Bones Of The Lower Limb
The lower limb consists of many regions. The following bones are present in various regions of the lower limb:
Pelvic (Hip) Region
Bones of Pelvic (Hip) Region region form the pelvic girdle. The pelvic girdle consists of two hip bones. These bones are united to each other in the midline anteriorly to form a joint known as the pubic symphysis.
Both the hip bones unite posteriorly with the sacrum at the sacroiliac joint. The pelvic girdle (two hip bones) and sacrum together form a basin-like structure called a bony pelvis.
Thigh Bones
This region consists of a single bone called as femur. The upper end of this bone articulates with a hip bone to form a hip joint. The lower end of the femur articulates with the upper end of the tibia to form the knee joint.
Leg Bones
This region consists of two long bones, i.e., medially placed tibia and laterally placed fibula. These two bones, at their lower end, articulate with talus to form ankle joint.
Foot Bones
The skeleton of the foot consists of many bones, i.e., tarsals, metatarsals, and phalanges. These bones form many joints, i.e., intertarsal, tarsometatarsal, metatarsophalangeal, and interphalangeal.

Hip Bone
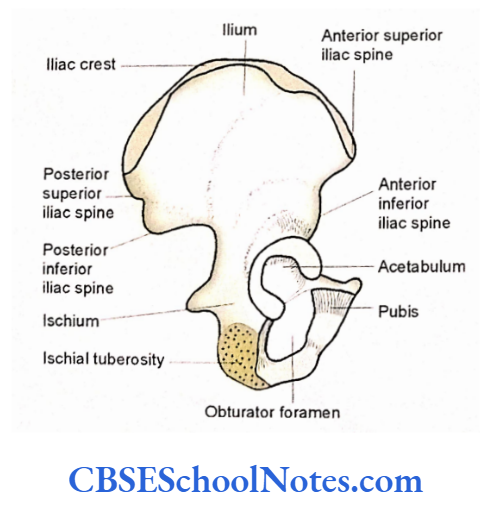
The hip bone is n large, irregular, and flat bone. The middle portion of the bone is constricted and carries a cup-shaped deep cavity on the lateral aspect of the bone. This cavity is known as the acetabulum. The bone is expanded above and below the acetabulum.
Read and Learn More Human Osteology Notes
There is the presence of a large oval or triangular aperture just below and medial to the acetabulum. It is called as obturator foramen.
The bone above the acetabulum is expanded and flat. This portion is called ilium. The bone below the acetabulum consists of two parts, i.e., the anterior and inferior, pubis and posterior and inferior, ischium.
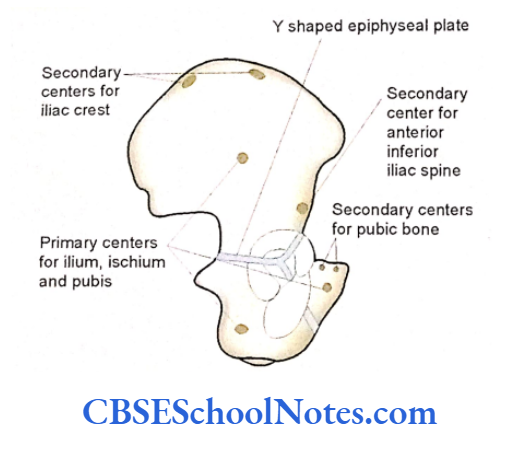
(Though an adult hip bone is a single bone at birth each hip bone consists of three separate primary bones, i.e., ilium, ischium, and pubis.
These three bones are joined to each other by a Y-shaped tri-radiate hyaline cartilage. These three components of hip bones join each other at the acetabulum. However, these three bones begin to fuse at 15 to 17 years of age.
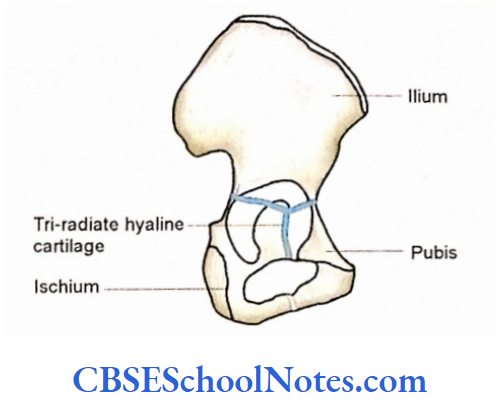
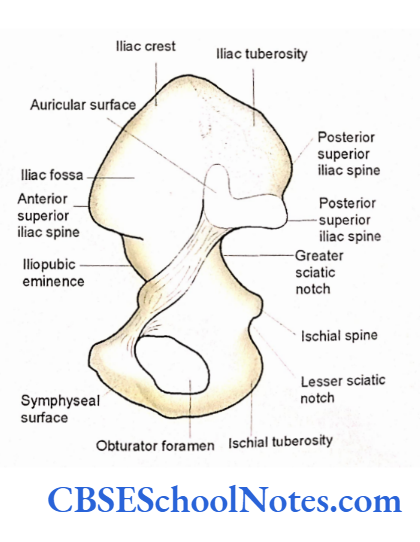
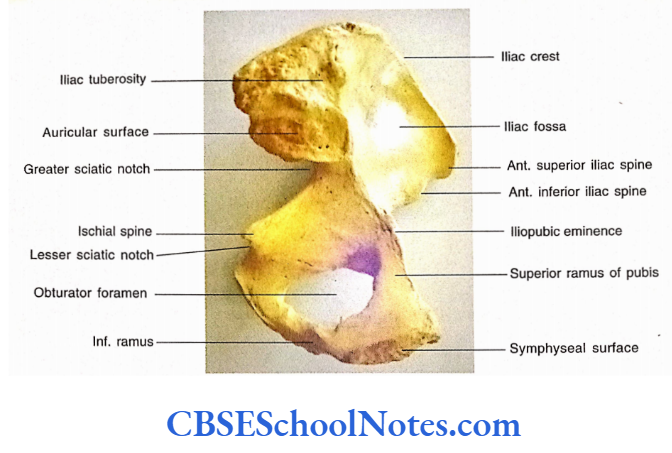
Though in an adult bone, the site of fusion is not visible between three bones, their names are still used as three parts of hip bone). In Fig. 3.4 medial view of the hip bone is shown.
Hip Bone Side Determination
Take the help of your teacher to determine the side of the hip bone
- The expanded flat part called as ilium, should be kept upwards (superiorly).
- The other expanded part (pubis and ischium) with the obturator foramen should be kept downwards (interiorly).
- The acetabulum should face laterally.
- The lower expanded part (below the acetabulum) has two parts, i.e., thin pubis and thick ischium. The pubis should be directed anteriorly and the ischium posteriorly.
- Many students find it difficult to keep the bone in an anatomical position.
- Therefore you should learn the anatomical position of this bone only after you have learned the general features of all three parts (ilium, ischium, and pubis).
Ilium
Ilium is the largest part of the hip bone. It forms the upper fan-shaped expanded part above the acetabulum. The upper 2/5th of the acetabulum is formed by the ilium.
Ilium General Features
The ilium presents:
- Two ends-Upper and lower.
- Three borders-Anterior, posterior, and medial.
- Three surfaces-Gluteal (lateral), iliac fossa, and sacropelvic.
ilium Ends
- Upper end-The upper end is in the form of an expanded border. It is also called an iliac crest. The iliac crest is a thick and curved border, which is convex upwards.
- This extends between two projections, i.e., anterior superior iliac spine and posterior superior iliac spine.
- The iliac crest is subdivided into ventral and dorsal segments.
- The ventral segment is anterior 2/3rd of the iliac crest and presents an outward convexity, while the dorsal segment forms posterior 1/3 of the crest and presents outward concavity.
- The thick ventral segment of the iliac crest shows an outer lip, intermediate area, and inner lip.
- The outer lip presents a prominence about 5 cm behind the anterior superior iliac spine. This is called as tubercle of the iliac crest.
- The dorsal segment of the iliac crest presents medial and lateral sloping surfaces separated by a ridge.
Lower end-The lower end of the ilium lies in the acetabulum and forms the upper 2/5th of this cup-shaped cavity. At the lower end, ilium becomes continuous with the ischium and pubis. The lower end of the ilium meets with the pubis at iliopubic eminence.
Ilium Borders
Anterior border The anterior border of the ilium extends from the anterior superior iliac spine to the acetabulum. The lowest part of this border projects forwards, near the upper margin of the acetabulum, to form the anterior inferior iliac spine.
The posterior border extends from the posterior superior iliac spine to the greater sciatic notch.
Here it becomes continuous with the upper end of the posterior border of the ischium. This border presents a posterior inferior iliac spine and greater sciatic notch.
Medial border The medial border is present on the inner aspect (medial surface) of the ilium. This border extends from the iliac crest to the iliopubic eminence.
It lies between the iliac fossa and the sapropelic surface of the ileum. The medial border is rough in its upper l/3rd, sharp in its middle third, and rounded in the lower l/3rd. The lower one-third of the medial border is called an arcuate line.
Ilium Surfaces
The ilium has an outer gluteal surface and an inner surface, which is further divided into the iliac fossa and sapropelic surface.
The gluteal surface surface is the lateral surface (outer aspect) of the ilium. It has three rough curved lines (the posterior, anterior, and inferior gluteal lines), which divide the gluteal surface into four areas.
Iliac fossa-The iliac fossa is present on the anterior part of the medial surface of the ilium, in front of the medial border. The Iliac fossa presents shallow concavity and has a smooth surface.
The sapropelic surface is also present on the medial surface of the ilium behind the iliac fossa and medial border. It is subdivided into three parts, i.e., iliac tuberosity, auricular surface, and pelvic surface.
The iliac tuberosity is the upper rough part.
The auricular surface is ear-shaped and articular. It is the middle part of the sacropelvic surface, which articulates with the sacrum to form the sacroiliac joint.
The pelvic surface is the smooth surface below and in front of the auricular surface. This surface is continuous with the pelvic surface of the ischium. This surface may present a pre-auricular sulcus in the females who have given birth to children (multiparous).
Pubis
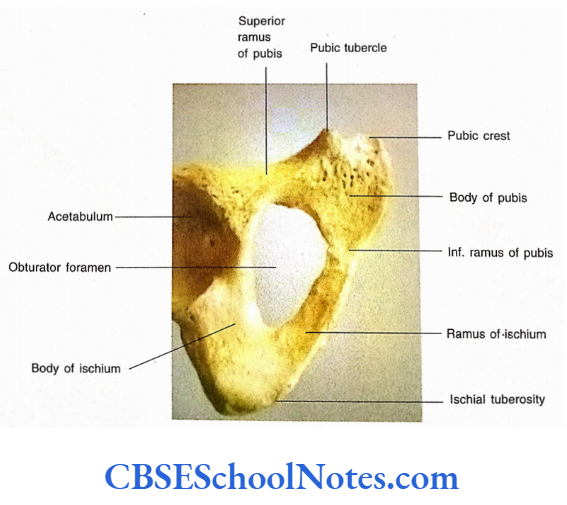
The pubis or pubic bone is situated ventromedial to ilium and ischium. It consists of a body, a superior ramus, and an inferior ramus.
Body of Pubis
The body is flattened and presents three surfaces, i.e., anterior, posterior (pelvic), and medial (symphyseal). The anterior surface faces downwards, forward, and laterally. The posterior surface is smooth and directed upwards and backward.
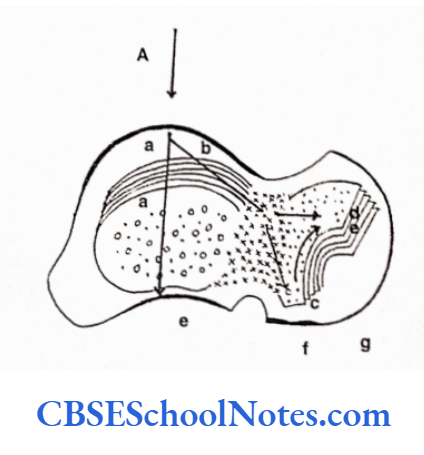
The symphyseal surface articulates with the corresponding surface of the opposite pubic bone to form a joint known as a pubic symphysis. This surface shows the presence of ridges that change with increasing age (See Further Details).
The superior border of the body of the pubis is thick and known as a pubic crest. At the lateral end of the pubic crest, there is a projection, the pubic tubercle.
Superior Ramus of Pubis
The superior ramus of the pubis arises from the upper and lateral parts of the body of the pubis.
