Bones Of The Head And Neck Regions
- The bones of the head and neck regions consist of the skull, cervical vertebrae, and hyoid bone.
- The skull forms the skeleton of the head region. the skull contains a large cavity for the lodgment of the brain (called a cranial cavity) and two small cavities for the lodgment of the eyes (called orbits).
- On the anterior aspect of the skull, there are two openings, i.e., the opening of nasal cavity and the opening of the oral cavity (mouth).
- Below the skull, the skeleton of the neck is formed by the seven cervical vertebrae.
- The hyoid bone is a small bone, present in the upper part of the neck in front of the 3rd cervical vertebra.
Anterior Nasal Aperture
Skull
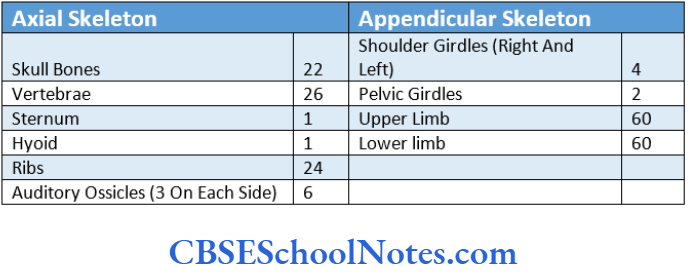
The skull (the skeleton of the head) is formed by 22 bones. These bones are firmly joined to one another and are immobile except for the bone of the lower jaw (mandible), which moves at the temporomandibular joint. The skull is divided into two parts, i.e., cranium and facial skeleton.
Cranium
- It is also known as the neuro-cranium, brain box, or calvaria. The cranium is the upper and posterior part of the skull.
- Cranium means skull minus the mandible.
- It consists of 8 bones. Out of these 8 bones, 4 are unpaired (frontal, occipital, sphenoid mid ethmoid) and 2 are paired (parietal and temporal).
- The joints between these bones are immobile and are known as sutures.
- The cranium has a dome-like roof (called a vault or skull cap) and a floor or cranial base (called basi-cranium.
Anterior Nasal Aperture
Facial Skeleton (Viscerocranium)
- The facial skeleton forms the anterior part of the skull. It contains orbital and nasal cavities and includes upper and lower jaws (maxillae and mandible).
- In addition to the frontal bone, the facial skeleton consists of 14 bones. Out of these 6 are paired (lacrimal, nasal, maxillae, zygomatic, palatine, and inferior nasal conchae). While the mandible and vomer are single bones.
Read and Learn More Human Osteology Notes
Anatomical Position of the Skull
To obtain the anatomical position of the skull, it is kept in the “Frankfurt horizontal plane”.
- Hold the skull in such a way that the inferior border of the orbit and the superior border of the external acoustic meatus of the right and left sides lie in the same horizontal plane.
- Students are suggested to identify various bones of a dry skull with the help. Once they can identify various bones in the skull then only they should proceed to study the details of the skull as seen from various aspects.
Anterior Nasal Aperture
A dry skull may be viewed from:
- Above (norma verticalis,.
- Behind (norma occipitalis,
- Front (norma frontalis). The walls of the orbital cavity can also be examined from this view.
- And from the side (norma lateralis,.
- Below (norma basalis externa,
- The roof of the calvaria (skull cap) may be removed by a transverse cut to examine the inside of the floor of the cranium.
- The interior of the base of the skull (norma basalis interna) is divided into three cranial fossae, i.e., anterior, middle, and posterior. The inner aspect of the skull cap.
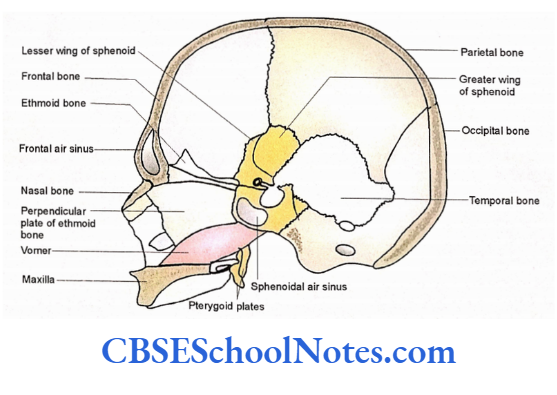
- The section of the skull in the para-median plane will help us to study the nasal cavity.
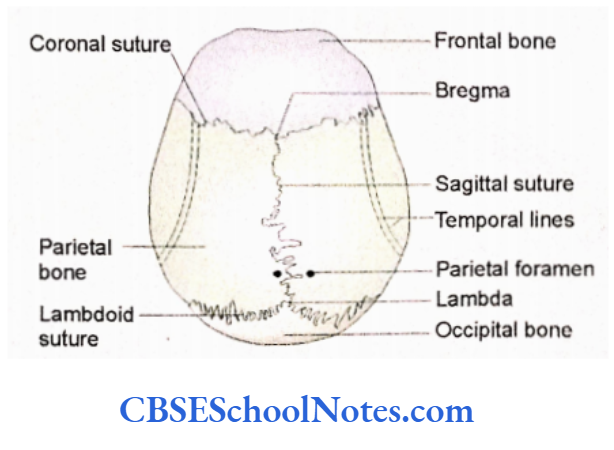
Superior Aspect Of The Skull (Norma Verticals)
When the skull is viewed from above it appears oval. It is relatively wider nearer its occipital pole (posteriorly). The bones forming the skullcap (roof of the brain box) are visible from this aspect.
Anterior Nasal Aperture
Bones Forming the Norma Verticalis
- Frontal bone
- It is a single bone that forms the anterior part of the norma verticalis.
- Parietal bones
- These are paired bones and lie posterior to the frontal bone on each side of the midline.
- Occipital bone—It is a single bone and lies posterior to the parietal bones.
Sutures (Joints) Present in the Normal Verticalis
The following three sutures and their meeting points are seen in this norma:
- Coronal suture—It lies between the frontal and right and left parietal bones.
- Sagittal suture—It is present in the midline between the right and left parietal bones.
Norma Basalis Interna
Lambdoid suture
- It lies between the occipital and two parietal bones.
- Bregma—It is a landmark point, where coronal and sagittal sutures meet each other. It is present in the midline.
Lambda
- It is present at the junction of the sagittal and lambdoid sutures.
Features of Norma Verticalis
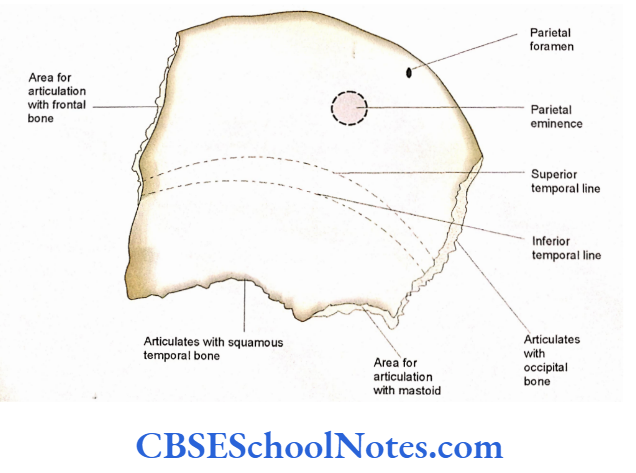
- The parietal foramen is present near the sagittal suture about 3.5 cm anterior to the lambda. It transmits a small emissary vein, which connects the superior sagittal sinus with the veins of the scalp.
- Parietal eminence is the area of the maxi¬ mum convexity on the parietal bone. It is present on the posterolateral aspect of the parietal bone.
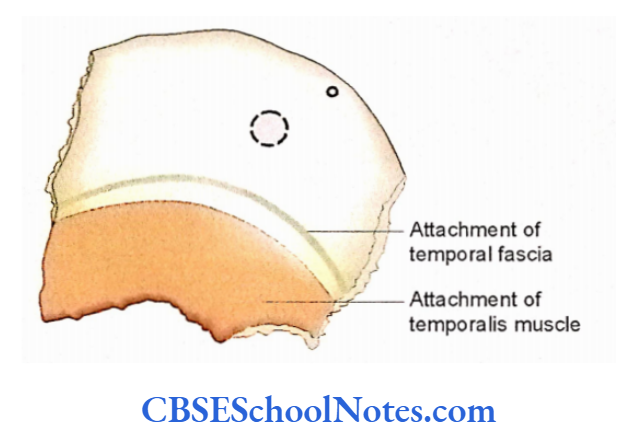
- Superior and inferior temporal lines are seen on the lateral side of the frontal and parietal bones. The superior temporal line gives attachment to the epicranial aponeurosis and temporal fascia. The inferior temporal line gives attachment to the temporalis muscle.
- The vertex is the highest point of the skull and is situated near the midpoint of the sagittal suture.
Applied Importance
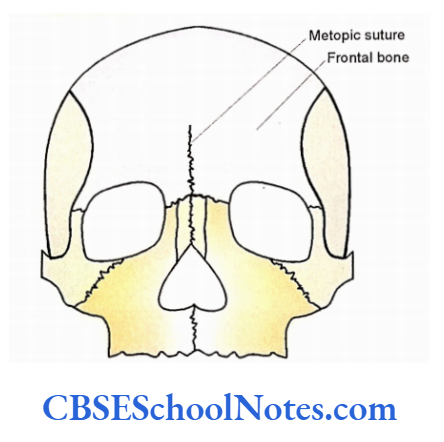
Metopic Suture
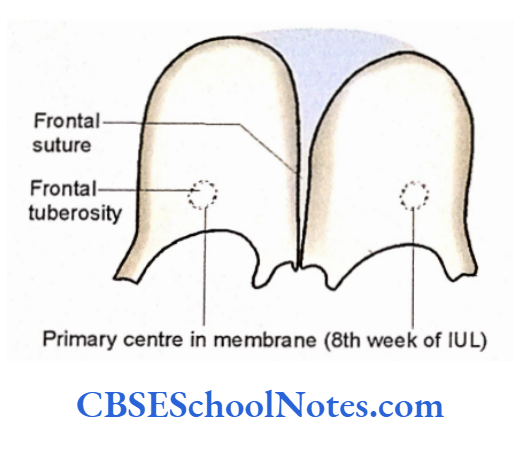
The right and left halves of the frontal bone are ossified from separate centers. There exists a frontal suture between two frontal bones before the age of 6 years. In some adult skulls, this suture may persist in full or in part and is known; as a metopic suture.
Sutural Bones
Isolated small bony ossicles (bones) are sometimes observed along the lambdoid and sagittal sutures. These are called sutural bones. They are formed due to; ossification from separate centers
Norma Basalis Interna
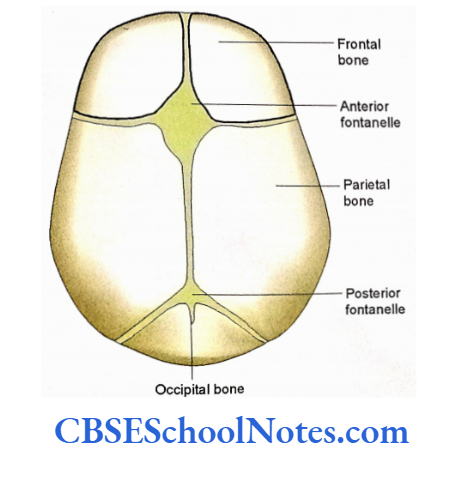
Fontanelle
In the skull of a newborn there are membranous I gaps at the site of bregma and lambda. These are called anterior and posterior fontanelles respectively.
The anterior fontanelle closes (the membranous gap of the anterior fontanelle is replaced by bone) by 18 months of age, while the posterior closes by 2 to 3 months of age.
Following are the functions of fontanelle: Fontanelle allows molding of the skull during birth, as the head passes through the birth canal.
- They also allow the brain to grow.
- An increased intracranial tension leads to the bulging of the anterior fontanelle.
- Similarly, depression of the anterior fontanelle indicates dehydration.
- One can easily draw the blood for testing or inject drugs in the superior sagittal sinus through anterior fontanelle.
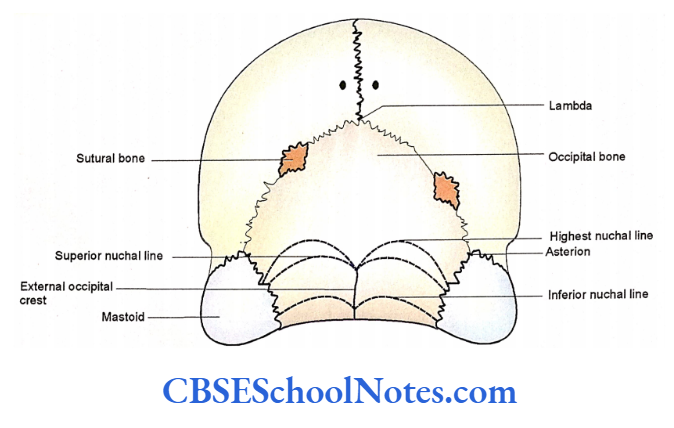
The Posterior Aspect Of The Skull (Norma Occipitalis)
Bones Seen in Norma Occipitalis
- Right and left parietal bones.
- Squamous part of the occipital bone.
- Mastoid part of the right and left temporal bone.
Norma Basalis Interna
Sutures (Joints) Seen in Norma Occipitalis
- Posterior part of the sagittal suture in midline.
- The lambdoid suture between two parietal and occipital bones.
- Right and left parietomastoid sutures between the parietal and the mastoid part of the temporal bones.
- Right and left occipitomastoid sutures between occipital and mastoid bones.
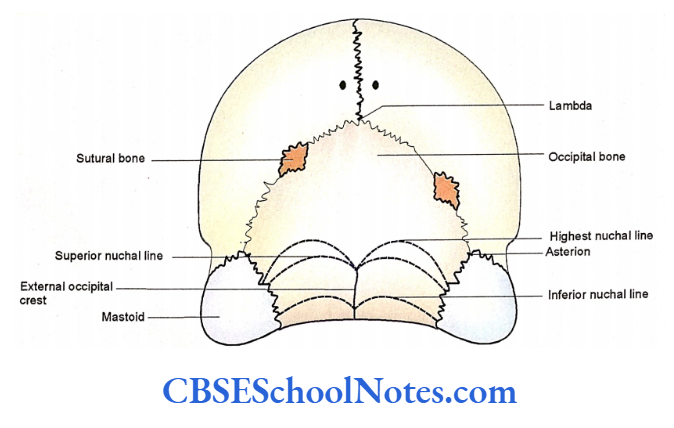
- The parietal, occipital, and mastoid bones, on each side, meet at a point, which is known as an asterion. It is at a junction of the lambdoid, parietomastoid, and occipitomastoid sutures.
