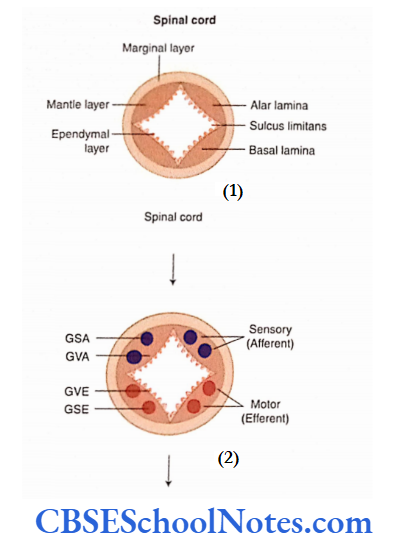
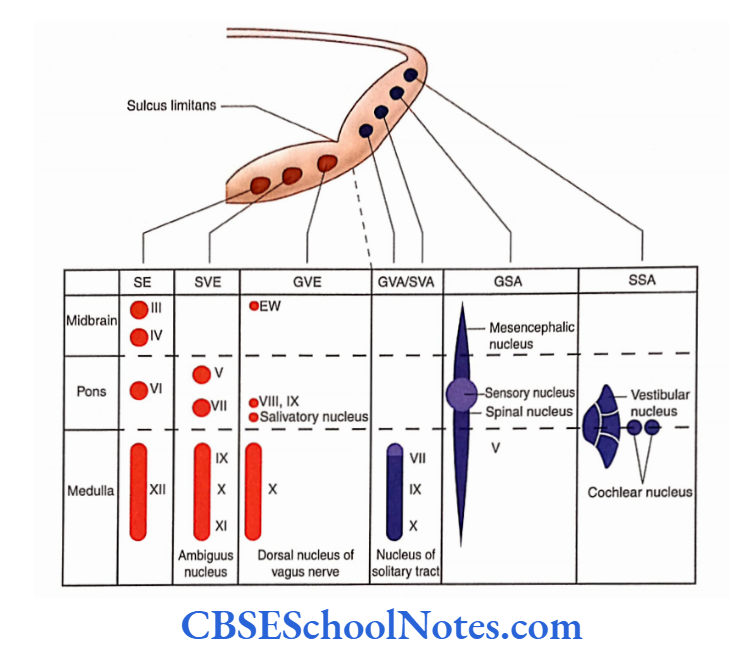
The nuclear aggregates or columns of basal and alar laminae are arranged functionally in a definite sequence when traced from the medial to the lateral side.
In the spinal cord, these include the following
1. Nuclear columns of basal lamina
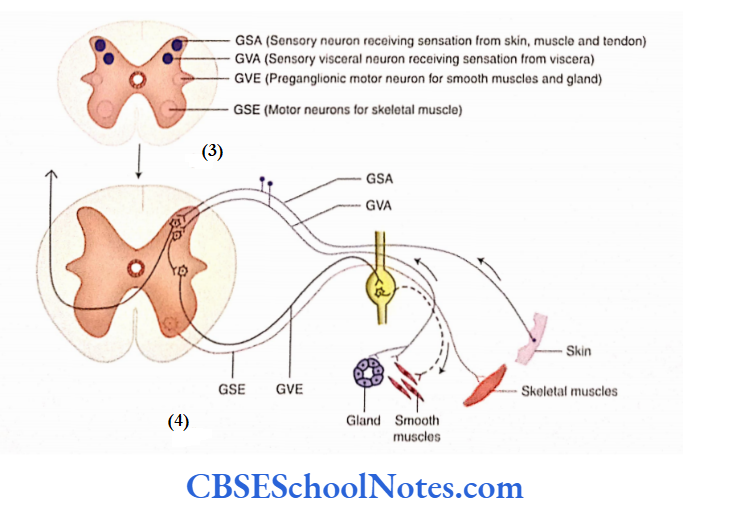
- General somatic efferent (GSE)
- General visceral efferent (GVE)
2. Nuclear columns of alar lamina
- General visceral afferent (GVA)
- General somatic afferent (GSA)
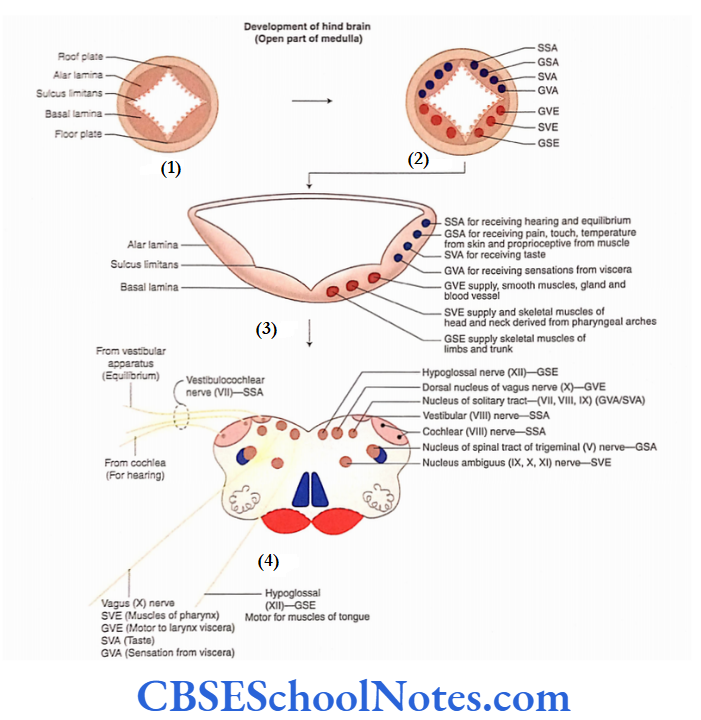
However, in the brainstem, two more special sensory columns are added in the alar lamina (SSA and SVA).
Similarly, one more special visceral efferent column (SVIv) is added to the basal lamina.
Cranial Nerve Nuclei In Brainstem Hindbrain
The functional components of cranial nerve nuclei are
Somatic Efferent Column
- The somatic efferent (SE) column consists of motor nuclei of the cranial nerves 3, 4, 6, and 7.
- The nuclei of this column supply the skeletal muscles derived from somites.
- The nuclei of the cranial nerves 3, 4, and 6 nerves innervate muscles responsible for the movements of the eyeball.
- The nucleus of the cranial nerve 7 innervates the muscles of the tongue.
Special Visceral Efferent Column
- This column includes also the motor nucleus nuclei ambiguus of the cranial (for, nerves and cranial nerves).
- These nuclei innervate skeletal muscles derived from the pharyngeal or branchial arches (branchiomotor).
- These branchiomotor skeletal muscles of the head and neck (muscles of the face, muscles of mastication, muscles of palate, pharynx, and larynx) are also known as special visceral muscles.
General Visceral Efferent Column
- The GVE column consists of parasympathetic motor nuclei, i.e. Edinger-Westphal nucleus, superior and inferior salivatory nuclei, and dorsal nucleus of the vagus.
- The axons from these nuclei innervate the smooth muscles of the viscera, blood vessels, and exocrine glands.
- These nuclei consist of preganglionic nerve cells whose axons terminate in the ganglia closely related to viscera.
- The postganglionic fibers from these ganglia arise and supply the smooth muscles of organs and glands.
General Visceral Afferent and Special Visceral Afferent Columns
- It is believed that both of these sensory columns have a single nucleus which is known as the ‘nucleus of the temporal tract’.
- It receives general visceral sensations from the pharynx, larynx, trachea, esophagus, and thoracic and abdominal viscera.
- It also receives the sensation of taste, a special sensation, from the tongue, epiglottis, and palate.
- This column receives sensory fibres from 7, 9, and 10 cranial nerves.
General Somatic Afferent Column
This column consists of three sensory nuclei of the 5 cranial nerves:
- The main sensory nucleus,
- Spinal nucleus and
- The mesencephalic nucleus of the trigeminal nerve.
- The main sensory and spinal nuclei are concerned with exteroceptive sensations (pain, touch, and temperature) from the region of the face.
- The mesencephalic nucleus receives proprioceptive impulses from the muscles of mastication, facial muscles, ocular muscles, and muscles of the tongue.
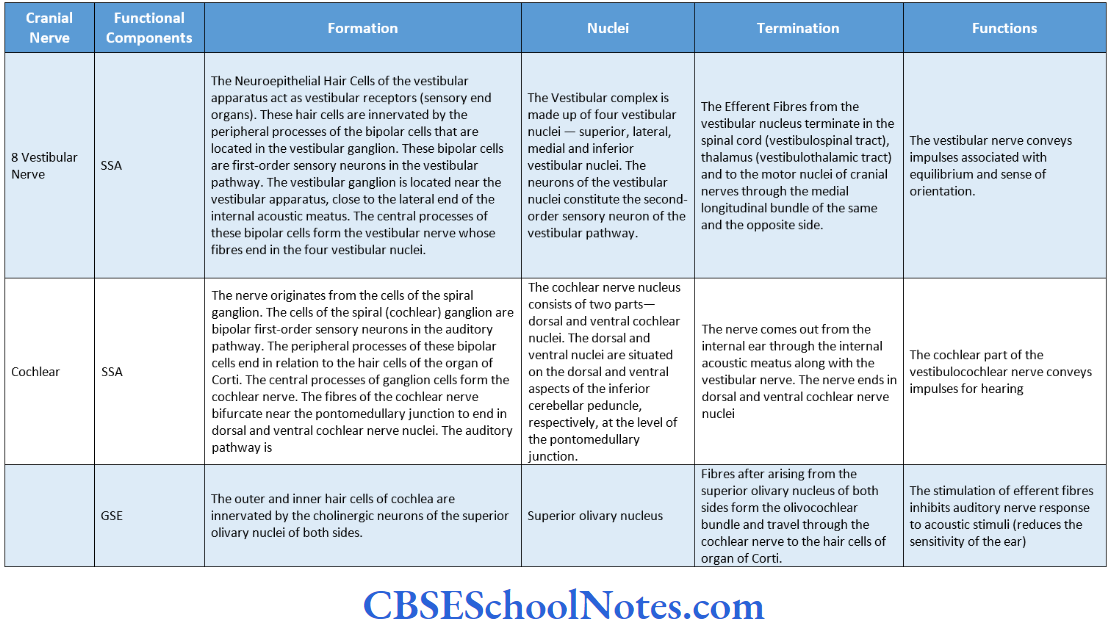
Special Somatic Afferent Column
- The special somatic afferent column consists of sensory nuclei:
- Vestibular and Cochlear.