Laterally it extends above the obturator foramen upto the iliopubic eminence where it joins the ilium. Here it also forms the pubic part (anterior 1/5) of the acetabulum. It has three borders (anterior, posterior, and inferior) and three surfaces (pectineal, pelvic, and obturator).
Pubis Borders
- The anterior border is also known as the obturator crest and extends from the pubic tubercle to the acetabular notch.
- The posterior border or pectineal line (pecten pubis) extends from the pubic tubercle to the iliopubic eminence.
- It is a sharp border, which behind the iliopubic eminence becomes continuous with the arcuate line of ilium.
- The inferior border forms the upper border of the obturator foramen.
Pubis Surfaces
- The pectineal surface is situated between the pectineal line and the obturator crest. It is triangular and extends between the pubic tubercle and iliopubic eminence.
- The pelvic surface lies between the pectineal and inferior border of the superior ramus. It is smooth and continuous medially with the pelvic surface of the body of the pubis.
- The obturator surface is situated between the obturator crest and the inferior border. It is a grooved surface and forms the upper boundary of the obturator canal.
Inferior Ramus of Pubis
It extends downwards and laterally from the lower and lateral parts of the body of the pubis. The inferior ramus of the pubis meets the ramus of the ischium to form the conjoined ischiopubic rami. The conjoined ischiopubic rami form the medial boundary of the obturator foramen. It has an anterior and a posterior surface.
Ischium
The ischium forms the posteroinferior part of the hip bone. It consists of a body and a ramus.
Ischium Body
The body lies postero inferior to the acetabulum. It has two ends (upper and lower), three borders (anterior, posterior, and lateral), and three surfaces (femoral, dorsal, and pelvic).
Ischium Ends
- The upper end of the body forms the 2/5 of the posterior and the inferior part of the acetabulum.
- The lower end forms the ischial tuberosity. The ramus of the ischium extends from the lower end of the body upwards, forwards, and medially to meet the inferior ramus of the pubis.
Ischium Borders
- The anterior border forms the posterior margin of the obturator foramen.
- The posterior border is continuous with the posterior border of the ilium. It presents a triangular projection called an ischial spine.
- The ischial spine is placed between the greater sciatic notch (above) and the lesser sciatic notch (below).
- The lateral border extends from the lower margin of the acetabulum and becomes continuous with the lateral margin of the ischial tuberosity.
Ischium Surfaces
- The femoral surface is situated between the anterior and lateral borders.
- The dorsal surface is continuous above the gluteal surface of the ilium. The lower part of the dorsal surface has a large rough area known as ischial tuberosity.
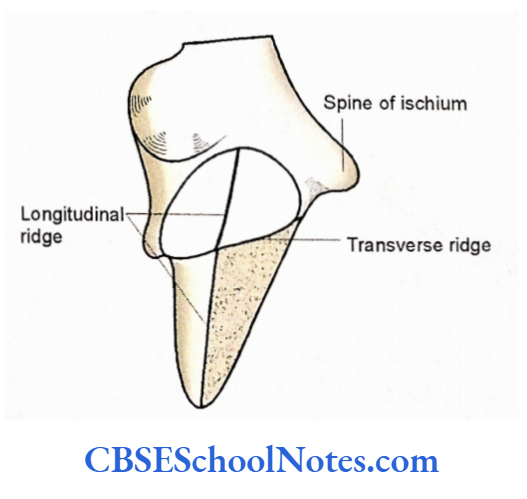
- This tuberosity is divided by a transverse ridge in an upper quadrilateral part and a lower triangular part. Each of these parts (upper and lower) is again divided into medial land lateral parts.
- The pelvic surface of the ischium is smooth and lies between the anterior and posterior borders.
Ramus of Ischium
- It extends from the lower part of the body and runs upwards, forwards, and medially.
- Here it meets the inferior ramus of the pubis and forms the conjoined ischiopubic ramus.
- The conjoined ischiopubic ramus presents upper and lower borders and an outer and inner surface.
Obturator Foramen
It is a large triangular or oval foramen in the lower part of the hip bone. It is situated between the pubis and ischium.
The obturator foramen is bounded above by the superior ramus of the pubis, medially by the body of the pubis and conjoined ischiopubic ramus, and laterally by the body of the ischium.
Acetabulum
- The acetabulum is a deep cup-shaped cavity facing laterally and anterior inferiorly. It is situated on the constricted middle part of the hip bone. All three parts of the hip bone (pubis, ischium, and ilium) contribute to its formation.
- The acetabulum articulates with the head of the femur to form the hip joint.
- The margin of the acetabulum is sharp and deficient in the anteroinferior part. This gap in the margin is called an acetabular notch.
- The floor of the acetabulum has a horseshoe-shaped articular surface (lunate surface) and a non-articular central acetabular fossa.
Anatomical Position of Hip Bone Keeps the bone in such a way that:
- The pubic bone lies anteriorly and the symphyseal surface of the pubis lies in the median plane.
- The acetabulum faces laterally and slightly anteriorly.
- The pubic tubercle and anterior superior iliac spine should lie in the same coronal plane.
- The posterior surface of the body of the pubic bone should face postero-superiorly.
- The ischial spine and superior end of the pubic symphysis are approximately in the same horizontal plane.
Acetabulum Particular Features
Ilium
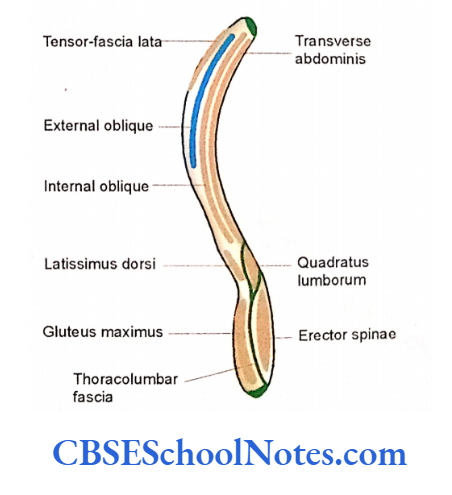
- The external oblique muscle of the abdomen is inserted on the outer lip into the anterior 2/3rd of a ventral segment of the iliac crest.
- The internal oblique originates from the intermediate area of the ventral segment of the iliac crest.
- The inner lip gives origin to transverse abdominis.
- The tensor-fascia lata muscle arises from the outer lip of the iliac crest near its anterior part.
- Part of the latissimus dorsi arises from the posterior most of the outer lip of the ventral segment.
- The quadratus lumborum arises from the posterior one-third of the inner lip of the ventral segment of the iliac crest.
Attachment of the Muscles on the Dorsal 1/3rd of the Iliac Crest
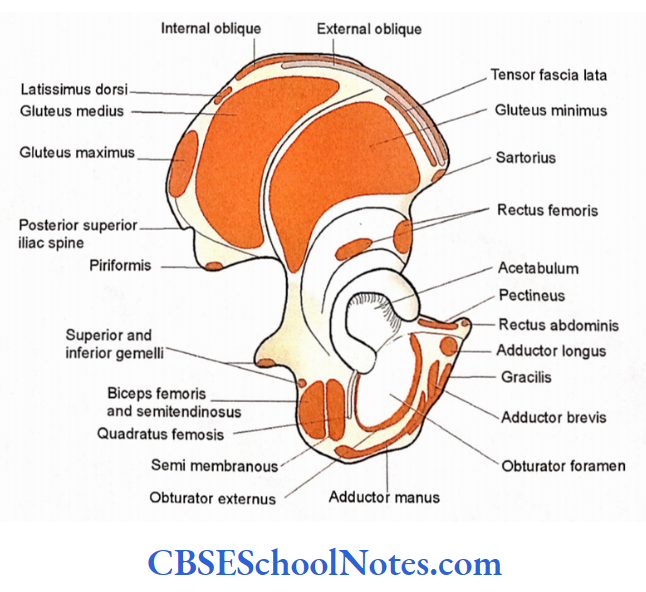
- The lateral surface of the dorsal segment of the iliac crest gives origin to the gluteus maximus muscle.
- The erector spinae arises from the medial surface of the dorsal segment of the iliac crest.
- Attachment of the Muscles on the Outer Surface (Gluteal Surface) of Ilium.
- The area behind the posterior gluteal line gives origin to the gluteus maximus.
- The area between anterior and inferior posterior gluteal lines gives origin to gluteus medius.
- The area between the anterior and inferior lines gives origin to the gluteus minimus.
- The area below the inferior gluteal line gives origin to the reflected head of the rectus femoris.
Attachment of Muscles on the Inner Aspect (Sacropelvic Surface and Iliac Fossa) of the Ilium
- The iliacus muscle arises from the upper 2/3rd of the iliac fossa.
- The pelvic part of the sapropelic surface of the vilium above the obturator foramen gives origin to the obturator internus muscle.
Muscles Attached to the Anterior Border and Sciatic Notch of the Ilium.
- The anterior superior iliac spine and an area below it give origin to the sartorius muscle.
- The straight head of the rectus femoris arises from the anterior inferior iliac spine.
- A small part of the piriformis arises from the upper border of the greater sciatic notch.
Pubis
Muscles Attached to the Pubic Bone
- The adductor longus muscle arises from a rounded tendon from the anterior surface of the body of the pubis.
- The origin of pyramidal is just above the origin of the adductor longus.
- Note the attachments of gracilis, adductor brevis, and obturator externus on the anterior surface of the body (from medial to lateral).
- These attachments also extend further downwards on the outer surface of the conjoined ischiopubic ramus.
- The obturator internus arises from the pelvic surface of the body and the superior and inferior ramus of the pubic bone.
- The pelvic (posterior) surface of the body gives origin to the anterior fibers of the levator ani.
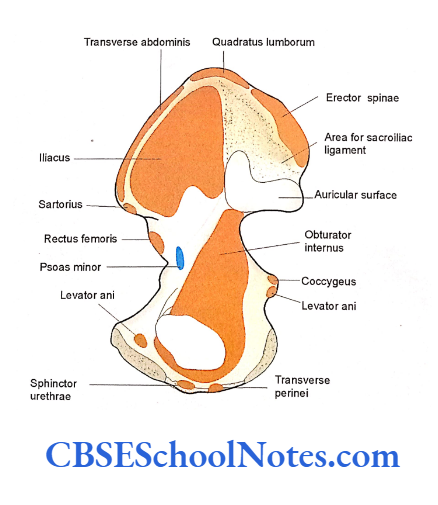
- The pectineus arises from the pectineal surface of the superior ramus of the pubis.
- Rectus abdominis arises from the pubic crest.
Ischium
Muscles Attached to Ischium
- Note the origin of superior and inferior gemelli concerning lesser sciatic notch.
- The quadratus fetnoris muscle arises from the femoral surface of the ischium.
- The obturator extemus arises from the body and ramus of ischium close to the obturator foramen.
- Posterior fibers of the levator ani and coccygeus muscles arise from the pelvic surface of the ischial spine.
- The origin of muscles from the ischial tuberosity. The adductor magnus arises from the lower lateral part of the ischial tuberosity. The origin also extends on the outer surface of the ramus of ischium.
- The semi-membranosus arises from the upper lateral part of the ischial tuberosity.
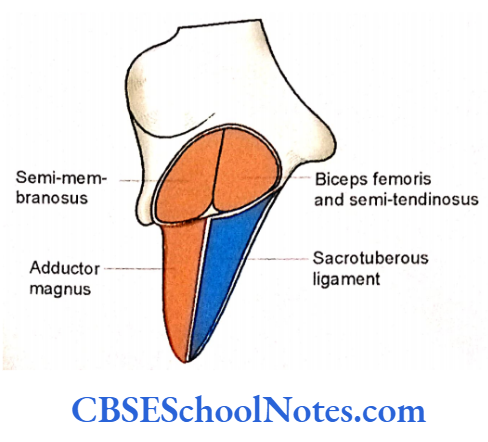
- The upper medial part of ischial tuberosity gives origin to the long head of the biceps fetnoris and Semitenditwsus.
Attachment of Ligaments and Fascia on the Hip Bone
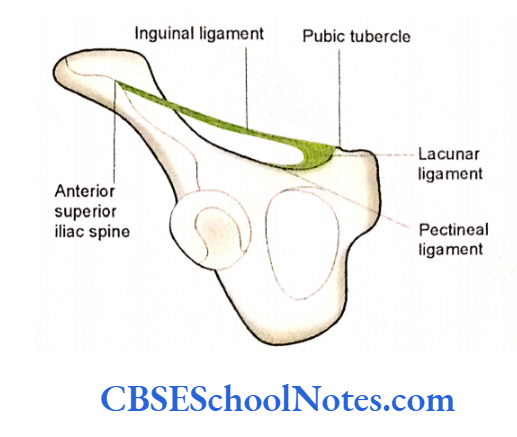
- The inguinal ligament is attached medially on the pubic tubercle and laterally on the anterior superior iliac spine.