Features
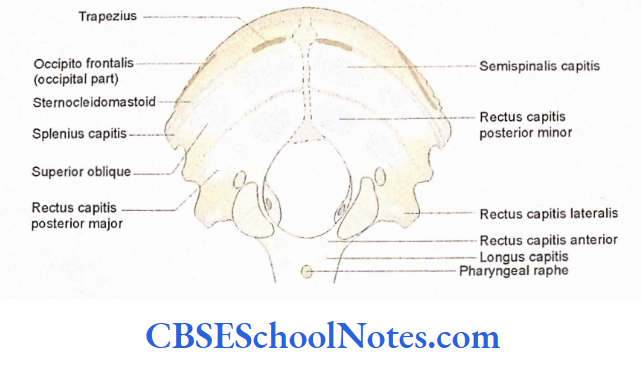
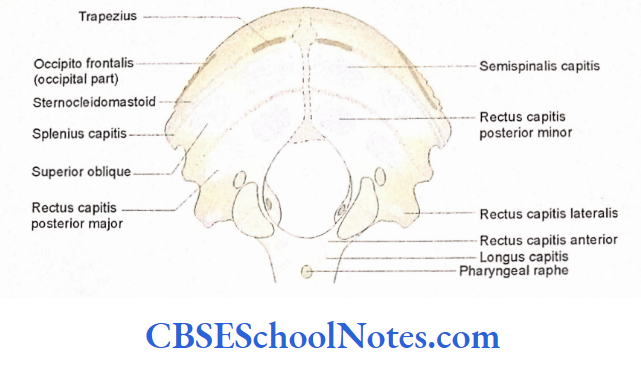
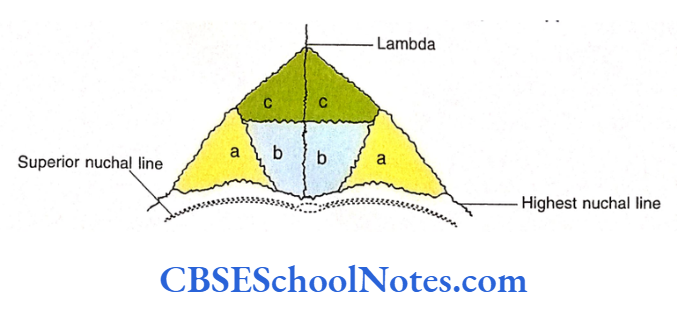
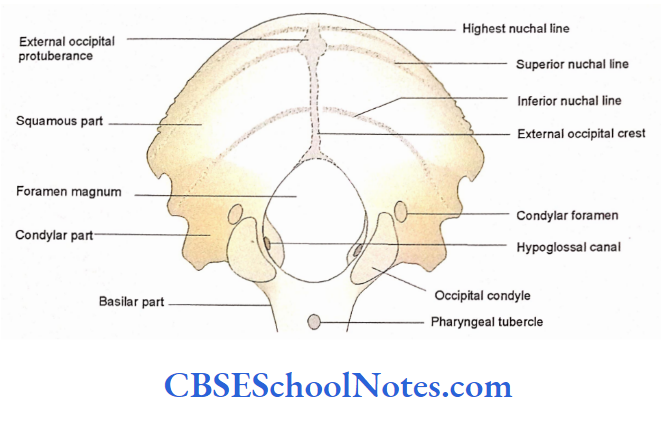
- The external occipital protuberance is a palpable midline elevation. The highest point on this protuberance is also known as inion.
- The superior nuchal lines extend laterally from each side of the external occipital protuberance to the mastoid process.
- These lines mark the upper limit of the neck. The trapezius and sternocleidomastoid muscles are attached to this line.
- The external occipital crest descends downwards from the external occipital protuberance to the foramen magnum. It gives attachment to the ligamentum nuchae. The right and left inferior nuchal lines run laterally from the crest.
- The right and left highest nuchal lines are present just above the superior nuchal lines.
- These lines give attachment to the epicranial aponeurosis and the occipital belly of the occipitofrontalis.
- The mastoid foramen is situated close to the occipitomastoid suture and transmits an emissary vein and meningeal branch of the occipital artery.
- One or more sutural bones may be present at the lambda, lambdoid suture or at asterion.
- Between superior and inferior nuchal lines semispinalis capitis and obliquus capitis superior muscles are attached.
- Between the inferior nuchal line and posterior margin of the foramen, magnum rectus capitis posterior major and minor are attached.
Norma Basalis Interna
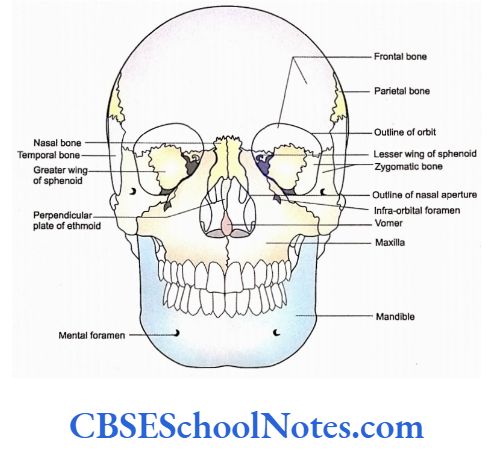
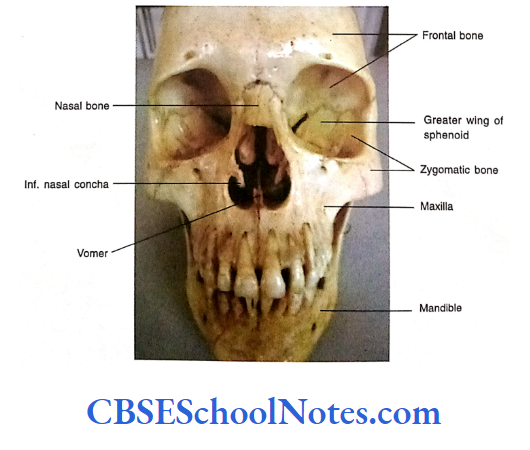
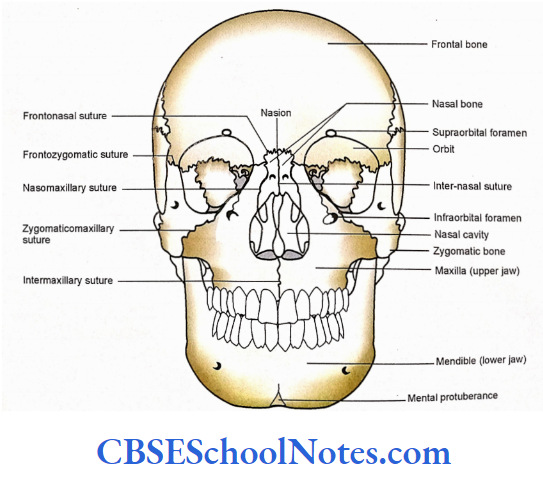
Anterior Aspect Of The Skull (Norma Frontalis)
This aspect of the skull forms the facial skeleton and consists of the forehead, orbits, nasal region, malar prominence, and upper and lower jaws.
Bones Seen in the Norma Frontalis
Identify the following bones from above downwards.
- Frontal bone.
- Nasal bones.
- Zygomatic bones.
- Maxillae.
- Mandible.
The frontal bone and mandible are single bones, while nasal, zygomatic and maxillae are paired bones.
Sutures (Joints) Seen in the Norma Frontalis
Identify the following sutures, which are present close to the median plane:
- The frontonasal suture is present between the nasal process of the frontal bone and nasal bones.
- The front-maxillary suture is present between the nasal part of the frontal bone and the frontal process of the maxilla.
- The inter-nasal suture is present in the midline between two nasal bones above the nasal aperture.
- The naso-maxillary suture is present between the lateral border of the nasal bone and the frontal process of the maxilla.
- The inter-maxillary suture is present between the right and left maxilla below the nasal aperture.
Identify the following sutures present laterally in the norma frontalis:
- The fronto-zygomatic suture is present between the zygomatic process of the frontal bone and the frontal process of the zygomatic bone. This suture is present on the lateral border of the orbit.
- The zygomatico-maxillary suture is between the zygomatic process of the maxilla and the maxillary process of the zygomatic bone.
- The nasion is the meeting point of internasal and frontonasal sutures. It is present in the midline at the root of the nose.
Sulcus Chiasmaticus
Features of the Norma Frontalis
For ease of understanding norma frontalis is studied under the following headings:
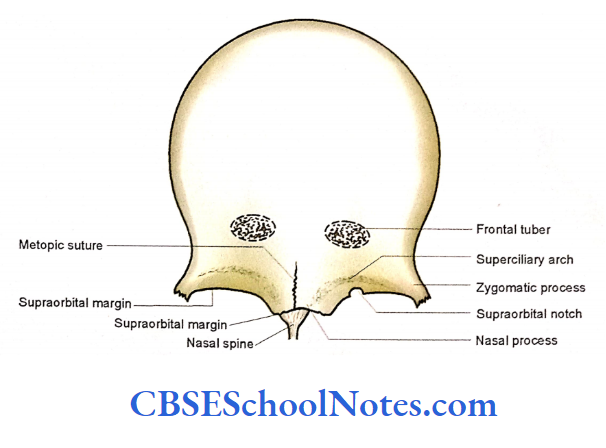
Forehead
- The squamous part of the frontal bone forms the skeleton of the forehead. In the fetal and infant skulls the two halves of the frontal bone are separated by the frontal suture.
- Two frontal bones remain separated upto 6 years of age. In some adults, this suture may persist as a metopic suture.
- The glabella is the smooth, slightly depressed middle area just above the nasion.
- The superciliary arches are curved elevations above the medial part of supraorbital margins. They extend laterally from glabella.
- The frontal eminences are paired with rounded elevations above the superciliary arches.
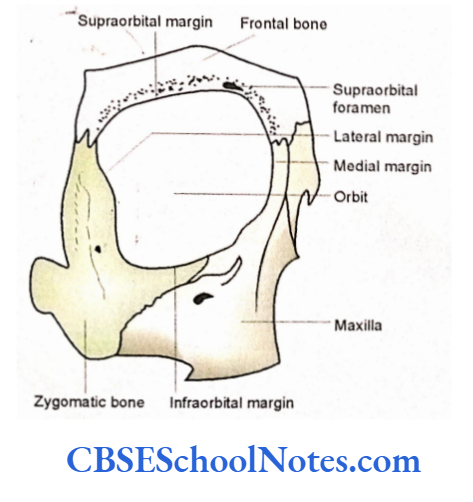
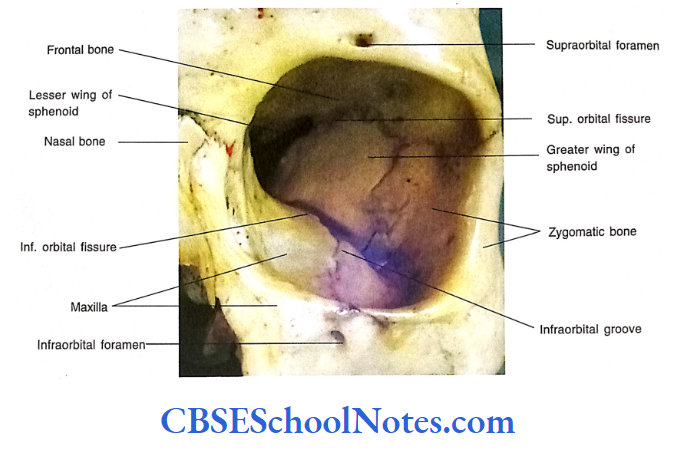
Orbital Openings
Each orbital opening is quadrangular in shape and presents four margins.
- The supraorbital margin is formed by the frontal bone. This border presents a supraorbital notch or foramen at the junction of medial 1/3 with lateral 2/3.
- The supraorbital nerve and vessels pass to the forehead through the supraorbital notch or foramen. The supratrochlear vessels and nerve pass medial to the supraorbital notch.
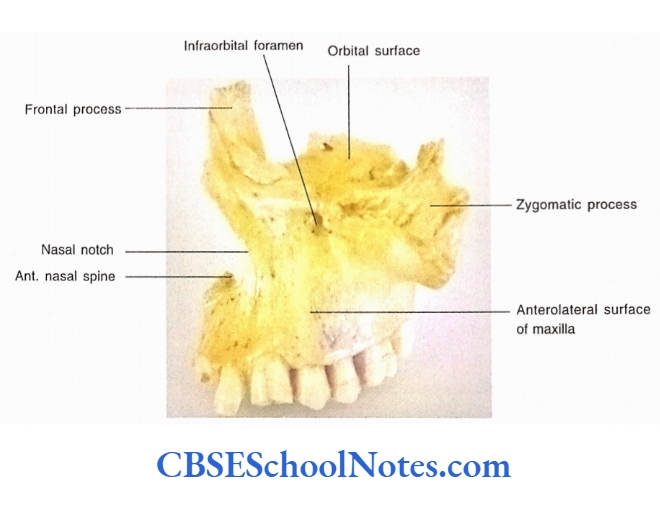
- The infraorbital margin is formed by the maxilla medially and zygomatic bone laterally.
- The infraorbital foramen is present just below this margin, which transmits the infraorbital nerve and vessels.
- The lateral margin of the orbit is formed by the zygomatic and frontal bones.
- The medial margin is formed by the frontal bone and the frontal process of the maxilla.
- A detailed description of the orbital cavity is given later.
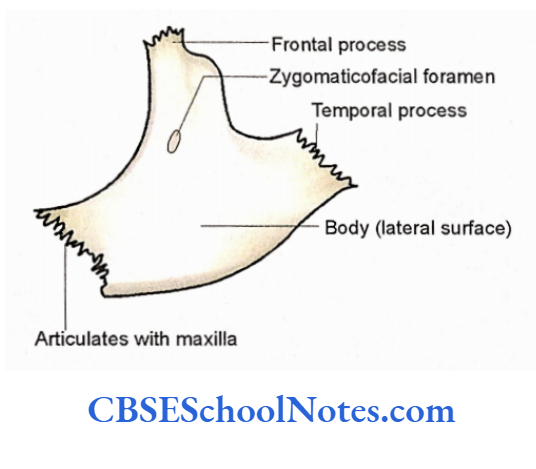
Malar Prominence
- The prominence of the cheek is formed by the zygomatic bone. It is situated inferolateral to the orbit.