- The vestibular nuclei convey impulses associated with equilibrium while the cochlear nuclei convey impulses for hearing.
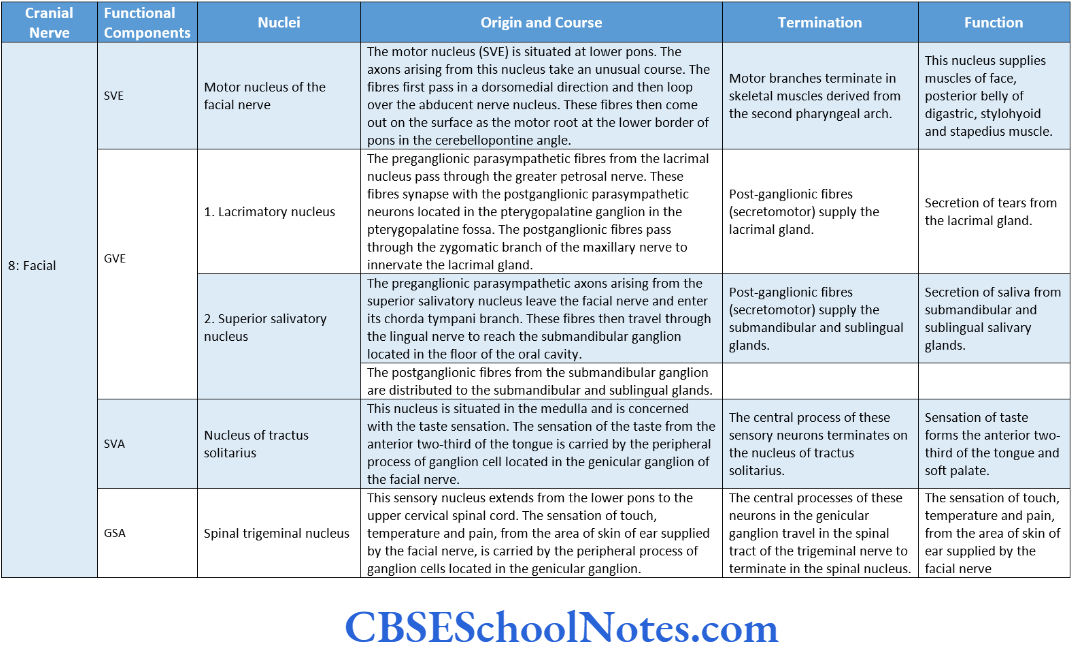
Functional Components, Nuclei, Origin, Course, And Termination Of Cranial Nerves
- Students should note that a detailed description of intracranial and extracranial course and termination of an individual cranial nerve is out of the scope of this book.
- Therefore, only a brief description of the termination of cranial nerves is given here.
- Students should read the detailed description of the course and termination of these cranial nerves from a textbook on the gross anatomy of the Head and Neck.
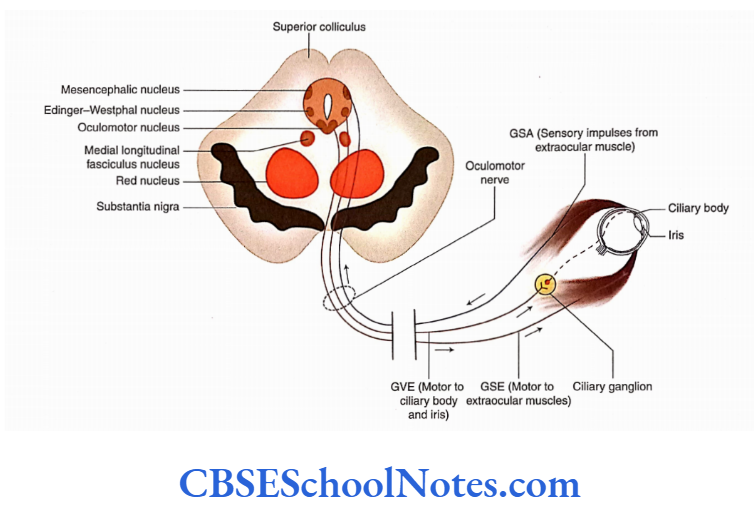
Oculomotor Nerve
The oculomotor nerve is the third cranial nerve. It is predominantly a motor nerve that innervates the majority of extraocular muscles.
These include the superior rectus, inferior rectus, medial rectus, inferior oblique and levator palpebrae superioris.
Origin, Course, and Termination
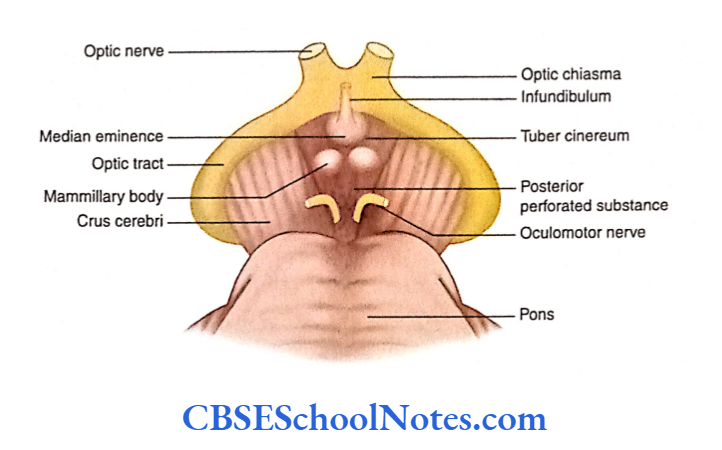
- The oculomotor nerve emerges out on the medial aspect of the cerebral peduncle, in the interpeduncular fossa.
- Thereafter, the nerve passes through the cavernous sinus and the superior orbital fissure.
- The oculomotor nerve then enters the orbit (after passing through the superior orbital fissure) and supplies all the extraocular muscles except the lateral rectus and superior oblique.
- The main oculomotor nerve nucleus is located in the midbrain at the level of superior colliculus The oculomotor nerve has three functional components.
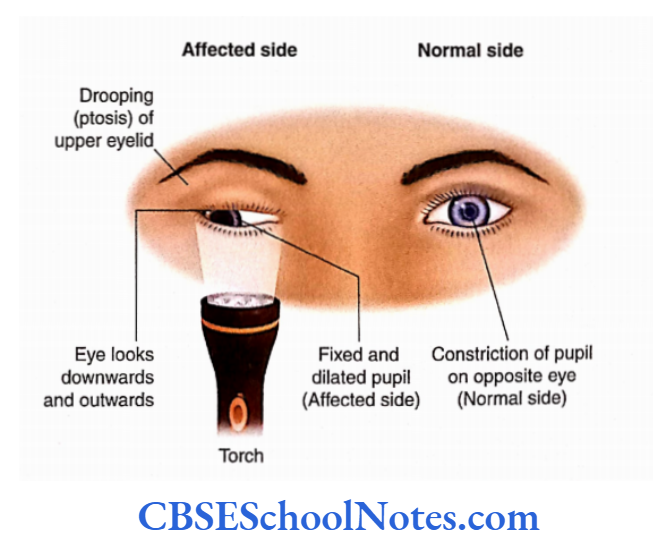
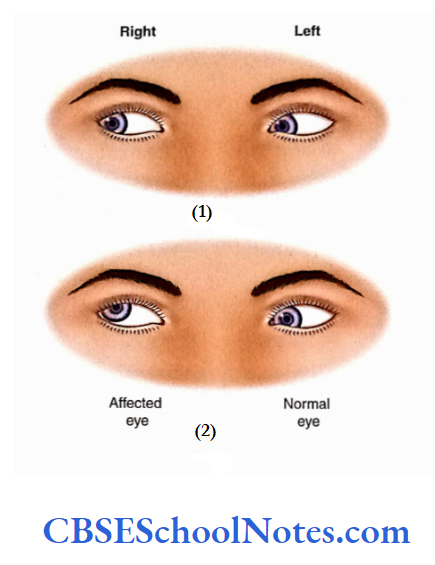
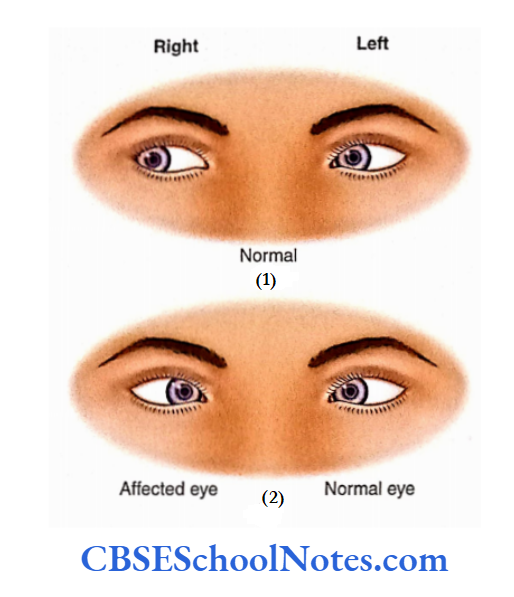
The lesion ofthe oculomotor nerve may present in the form of various clinical signs, as follows.
Squint: This is seen due to the unopposed action ofthe lateral rectus and superior oblique muscles. The eyeball moves downwards and outwards on the affected side.
Diplopia: Diplopia or double vision is seen when the patient tries to look medially, superiorly, or inferiorly.
Ptosis: The paralysis of the levator palpebral superioris muscle leads to drooping ofthe upper eyelid.
Loss of accommodation reflex is due to paralysis of the ciliary muscle.