- The conjoined tendon is attached to the pubic crest and pectin pubis.
- The lacunar ligament is attached to the pubic tubercle and pectin pubis.
- The anterior wall of the rectus sheath is attached to the pubic crest.
- The fascia lata is attached to the outer lip of the iliac crest, pubic crest, and lower border of the conjoined ischiopubic ramus.
- The anterior and middle layer of thoraco lumbar fascia is attached to the iliac crest, anterior and posterior to the attachment of the quadratus lumborum muscle.
- The superior and inferior fascia of the urogenital diaphragm are attached to the conjoined ischiopubic rami.
- The acetabular labrum is attached to the margin of the acetabulum.
- The iliac tuberosity (on the sapropelic surface) gives attachment to the dorsal and interosseous sacroiliac ligament.
- The posterosuperior and posteroinferior iliac spines and posterior border of the ilium give attachment to the upper end of the sacrotuberous ligament.
- The lower end of this ligament is attached to the medial margin of the ischial tuberosity.
- The sacrospinous ligament is attached to the ischial spine.
Blood Vessels and Nerves to the Hip Bone
- The pudendal nerve, nerve to the obturator interims, and internal pudendal vessels lie about the posterior surface of the ischial spine.
- The obturator vessels and nerve lie close to the inferior border of the superior ramus of the pubis (in the obturator canal).
- The superior gluteal vessels and nerves concern the gluteal surface of the ilium.
- The femoral surface of the body of the ischium is with the sciatic nerve and nerve to the quadratus femoris.
Ischium Ossification
The hip bone is organized by three primary centers. Many secondary centers appear at puberty and fuse with the rest of bone between 20 and 25 years of age (two secondary centers for iliac crest, two for acetabular cartilage, one for anterior inferior iliac spine, one for pubic tubercle, and one for pubic crest).

Clinical importance fractures
- Fractures of the hip bone are not very common. They may occur due to roadside accidents or due to sports injuries.
- The direct anteroposterior compression of the hip bone leads to a fracture of the pubic rami. Lateral compression may produce a fracture of the acetabulum.
- Similarly, a fall on the feet from a roof may lead to a fracture of the superior margin of the acetabulum.
- During sports, a sudden pull of muscles attached to anterior superior and inferior iliac spines, ischial tuberosity, and ischiopubic rami may lead to the tearing of these bony projections. These kinds of fractures are called avulsion fractures.
- In this kind of fracture, a small part of the bone with a piece of tendon or ligament attached is torn away.
Femur
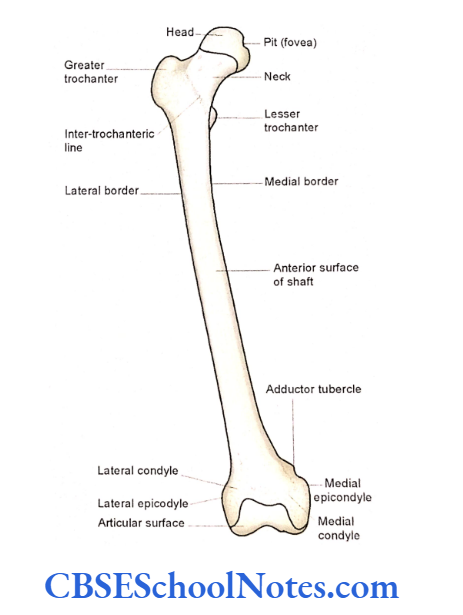
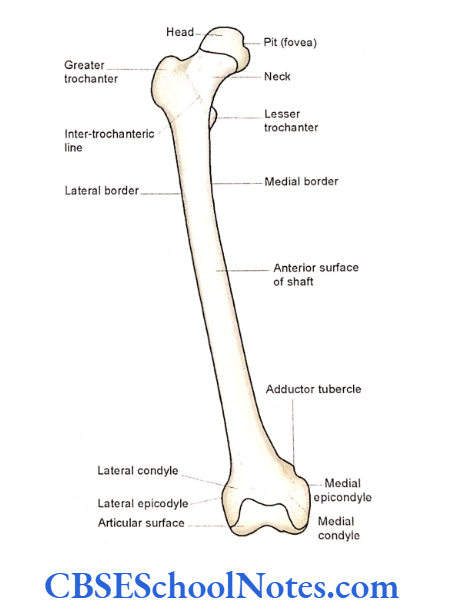
- The femur is the bone of the thigh region. It is the longest, strongest, and heaviest bone in the body. The femur consists of a shaft, an upper end, and a lower end.
- The upper end presents a rounded head, which articulates with the acetabulum of the hip bone to form a hip joint. The head is joined to the shaft by an elongated neck.
- The lower end of the femur is expanded and presents two condyles, i.e., medial and lateral, which articulate with tibia and patella to form the knee joint.
- The anterior surface of the shaft is smooth and convex forwards. There is the presence of a rough and thick vertical ridge (lined aspera) on the posterior aspect of the shaft.
Femur Side Determination
- The rounded head is the upper end of the bone.
- The head should be directed upwards, medially, and slightly forward.
- The smooth convex surface of the shaft should be directed forward.
Femur Anatomical Position
The shaft of the femur is obliquely placed (the lower end of the femur is directed downwards and medially).
Because the upper ends of two femora are widely separated by two hip bones two knee joints are placed close to each other when a person stands in the anatomical position.
As the female pelvis is broader the knee joints are more closely placed in females as compared to males.
- Keep the bone in such a way that the head faces upwards, medially, and slightly forwards.
- The long axis of the shaft should be directed downwards and medially so that the two lower surfaces of both the femoral condyles lie in the same horizontal plane.

Femur General Features
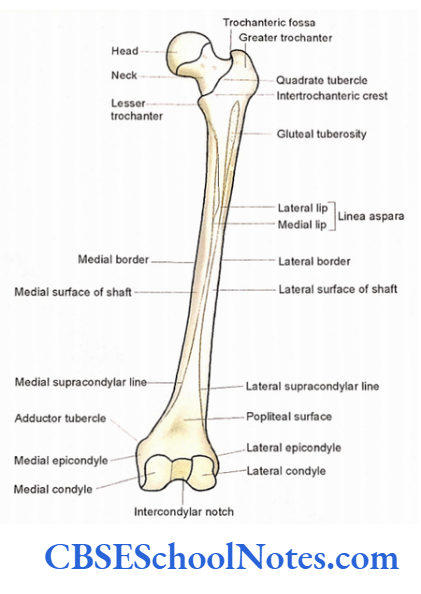
The Upper End
The proximal end of the femur consists of a rounded head, neck, and two trochanters (greater and lesser).
Femur Head
The head is like a ball, which forms about 2/3rd of a sphere. Near its middle, there is the presence of a pit for attachment of ligamentum teres.
Femur Neck
The neck connects the head to the shaft. The head and neck make an angle of about 126 degrees with the long axis of the body of the femur. The neck has a superior and an inferior border and an anterior and a posterior surface.
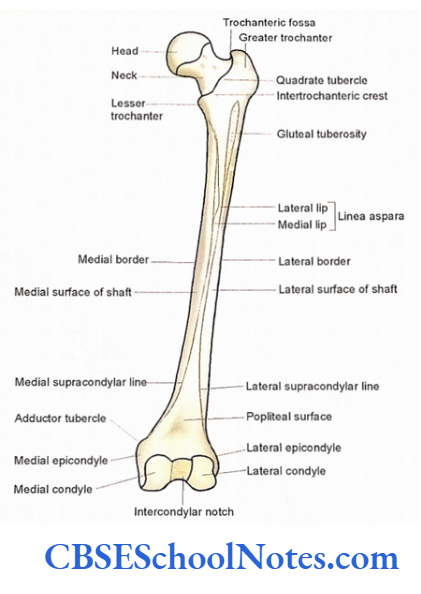
Femur Trochanters
Greater and lesser trochanters are two large elevations at the junction of the neck with the shaft. The greater trochanter is a large, laterally placed quadrilateral mass.
This trochanter presents three surfaces (anterior, medial, and lateral) and a superior and posterior border. The medial surface of the greater trochanter presents a deep depression called as trochanteric fossa. The lateral surface presents an oblique ridge that runs forward and downwards.
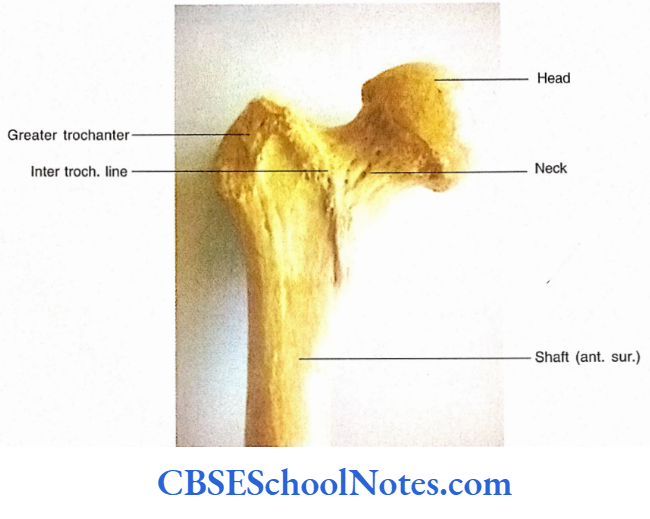
The lesser trochanter is a conical projection, directed medially and situated on the posteromedial surface at the neck-shaft The site where the neck joins the shaft, on the anterior aspect, is indicated by the presence of an intertrochanteric line.
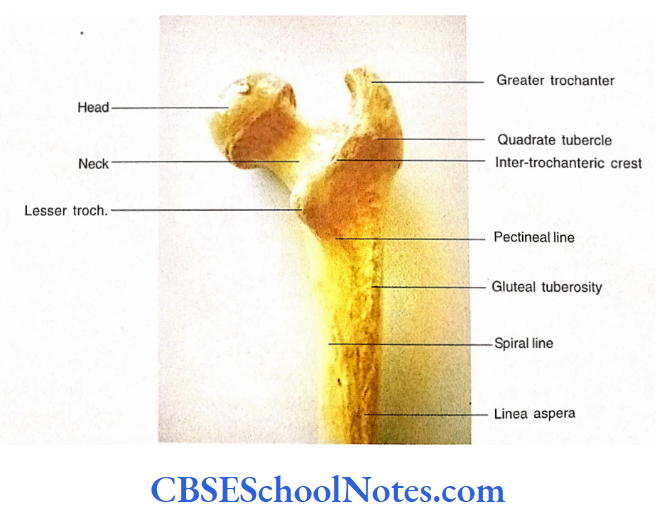
This rough line runs between greater and lesser trochanters. On the posterior aspect, a similar but smoother ridge joins two trochanters.
This is known as the intertrochanteric crest, which marks the junction of the neck with the shaft posteriorly. The middle of the intertrochanteric crest presents a quadrate tubercle.
The Shaft
The shaft or body of the femur shows a slight bowing anteriorly. The shaft is narrowest in the middle but expanded towards the upper and lower ends.
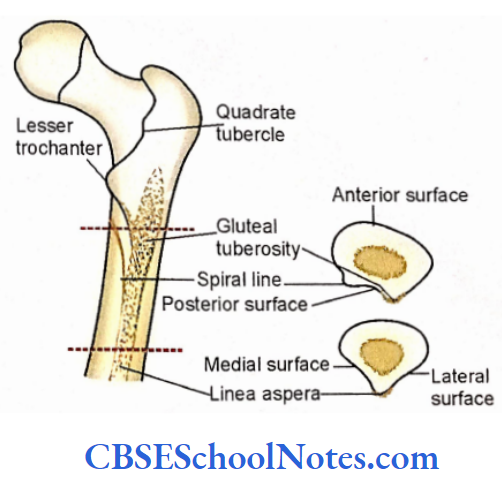
- The shaft presents three surfaces (anterior, medial, and lateral) separated by three borders (medial, lateral, and posterior).
- The medial and lateral borders are rounded and featureless.
- The posterior border or linen aspera is a broad, rough vertical ridge.
- As the linea aspera is broad in the middle part of the shaft it presents a medial lip, a lateral lip, and an intermediate area.
- When the linea aspera is traced upwards its lateral lip continues as broad rough gluteal tuberosity and the medial lip continues as a narrow rough spiral line.
- The upper end of gluteal tuberosity extends upto the greater trochanter.
- There lies a small triangular surface (posterior surface) between the gluteal tuberosity and spiral line in the upper third of the shaft.