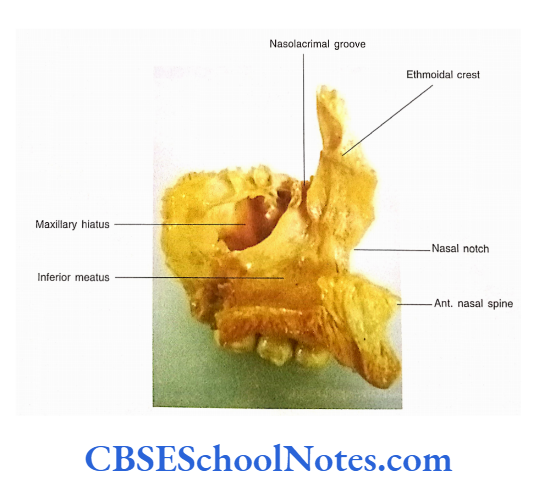
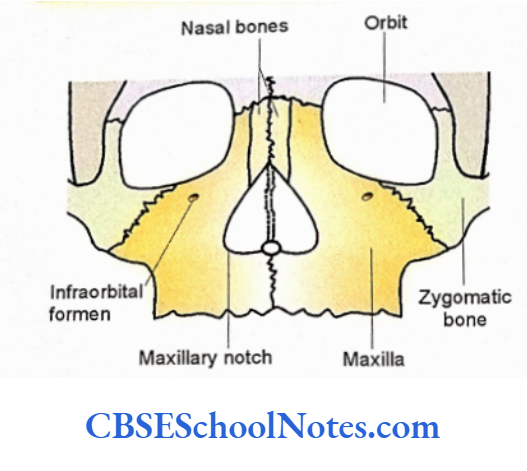
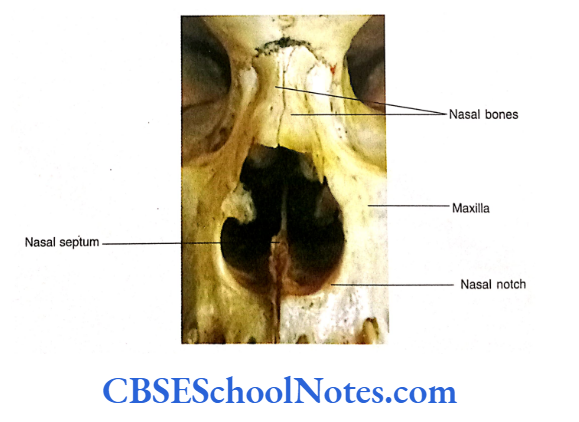
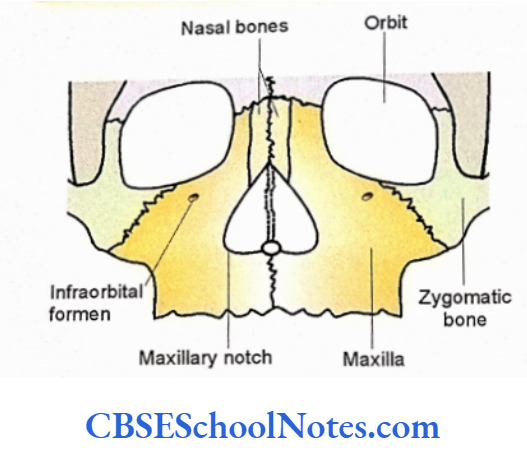
- The zygomatico-facial foramen is present on the bone, which transmits the nerve of the same name. Anterior Nasal Aperture The nasal aperture is piriform in shape.
- It is bounded above by the right and left nasal bones, while lateral and inferior boundaries are formed by the nasal notches of the right and left maxilla.
- The anterior nasal spine is a median bony projection from the maxillae.
- Margins of the anterior nasal aperture give attachment to the nasal cartilage.
- In the depth of the anterior nasal aperture nasal septum can be seen in the midline. This septum separates the cavity of the nose into right and left nasal cavities. A detailed description of the nasal cavity.
Sulcus Chiasmaticus
Upper Jaw (Maxillae)
The upper jaw is formed by the right and left maxilla.
- The alveolar process of the maxilla bears the sockets for the upper teeth.
- The root of the canine tooth produces an elevation on the upper jaw, which is known as canine eminence.
- The canine fossa is situated just lateral to the canine eminence.
- The incisive fossa is situated above the incisor teeth.
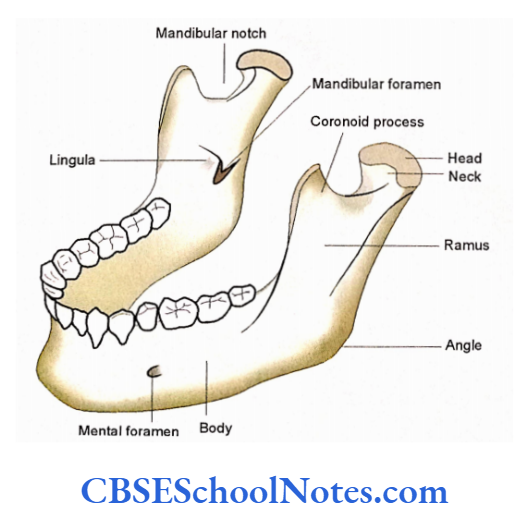
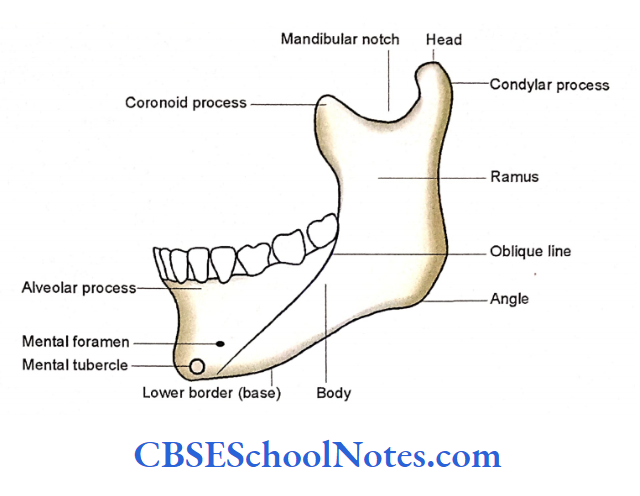
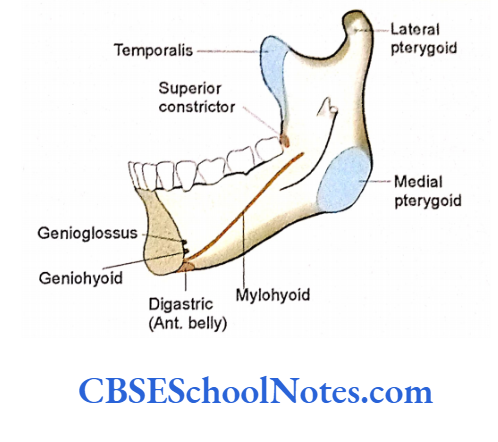
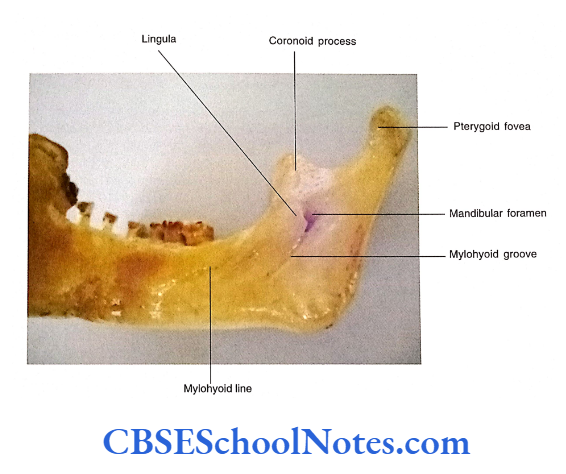
Lower Jaw (Mandible)
The lower jaw is formed by the mandible.
- The mandible is the only movable bone of the skull.
- The alveolar processes house the lower teeth.
- The mental foramen is present below the 2nd premolÿr teeth. It gives passage to the mental nerve and vessels.
- The anterior surface of the symphysis menti presents a triangular elevation, the mental protuberance.
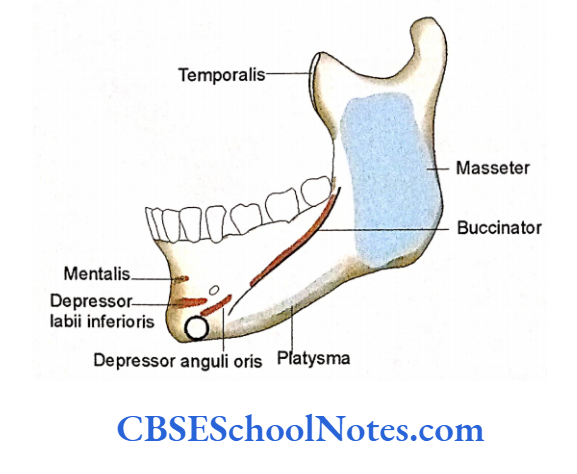
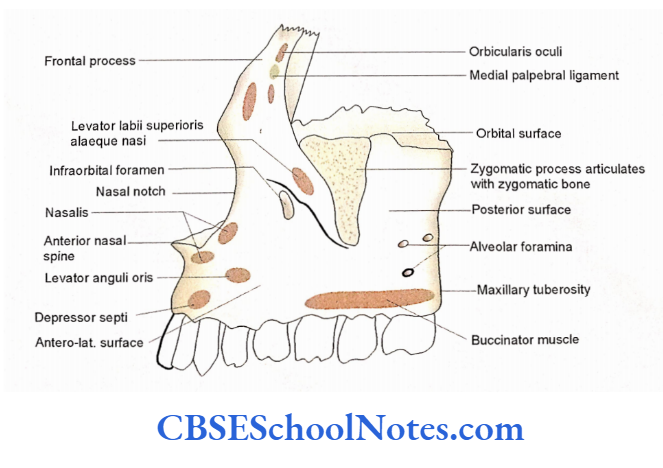
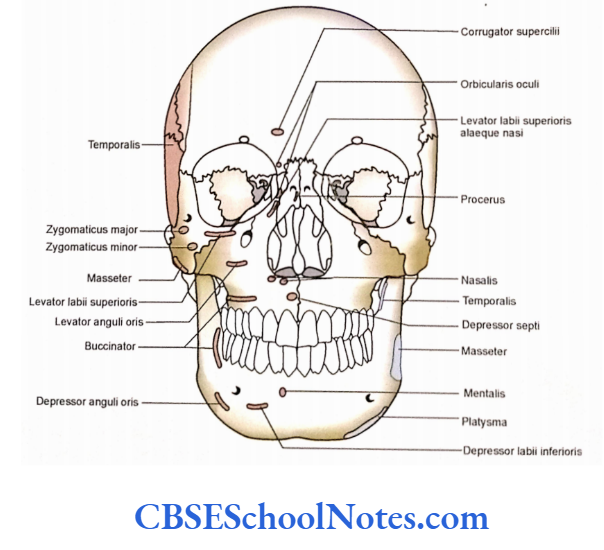
Attachment of Muscles in the Norma Frontalis
Students should study the attachment of muscles on the norma frontalis
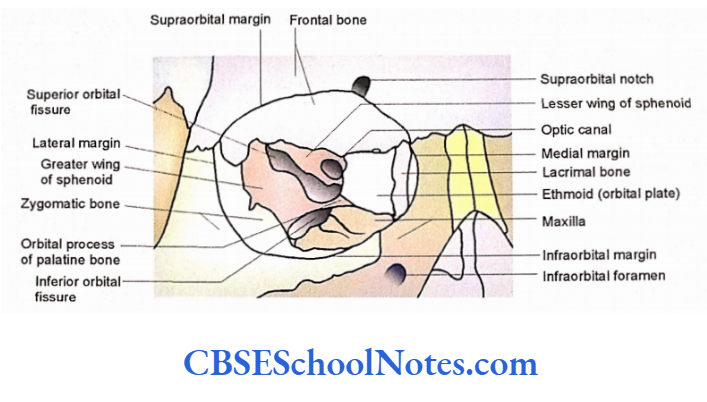
The Orbital Cavity
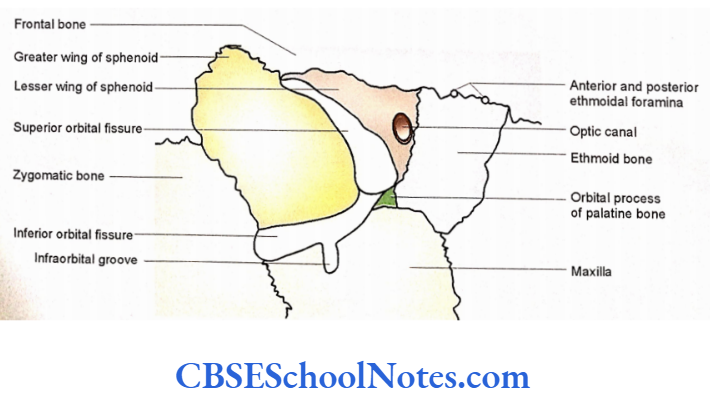
We have already studied the orbital margin in this chapter. Here, we shall study the walls and various openings of the orbital cavity.
The orbit is like a four-sided pyramid. It has a base, an apex, a roof, a floor, a medial wall, and a lateral wall.
Sulcus Chiasmaticus
The Base
The base of the orbit is the orbital opening. It has four margins, i.e., upper, lateral, medial, and inferior margins.
The Apex
The apex of the orbit lies posteriorly.
The Medial Wall
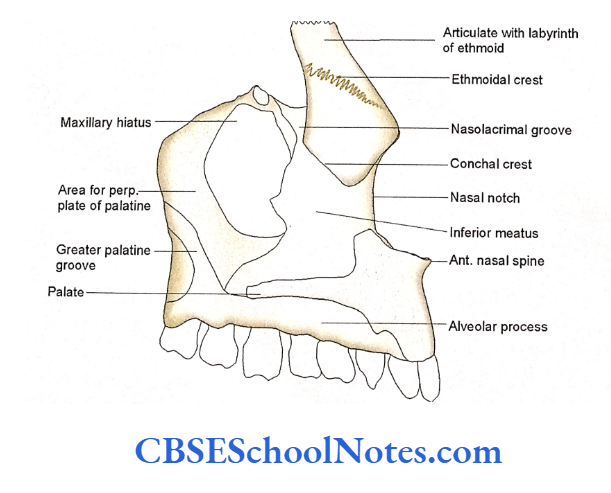
The medial wall of the orbit, from anterior to posterior, is formed by the frontal process of the maxilla, lacrimal bone, orbital plate of the ethmoid, and body of the sphenoid.
- Most anteriorly the medial wall shows a deep groove called a lacrimal groove.
- This groove lodges the lacrimal sac. It is bounded anteriorly and posteriorly by the anterior and posterior lacrimal crests, respectively.
- Most of the medial wall is formed by the orbital plate of the ethmoid.
- The anterior and posterior ethmoidal foramina are present at the superior border of this bone.
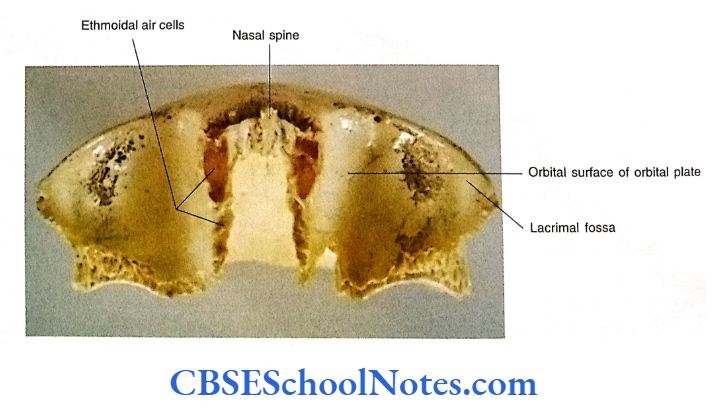
The Superior Wall or Roof
The superior wall is formed mainly by the orbital plate of the frontal bone. Most posteriorly, a small part of the roof is also formed by the lesser wing of the sphenoid.
Anteromedially there is the presence of a small depression called the trochlear fossa, which gives attachment to the pulley for the superior oblique muscle.