Dilatation of pupil (mydriasis): Due to the damage of parasympathetic fibers, the unopposed action of sympathetic fibers leads to the dilation of the pupil.
Loss of light reflex: In cases of 3 nerve palsy, the dilated pupil fails to constrict in response to light.
Exophthalmos: The affected eyeball looks prominent as compared to a normal eye. This is due to paralysis of many extraocular muscles which keep the eyeball retracted.
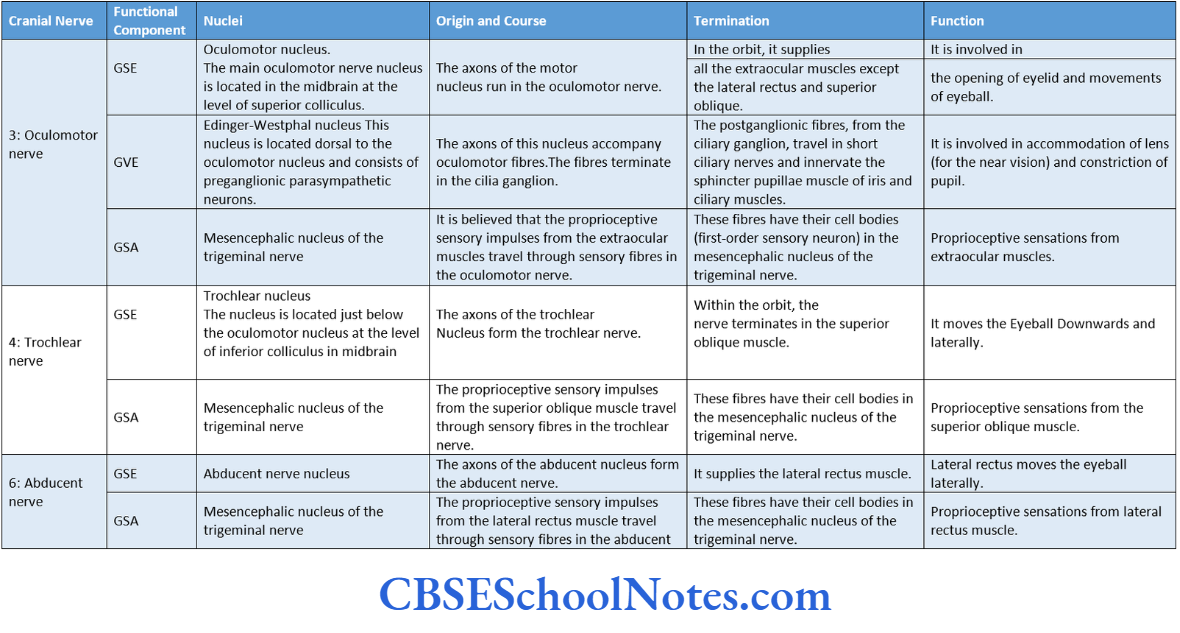
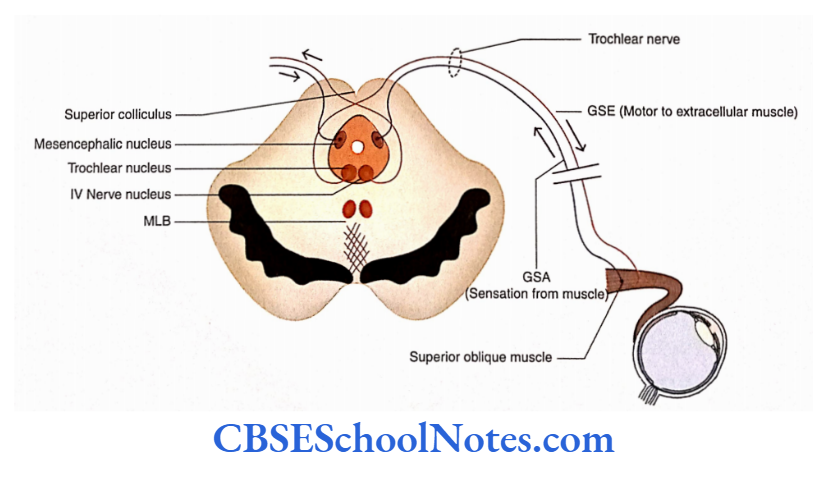
Trochlear Nerve
Trochlear Nerve Location of Nucleus
The trochlear nerve nucleus is located just below the oculomotor nucleus at the level of the inferior colliculus.
Trochlear Nerve Origin, Course, and Termination
- The fibers arising from the trochlear nerve nucleus follow an unusual course, i.e. these fibres curve backward around the periaqueductal grey matter and decussate in the superior medullary velum.
- The nerve emerges outside the brain immediately caudal to the inferior colliculus on each side ofthe frenulum veil
- The nerve then runs laterally and winds forward around the cerebral peduncle lying between the posterior cerebral and superior cerebellar arteries.
- The nerve soon passes through the lateral wall of the cavernous sinus and reaches the orbit after passing through the superior orbital fissure.
- Within the orbit, the nerve supplies the superior oblique muscle.
The trochlear nerve is a mixed nerve and has two functional components:
- SE and
- GSA.
For functional components, nuclei, origin, course, and termination of nuclear fibers and function of the trochlear nerve,
Trochlear Nerve Effects of Damage
- Squint: Damage to the trochlear nerve clinically produces a squint in the affected eye, and the affected eyeball in these cases moves in a superolateral direction.
- Diplopia: This occurs when the patient tries to look downwards. Thus, the patient will have difficulty in walking downstairs.
Trochlear Nerve Clinical Observations
The patient is unable to look inferolaterally, on the affected side, when asked to do so. This is due to paralysis ofthe superior oblique muscle.
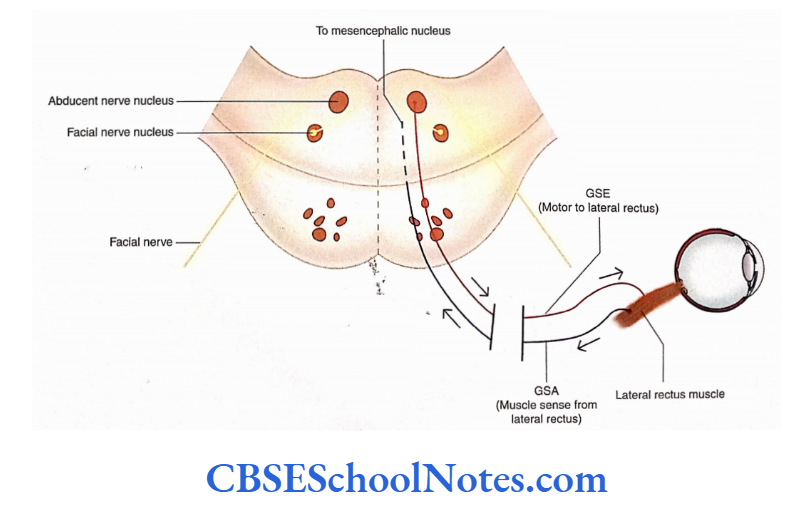
Abducent (Abducens) Nerve
Abducent Nerve Location of Nucleus
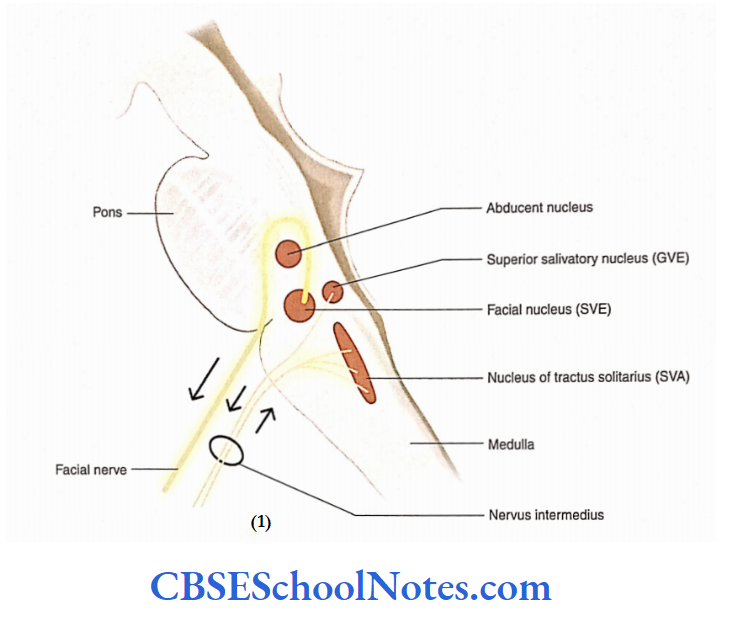
The motor nucleus of this nerve is located at the level of lower pons. It lies beneath the facial colliculus on the floor of the fourth ventricle.
Abducent Nerve Origin, Course, and Termination
- The neurons of this nucleus give origin to the fibers (axons) that pass through the tegmentum of the pons, in a ventral direction.
- The nerve comes out on the surface of the brainstem at the junction of the pons and pyramid.
- After lying in the lateral wall of the cavernous sinus, the nerve reaches the orbit through the superior orbital fissure and supplies the lateral rectus muscle.
The abducent nerve consists of two functional components:
- GSE and
- GSA.
For functional component, nuclei, origin, course, and termination of nuclear fibers and function of the abducent nerve.
- Medial squint: Damage to this nerve results in a clinical condition whereby the eyeball rotates medially; this condition is referred to as medial squint.
- Diplopia (double vision): It occurs when the patient tries to look on the lateral side.
- Damage to the nerve: This is suspected if the eyeball turns medially on the affected side when the patient is asked to look towards the lateral side.