- When the linea aspera is traced downwards its medial lip continues below as medial supracondylar line.
- Similarly, the lateral lip of linea aspera continues below a lateral supracondylar line. The triangular surface between these two lines is called as popliteal surface.
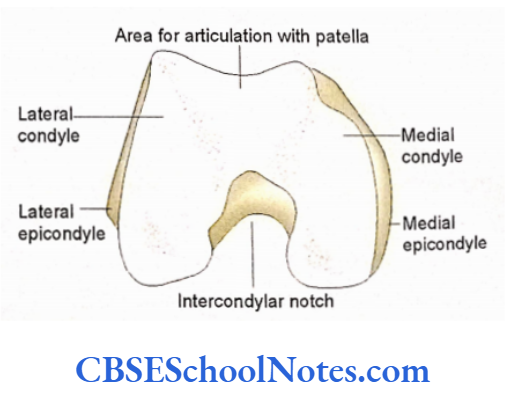
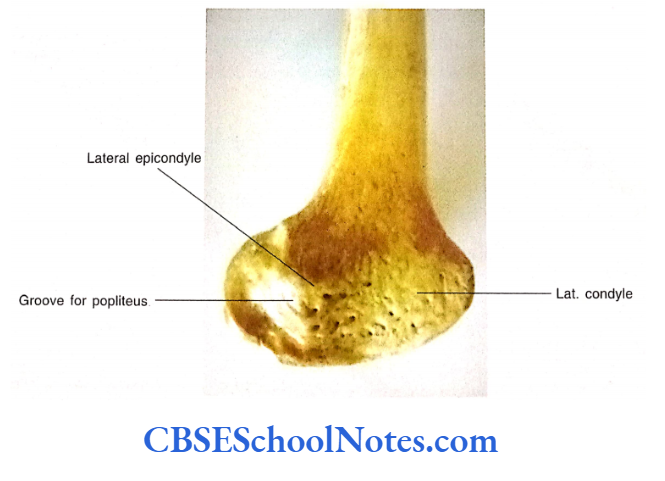
Lower End
The lower expanded end of the femur consists of medial and lateral condyles, intercondylar fossa, and articular surfaces (tibial and patellar) for articulation with the tibia and patella.
Two condyles are joined together anteriorly but separated posteriorly by the intercondylar fossa or notch.
- Both the condyles of the femur articulate with the corresponding condyles of the tibia and patella to form the knee joint.
- Each condyle presents five surfaces, i.e., anterior, posterior, medial, lateral, and inferior.
- The anterior surfaces of two condyles present an articular patellar surface. It articulates with the posterior surface of the patella.
- The outer surface of both the condyles (medial surface of medial condyle and lateral surface of lateral condyle) is rough and convex.
- The prominent bony points on the outer surfaces of both condyles are called epicondyles.
- An adductor tubercle is present postero-superior to the medial epicondyle at the lower end of the medial supracondylar ridge.
- The inner surface of both the condyles, i.e., the lateral surface of the medial condyle and the medial surface of the lateral condyle form the medial and lateral walls of the intercondylar fossa.
- The inferior and posterior surfaces of both the condyles are articular and articulate with tibia. Anteriorly, the tibial articular surfaces of both condyles are continuous with the patellar surface.

Femur Particular Features
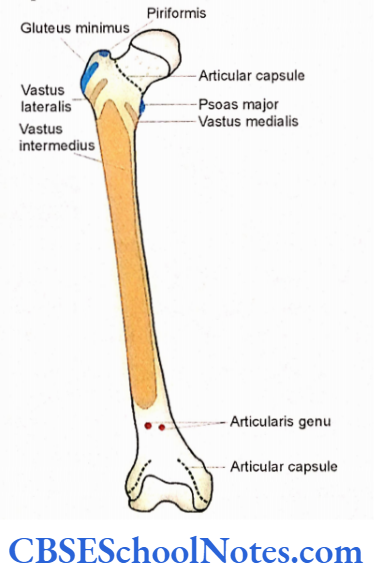
- Muscles Attached to the Upper End of the Femur
- The obturator interims and two Gemelli are inserted on the medial surface of the greater trochanter.
- The obturator externus is attached into the trochanteric fossa.
- The piriformis is inserted on the upper border of the greater trochanter.
- The gluteus minimus is inserted on the anterior surface of the greater trochanter.
- The gluteus medius is inserted on the lateral aspect of the greater trochanter.
- The psoas major is inserted on the lesser trochanter.
- The quadratus femoris is attached to the quadrate tubercle.
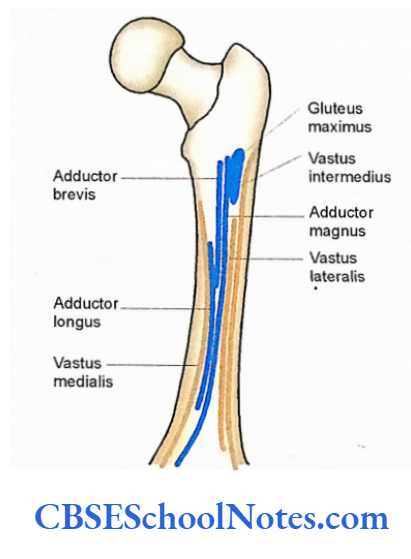
Muscles Attached to the Shaft of the Femur
- The iliacus and pectineus are inserted just below the lesser trochanter.
- The insertion of pectineus lies between the gluteal tuberosity and the spiral line.
- A part of the gluteus maximus is inserted on the gluteal tuberosity.
- The vastus medialis has a linear origin, i.e., from the lower part of the intertrochanteric line, spiral line, the medial lip of linea aspera, and upper 2/3rd of the medial supracondylar line.
- Similarly, the origin of vastus lateralis is also linear. It arises from the upper part of the intertrochanteric line, greater trochanter, lateral margin of the gluteal tuberosity, and lateral lip of linea aspera.
- The vast intermediate originates from the anterior and lateral surfaces of the shaft.
- Students should note the attachments of the following structures on the linea aspera, from medial to lateral side, with the help.
- The vastus mediaiis on the medial lip, medial intermuscular septum, adductor brevis (above) adductor longus (below), adductor magnus, posterior intermuscular septum, short head of biceps femoris, lateral intermuscular septum and vastus lateralis.
Muscles attached to the lower end of the femur
- The popliteus muscle takes its origin from the groove present below the lateral epicondyle.
- The medial head of the gastrocnemius arises from the popliteal surface above the medial epicondyle.
- The lateral head of the gastrocnemius arises from the lateral surface of the lateral condyle.
- The lower part of the lateral supracondylar line gives origin to the plantaris.
- The adductor magnus is inserted on the medial supracondylar line.
- The tendon of the ischial part of the adductor magnus is attached to the adductor tubercle.
Attachments of Ligaments and Intermuscular Septa on the Femur A Few important ligaments and septa are described below:
- The pit or fovea on the head of the femur gives attachment to the ligamentum teres.
- The medial intermuscular septum is attached to the medial lip of linea aspera and the lateral septum is attached to the lateral lip.
- The posterior intermuscular septum is attached to the intermediate area of linea aspera.
- The posterior cruciate ligament is attached to the lateral surface of the medial condyle.
- The anterior cruciate ligament is attached to the medial surface of the lateral condyle.
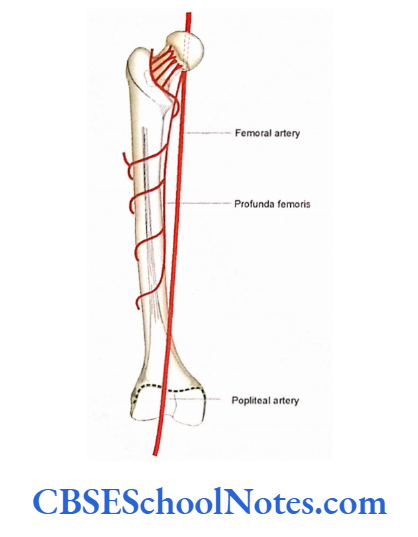
Blood Vessels Concerning the Bone
- The femoral artery lies anterior to the head of the femur.
- The popliteal artery lies on the popliteal surface of the bone.
- Any major nerve is not directly related to the femur.
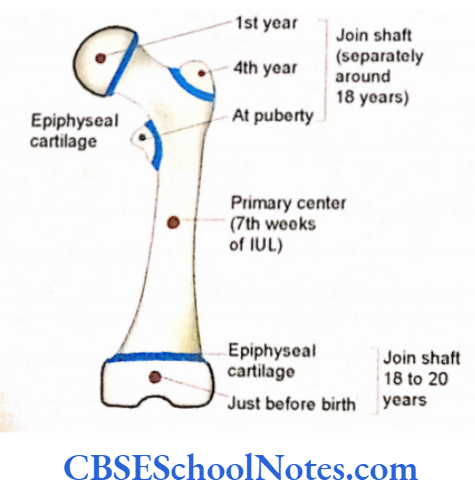
Femur Ossification
The femur ossifies by one primary and four secondary centers (three for the upper end and one for the lower end. The lower end is the growing end of the femur.
Clinical importance
- The secondary center for the lower end appears just before birth (ninth months of intrauterine life).
- The presence of this center indicates that the fetus is mature (viable) enough to survive after birth.
- The above fact is used as medicolegal evidence in case if a newborn infant found dead was capable of living at birth or not.
- The fracture of the neck of the femur is common in old people, especially in females.
- The fracture through the neck of the femur is also associated with the injury to blood vessels lying on the surface of the neck.
- These vessels are responsible for the blood supply of the head. Rupture of these blood vessels leads to degeneration of the femoral head (avascular necrosis of the head).
- Fracture of the femur between greater and lesser trochanter is also common in old persons.
- Fracture of the shaft is usually a clue to direct injury as in vehicle accidents.
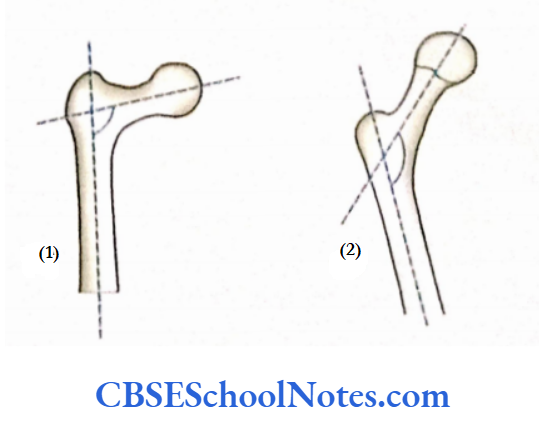
- If the angle of inclination (the angle between the long axis of the body and the long axis of the neck) is reduced then the condition is called coxa vera.
- If this angle is increased the condition is called coxa valga. The normal angle is about 125.
Tibia
- The skeleton of the leg is formed by two long bones, i.e., the tibia and fibula.
- The tibia is the medial weight-bearing bone of the leg. It consists of an upper end and a lover end and a shaft or body. The upper end of the tibia is expanded and bears medial and lateral condyles.
- These condyles articulate with the lower end of the femur to form the knee joint.
- The lower end of the tibia on its medial aspect bears a downward projection called medial malleolus.
- The shaft or the body of the bone bears a prominent sharp ridge known as an anterior border. The upper end of the anterior border bears a projection called tibial tuberosity.
Tibia Side Determination
- The expanded upper end (bearing medial and lateral condyles) should be directed upwards.
- The sharp and prominent anterior border and the tibial tuberosity should be placed anteriorly.
- Medial malleolus at the lower end should face medially.
Tibia Anatomical Position
Bone should be kept vertically by holding it in the same hand, to the side it belongs.