Anterolaterally there is a deep fossa called as lacrimal fossa for lacrimal gland.
Skull Regions
The Lateral Wall
It is formed anteriorly by the zygomatic bone and posteriorly by the greater wing of the sphenoid.
The Inferior Wall or Floor
It is mainly formed by the maxilla. The small anterolateral part of the floor is also formed by the zygomatic bone. Most posteriorly the floor is formed by the orbital process of the palatine bone.
Fissures, Canals, and Foramina of the Orbital Cavity
The orbital cavity communicates with the neighboring regions of the skull through superior and inferior orbital fissures, optic and infraorbital canals, and various foramina.
It is present posteriorly between the roof and posteriorly with the pterygopalatine fossa lateral wall of the orbital cavity.
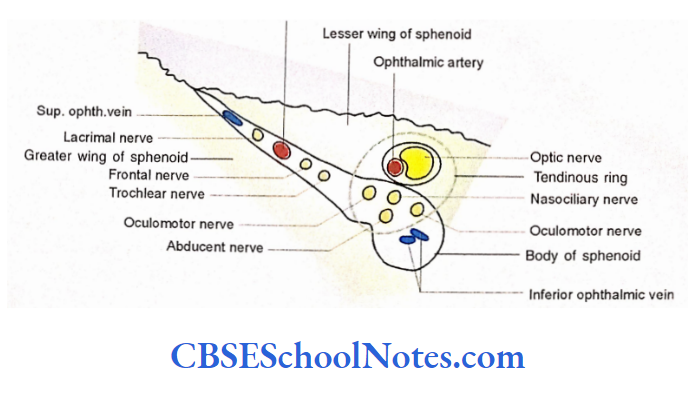
The Superior Orbital Fissure
It is posteriorly between the infratemporal fossa. bounded above by the lesser wing of the fissure gives passage to the maxillary sphenoid, medially by the body of the sphenoid and Zygomatic nerves, emissary veins, and below and laterally by the greater wing infraorbital vessels. of the sphenoid.
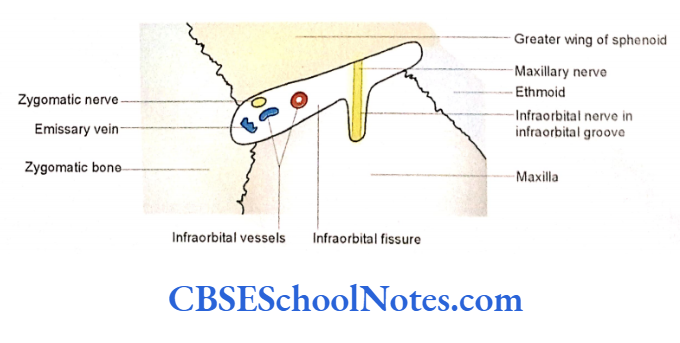
The Inferior Orbital Fissures
It is present posteriorly between the lateral wall and the floor of the orbit. It is bounded above and laterally by the greater wing of the sphenoid and below and medially by the maxilla.
It communicates sphenoid and below and medially by the maxilla. It communicates The fissure gives passage to the maxillary and Zygomatic nerves, emissary veins, and infraorbital vessels.
Skull Regions
The Optic Canal
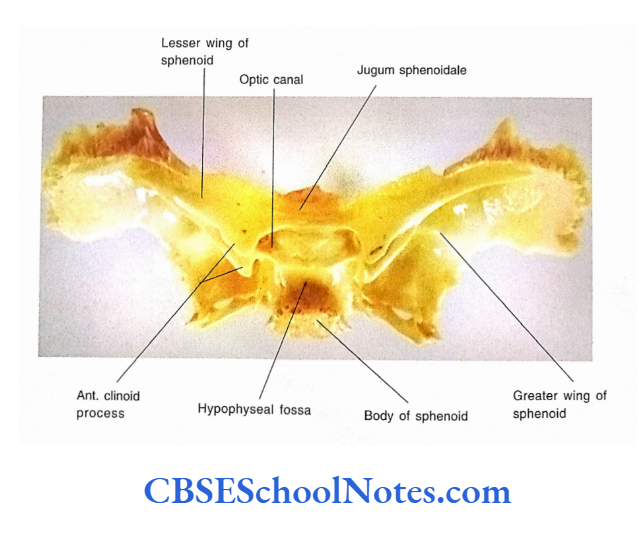
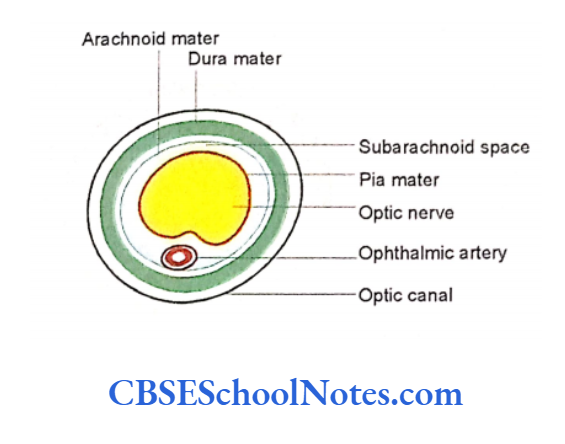
The Optic canal is present at the apex of the orbital cavity at the junction of the roof and medial wall. It is bounded medially by the body of the sphenoid and laterally by the lesser wing. It communicates with the middle cranial fossa and transmits the optic nerve along with its meningeal covering and ophthalmic artery. A common tendinous ring, which gives origin to four recti muscles of the eye, is attached surrounding the opening of the optic canal.
The Infraorbital Canal
The infraorbital canal is present in the bony substance of the maxilla. The canal is continuous posteriorly on the floor of the orbit as an infraorbital groove and opens anteriorly at the infraorbital foramen.
It gives passage to the infraorbital nerve and vessels. The infraorbital nerve is the continuation of the maxillary nerve.
Anterior and Posterior Ethmoidal Foramina
These two small foramina are present at the upper border of the orbital plate of the ethmoid (at the junction of the roof and medial wall of the orbit, These foramina transmit the anterior and posterior ethmoidal nerves and vessels to the anterior cranial fossa.
Skull Regions
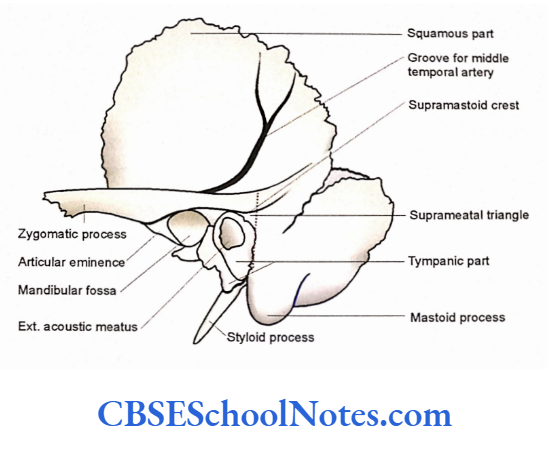
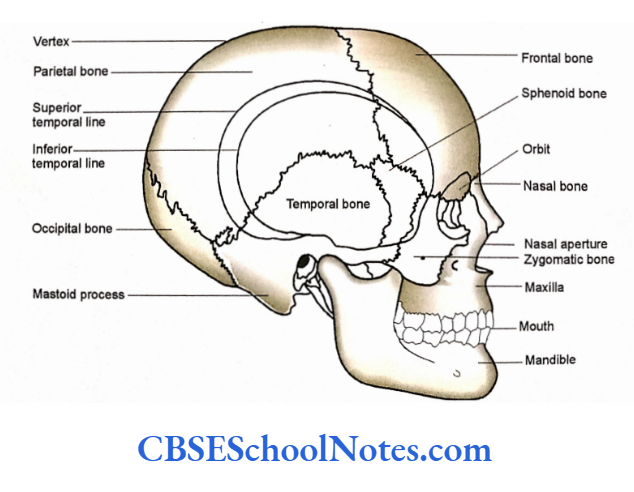
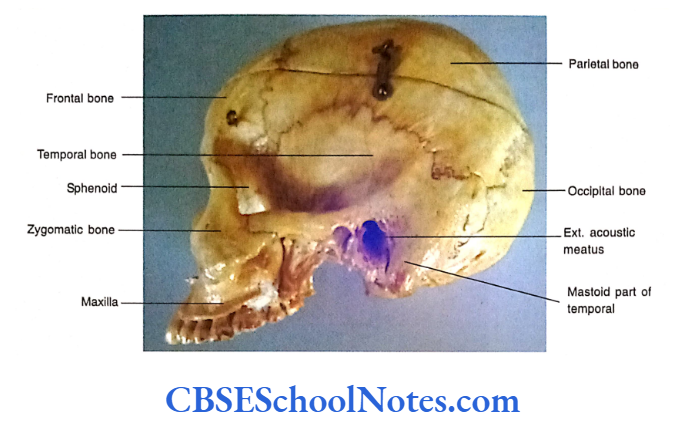
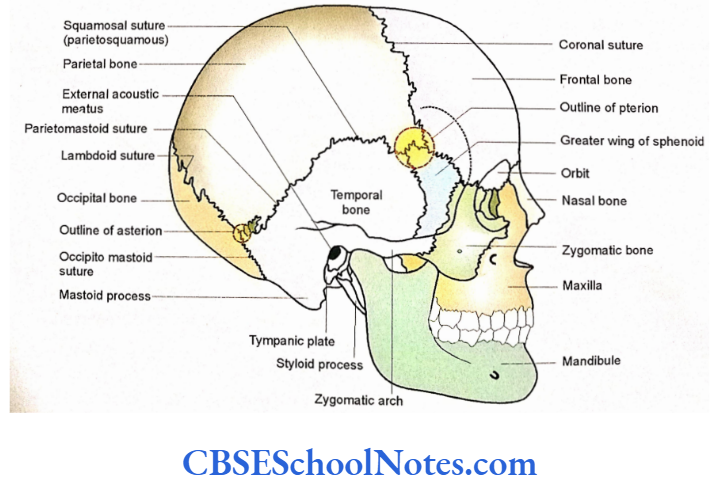
The Lateral Aspect Of The Skull (Norma Lateralis)
This aspect of the skull is formed by cranial and facial bones. The posterosuperior region of norma lateralis (cranial part) includes the temporal fossa, external acoustic meatus, and mastoid part of the temporal bone.
The anteroinferior part of the norma lateralis (facial part) includes the zygomatic arch, infratemporal fossa, lateral aspect of the maxilla and mandible.
Bones Seen in the Norma Lateralis
Identify the following bones on the lateral aspect of the skull:
- Frontal.
- Parietal.
- Occipital.
- Nasal.
- Maxilla.
- Zygomatic.
- Sphenoid.
- Temporal
- Mandible
Sutures (Joints) of the Norma Lateralis
Many sutures, which are seen in this aspect, have been already observed while studying norma frontalis, verticalis, and occipitalis. Hence, we shall study the sutures present in the central region of the norma lateralis.
H Shaped Suture
- The H-shaped suture is the meeting point of four bones, i.e., frontal, parietal, greater wing of the sphenoid, and squamous part of the temporal bone.
- A small circular area enclosing parts of all four bones is called a “pterion”.
- The pterion lies on the floor of the temporal fossa. The horizontal limb of the suture is the joint between the anteroinferior angle of the parietal bone and the greater wing of the sphenoid (parietosphenoid suture).
- The greater wing of the sphenoid articulates anteriorly with the frontal bone (at front sphenoidal suture) and posteriorly with the squamous part of the temporal bone (at temporosphenoidal suture).
The Parietosquamous and Parietomastoid Sutures
The lower border of the parietal bone articulates anteriorly with the squamous part of the temporal bone at parietosquattious suture and posteriorly with the mastoid bone at the parietomastoid suture.
Lambdoid Suture
At this suture, the posterior border of the parietal bone articulates with the occipital bone.
Occipitomastoid Suture
Here the occipital bone articulates with the mastoid part of the temporal bone. Features of the Norma Lateralis Following bony features are seen on the lateral aspect of the skull:
Skull Regions
Temporal Lines
Superior and inferior temporal lines are seen in this aspect. The superior line starts at the zygomatic process of the frontal bone. It arches upwards and backward crossing the coronal suture and fades away on the temporal bone.
It gives attachment to epicranial aponeurosis and temporal fascia. The inferior line starts along with the superior and runs inferior and parallel to it. Posteriorly, it runs downwards and forwards on the temporal bone to become continuous with the supramastoid crest.
The crest is further continuous anteriorly with the posterior root of the zygoma. The inferior temporal line limits the attachment of the temporalis muscle.
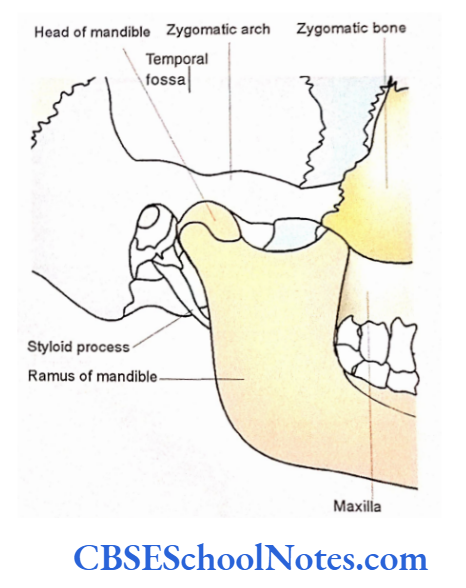
Zygomatic Arch
The zygomatic arch is formed by the articulation between the temporal process of the zygomatic and the zygomatic process of the temporal bone. At the posterior end and its lower border, the zygomatic arch bears a tubercle called as root of the zygoma.
Here the zygomatic arch divides into anterior and posterior roots. Trace the posterior root backwards along the lateral margin of the mandibular fossa, and then above the external acoustic meatus to become continuous with the supramastoid crest.
The anterior root passes horizontally as the articular tubercle, which lies anterior to the mandibular fossa.
The temporal fascia is attached to the upper border of the zygomatic arch. The lower border and inner surface of the arch give origin to the masseter muscle.
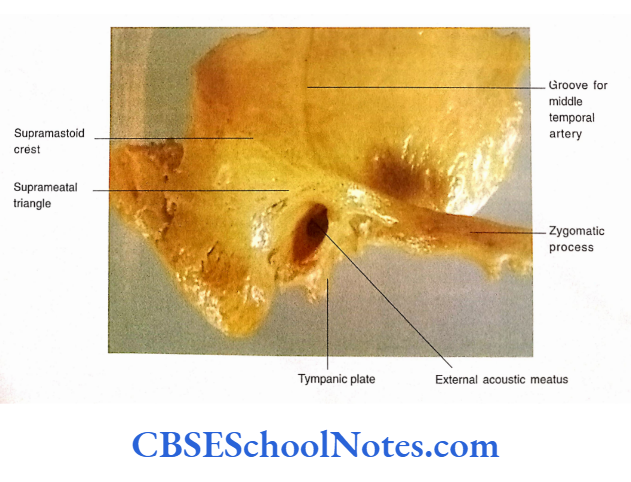
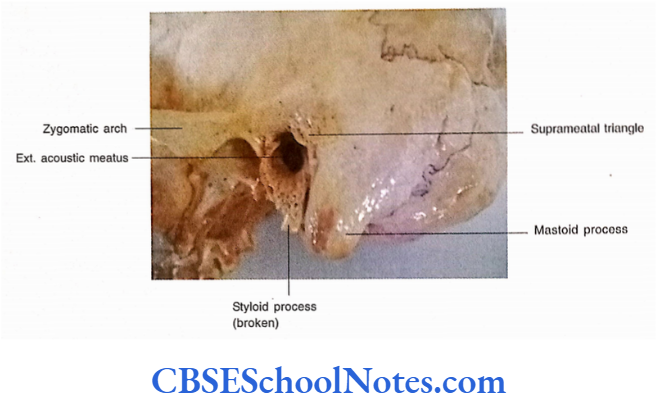
The External Acoustic Meatus
- The tympanic plate and squamous part of the temporal bone form the external acoustic meatus.