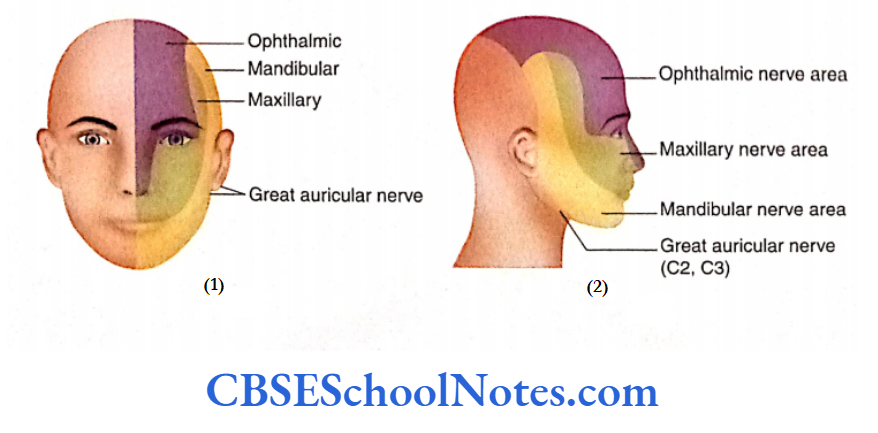
Trigeminal Nerve
The trigeminal is a mixed nerve and consists of three divisions:
- Ophthalmic,
- Maxillary, and
- Mandibular.
Therefore, it is called a trigeminal nerve.
Trigeminal Nerve Origin, Course, and Termination
- The trigeminal nerve is attached to the ventrolateral surface of the pons by the motor and sensory roots.
- The sensory root is big and lies lateral to the smaller motor root. Both motor and sensory roots run forward and laterally over the apex of the petrous temporal bone to reach the middle cranial Fossa.
- Here, the sensory root contains a ganglion (semilunar ganglion), which is enclosed in the recess of dura matter called a trigeminal cave. This ganglion contains pseudo-unipolar neurons, which are first-order neurons in the sensory pathways.
At its distal end, the semilunar ganglion branches into three divisions:
- Ophthalmic,
- Maxillary and
- Mandibular.
The motor root passes deep to the semilunar ganglion and fuses with the mandibular nerve.
The ophthalmic and maxillary are sensory nerves while the mandibular nerve consists of both motor and Three divisions of the trigeminal ophthalmic, maxillary, and mandibular—leave the cranial cavity through the superior orbital fissure, foramen rotundum, and foramen ovale, respectively.
Ophthalmic Nerve
After its origin from the semilunar ganglion, the ophthalmic division pierces the dura and lies in the lateral wall of the cavernous sinus.
Before entering the superior orbital fissure, it divides into three branches:
- Lacrimal,
- Frontal and
- Nasocilliary.
All three nerves give many branches in the orbit (For details of text and diagrams, refer to a textbook of Gross Anatomy.)
Through these branches, it supplies sensory fibers to the eyeball, conjunctiva, part of the nasal cavity, skin of the forehead, and lacrimal gland.
The ciliary ganglion is attached to the nasociliary nerve.
Maxillary Nerve
- After piercing the dura of the trigeminal cave, this nerve lies in the lateral wall of the cavernous sinus inferior to the ophthalmic division.
- The nerve leaves the skull through the foramen rotundum and enters in pterygopalatine fossa. From here, it reaches the orbit through the infraorbital fissure.
- In the orbit, it runs in the infraorbital groove and appears on the face through the infraorbital foramen. Here, it terminates by dividing by the number of branches.
- Through the pterygopalatine ganglion, it conveys the secretomotor (parasympathetic) fibers to the lacrimal gland and glands present in the nasopharyngeal mucosa.
- The nerve is sensory to the skin of the middle face, nasal cavity, gums maxillary teeth, and palate.
Mandibular Nerve
- The motor root of the trigeminal nerve fuses with the mandibular as it passes through the foramen ovale.
- After coming out through the foramen ovale, it lies in the infratemporal fossa as the trunk ofthe mandibular nerve.
- The trunk soon divides into anterior and posterior divisions. Many branches arise from the trunk, anterior, and posterior divisions. (For details of text and diagrams, refer to the textbook of Gross Anatomy.)
- As the mandibular nerve is a mixed nerve, it supplies motor fibers to the muscles of mastication and other muscles. It supplies the sensory fibers to the skin of the lower face, gum, and teeth of the lower jaw.
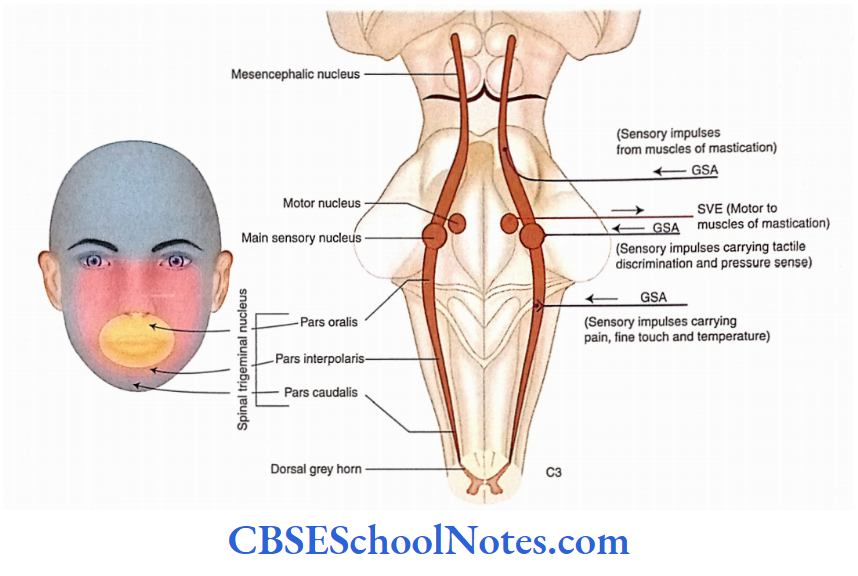
Location of Trigeminal Nuclei
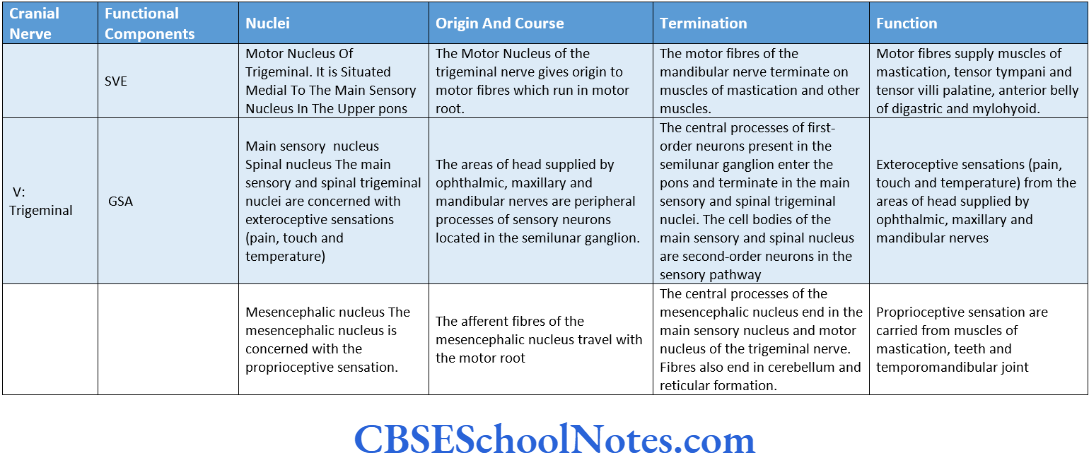
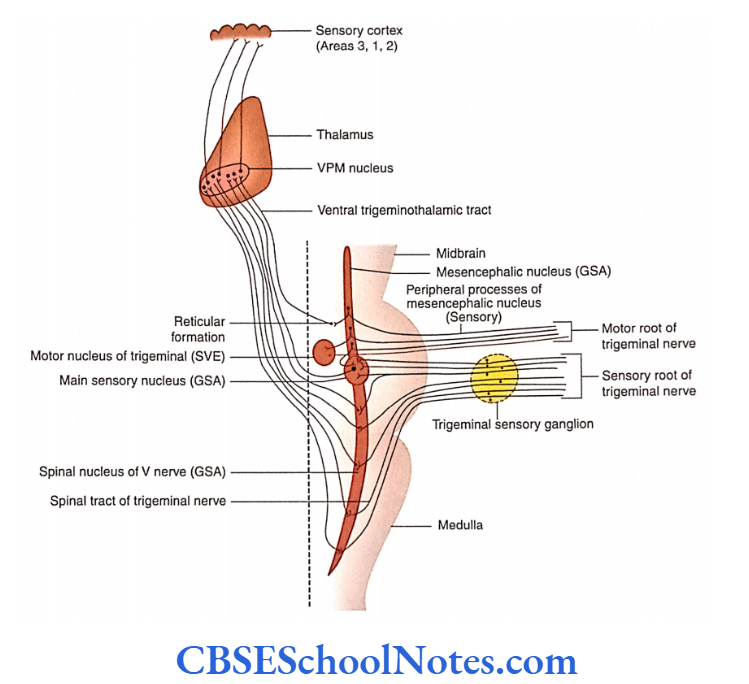
The trigeminal nerve is represented by three sensory nuclei and a single motor nucleus. The sensory nuclei (GSA) are the main sensory nucleus, a nucleus of the spinal tract, and the mesencephalic nucleus.
The motor nucleus (SVE) is referred to as the motor nucleus of the trigeminal nerve For functional component, nuclei, origin, course, and termination of nuclear fibers and function of the trigeminal nerve.
Trigeminal Neuralgia
- In this disorder of the trigeminal nerve, episodes of intense, stabbing pain occur in the area of distribution of one of the trigeminal nerve divisions.
- The maxillary division is most frequently involved and the ophthalmic division is least affected.
- Pain usually occurs in a specific zone of the face such as around the nose and mouth. The pain lasts for a few seconds to about 1-2 minutes but occurs repeatedly. The pain may be triggered by touching an especially sensitive area of skin.
- The exact cause of this disorder is not known. It is believed that the pressure of an artery leads to demyelination of the sensory nerve fibers. The short-circuiting of electrical impulses among the demyelinated axons is considered to generate an abnormal signal of pain.
- Painkiller drugs are of limited help. Severe cases can also be treated by cutting the nerve or by transection of the spinal trigeminal tract in the lower medulla.