Tibia General Features
Tibia Upper End
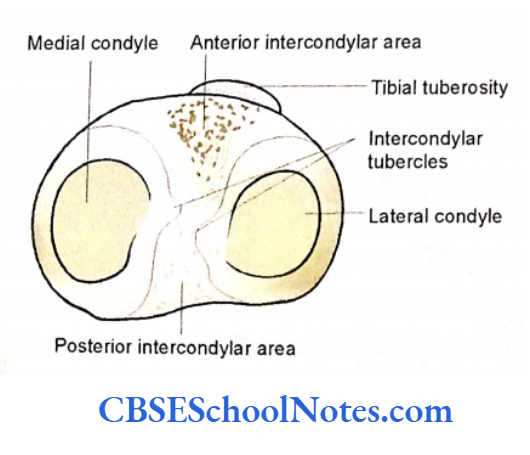
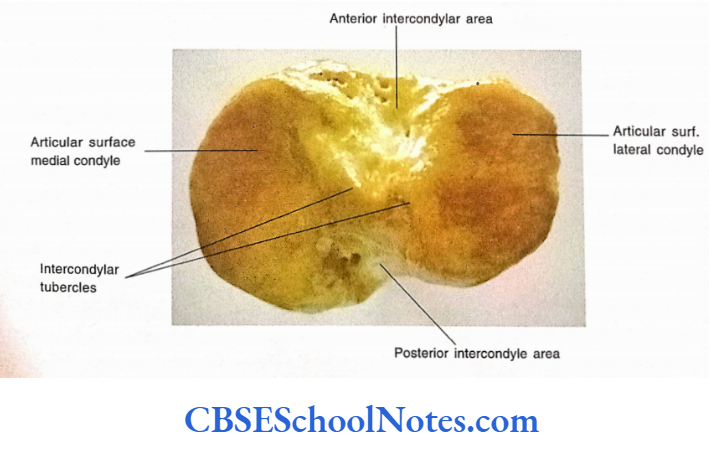
- The upper end consists of medial and lateral condyles, an intercondylar area, and a tibial Shaft tuberosity.
- The upper surface of the medial and lateral condyles is articular.
- The articular surface of the medial condyle is oval and large while that of the lateral condyle is small and circular.
- A non-articular rough area is placed between two articular surfaces. This is known as the intercondylar area.
- There is the presence of an elevation in the middle of the intercondylar area (intercondy- lar eminence). This eminence is formed by two tubercles, i.e., medial and lateral intercondylar tubercles.
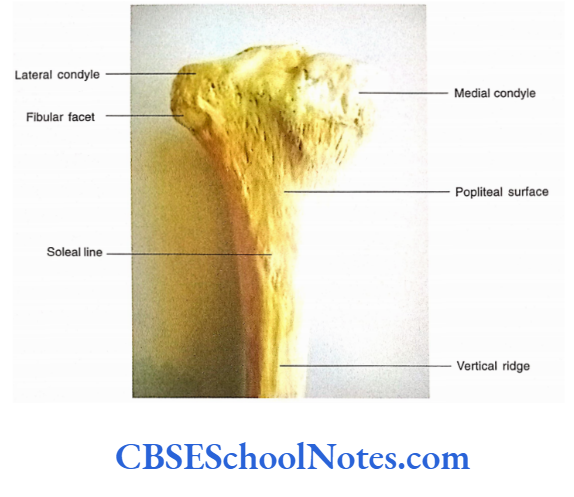
- The posterior surface of the medial condyle is deeply grooved.
- The posterolateral surface of the lateral condyle bears a circular articular facet for the head of the fibula. This articulation is known as the superior tibio-fibular joint.
- The anterior surface of both condyles bears a triangular area. The apex of this triangle is directed downwards and there lies a rough projection called tibial tuberosity.
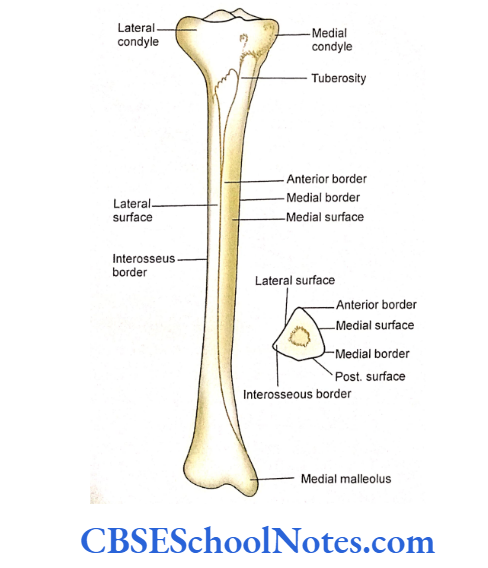
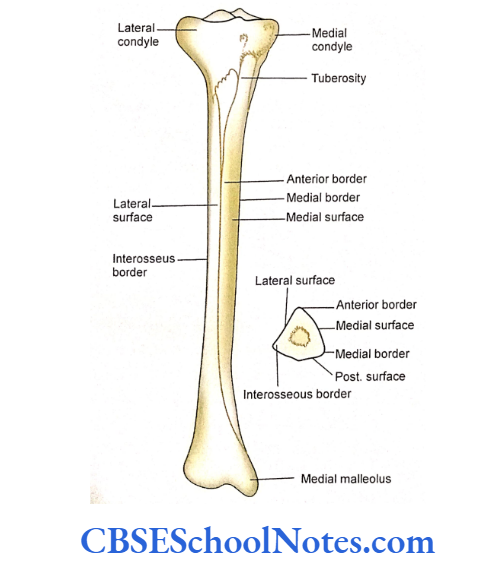
- The shaft of the tibia is triangular in cross-section, hence presenting three borders (anterior, medial, and lateral or interosseous) and three surfaces (medial, lateral, and posterior).
- The anterior border extends from the tibial tuberosity to the anterior margin of the medial malleolus. It is a sharp, subcutaneous border.
- The medial border extends from the medial condyle to the posterior border of the medial malleolus.
- The lateral or interosseous border extends from the lateral condyle to the anterior border of the fibular notch at the lower end of the tibia.
- The lateral surface lies between the anterior and interosseous borders.
- The medial surface lies between the anterior and medial borders. This surface is smooth because it is subcutaneous.
- The posterior surface lies between medial and lateral borders. This surface is marked by the presence of an oblique sole line. Thus posterior surface presents a triangular area above the sole line and a medial and a lateral area below the sole line
Tibia Lower End
- This end of the tibia is much less expanded as compared to the upper end. This end projects downwards and medially as the medial malleolus.
- The posterior surface of the malleolus presents a groove. The lateral surface of the lower end shows a triangular area (fibular notch) for articulation with the fibula to form an inferior tibiofibular joint.
- The inferior surface of the lower end including the medial malleolus is articular and articulates with the body of the talus to form the ankle joint.
Tibia Particular Features
Attachment of Muscles on Tibia
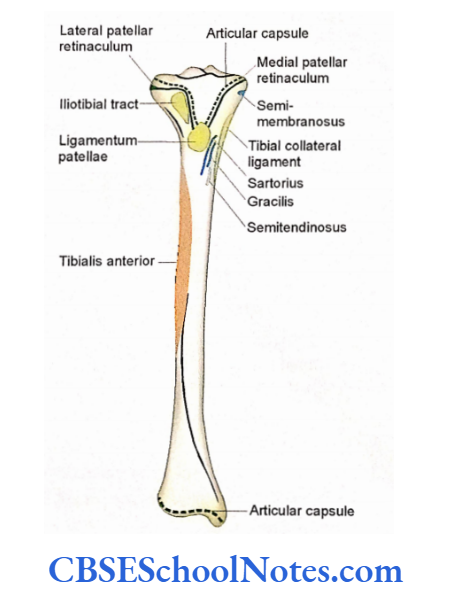
- The tibial tuberosity gives attachment to the lignmentum patellae (tendon of quadriceps femoris).
- The semi-membranosus is inserted in the horizontal groove on the posterior surface of the medial condyle.
- The upper part of the media surface receives the insertion of three muscles from before backward, i.e., sartorius, gracilis, and semitendinosus.
- The upper 2/3rd of the lateral surface gives origin to the tibialis anterior.
- On the posterior surface of the bone, the popliteus is inserted above the sole line.
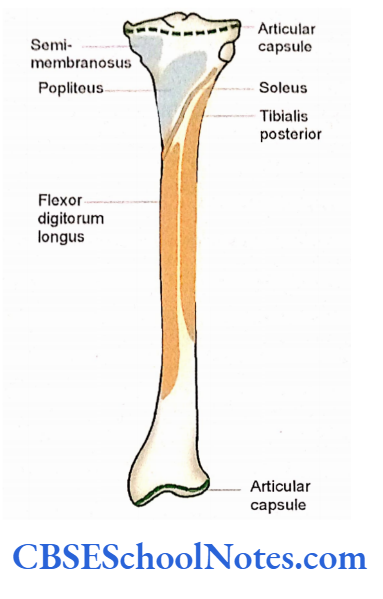
- The sole line itself gives origin to the soleus muscle.
- The medial area below the soleal line, on the posterior surface, gives origin to the flexor digitorum longus. While the lateral area gives origin to the tibialis posterior.
Attachment of Ligaments on the Tibia
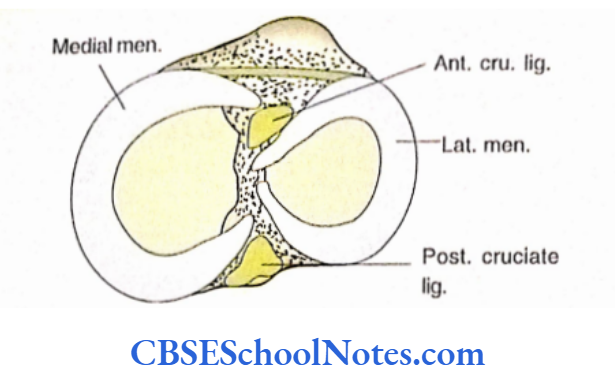
- The anterior and posterior parts of the intercondylar area give attachment to the following structures from before backward anterior horn of medial meniscus, anterior cruciate ligament, anterior horn of lateral meniscus, posterior horn of lateral meniscus, posterior horn of medial meniscus, and posterior cruciate ligament.
- The lower end of the iliotibial tract is attached to a small triangular area on the anterior surface of the lateral condyle.
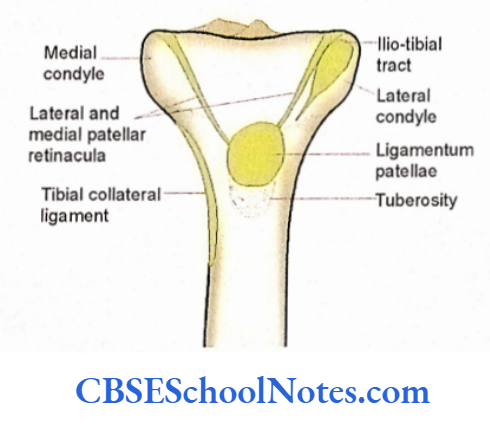
- The tibial collateral ligament is attached to the medial surface near the upper end of the medial border.
- The interosseous or lateral border gives attachment to interosseous membrane.
- The fibular notch gives attachment to the interosseous tibiofibular ligament.
Tendons, Blood Vessels, and Nerves Related to Tibia
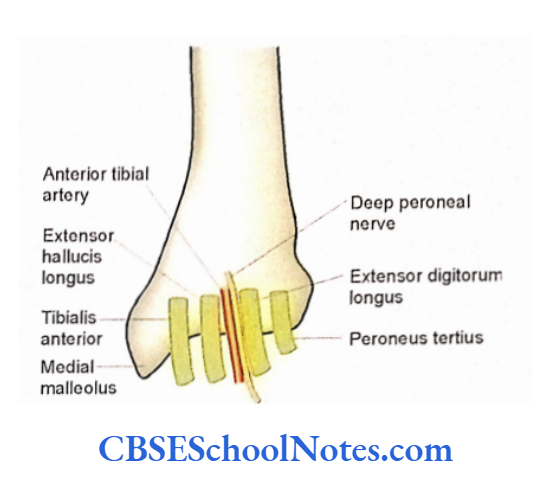
Following tendons, vessels, and nerves are related on the anterior aspect of the lower end (from medial to lateral): tibialis anterior, extensor hallucis longus, anterior tibial vessels, deep peroneal nerve, extensor digitorum longus, and peroneus tertius.
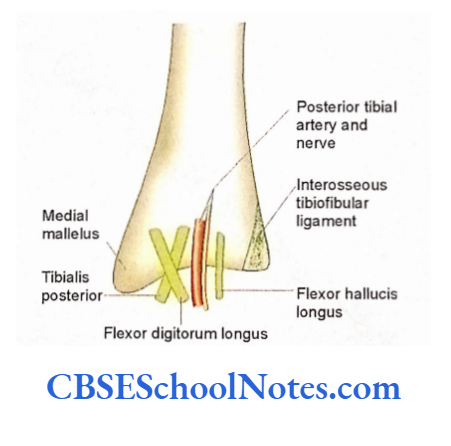
Following tendons, vessels, and nerves are related to the posterior aspect of the lower end of the tibia (from medial to lateral side): tibialis posterior, flexor digitorum longus, posterior tibial vessels, posterior tibial nerve, and flexor hallucis longus.