- The roof and upper part of the posterior wall are formed by squamous temporal bone, while the lower part of the posterior wall, floor, and anterior wall are by the tympanic plate.
- The margin of the meatus gives attachment to the cartilaginous part of the external acoustic meatus.
Supramental Triangle
It is a depression, situated postero-superior to the external acoustic meatus.
It is bounded above by the supra mastoid crest, in front by the posterosuperior margin of the external acoustic meatus, and behind by a vertical line drawn along the posterior margin of the meatus. Deep in this triangle lies the mastoid antrum.
Mastoid Process
The mastoid part of the temporal bone lies behind the external acoustic meatus. It is continuous above the squamous temporal bone.
The mastoid process is a downward conical projection from the mastoid part of the temporal bone. The asterion is the junctional point of three sutures, i.e., parietomastoid, occipital mastoid, and lambdoid.
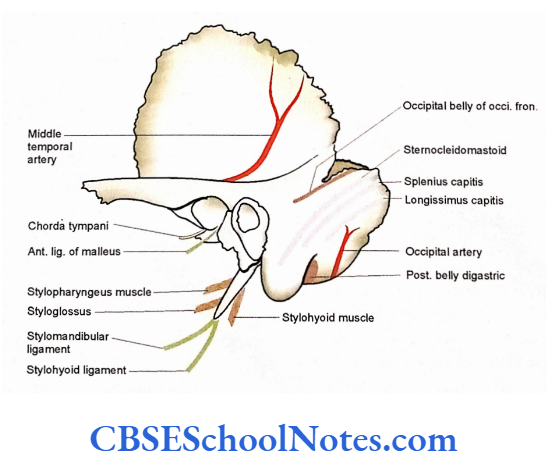
The external surface of the mastoid provides attachment to the sternocleidomastoid, splenius capitis, and longissimus capitis muscles.
A mastoid foramen pierces the bone near the occipitomastoid suture. It transmits an emissary vein from the sigmoid sinus and the meningeal branch of the occipital artery.
Skull Regions
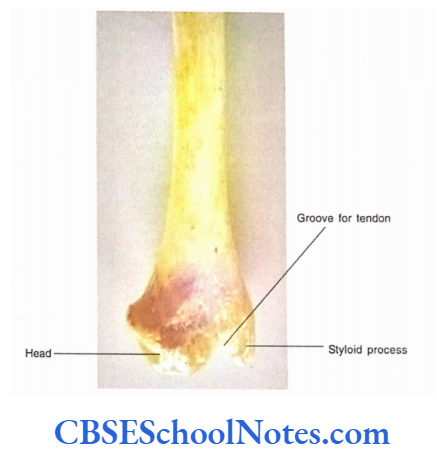
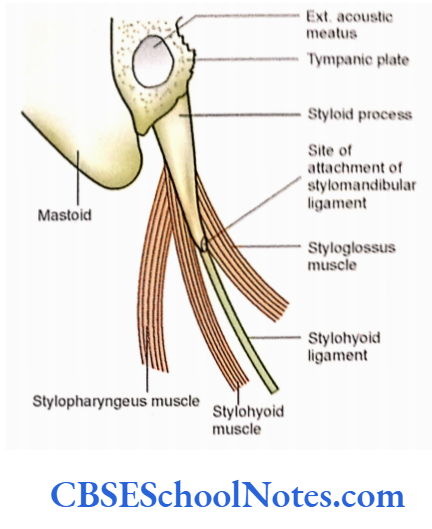
The Styloid Process
- The styloid process is seen when the skull is viewed from the lateral side. It is about a 2 to 5 cm long process projecting downwards, forwards, and medially.
- It is situated in front of the mastoid process on a deeper plane. It gives attachment to the styloglossus, stylohyoid, and stylopharyngeus muscles. The stylohyoid and stylomandibular ligaments are also attached to it.
Temporal Fossa
This is a shallow fossa that lies above the zygomatic arch. The temporalis muscle is located in this fossa.
This fossa is bounded:
- Posteriorly and superiorly by temporal lines.
- Anteriorly by the temporal surface of the frontal and zygomatic bones.
- Interiorly by the superior border of the zygomatic arch and supramastoid crest (on the lateral side). Interiorly on the medial side by the infratemporal crest of the greater wing of the sphenoid.
- Between zygomatic arch and infratemporal crest temporal fossa communicates below with the infratemporal fossa.
- Floor of the temporal fossa is formed by the part of the frontal, parietal, temporal and greater wing of the sphenoid bones. The circular area enclosing all these four bones and H shaped suture is called as pterion.
- It is situated 4 cm above the mid point of the zygomatic arch and 3.5 cm behind the frontozygomatic suture.
- The middle meningeal vein, anterior branch of middle meningeal artery, and stem of the lateral sulcus of brain lie deep to the pterion.
- The contents of the temporal fossa are temporalis muscle, deep temporal vessels and nerves and zygomaticotemporal nerve.
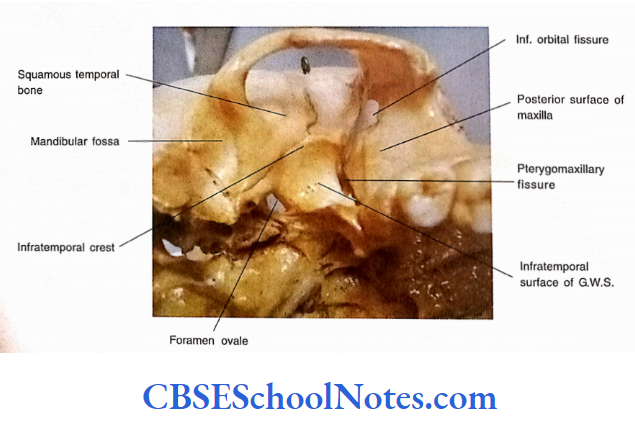
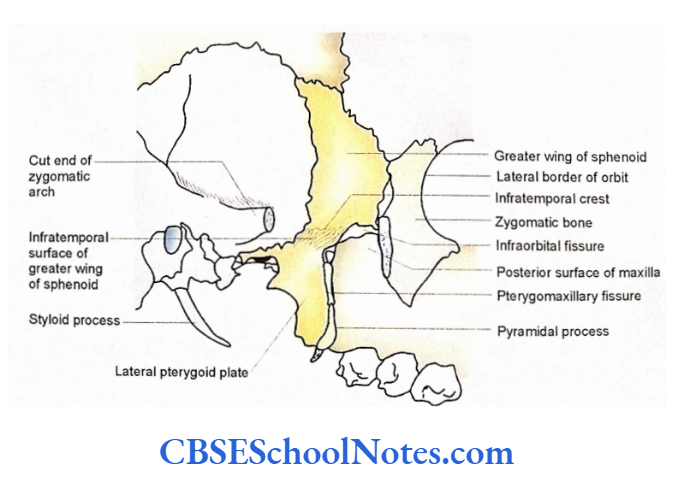
Infratemporal Fossa
It is an irregular fossa below the zygomatic arch and behind the maxilla. It communicates above with the temporal fossa deep into the zygomatic arch.
Boundaries
- Anterior wall: The posterior surface of the body of the maxilla bone. The surface of the maxilla shows many perforations (openings) for posterosuperior alveolar nerves and vessels.
- Medial wall: It is formed by the lateral pterygoid plate and pyramidal process of palatine bone. The junction of the anterior and medial walls shows a fissure called a term gomaxillaiy fissure. Deep to the fissure lies the pterygopalatine fossa.
- Lateral wall: It is formed by the ramus and coronoid process of the mandible.
- Roof: The roof is formed by the temporal surface of the greater wing of the sphenoid. At the junction of the roof and anterior wall, lies the lateral part of the inferior orbital fissure through which the infratemporal fossa communicates with the orbit Foramen ovale and foramen spinosum are present in the roof of the infratemporal fossa.
- Floor: It is not bounded but open.
- Posterior wall: It is also open.
The contents of the infratemporal fossa are as mentioned below:
- Lateral and medial pterygoid muscles and lower part of the temporalis.
- The maxillary artery and its branches, pterygoid venous plexus.
- Mandibular, maxillary and chorda tympani nerve and otic ganglion.
Skull Regions
Pterygopalatine Fossa
It is a small pyramidal space situated below the apex of the orbit and deep to the pterygomaxillary fissure.
Boundaries
Anterior: Posterior surface of the body of the maxilla.
Posterior: Root of the pterygoid process and the anterior surface of the greater wing of the sphenoid.
Medial: The perpendicular plate of the palatine bone.
Lateral: It is open and communicates with the infratemporal fossa through the pterygo¬ maxillary fissure. (The pterygomaxillary fissure is a triangular gap bounded anteriorly by the maxilla and posteriorly by the pterygoid process.
It transmits the third part of the maxillary artery, maxillary nerve, and posterior superior alveolar nerve and vessels).
Roof: Medially it is bounded by the body of the sphenoid and orbital process of the palatine bone. Laterally it communicates with the inferior orbital fissure.
Floor: It is closed due to the fusion of the anterior and posterior walls.
Communications of the Pterygopalatine Fossa
It communicates with the following:
- The orbit-Through the infraorbital fissure.
- The infratemporal fossa-Through pterygomaxillary fissure.
- The nasal cavity-Through sphenopalatine foramen.
- The middle cranial fossa-Through the foramen rotundum.
- The foramen lacerum—Through pterygoid canal.
Contents of the Pterygopalatine Fossa
- Maxillary nerve, pterygopalatine ganglion and its branches.
- The third part of the maxillary artery.
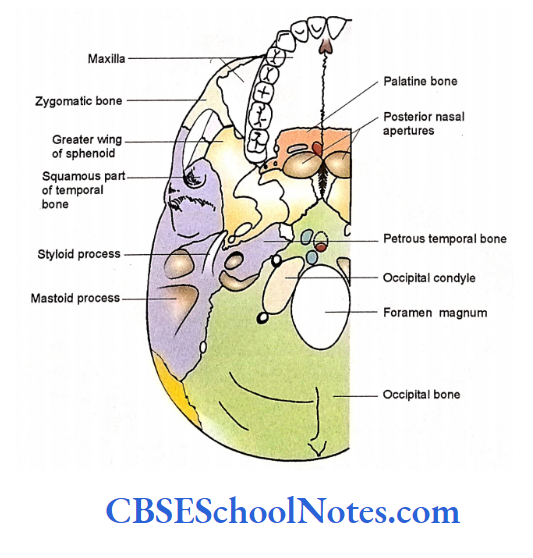
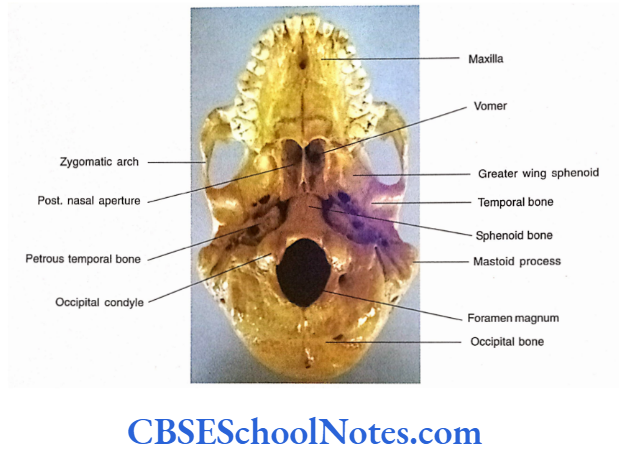
The Norma Basalis Externa
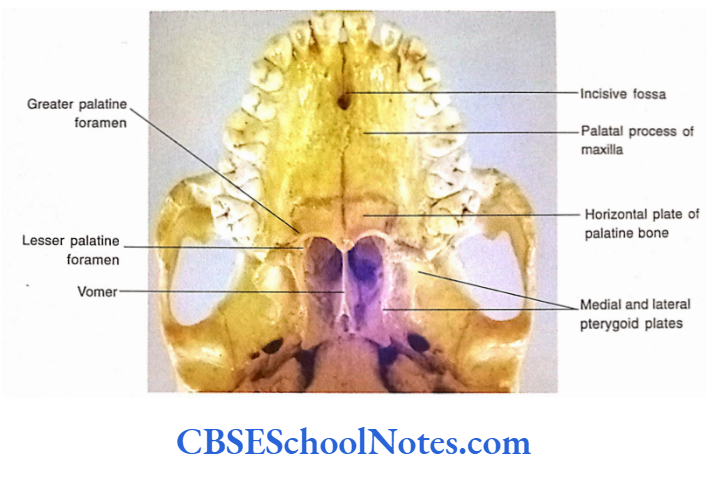
To visualize the base of the skull, it is necessary to detach the mandible from the rest of the skull. The base of the skull is formed, from anterior to posterior, by maxillae, palatine, vomer, sphenoid, temporal and occipital bones.
For the convenience of description, the norma basalis is divided into anterior, middle, and posterior parts by two imaginary horizontal lines.
The first imaginary horizontal line is drawn along the posterior border of the hard palate and the second line passes through the anterior margin of the foramen magnum.
Anterior Part of the Norma Basalis Externa
It is formed by the alveolar arch of the maxilla and hard palate.
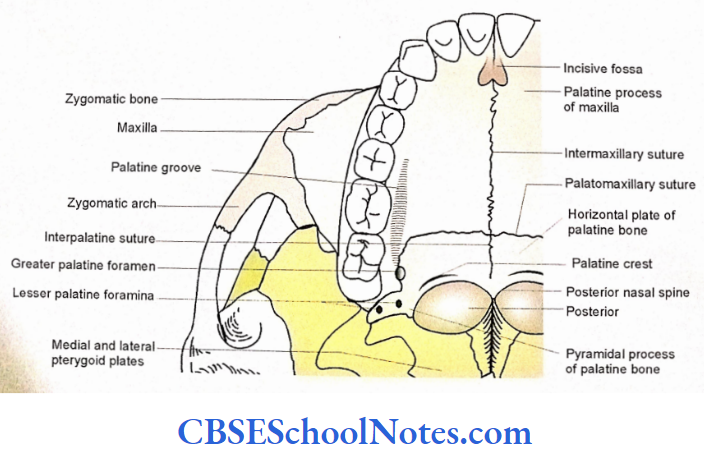
Alveolar Arch
The alveolar arch is formed by the alveolar processes of the right and left maxillae. It is horseshoe-shaped and possesses the sockets for the roots of the teeth of the upper jaw.