- As the three divisions of the trigeminal nerve are somatotopically arranged in this tract, the transaction of fibers of a single division ofthe trigeminal nerve can be achieved.
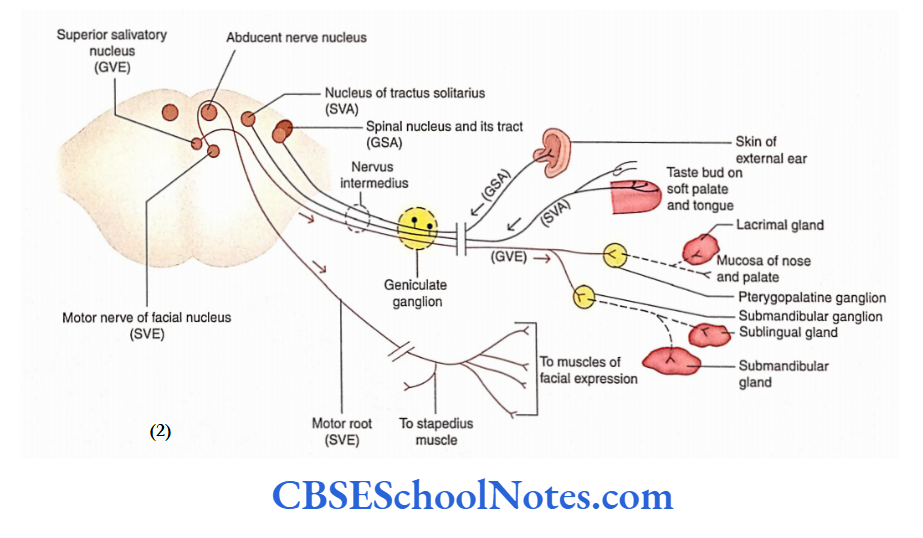
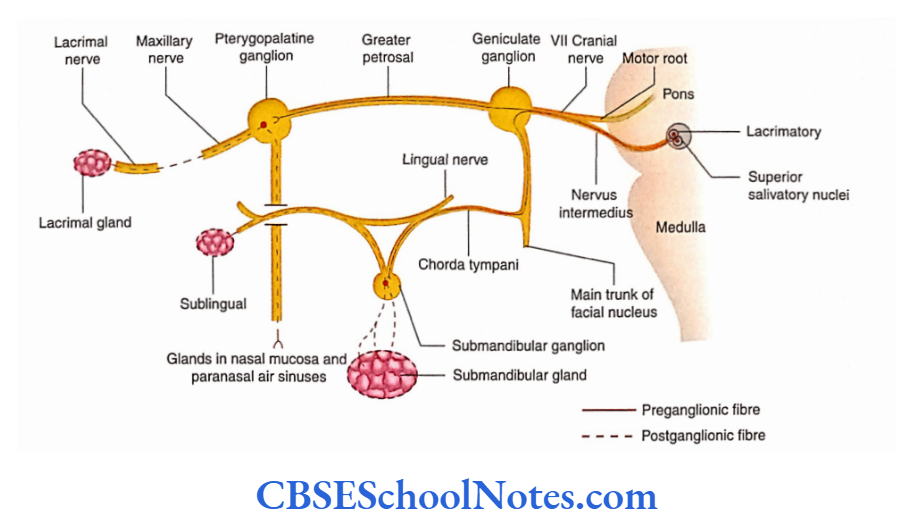
Facial Nerve
The facial nerve is a mixed nerve. It conveys the following:
- Sensation of taste.
- It is motor to all the skeletal muscles derived from the second pharyngeal arch.
- The nerve is secretomolor to lacrimal, submandibular and sublingual salivary glands.
The facial nerve emerges at the lower border of the pons in the cerebellopontine angle.
It has two roots:
- Facial nerve proper (containing motor fibers, SVE) and
- Nervus intermedius (containing sensory and preganglionic parasympathetic fibers.
- The nerve soon enters the internal acoustic meatus.
- Origin, Course, and Termination
The facial nerve arises from two roots:
- Motor and Sensory. Its sensory branch is also known as nervus intermedius.
- Both the roots are attached to the lower border of the pons medial to the 8 cranial nerve.
- The facial nerve, along with the 8 cranial nerve, enters the internal acoustic meatus. In the meatus, the sensory and motor roots of the facial nerve fuse to form a single trunk.
- In the facial canal, it runs laterally above the bony labyrinth of the internal ear. It then bends sharply backward to run in the medial wall of the middle ear. This bend is thick as it contains a genicular ganglion.
- At the junction of the medial and posterior walls of the middle car, it again bends downwards to come out of the skull through the stylomastoid foramen.
Within the facial canal, the nerve has three branches:
- Greater petrosal,
- Nerve to stapedius and
- Chorda tympani.
Soon after its exit from the stylomastoid foramen, it gives posterior auricular, digastric, and stylohyoid branches.
The nerve enters the posteromedial surface of the parotid gland and within the substance of the gland, it divides into five terminal branches (temporal, zygomatic, buccal, marginal mandibular, and cervical).
For functional components, nuclei, origin, course, and termination of nuclear fibers and function of the Facial nerve,
Cortical Connections of Motor Nucleus
The motor nucleus of the facial nerve is innervated by the corticonuclear fibers (supranuclear fibers) arising from the cerebral cortex. The fibers arising from the fascial nucleus (infranuclear fibers) innervate facial muscles.
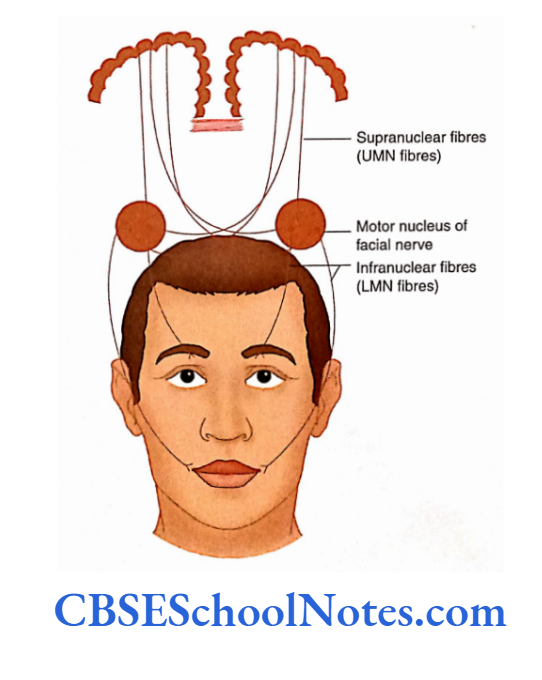
The neurons of the facial nerve supplying the muscles of the upper part of the face have double innervation, i.e. they are supplied by corticonuclear fibers from the same and opposite cerebral hemispheres.
However, the neurons of the facial nerve supplying muscles of the lower face are supplied by corticonuclear fibres of the opposite cerebral hemisphere only.
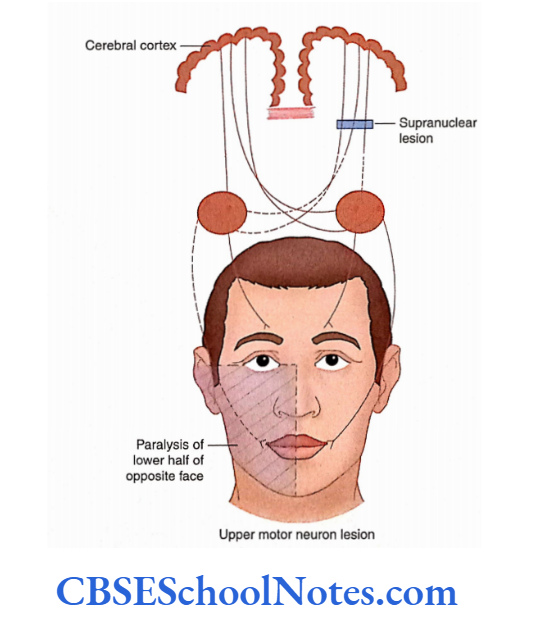
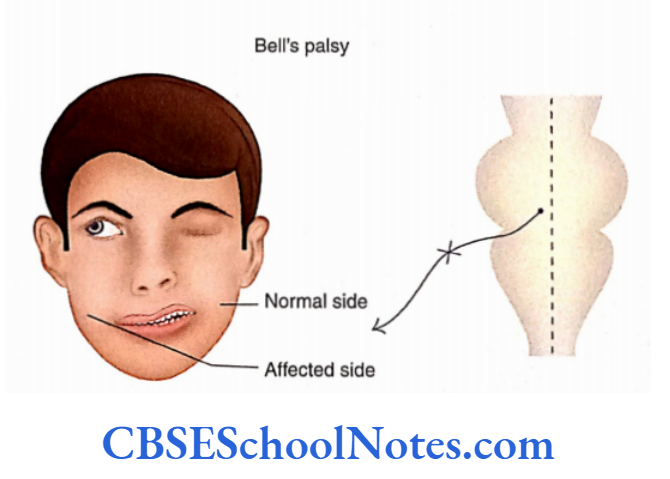
Neuroanatomical Basis of Facial Nerve Palsy
Supranuclear lesions (upper motor neuron [UMN] lesion): In the case of this lesion, only the muscles of the lower half of the face on the opposite side are paralyzed.
The muscles of the upper part of the face remain functional. This is because the muscles of the upper face receive bilateral corticonuclear connections and escape paralysis.
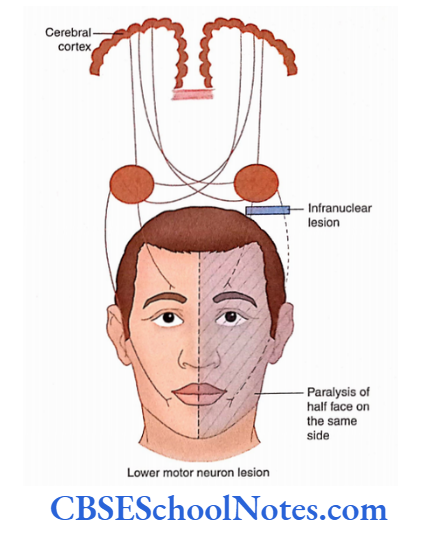
Nuclear and intranuclear lesions (lower motor neuron [LMN] lesion or Bell’s palsy): This kind of lesion is also known as LMN lesion and involves the axons of the facial motor nucleus.