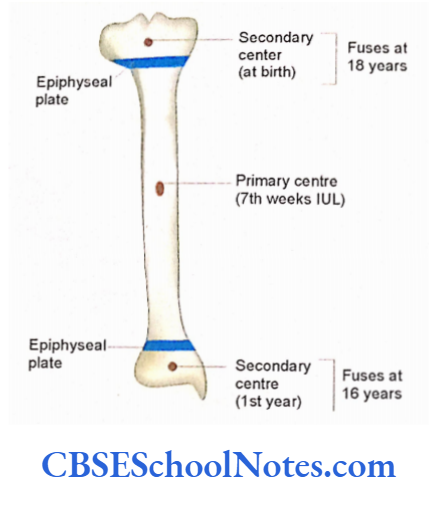
Tibia Ossification
Tibia ossifies from three centers, i.e., one primary center for the shaft and two secondary centers one each for the upper and lower end. The upper end is the growing end of the tibia.
Tibia Clinical importance
- The most common site for the fracture of the tibia is at the junction of the middle and lower 1/3rd.
- This is because the tibia is narrowest at this point. The fracture of the lower 1/3rd of the tibia is difficult to heal as this part of the tibia is devoid of muscle attachment and the periosteal blood supply is poor.
- The tibia is subjected to severe torsion during various sports, which may lead to diagonal fracture of the tibial body. The body of the tibia is also the most common site for compound fracture.
- In a compound fracture, blood vessels and skin are torn by the fractured end of the tibia. This is because the tibia is subcutaneous hence skin is easily torn.
Fibula
The fibula is the lateral bone of the leg. Though the slender fibula has no weight-bearing function, but gives attachment to muscles and its lower end (lateral malleolus) takes part in the formation of the ankle joint.
The fibula has an upper end, a lower end, and an intervening shaft.
The upper rounded end is also known as the head. The head bears a styloid process and an oval articular surface for articulation with the lateral condyle of the tibia.
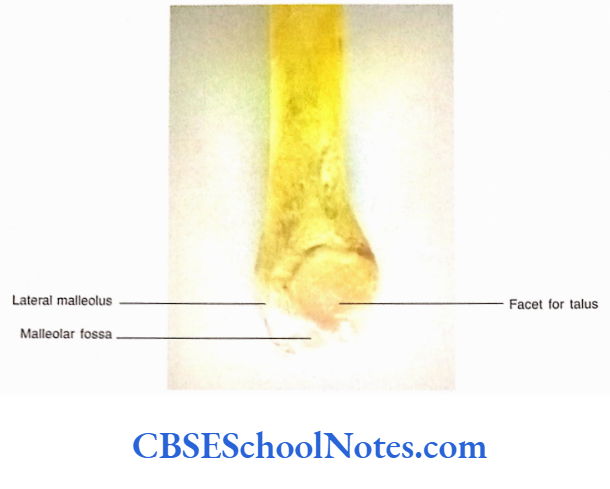
The lower end of the fibula is expanded anteroposteriorly to form the lateral malleolus.
The medial surface of the lower end presents a triangular articular surface front and a depression, the malleolar fossa, just posteroinferior to the triangular articular surface.
Fibula Side Determination
The side of the fibula can be determined just by looking at its lower end Keep the lower end (lateral malleolus) downwards.

- The triangular articular surface of the lateral malleolus should face medially.
- The malleolar fossa should face downwards, backward, and medially.
Fibula Anatomical Position
Once you have determined the side of the bone then hold the bone vertically in the hand of the same side to which it belongs.
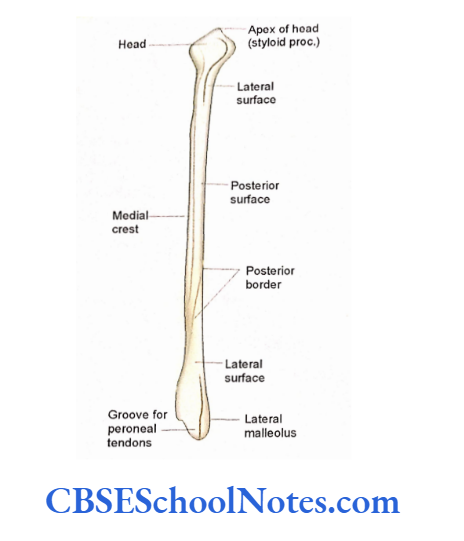
Fibula General Features
Upper End or Head
- It has a pointed apex known as the styloid process.
- The superior surface of the upper end bears an oval articular facet.
- The neck is the constricted part of the bone just below the head.
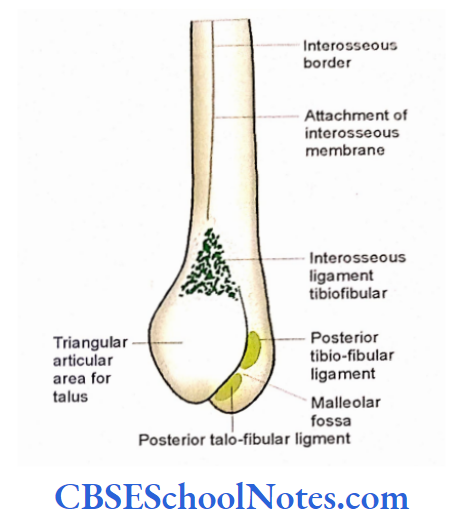
Lower The End lateral Lateral malleolus
- The malleolus presents lateral, medial, and posterior surfaces and an anterior border.
- The lateral surface is convex, triangular, and continuous above with anterior border. It is a subcutaneous surface.
- The medial surface bears a triangular articular facet for the articulation with the talus.
- Behind the facet there is a rough depression called a malleolar fossa.
- The posterior surface presents a groove for the tendon.
Shaft
The shaft of the fibula has three borders (anterior, interosseous, and posterior) and three surfaces (medial, lateral, and posterior).
(As the borders and surfaces of fibula are difficult to identify, take the help of your teacher. Hold the bone in the anatomical position and trace these borders as described below).
Anterior Border
It begins just below the anterior surface of the head. Trace this sharp border downwards near the lower end of the bone this border splits to enclose a subcutaneous triangular surface on the lateral aspect of the lateral malleolus.
Interosseous Border
- This border is very close and medial to the anterior border.
- It begins just below the anterior surface of the head. When traced downwards it passes medially to end in a rough triangular surface on the medial surface of the lower end.
Posterior Borders
It extends from the posterior aspect of the head to the lateral lip of a groove on the posterior aspect of the lateral malleolus.
Medial (Extensor) Surface It is a very narrow surface and lies between anterior and interosseous borders. It is also known as the anterior surface.
Lateral (Peroneal) Surface It lies between anterior and posterior borders. At the lower end, this surface becomes continuous with the posterior aspect of the lateral malleolus
Posterior (Flexor) Surface
It lies between the interosseous and the posterior border. This surface in its upper 2/3rd is divided into medial and lateral parts by a sharp vertical ridge called as medial crest, of
Attachment of Intermuscular Septum
- The anterior and posterior borders give attachment to the anterior and posterior intermuscular septum.
- The interosseous border gives attachment to the interosseous membrane.
- The medial crest gives attachment to the transverse intermuscular septum.
Attachment of Muscles on Fibula
The medial or extensor surface gives origin to three muscles, i.e., the extensor digitorum.
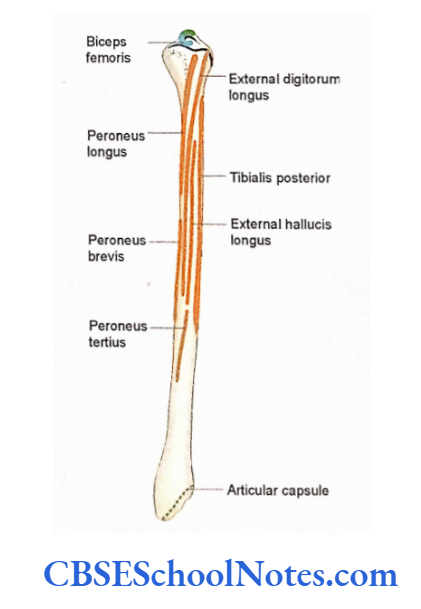
- longus (from its upper 3/4th surface), extensor hallucis longus (from its middle 2/ 4th), and peroneus tertius from the lower 1 /4th below the origin of extensor digitorum longus.
- The posterior surface gives origin to the tibialis posterior from the anterior concave surface lying anterior to the medial crest.
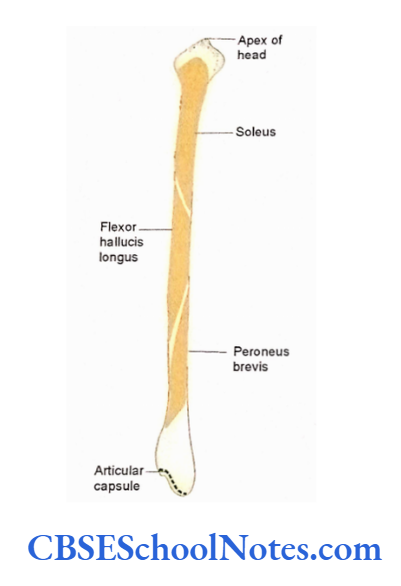
- The surface posterior to the medial crest gives origin to the soleus in the upper 3/4th and flexor hallucis longus from its lower 3/4th.
- The lateral surface gives origin to the peroneus longus from its upper 3/4th and peroneus brevis from its lower 2/3rd. In the middle third of this surface peroneus brevis lies in front of peroneus longus.
- The lower end of the fibula is devoid of muscular attachments
Tendons and Nerves with Fibula
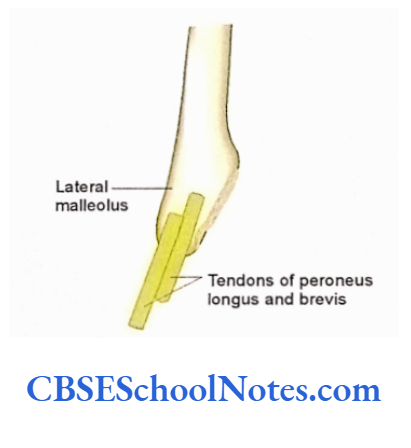
- The tendon of the peroneus longus and brevis are related to the posterior surface of the lateral malleolus.
- The common peroneal nerve is related to the lateral aspect of the neck of the fibula.
Fibula Ossification
The fibula is organized by three centers. One primary center for the shaft and two secondary centers, one each for the upper and lower ends.
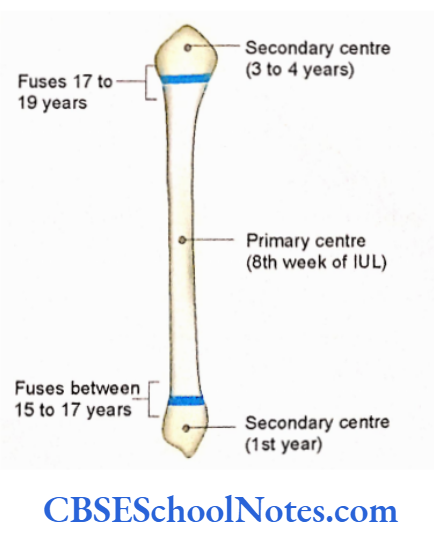
The fibula is an exception to the law of “growing end” (i.e., the secondary center, which appears first is also the first to fuse with the bone formed by the primary center).
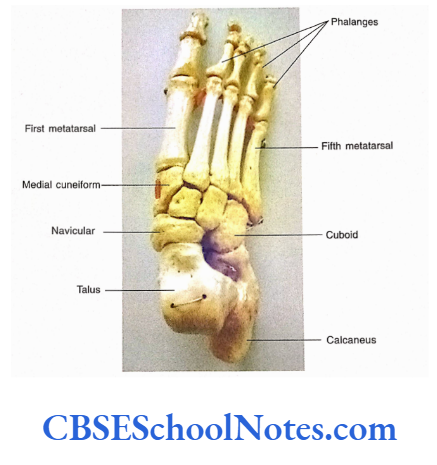
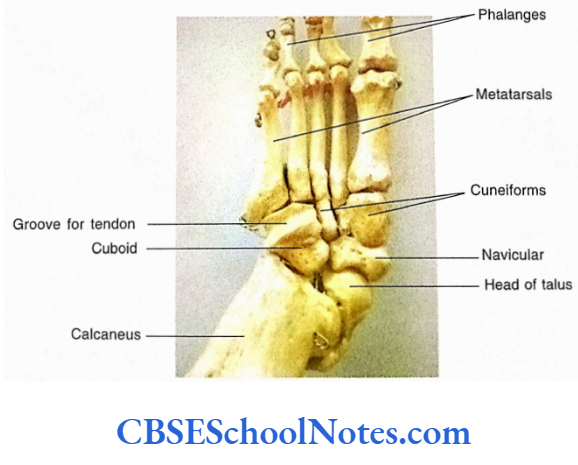
Bones Of The Foot
- The bones of the foot consist of tarsus, metatarsus, and phalanges. Each foot consists of 7 tarsal, 5 metatarsal, and 14 phalanges, which are arranged proximodistally.