Skull Regions
Hard Palate
- The hard palate lies within the alveolar arch.
- The anterior 2/3 of the hard palate is formed by the palatine processes of the right and left maxillae.
- The posterior 1/3 is formed by the horizontal plates of palatine bones.
Hard Palate Features
Sutures (joints) and foramina are seen in the anterior part of the norma basalis.
Intermaxillary, interpalatine, and palato maxillary sutures. All the above three sutures are collectively called cruciform sutures.
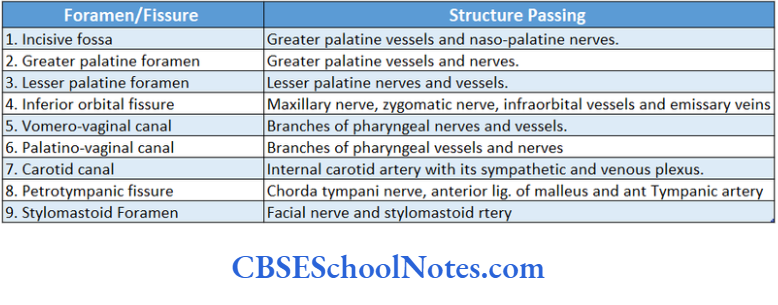
The Greater Palatine Foramen
- It is situated just medial to the third molar, posterior to the palatomaxillary suture.
- A groove rims forward from this foramen. This foramen transmits greater palatine vessels and nerves.
The Lesser Palatine Foramina
- These are two to three small foramina situated behind the greater palatine foramen. These foramina are present in the pyramidal process of the palatine bone.
- The lesser palatine vessels and nerves pass through these foramina. The Incisive Fossa It is a triangular depression in the median plane behind the central incisor teeth.
- The right and left lateral walls of the fossa bear lateral incisive foramen, which communicate with the floor of the nasal cavity. It gives passage to the nasopalatine nerve and greater palatine vessels.
- Pyramidal Process of the Palatine Bone It occupies the gap between the lower end of the medial and lateral pterygoid plates.
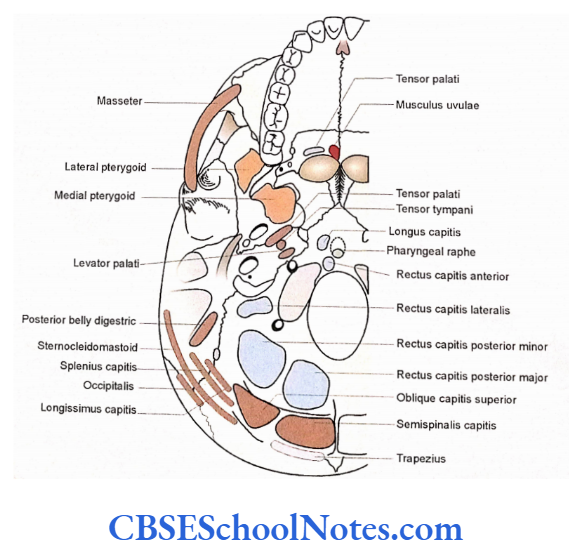
The Posterior Nasal Spine
It is a midline projection from the posterior border of the hard palate. It gives attachment to the musculus uvulae on each side.
Palatine Crest
It is a curved ridge a little in front of the posterior border of the hard palate. It gives attachment to the palatine aponeurosis and the tendon of tensor veli palatini.
Premaxilla
It is a triangular piece of maxilla holding four incisor teeth. In young persons a suture may be seen running from the posterior part of the incisive fossa laterally between the lateral incisor and canine teeth, separating the premaxilla from the rest of the maxilla.
The Middle Part of the Norma Basalis Externa
The middle part extends between two imaginary lines, i.e., the anterior line drawn along the posterior border of the hard palate and a posterior line drawn along the anterior margin of the foramen magnum.
The structures present in the region are divided into median areas and right and left areas.
The bones present in the median area, from anterior to posterior are
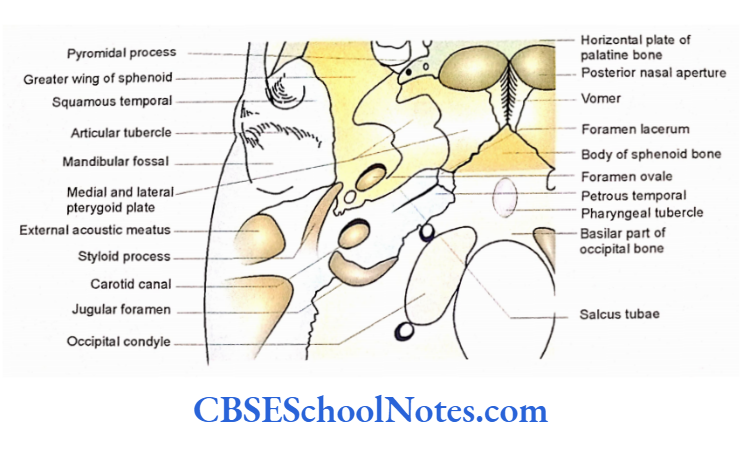
- The posterior border of the vomer.
- Body of sphenoid.
- Basilar part of the occipital bone.
The bones in the lateral area are:
- Medial and lateral pterygoid plates on the right and left side. These plates are the part of the sphenoid bone.
- The infratemporal surface of the greater wing of the sphenoid. It is situated lateral to the pterygoid plates.
- Temporal bone with its squamous, tympanic, and petrous parts.
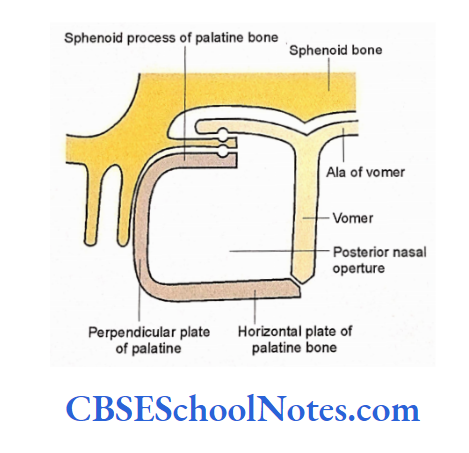
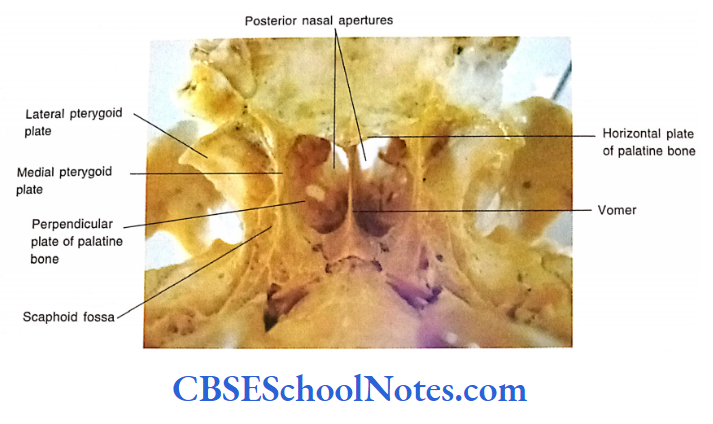
Posterior Nasal Apertures and Related Structures Features
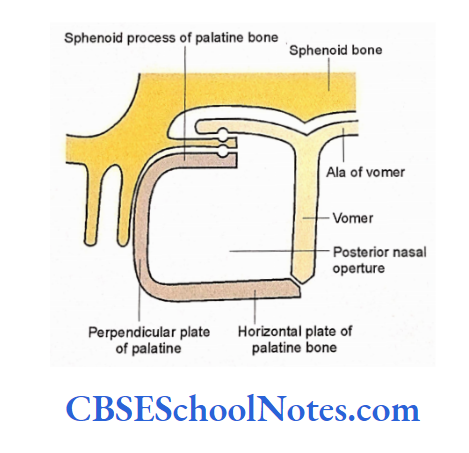
The Posterior Nasal Apertures and Related Structures These are quadrilateral in shape and situated above the posterior margin of the hard palate.
- The posterior border of the vomer separates the right and left apertures from each other, thus forming the medial boundary of each aperture.
- The superior surface of the horizontal plate of palatine bone forms the floor of the posterior nasal aperture.
- Laterally, each aperture is bounded by the perpendicular plate of palatine bone, which articulates with the medial pterygoid plate, posteriorly.
- The roof of the aperture is formed by the ala of the vomer and the sphenoidal process of the palatine bone.
The upper border of the vomer splits into two alae close to the inferior surface of the body of the sphenoid.
The midline groove between two alae of the vomer articulates with the sphenoidal rostrum (which is a midline ridge on the inferior surface of the body of the sphenoid).
The undersurface of the ala of the vomer, on each side, is overlapped by the vaginal process, which arises from the root of the medial pterygoid plate.
There exists a narrow vomer original canal between the undersurface of the ala of the vomer and the upper surface of the vaginal process.
It is present occasionally and gives passage to the pharyngeal vessels and nerves. From the upper end of the perpendicular plate of the palatine bone, there extends a sphenoidal process medially, which overlaps the undersurface of the vaginal process.
A narrow canal is present between the undersurface of the vaginal process and the superior surface of the sphenoidal process.
It is called as palatinovaginal canal and gives passage to the pharyngeal vessels and nerves. The vomerovaginal canal is situated posteriorly as compared to the palatinovaginal canal.
The Median Bar of Bone
- Just behind the alae of vomer bone there is the presence of a broad bar of bone in the midline. It extends upto the foramen magnum. It is formed by two bones, i.e.,
- Under the surface of the body of the sphenoid and basilar part of the occipital bone. These two bones (body of sphenoid and occipital bone) remain separated from each other by a cartilaginous synchondrosis joint which later fuses at about 25 years of age.
- A median elevation is seen just in front of the foramen magnum. It is known as the pharyngeal tubercle, which gives attachment to pharyngeal raphae and fibers of the superior constrictor.
- Note the attachment of longus capitis and rectus capitis anterior on the basilar part of the occipital bone.
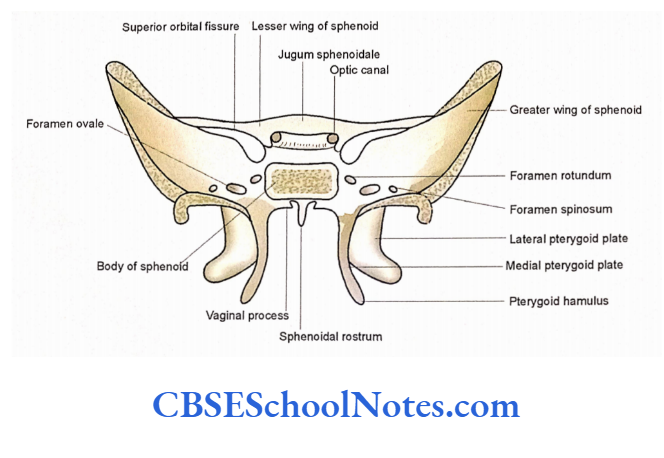
Pterygoid Processes
- Each pterygoid process descends vertically downwards from the junction of the body and the greater wing of the sphenoid.
- The anterior surface of the root of the pterygoid process forms the posterior wall of the pterygopalatine fossa.
- The pterygoid process consists of medial and lateral pterygoid plates.
- The pterygoid plates unite anteriorly and enclose a fossa (pterygoid fossa), which faces posterolaterally.
- The anterior surface of the fused medial and lateral pterygoid plates form the posterior boundary of the pterygomaxillary fissure.
- At the lower end, a gap between medial and lateral pterygoid plates is occupied by the pyramidal process of the palatine bone
The Medial Pterygoid Plate
- Trace above the posterior border of the medial pterygoid plate. It ends in a small fossa the “scaphoid fossa”. It gives attachment to the tensor veli palatini.
- The lower end of its posterior border projects downwards and laterally as a hook, the hamulus. Around the hamulus, the tendon of tensor veli palatini turns medially to enter the soft palate. The hook of the hamulus also gives attachment to the pterygomandibular raphe.
- Its posterior border gives attachment to the pharynx basilar fascia.
- An angular process (process tubarius) projects backward from the middle of the posterior border of the medial pterygoid plate. This process supports the medial end of the auditory tube.
- The lower end of the posterior border with the pterygoid hamulus gives origin to the superior constrictor muscle.
The Lateral Pterygoid Plate
- The medial surface of the lateral pterygoid plate gives origin to the deep head of the medial pterygoid muscle.
- Its lateral surface gives origin to the lower head of the lateral pterygoid muscle.
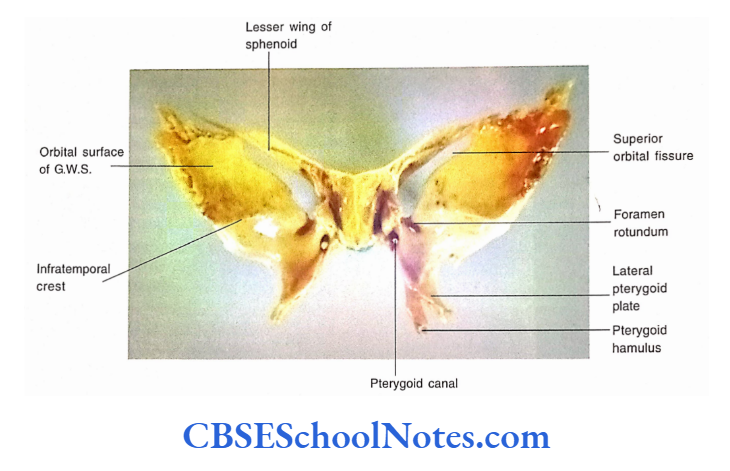
Infratemporal Surface of the Greater Wing of Sphenoid
This surface of the greater wing of the sphenoid extends laterally from the root of the lateral pterygoid plate. It is pentagonal and forms the roof of the infratemporal fossa.
- Anteriorly it forms the posterolateral border of the inferior orbital fissure.
- Laterally the surface is limited upto the infratemporal crest. Beyond this crest, the greater wing extends to the temporal surface.
- Postero-laterally it articulates with the squamous part of the temporal bone.
- Posteromedially it articulates with the petrous part of the temporal bone. At the junction of these two bones, a sulcus is formed, which is known as sulcus tubae.
The sulcus lodges the cartilaginous part of the auditory tube
The posterior-most of this bone projects down as the spine of the sphenoid.
The spine of the sphenoid gives attachment to:
Ligaments-Sphenomandibular, pterygospinous, and anterior ligament of the malleus.
Muscles-Posterior fibers of tensor veli palatine.
Related structures- Auriculotemporal nerve (laterally) chorda tympani nerve and auditory tube (medially).
The infratemporal surface of the greater wing of the sphenoid gives origin to the upper head of the lateral pterygoid muscle.
This surface presents two foramina, i.e., foramen ovale and spinosum. The foramen ovale is oval and presents posterolateral to the root of the lateral pterygoid plate. Foramen spinosum is small rounded foramen situated posterolateral to foramen ovale.