The lesion may occur anywhere along the course of the facial nerve. The infranuclear paralysis of the facial nerve is called Bell’s palsy.
The most common site of internuclear lesion is near the stylomastoid foramen, though the nerve may get affected anywhere in the facial canal in the petrous temporal bone.
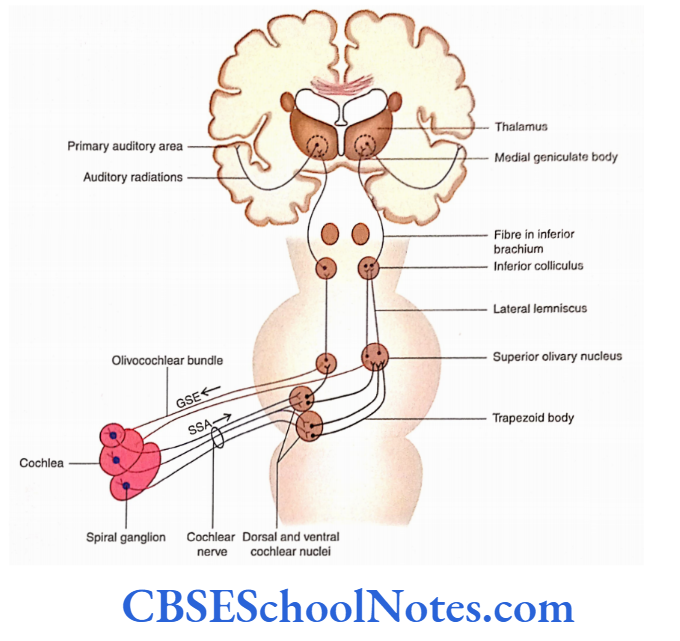
Vestibulocochlear Nerve
The vestibulocochlear nerve (8 cranial nerve) is predominantly sensory.
Anatomically and functionally, the nerve consists of two different parts:
Vestibular and Cochlear. The nerve comes out from the internal ear through the internal acoustic meatus.
After passing through the meatus, the vestibulocochlear nerve enters the brainstem at the lower border of pons posterolateral to the attachment of the facial nerve.
Lower Motor Neuron Lesion of the Vagus Nerve
The nuclear and intranuclear lesions will lead to the following clinical features depending on whether the lesion is unilateral or bilateral.
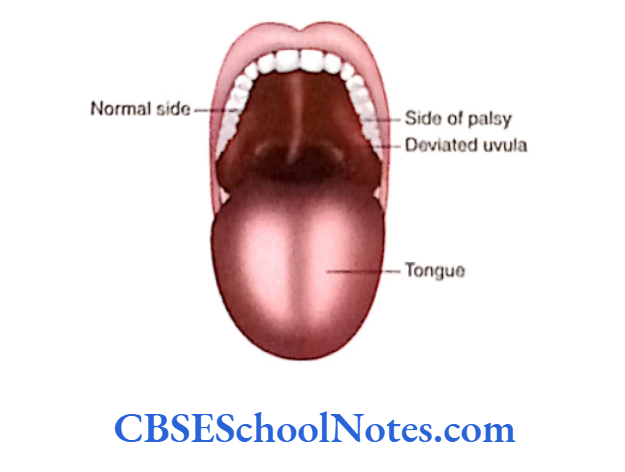
1. Unilateral lesion will present with the following features:
Paralysis of soft palate on the same side of the lesion. The soft palate elevates and the uvula deviates to the normal side due to the unopposed action of muscles on the normal side.
- Speech is affected and the ‘gag reflex’ is absent.
- Paralysis of pharyngeal muscles will lead to difficulty in swallowing.
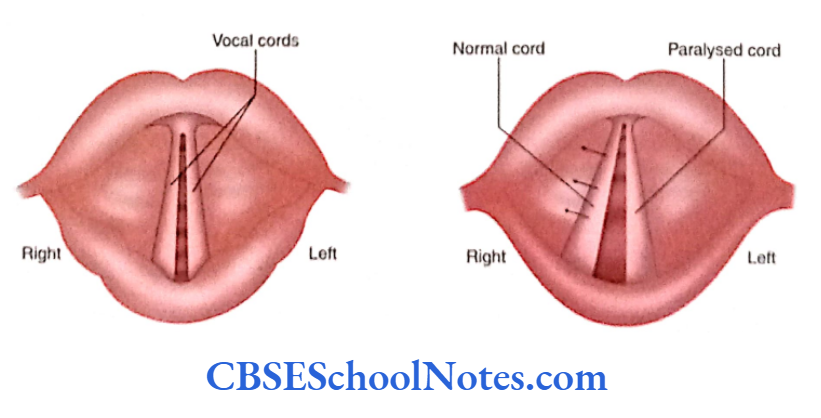
- Unilateral paralysis of laryngeal muscles will result in
hoarseness of voice and dyspnoea. - Loss of sensations from the mucous membrane of the pharynx and larynx, on the side of the lesion, would result in loss of cough reflex.
Bilateral lesions will show the following features:
Complete paralysis of the larynx. Both vocal cords are paralyzed; hence, there is a complete loss of voice. Death may result due to asphyxia.
Due to complete paralysis of the pharyngeal and palatine muscles, swallowing and speech are severely affected. The gag reflex is absent.
Origin, Course, and Termination
- The vagus nerve is attached superficially in the posterolateral sulcus of the medulla by 10-12 rootlets, just below the attachment of the glossopharyngeal nerve.
- These rootlets join to form a single trunk and leave the cranial cavity through the intermediate part of the jugular foramen. The vagus nerve receives fibers from the cranial root of the accessory nerve.
- The nerve bears two sensory ganglia: Superior and Inferior. The superior ganglion is situated in the jugular foramen and the inferior ganglion is just below the foramen.
- The nerve runs downwards within the carotid sheath between the internal carotid artery and the internal jugular vein till it reaches the root of the neck.
- On the right side, it enters the thorax by crossing the right subclavian artery whereas on the left side, it enters the thorax between the left common carotid and the left subclavian arteries.
- It gives many branches in the neck for the pharynx and larynx. It supplies parasympathetic branches to thoracic viscera and terminates in the abdomen by supplying many abdominal viscera.
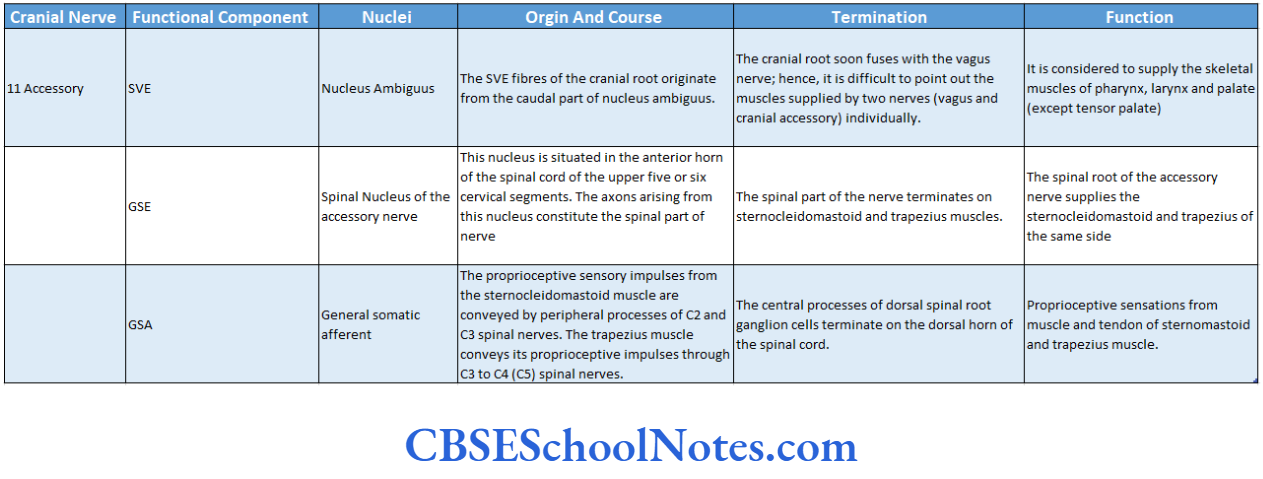
Accessory Nerve Nuclei
The accessory nerve is predominantly a motor nerve. The nerve consists of two distinct parts:
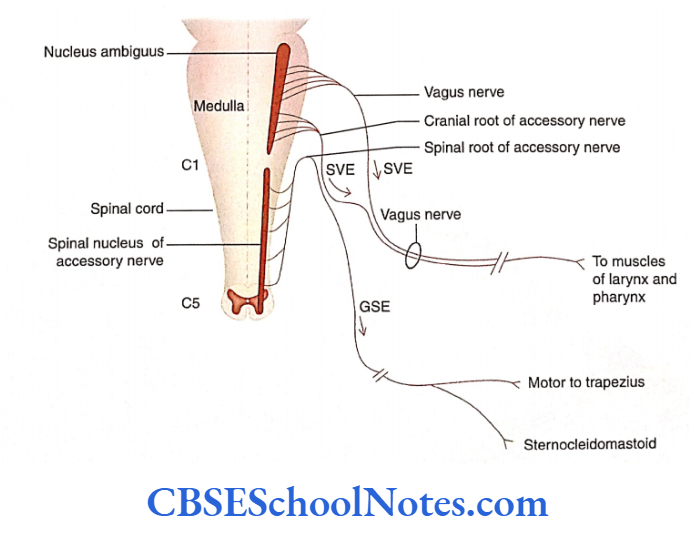
Cranial root and Spinal root. The cranial root (SVE) originates from the nucleus ambiguus and the spinal root (GSE) from the spinal nucleus of the accessory nerve. There is a sensory component also (GSA)
Accessory Nerve Nuclei Origin, Course, and Termination
The cranial and spinal roots of the accessory nerve take origin separately from their respective nuclei.