- Though we shall study the features of individual bones of the foot students are advised to study an articulated skeleton of the foot to see the arrangement of these bones with each other.
- In my opinion, undergraduate students, need not study every bone of the foot in detail. Therefore, only two tarsal bones (calcaneus and talus) are described in detail.
Tarsal Bones
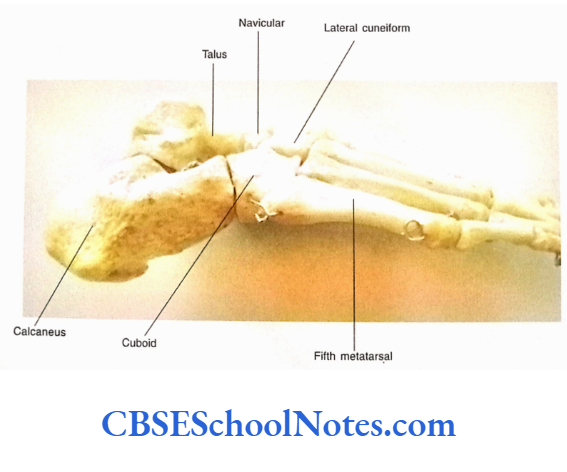
- These are short bones, which form the posterior half of the foot. They are arranged in three rows. The proximal row consists of the talus and calcaneus.
- The calcaneus is the largest tarsal bone and forms the heel of the foot. Placed above the anterior 2/3rd of the calcaneus.
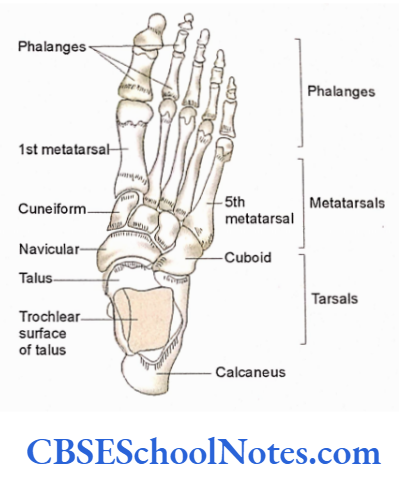

There is another tarsal bone called a talus. The talus articulates with the lower end of the tibia and fibula to form the ankle joint. Anterior to the calcaneus and talus, the middle row is formed by navicular and cuboid bones.
The proximal end of the navicular bone articulates with the head of the talus and is placed medially.
The cuboid bone is placed laterally and articulates proximally with the calcaneus.
The distal surface of the navicular bone articulates with the other three tarsal bones, i.e., medial, intermediate, and lateral cuneiforms.
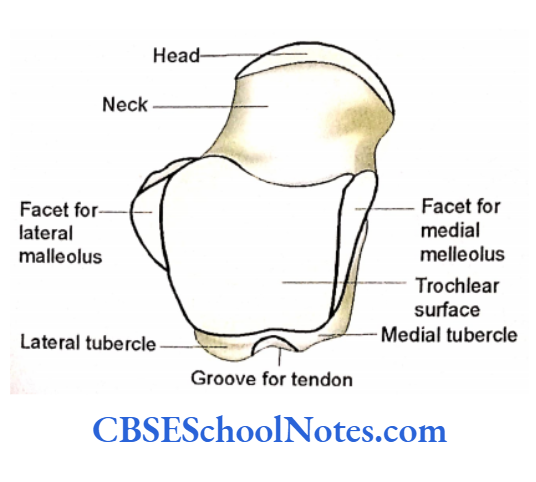
Talus
The talus has a body, neck, and head. It is situated on the calcaneus.
Body
- The superior surface of the body is articular and bears a large trochlear articular surface for articulation with the lower end of the tibia.
- The medial surface of the body shows a comma-shaped articular facet for articulation with the medial malleolus. While the lateral surface bears a large triangular facet for articulation with the lateral malleolus of the fibula.
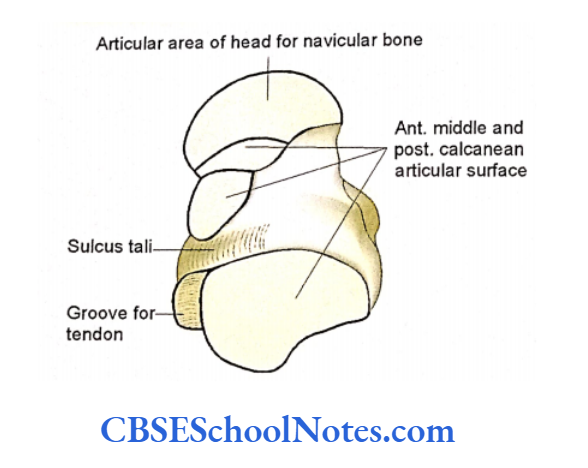
- The inferior surface of the body of the talus presents a concave facet, which articulates with the convex facet on the upper surface of the middle third of the calcaneus to form the talar joint.
- The posterior surface is narrow and has a groove for a tendon. This groove has a prominent lateral tubercle and a less prominent medial tubercle.
Neck
The neck of the talus projects forward and medially from the body of the talus. It is nonarticular and bears a groove (sulcus tali) on its inferior surface.
Head
The rounded head is directed forwards, medially, and slightly downwards. The head bears an extensive convex articular surface, which articulates anteriorly with the navicular bone and below with the upper surface of the sustentaculum tali of the calcaneus and spring ligament.
The talus is the only tarsal bone that has no muscular or tendinous attachments. The sulcus tali gives attachment to the interosseous talocalcanean ligament.
Talus Side Determination
- The rounded articular head should be directed forward.
- The large trochlear articular surface should face upward.
- The large triangular articular surface placed on the side of the body should face laterally.
Talus Anatomical Position
Hold the bone in such a way that the head is directed forwards, medially, and slightly downwards.
Calcaneus
The calcaneus is the largest and strongest tarsal bone of the foot. It forms the heel and is located below the talus.
It articulates superiorly with the talus and anteriorly with the cuboid bone. The calcaneus has six surfaces.
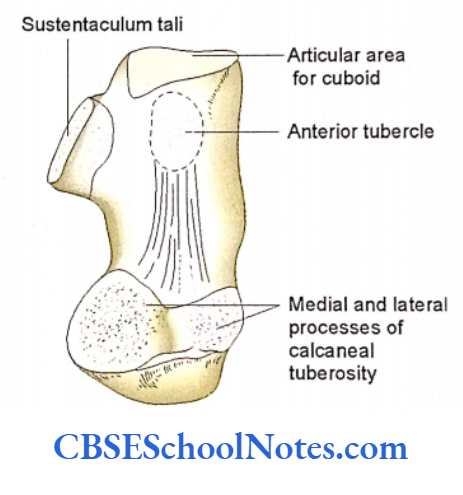
The anterior surface is articular and saddle in shape. It articulates with the cuboid bone.
The posterior surface is non-articular and roughing its middle part for the attachment of tendocalcaneus.
The medial surface is concave and bears a shelflike projection called sustentaculum tali.
The lateral surface of the calcaneus is flat and bears a peroneal tubercle.
The plantar or inferior surface of the calcaneus is rough and shows a large prominence on its posterior part called as calcaneal tuberosity.
The calcaneal tuberosity presents medial and lateral tubercles. The anterior part of the plantar surface bears an anterior tubercle.
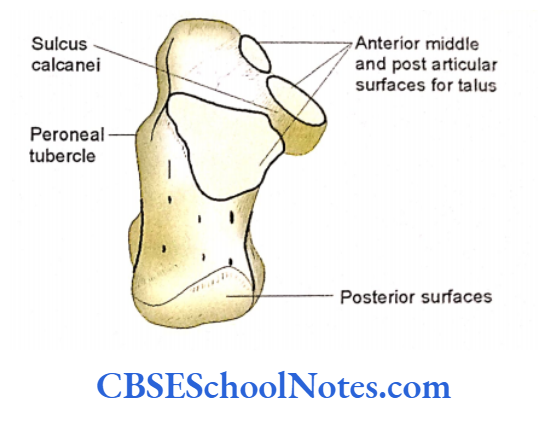
The dorsal or superior surface is partly articular and partly non-articular. It bears three articular facets (anterior, middle, and posterior facets) for articulation with the corresponding facets on the inferior surface of the talus.
There is the presence of a deep groove between the middle and posterior facets, sulcus calcanei. The sulcus calcanei and sulcus tarsi, in an articulated foot, form sinus tarsi.
Calcaneus Side Determination
- The anterior articular surface should face anteriorly.
- The superior surface bearing three articular facets should face upward.
- The sustentaculum tali projects medially.
Calcaneus Anatomical Position
Hold the bone in such a way that the articular area for the cuboid should face forward and laterally with a slight upward inclination.
Navicular
The navicular bone is boat-shaped. It articulates distally with the head of the talus and proximally with three cuneiforms. The medial surface of the bone bears a navicular tuberosity.
Cuboid
It is the lateral bone extending in the distal row of the tarsus. It is approximately cubical. Proximally it articulates with calcaneus and distally with the 4th and 5th metatarsals.
On the lateral and inferior aspect, it bears a groove for the tendon of the peroneus longus. On this aspect, behind the groove, there is the presence of tuberosity.
The medial surface of the cuboid has articular facets for lateral cuneiform and navicular bone.
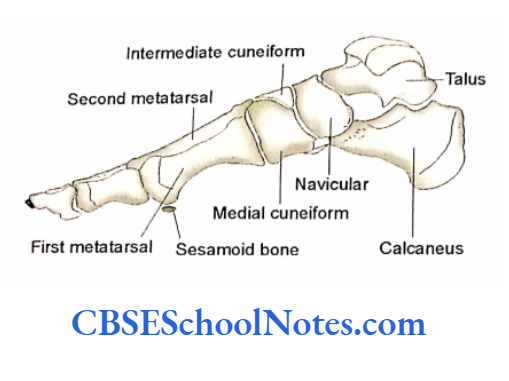
Cuneiform Bones
These are called medial, intermediate, and lateral cuneiforms. These bones articulate with the navicular proximally and with the bases of the 1st, 2nd, and 3rd metatarsals distally.
All these bones articulate with each other. The lateral surface of lateral cuneiform also articulates with the cuboid.
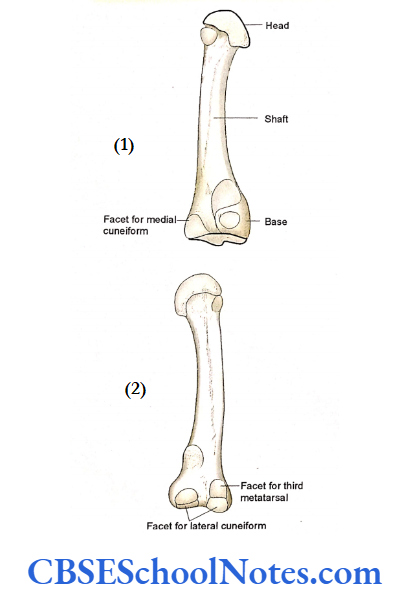
The metatarsal bones
- The metatarsals are classified as miniature long bones. The five metatarsal bones are numbered from medial to lateral side, i.e., 1st, 2nd, etc. The first metatarsal is the shortest and strongest as compared to the others.
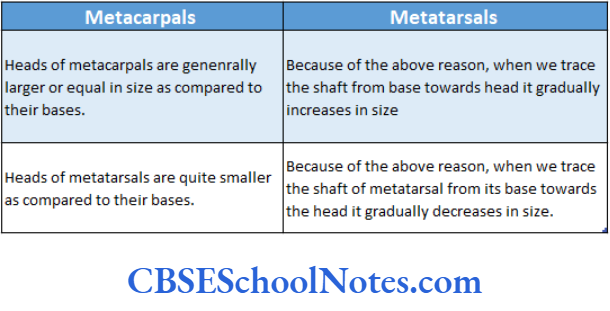
- The second metatarsal is the longest. Each metatarsal has a proximally placed base, distally placed head, and intervening body. The heads of metatarsals are rounded and articulate with the proximal phalanges.
- The base of each metatarsal is large as compared to its head and presents five surfaces (medial, lateral, dorsal, plantar, and proximal).