It is present anteriomedial to the spine of the sphenoid. Sometimes a small foramen may be seen medial to the foramen ovale, emissary sphenoidal foramen.
The Infratemporal Surface of the Squamous Part of the Temporal Bone This part is present posterolateral to the greater wing of the sphenoid and along with the infratemporal surface of the greater wing of the sphenoid it also forms the roof of the infratemporal fossa.
When a zygomatic process is traced backward this surface presents a tubercle (tubercle of the root of zygoma) where the zygomatic process divides into anterior and posterior roots.
The anterior root runs medially anterior to the mandibular fossa and bears an articular tubercle.
The posterior root forms the lateral boundary of the mandibular fossa. Behind the articular tubercle, the mandibular fossa is deep depression.
Both the articular tubercle and mandibular fossa, are articular and articulates with the head of the mandible.
The posterior part of the mandibular fossa is non-articular and formed by the tympanic plate of the temporal bone.
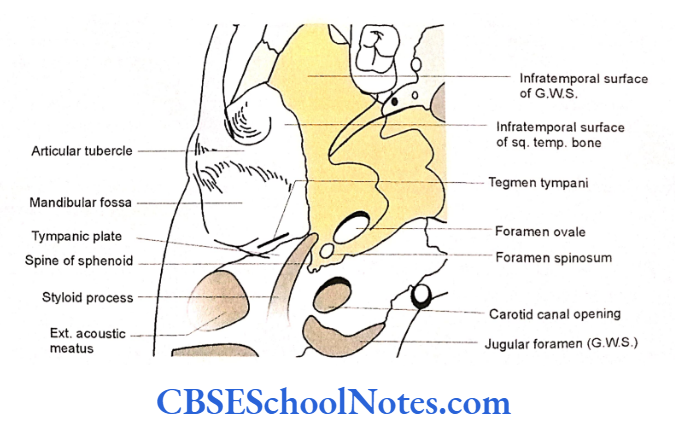
The Tympanic Part of the Temporal Bone
- The tympanic plate forms the anterior wall, floor, and lowermost part of the posterior wall of the external acoustic meatus.
- The squamous part of the temporal bone and tympanic plate unite with each other at the squamotympanic fissure, which is present on the floor of the mandibular fossa.
- The tegmen tympani part of the petrous temporal bone may project in the medial part of the squamotympanic fissure.
- The presence of the tegmen tympani divides the squamotympanic fissure into a petrosquamous fissure and a petrotympanic fissure.
- The petro-tympanic fissure gives passage to chorda tympani nerve, anterior tympanic artery and anterior ligament of malleus.
The Inferior Surface of Petrous Part of the temporal bone
The petrous part of the temporal bone is situated behind the greater wing of the sphenoid and lateral to the body of the sphenoid and basilar part of the occipital bone.
The apex of the bone is separated from the body of the sphenoid, the root of the pterygoid process, and the basilar part of the occipital bone by the foramen lacerum.
The carotid canal opens in the posterior wall of the foramen lacerum, while the pterygoid canal opens into its anterior wall. The upper part of the foramen lacerum is traversed by the internal carotid artery.
The nerve to the pterygoid canal is formed in the foramen lacerum by the union of the greater superficial petrosal and deep petrosal nerves. The nerve then passes through the pterygoid canal and enters the pterygopalatine fossa.
A quadrilateral area behind the apex of the petrous bone gives origin to tire levator veli palatini.
The lower opening of the carotid canal is situated just behind the quadrilateral area the inferior surface of the petrous temporal bone.
It transmits the internal carotid artery. Posterior to the lower opening of the carotid canal there lies the jugular fossa.
The sulcus tube is a groove, which lies between the posteromedial margin of the greater wing of the sphenoid and the petrous part of the temporal bone. It is occupied by the cartilaginous part of the auditory tube.
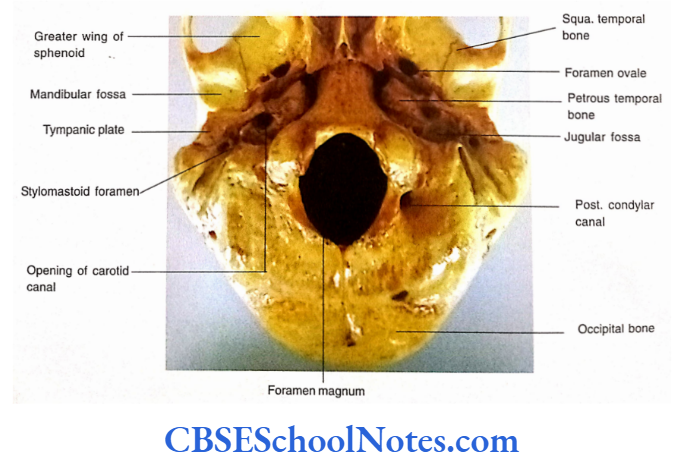
The Posterior Part of the Norma Basalis Externa
- The posterior part lies behind the imaginary line drawn along the anterior margin of the
foramen magnum. This part is also divided into median area and two lateral areas: - The median area consists of the foramen magnum and the squamous part of the occipital bone behind it.
- The condylar parts of the occipital bone are present on either side of the foramen magnum.
- The basilar part of the occipital bone lies anterior to the foramen magnum The bones in the lateral area, on each side, are the mastoid and styloid process.
The Median Area
The foramen magnum is large and oval. It connects the posterior cranial fossa above with the vertebral canal below.
The Basilar Part
The basilar part of the occipital bone is in The basilar part of the occipital bone is in sphenoid bone. These two bones are separated from each other by a primary cartilaginous joint in young but fuse in adults.
The pharyngeal tubercle is a small tubercle present on the inferior is a small tubercle present on the inferior attachment to the pharyngeal raphe.
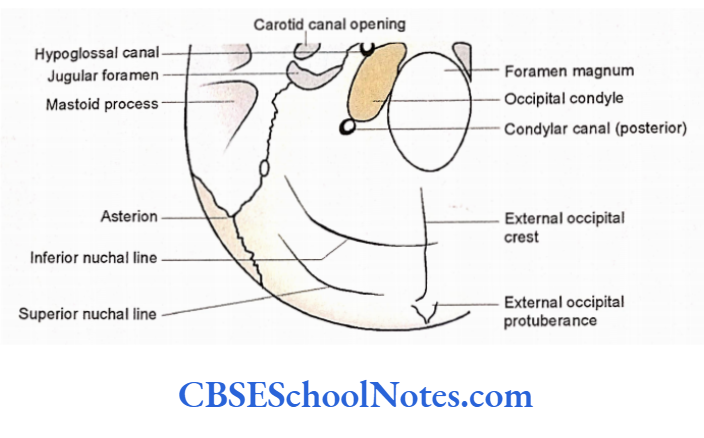
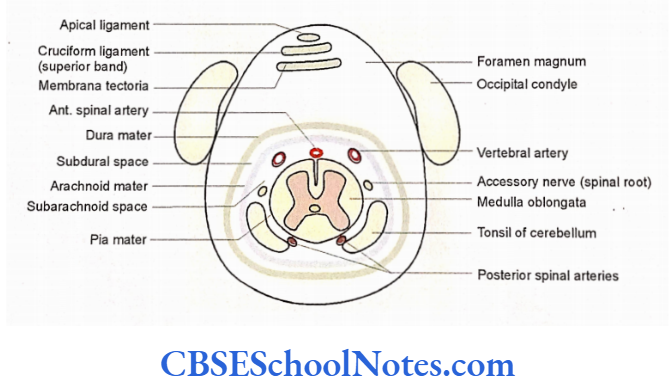
The Foramen Magnum
The alar ligaments, which are attached to the lateral margins of the foramen magnum, divide the foramen into small anterior and large posterior parts.
The structures passing through the anterior and posterior parts are shown. The anterior and posterior margins of the foramen magnum give attachment to the anterior and posterior atlanto-occipital membranes respectively.
The Condylar Parts
The condylar parts of the occipital bone consist of right and left occipital condyles, which are situated on each side of the foramen magnum. The jugular process is present lateral to each condyle. The condyles are set obliquely and their inferior surface is convex and articular.
Each condyle articulates with the corresponding upper surface of the lateral mass of the atlas vertebra (superior articular facet) to form an atlantooccipital joint.
There is an opening of the hypoglossal or anterior condylar canal on the lateral border of the condyle near its anterior end. It gives passage to the hypoglossal nerve, emissary vein, and meningeal branch of the ascending pharyngeal artery.
A condylar fossa is present posterior to each condyle which may show the presence of a canal which may show the presence of a canal to the emissary vein which connects the sigmoid sinus to occipital veins.
The jugular process articulates laterally with the petrous temporal bone by a primary cartilaginous joint. The anterior margin of the jugular process is free and known as the jugular notch. The jugular notch forms the posterior boundary of the jugular foramen.
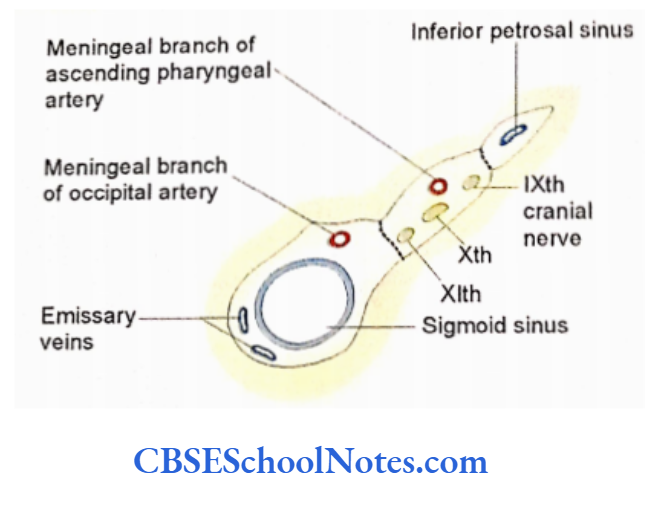
The Jugular Foramen
- This irregular large foramen is bounded anteriorly by the posterior border of the petrous temporal bone and posteriorly by the jugular notch of the jugular process of the occipital bone.
- It is divided into anterior, middle, and posterior parts. The posterior part of the jugular foramen presents a jugular fossa, which is due to the presence of depression in the petrous temporal bone.
- The mastoid canaliculus is an opening of a minute canal in the lateral wall of the jugular fossa which transmits the auricular branch of the vagus.
- The tympanic canaliculi are present on the ridge between the jugular fossa and the lower opening of the carotid canal. The structures pass through three divisions of the jugular foramen.
The Squamous Part ligament
This part lies behind the foramen magnum. In the midline, there extends an external occipital crest between the foramen magnum and the external occipital protuberance.
The upper end of the ligamentum nuchae is attached to the crest and protuberance. The superior and inferior nuchal lines and attachment of muscles in this area have already been described in “norma occipitalis”.
The Lateral Area
- In the lateral area, there are three important structures, i.e., styloid process, mastoid process, and stylomastoid foramen.
- Styloid Process It is a long conical process, which projects downwards, forwards, and medially below the tympanic part of the temporal bone.
- It lies lateral to the jugular fossa.
- It gives attachment to 3 muscles and two ligaments.
- It is related laterally to the parotid gland and medially to the internal jugular vein.
- Near its base, it is crossed by the facial nerve.
Mastoid Process
- It is a conical projection from the mastoid part of the temporal bone. The mastoid process is situated posterolateral to the styloid process.
- A deep groove (digastric groove) is seen on its medial aspect, which gives attachment to the posterior belly of the digastric muscle.
Stylomastoid Foramen
The stylomastoid foramen is present between styloid and mastoid processes, i.e., posterolateral to the styloid process and anteromedial to the mastoid process. The stylomastoid artery and facial nerve pass through it.
The Interior Of The Skull
- When the upper part of the vault of the skull (skull cap or calvaria) is removed we may see the inner surface of the cranial vault and the interior of the base of the skull.
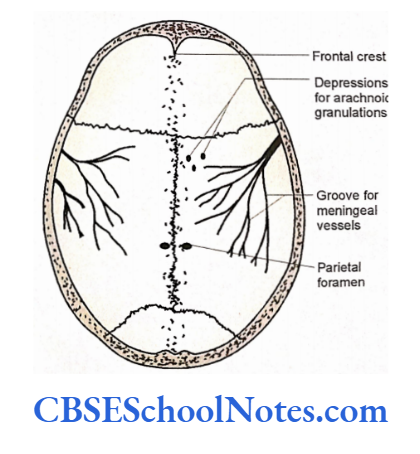
Inner Surface of the Cranial Vault
- The various bones and the intervening sutures forming the cranial vault are the same as observed in the norma verticalis.
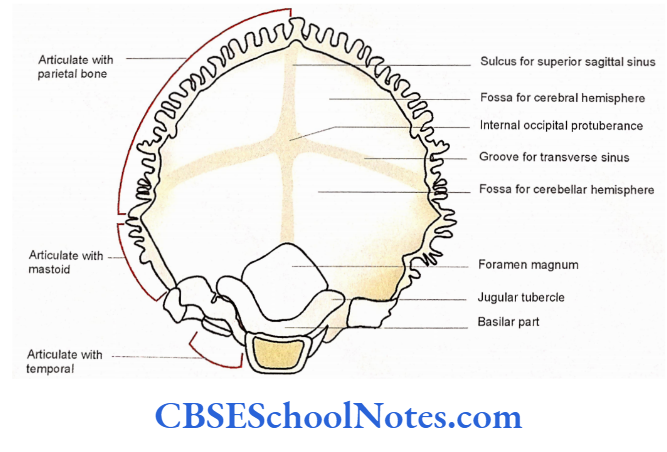
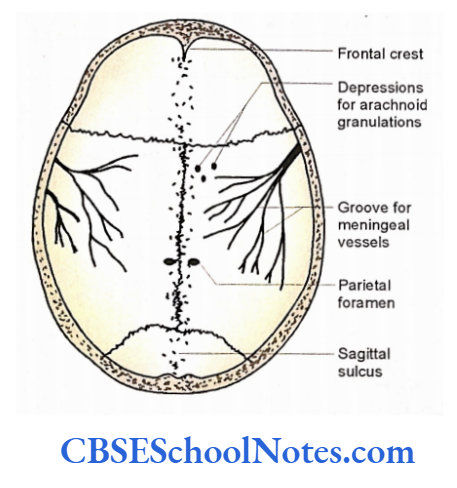
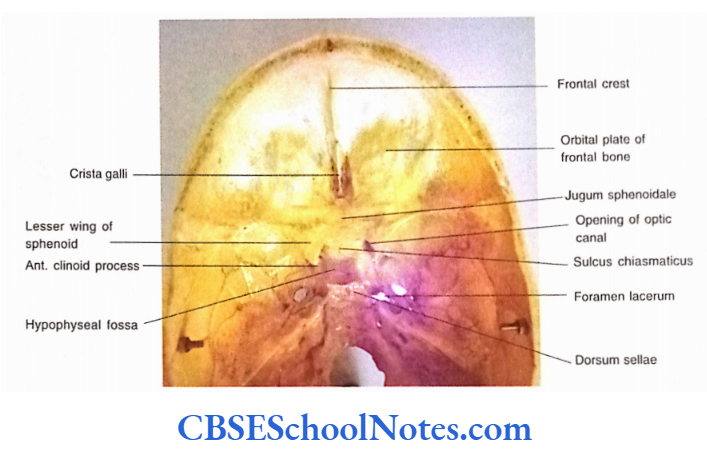
- The frontal crest is the midline structure present most anteriorly
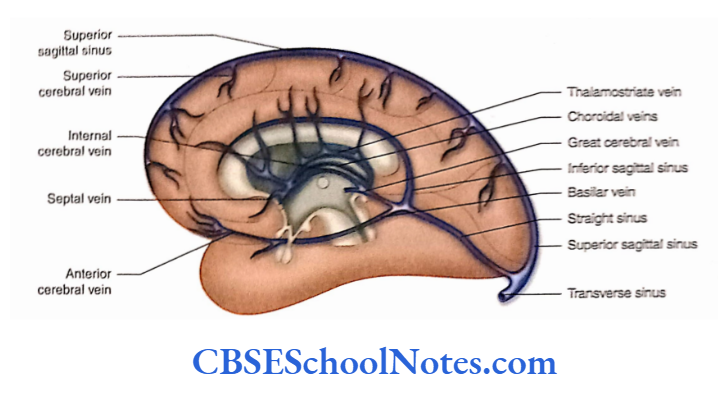
- A groove extends anteroposteriorly in the median plane, from the frontal crest to the internal occipital protuberance. This groove is known as the sagittal sulcus.