Cranial Root
- These fibers emerge as four to five rootlets from the posterolateral sulcus of the medulla, below the attachment of the filament of the vagus nerve. The rootlets of the cranial part join to form a trunk and then pass laterally toward the jugular foramen.
- During its course in the jugular foramen, the nerve joins the spinal root for a short distance. The two roots soon separate as they come out of the jugular foramen.
- The cranial root passes over the inferior ganglion of the vagus nerve and fuses with it to become part of the vagus nerve.
- The fibres of the cranial part of the accessory nerve are considered to supply all the intrinsic muscles of the larynx through the recurrent laryngeal branch of the vagus nerve.
Spinal Root
- The GSE fibers of the spinal root originate as five to six rootlets from the lateral aspect of the spinal cord between dorsal and ventral roots.
- These rootlets soon join to form a trunk that ascends through the vertebral canal and enters the skull through the foramen magnum.
- The nerve root comes out of the cranial cavity through the jugular foramen in association with the vagus and glossopharyngeal nerves.
- The spinal root of the accessory nerve supplies the sternocleidomastoid and trapezius on the same side.
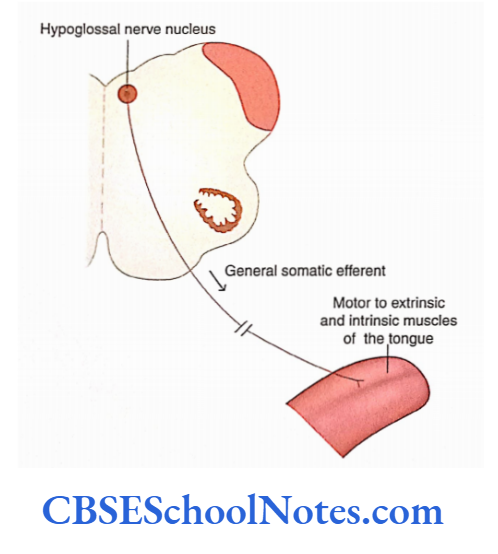
Hypoglossal Nerve
The hypoglossal nerve is motor to all the extrinsic and intrinsic muscles of the tongue except palatoglossus (which is supplied by the vagus nerve).
Though the hypoglossal nerve is predominantly a somatic motor nerve (GSE), it also contains proprioceptive (sensory, GSA) fibers from the muscles of the tongue.
Hypoglossal Nerve Origin, Course, and Termination
- The nerve exits on the ventral surface of the medulla, between the pyramid and the olive by 15-20 rootlets.
- These rootlets of the nerve soon join and leave the skull through the hypoglossal canal.
- Extracranially, the hypoglossal nerve descends lateral to the vagus nerve and just above the hyoid bone it enters the root of the tongue.
- The hypoglossal nerve is motor to all extrinsic and intrinsic muscles of the tongue, except for the palatoglossus muscles
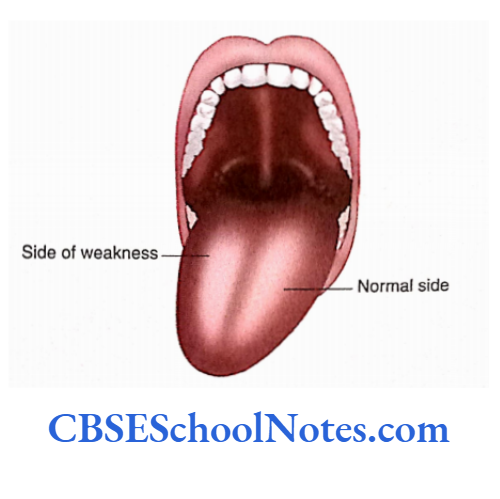
Hypoglossal Nerve Effect of Damage
If the hypoglossal nerve or nucleus is damaged, it leads to the following clinical effects:
- Impaired speech, chewing, and swallowing
- Deviation of tongue towards the injured side, if asked to protrude.
- Atrophy of the tongue towards the damaged side.
- Inability to protrude tongue if nerves on both sides are damaged.
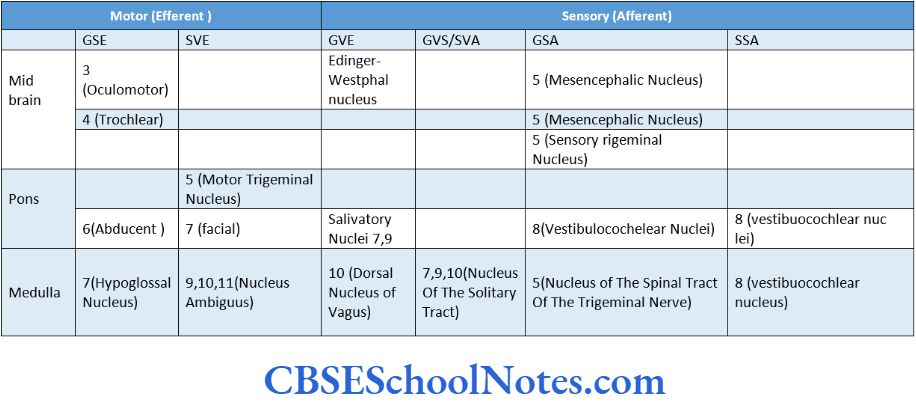
Cranial Nerves Nuclei Summary
- During the development of the neural tube, the alar lamina forms the sensory nuclei while the basal lamina forms the motor nuclei.
- The motor columns that develop in the basal lamina of the brainstem are GSE, SVE, and GVE.
- The sensory columns that develop in the alar lamina of the brainstem are GVA, SVA, GSA, and SSA.
- The somatic efferent column consists of nuclei of the cranial nerves 3, 4, 6, and 7.
- The SVE column includes the motor nuclei of cranial nerves 5,7 and nucleus ambiguus (9, 10, and 9). These nerves supply skeletal muscles derived from pharyngeal arches (branchiomotor).
- The GVE column consists of parasympathetic nuclei (secretomotor).
- GVA and SVA columns are represented by the ‘nucleus of solitary tract’. The nucleus receives sensory fibers from the viscera of neck, thorax, and abdomen; it also receives taste sensations from the tongue, epiglottis, and palate.
- The GSA column is represented by the sensory nuclei of the trigeminal nerve, namely the main sensory nucleus, spinal nucleus, and mesencephalic nucleus.
- The SSA column is represented by vestibulocochlear nuclei.
- The 3, 5, and 4 cranial nerves are predominantly motor nerves that supply extraocular muscles. These nerves are represented by SE and GVA columns. The 3 cranial nerve is additionally represented by the GVE column.
- The V cranial nerve is represented by a motor nucleus (SVE) and three sensory nuclei (GSA—mesencephalic, main sensory, and spinal nucleus).
- The trigeminal nerve is motor to muscles of mastication and it also carries sensory impulses from the skin of the scalp and face.
- The 7 nerve has the following functional columns: SVE (motor nucleus of the facial nerve), GVE (superior salivatory nucleus), and SVA (nucleus of the solitary tract). The facial nerve is motor to muscles of facial expression and secretomotor to salivary glands (except parotid). It also carries taste sensations from the anterior two-thirds of the tongue and soft palate.
- The 8 cranial nerve is predominantly a sensory nerve and the sensory component is represented by the SSA column.
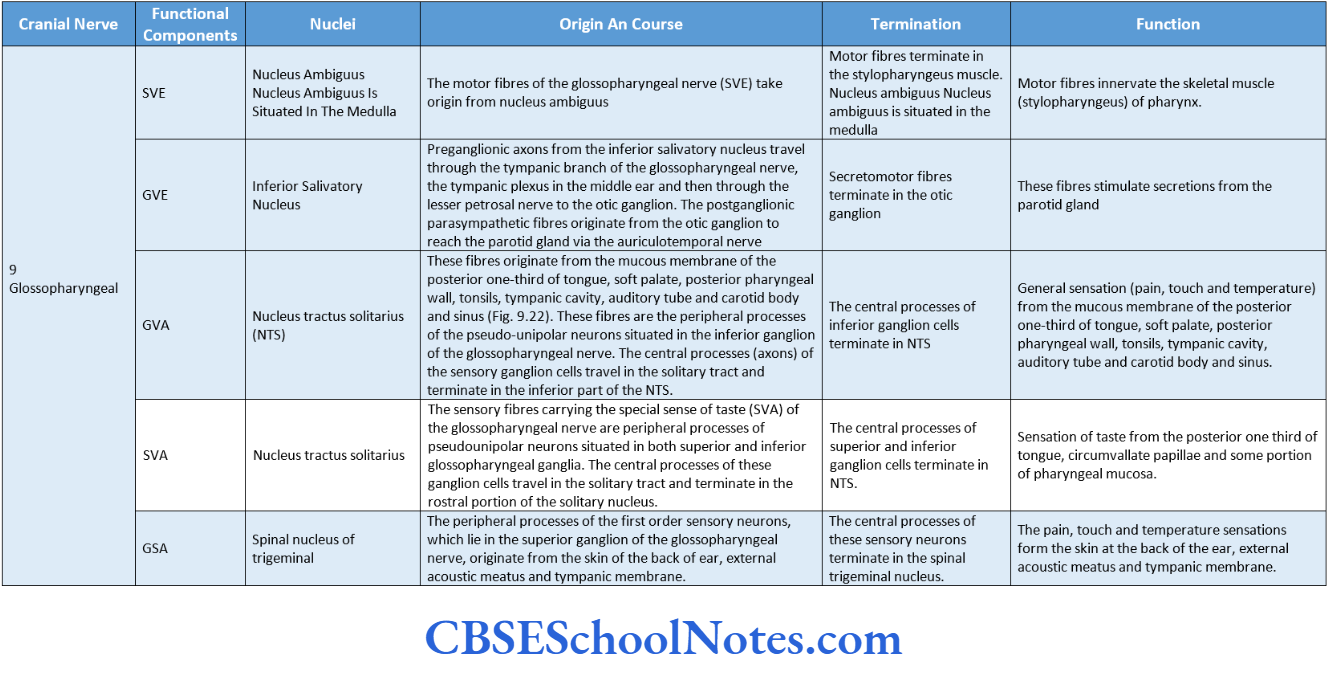
- The 7 cranial nerve is a mixed nerve and consists of the following functional components: SVE (nucleus ambiguus), GVE (inferior salivatory nucleus), GVA (NTS), and SVA (NTS).