- The base of 5th metatarsal has a large tuberosity for the insertion of the tendon of the peroneus brevis.
Phalanges
- Similar to the metatarsals, phalanges are also classified as miniature long bones. The first toe has two phalanges (proximal and distal).
- The lateral four toes have three phalanges each, i.e., proximal, middle, and distal. Each phalanx consists of a proximally placed base, a distally placed head, and an intervening body.
- The first toe consists of two phalanges and has only one interphalangeal joint. While the rest of the toes have proximal and distal interphalangeal joints.
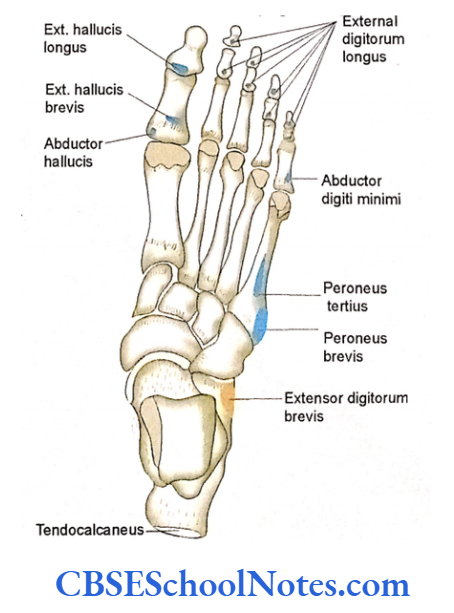
Particular Features Of The Bones Of The Foot
- The peroneus brevis is inserted on the lateral aspect of the base of the fifth metatarsal bone.
- The peroneus tertius is attached to the dorsal aspect of the base of the fifth metatarsal.
- The extens or digitorum longus is attached to the base of the middle and distal phalanges of the lateral four toes.
- The extensor hallucis longus is inserted on the base of the distal phalanx of the great toe.
- The tendocal caneous is inserted in the middle of the posterior surface of the calcaneus.
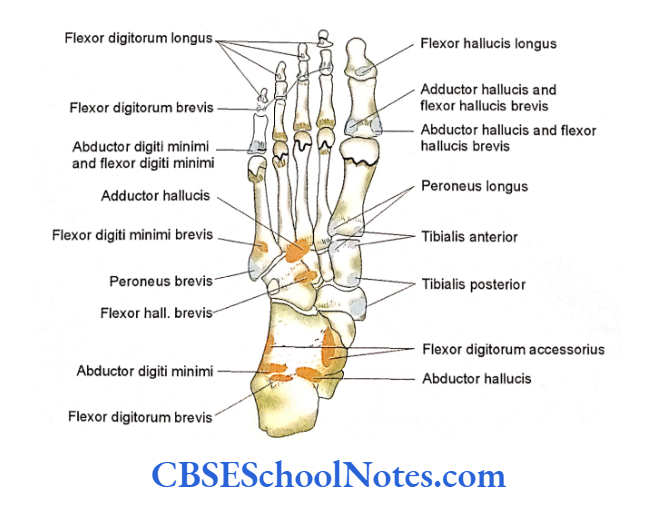
Attachment of Muscles on the Plantar Aspect of the Bones of Foot
- The flexor hallucis longus is inserted into the base of the distal phalanx of the great toe.
- The flex or digitorum longus is inserted into the plantar surface of the bases of the distal phalanges of lateral four digits.
- The peroneus longus muscle is inserted at the base of the first metatarsal and on the lateral aspect of the medial cuneiform bone.
- The tibialis anterior is inserted into the medial cuneiform and base of the first metatarsal on the medial and plantar aspects.
- The tendon of the tibialis posterior has very extensive insertion. It is mainly inserted into the tuberosity of the navicular bone and medial cuneiform.
- This tendon also sends slips to all other tarsal bones (except the talus) and bases of the 2nd, 3rd, and 4th metatarsals.
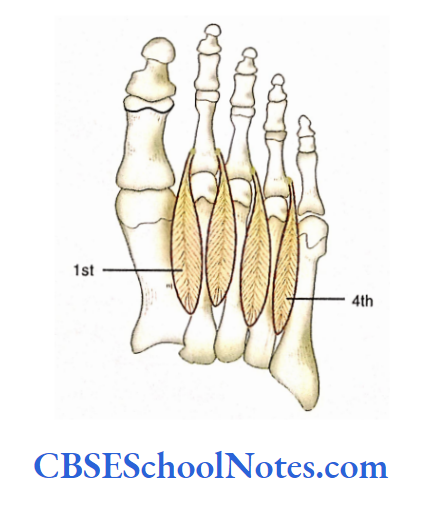
- Origin and Insertion of the Intrinsic Muscles of the Foot The dorsal aspect gives origin to the extensor digitorum brevis.
On the plantar surface, many intrinsic muscles are attached (flexor digitorum brevis, abductor digit minim abductor hallucis, flexor digitorum accessories, flexor hallucis brevis, adductor hallucis, and flexor digit minimi brevis).
Students should learn the origin and insertion of all these muscles with the help of The origin and insertion of plantar interossei shown in the dorsal interossei.
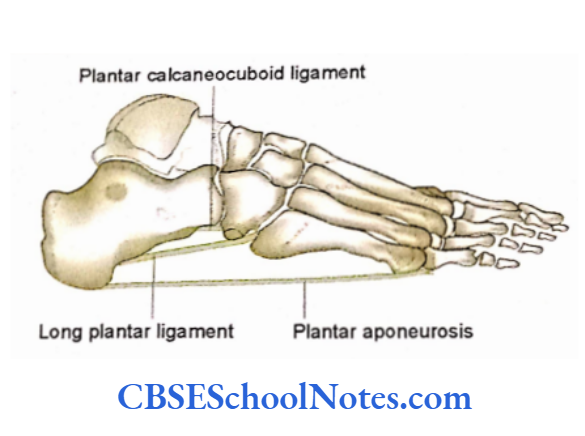
Attachment of Ligaments on the Bones of the Foot
- The bones of the foot give attachment to many ligaments. A few important ligaments are described here:
- The interosseous talocalcaneal ligament is attached between the sulcus tali of talus and sulcus calcanei of calcaneus.
- The spring ligament (plantar calcaneonavicular ligament) is attached to the anterior margin of sustentaculum tali of the calcaneus and the plantar surface of the navicular bone.
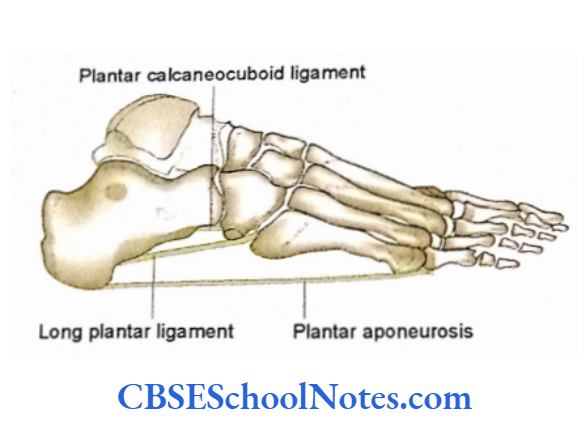
- On the plantar surface, the long plantar ligament is attached posteriorly to the tuberosity of the calcaneus and anteriorly to the cuboid bone and bases of the 2nd, 3rd, and 4th metatarsal bones.
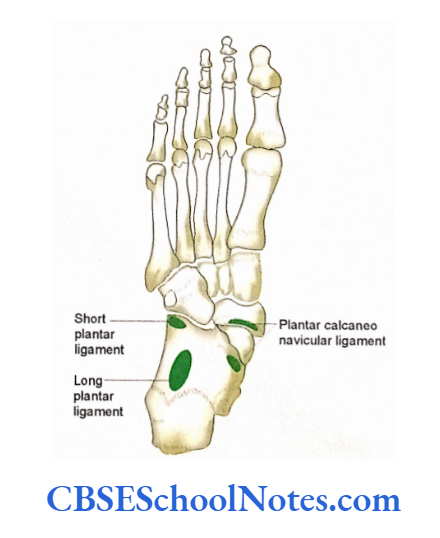
- The short plantar ligament is proximally attached to the anterior tubercle of the calcaneus and distally on the cuboid.
- The groove on the posterior aspect of the talus is related to the tendon of flexor hallucis longus.
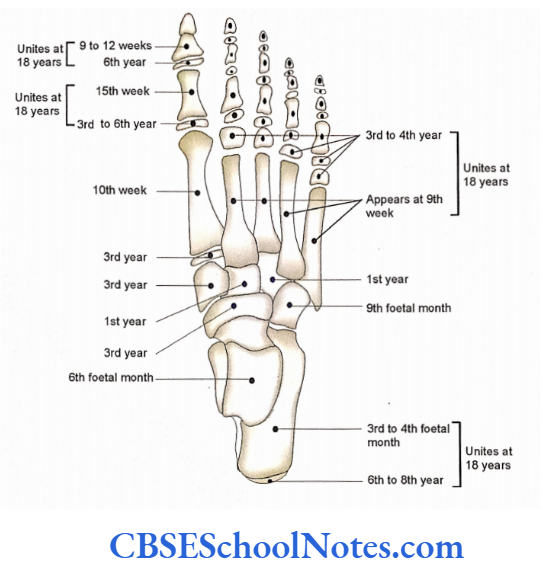
Ossification
Tarsal Bones
Calcaneus is classified by one primary center and one secondary center. All other tarsal bones ossify by one center only. The ossification of metatarsal and phalanges.
Patella
The patella is also known as the kneecap as it lies in front of the knee joint. It is a small triangular bone present in the tendon of the quadriceps femoris.
The patella is not a true bone as it is devoid of periosteum, hence it is classified as a sesamoid bone.
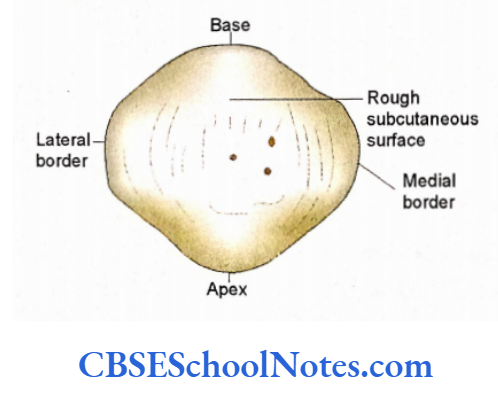
The patella has an apex, a base, medial and lateral borders, and an anterior and a posterior surface. The base forms the upper border of the bone.
The apex is directed downwards. The anterior surface is rough and subcutaneous while the posterior surface is mostly articular.
The articular surface is divided into a smaller medial and a large lateral surface by a vertical ridge. These surfaces articulate with the corresponding surfaces on the femoral condyles.
Patella Side Determination
- The apex of the patella should be directed downwards.
- The smooth articular surface should face posteriorly.
- The larger lateral part of the articular area should lie on the lateral side. The anterior surface is rough (presents several longitudinal ridges). The base, medial, and lateral borders give attachments to many muscles. The posterior surface is mostly articular.
Only a small portion near the apex is rough and gives attachment to the ligamentum patellae. The articular surface is divided into a large lateral and a small medial articular area by a vertical ridge.


These articular surfaces come in contact with the reciprocal patellar articular surface of the femur, i.e., the larger lateral area of the patella with lateral femoral condyle and medial area with medial condyle.
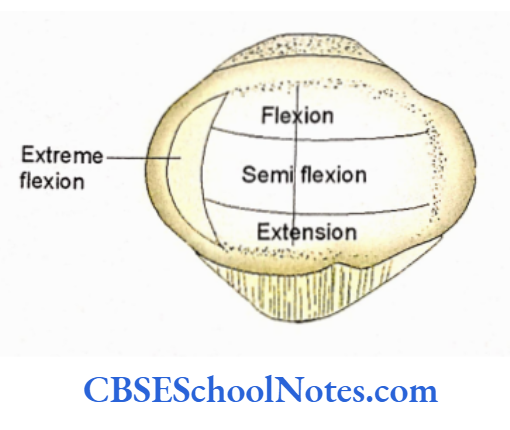
The medial articular area is further separated by a vertical ridge from the most medial narrow strip, which comes in contact with the medial condyle of the femur during full flexion.
As the patella moves downwards when the knee is flexed, its articular areas move on the articular areas at the lower end of the femur.
The various articular areas come in contact with the femur (from extension to full flexion).
Patella Ossification
The patella is cartilaginous up to three years of age. Several ossification centers appear in the patella between 3 to 6 years of age. These centers unite with each other and complete the ossification.