- The nerve gives motor innervation to the stylopharyngeus muscle and secretomotor innervation to the parotid gland; it also conveys general and taste sensations from the pharynx and the posterior one-third of the tongue.
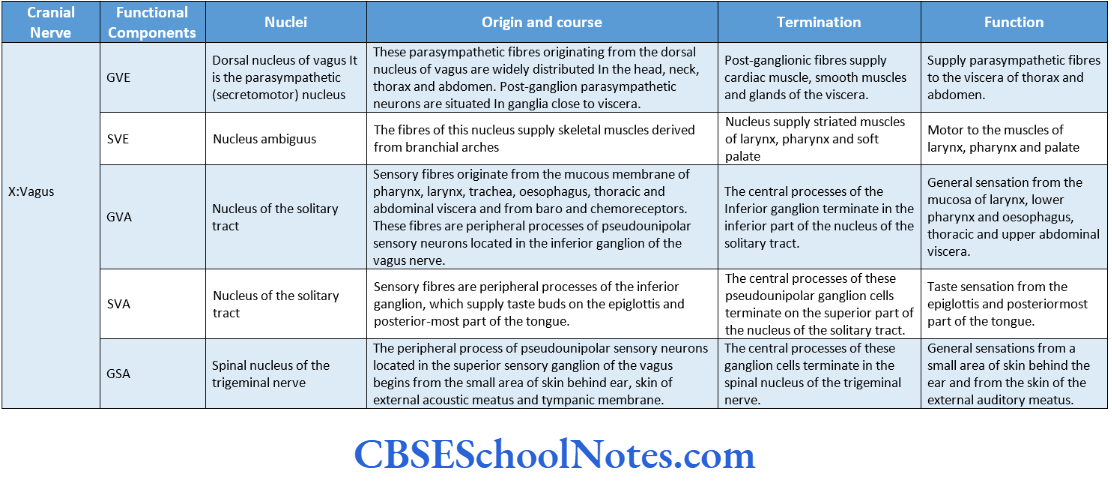
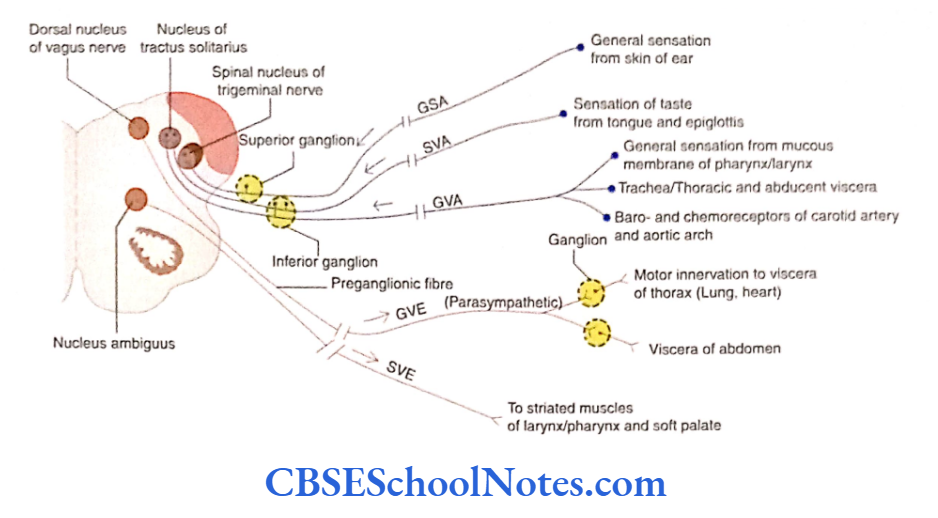
- The X cranial nerve is also a mixed nerve. It is represented by the following functional components: GVE (dorsal nucleus of vagus), SVE (nucleus ambiguus), GVA (NTS), SVA (NTS), and GSA (spinal nucleus of the trigeminal nerve).
- The vagus nerve is secretomotor to glands and viscera, branchiomotor to the pharynx, larynx, and soft palate, and carries general sensation from the viscera and special sensation of taste from the epiglottis and tongue.
- The 9 cranial nerve is predominantly a motor nerve and includes the following functional components: SVE (nucleus ambiguus), GSE (spinal nucleus of the accessory nerve), and GSA (proprioceptive fibers of the spinal nerve).
- The spinal accessory nerve innervates the trapezius and sternocleidomastoid muscles.
- The 7 cranial nerve is predominantly a motor nerve that innervates the musculature of the tongue. It has the following functional components: GSE (hypoglossal nerve nucleus) and GSA (proprioceptive).
Multiple Choice Questions
Question 1. Which of the following statements about cranial nerves is/are true?
- Cranial nerves 1 and 2 are attached to the forebrain
- Cranial nerves 9 to 12 are attached to the medulla
- Cranial nerves 3 and 4 are attached to midbrain
- Cranial nerve 4 is attached to the dorsal aspect of the brain
- All of the above
Answer: 5. All of the above
Question 2. Following are tried nerve cell columns in the basal lamina (efferent or motor columns) except
- GSE (general somatic efferent)
- SVE (special visceral efferent)
- GVE (general visceral efferent)
- SSE (special somatic efferent)
Answer: 4. GVE (general visceral efferent)
Question 3. Following are tried nerve cell columns in the alar lamina (efferent or sensory columns) except
- GVA (general visceral afferent)
- SVA (special visceral afferent)
- GSA (general somatic afferent)
- SSA (special somatic afferent)
- GSA (general sympathetic afferent)
Answer: 3. GSA (general somatic afferent)
Question 4. Which of the following cranial nerve nuclei does not belong to the general somatic efferent (GSE) column?
- Oculomotor nucleus
- Trochlear nucleus
- Facial nucleus
- Abducent nucleus
- Hypoglossal nucleus
Answer: 3. Abducent nucleus
Question 5. The special visceral efferent (SVE) column consists of the following nerve nuclei except
- Motor nucleus of the trigeminal nerve
- Facial nerve nucleus
- Nucleus ambiguus
- The dorsal nucleus of the vagus
Answer: 3. Nucleus ambiguus
Question 6. Which of the following nuclei belongs to the GVE column?
- Edinger-Westphal
- Salivatory nuclei
- Lacrimatory nucleus
- The dorsal nucleus of the vagus
- All of the above
Answer: 3. Lacrimatory nucleus
Question 7. The following nuclei belong to the GSA column except?
- Sensory trigeminal nucleus
- Mesencephalic nucleus
- Nucleus solitary tract
- Nucleus of the spinal tract of trigeminal
Answer: 3. Nucleus of solitary tract
Question 8. The following cranial nerve nuclei are located in the midbrain except?
- Oculomotor nerve nucleus
- Trochlear nerve nucleus
- Abducent nerve nucleus
- Edinger-Westphal nucleus
- Mesencephalic nucleus
Answer: 3. Edinger-Westphal nucleus
Question 9. Which of the following motor (efferent) nerve nuclei are located in pons?
- Abducent nerve nucleus
- Facial nerve nucleus
- Motor trigeminal nucleus
- Salivatory nucleus
- All of the above
Answer: 5. All of the above
Question 10. The following sensory (efferent) nuclei are located in the medulla except
- The nucleus of the spinal tract of trigeminal
- Vestibular nucleus
- Cochlear nucleus
- Nucleus of the solitary tract
- The main sensory nucleus of trigeminal
Answer: 5. Main sensory nucleus of trigeminal
Question 11. Which of the following nuclei represents the GVA and SVS columns?
- Nucleus solitary tract
- The main sensory nucleus of trigeminal
- The spinal nucleus of the trigeminal
- Mesencephalic nucleus
- Cochlear nucleus
Answer: 1. Nucleus of solitary tract
Question 12. Which of the following functional components is/are not present in the oculomotor nerve?
- SE
- GVE
- GSA
- GVA
Answer: 4. GVA
Question 13. Which of the following functional components are present in the trochlear nerve?
- SE and GSA
- SE, GVE, and GSA
- GVE and GSA
- None of the above
Answer: 1. SE and GSA
Question 14. Which of the following structures send their sensory proprioceptive impulses to the mesencephalic nucleus of the trigeminal nerve?
- Upper and lower teeth
- Periodontal ligaments and joint capsule
- Muscles of mastication
- Extraocular muscles
- All of the above
Answer: 5. All of the above
Question 15. The facial nerve has the following functions except
- It is motor to the muscle of the face
- It conveys the sensation of taste from the anterior two-thirds of the tongue
- It is secretomotor to lacrimal, submandibular and sublingual salivary glands
- It carries exteroceptive sensation from the skin of the face
- It carries exteroceptive sensation from the part of the skin of the external ear
Answer: 4. It carries exteroceptive sensation from the skin of the face
Question 16. Which of the following statements is/are true about the infranuclear facial nerve lesion in the facial canal?
- Paralysis of facial muscles
- Loss of taste from the anterior two-thirds of the tongue
- Secretion from submandibular, sublingual, and lacrimal glands is affected
- The sound seems abnormally loud
- All of the above
Answer: 5. All of the above
Question 17. Which of the following nuclei is not connected with the glossopharyngeal nerve?
- Nucleus ambiguus
- Inferior salivatory nucleus
- Nucleus of tractus solitarius
- Lacrimatory nucleus
Answer: 4. Lacrimatory nucleus
Question 18. Which of the following nuclei contribute to the vagus nerve?
- The dorsal nucleus of the vagus
- Nucleus ambiguus
- Spinal nucleus of the trigeminal nerve
- Nucleus of the solitary tract
- All the above
Answer: 5. All the above