- The superior sagittal sinus is lodged in the sagittal sulcus. At the internal occipital protuberance, this sinus becomes continuous with the right transverse sinus.
- The frontal crest and the margins of the sagittal sulcus give attachment to the falx cerebri.
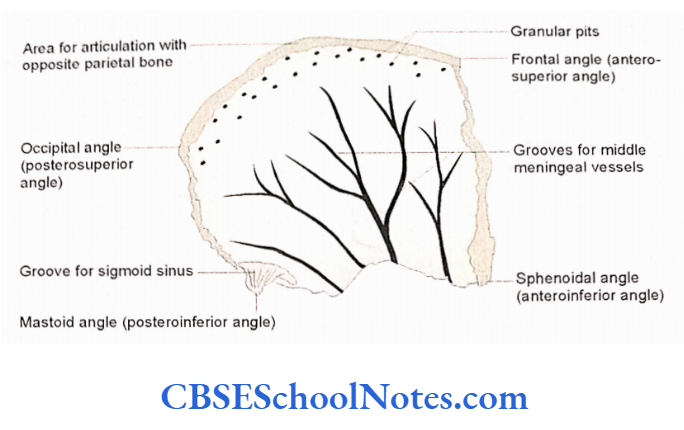
- Many small depressions {granular pits) are observed on each side of the sagittal sulcus. These are produced by the arachnoid granulations. Their number increases with the increasing age.
- Note the presence of parietal foramen on either side of the sagittal suture about 3.5 cm anterior to lambda. These foramina transmit emissary veins.
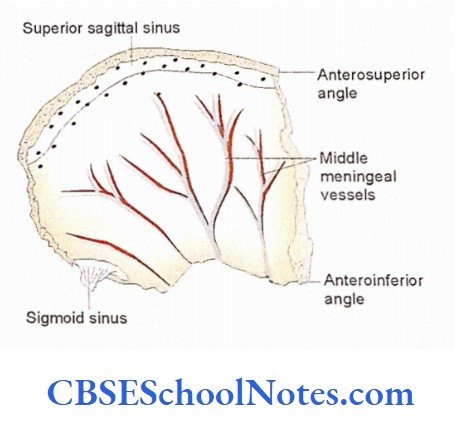
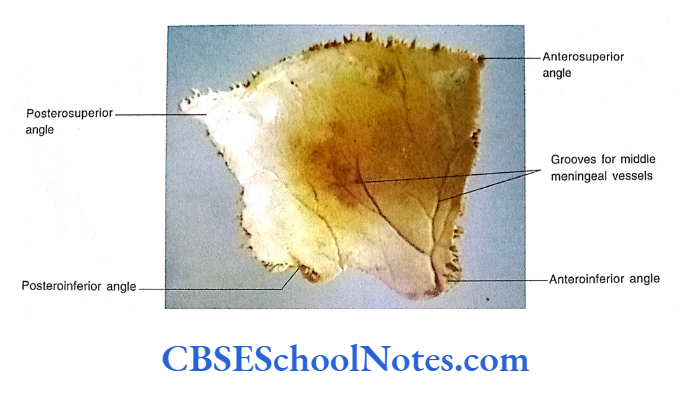
- The inner aspect of the calvaria shows the presence of grooves for the meningeal vessels. These grooves run backward and upwards from the anteroinferior angle of the parietal bone.
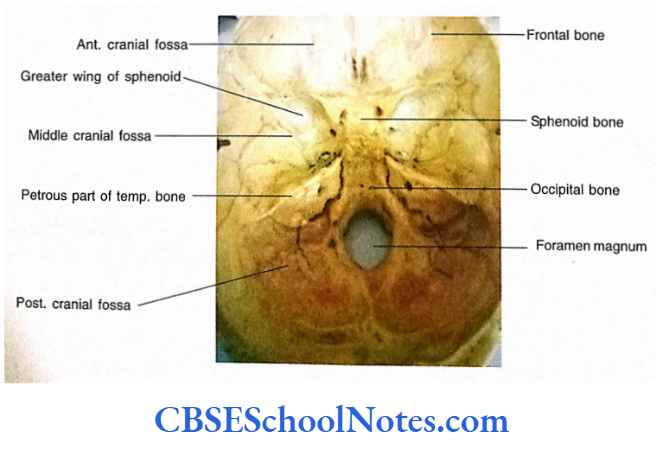
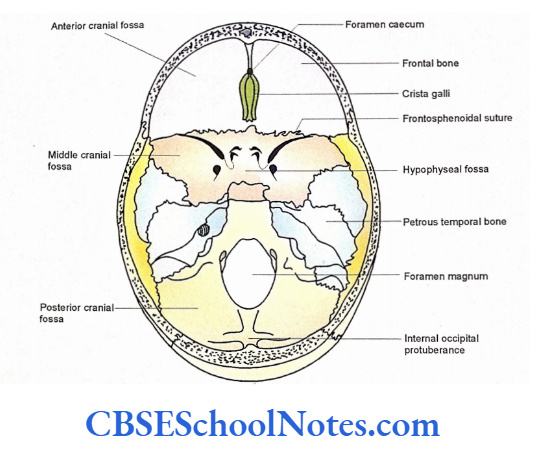
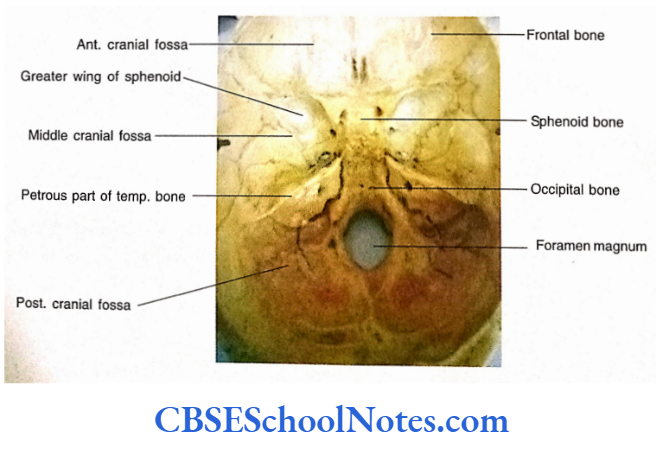
Interior of the Base of the Skull
The internal aspect of the base of the skull (norma basalis internal) as seen after the removal of the skull cap, can be divided into three fossae, i.e., anterior, middle, and posterior cranial fossae
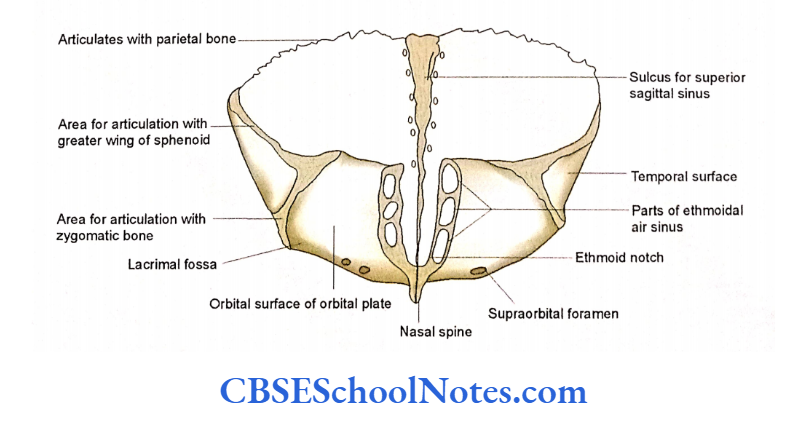
The Anterior Cranial Fossa
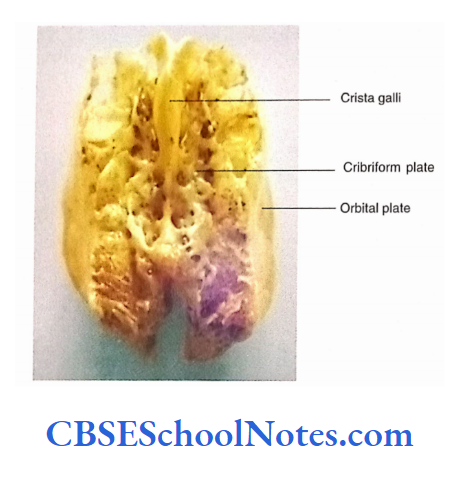
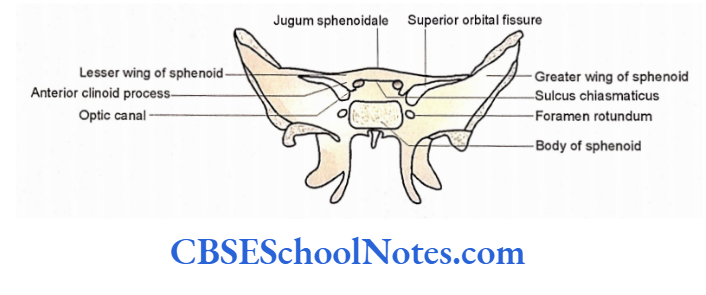
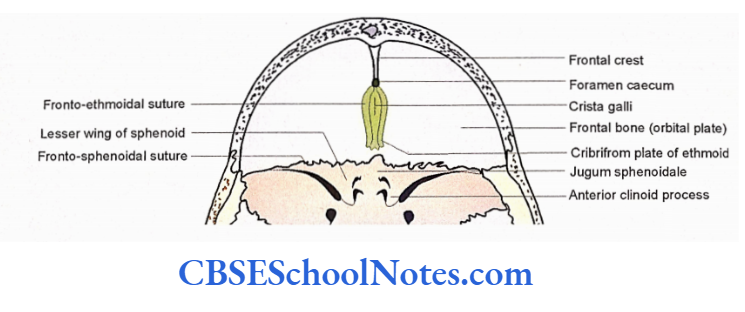
Bones of the Anterior Cranial Fossa The anterior cranial fossa is formed by the frontal bone, cribriform plate of the ethmoid, lesser wing of the sphenoid, and the anterior part of the superior surface of body of the sphenoid (jugum sphenoidal).
Sutures of the Anterior Cranial Fossa
With the help of identifying frontoethmoidal, frontosphenoidal, and sphenoethmoidal sutures.
Borders
The anterior and lateral boundaries of the fossa are formed by the frontal bone.
The posterior boundary is formed by the posterior border of the lesser wing of the sphenoid, the anterior clinoid process, and the anterior border of the sulcus chiasmaticus.
Floor
In the median region, the floor is formed by the cribriform plate of ethmoid and jugum sphenoidal.
While, the lateral region of the floor is formed by the orbital plates of the frontal bone and the lesser wings of the sphenoid, on each side.
Median Area of the Floor
- The most anterior structure in the midline is the frontal crest.
- Posterior to the frontal crest a triangular process, the crista galli, is seen. It projects upwards from the cribriform plate and provides attachment to the falx cerebri.
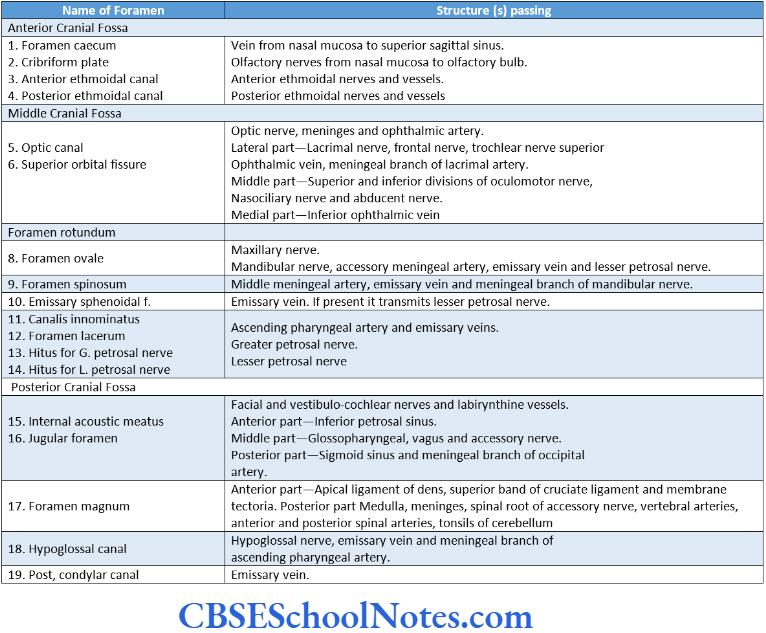
- Between the frontal crest and crista galli identify the foramen caecum. Sometimes it transmits a vein from the nasal mucosa to the superior sagittal sinus.
- The cribriform plate of ethmoid is present on either side of the crista galli between the orbital plates of the frontal bone. The cribriform plate separates the anterior cranial fossa from the nasal cavity.
- It presents many small apertures through which pass the olfactory nerves from the nasal mucosa to the olfactory bulb.
- On each side of the cribriform plate, there is an opening of the anterior and posterior ethmoidal canals.
- The anterior canal transmits anterior ethmoidal vessels and nerves, while the posterior canal transmits only posterior ethmoidal vessels.
- Posterior to the cribriform plate the median area of the floor is formed by jugum sphenoidale of the body of the sphenoid. It forms the roof of the sphenoidal air sinus. Lateral Area of the Floor On each side it consists of an orbital plate and a lesser wing of the sphenoid.
- The orbital plate of the frontal bone lies lateral to the cribriform plate on either side. It is convex and shows the impre¬ ssions of cerebral gyri.
- Laterally it forms the roof of the orbit and medially the roof of the ethmoidal sinuses. Posteriorly, the orbital plates articulate with the anterior margin of the lesser wing of the sphenoid.
- The lesser wings of the sphenoid are continuous with the jugum sphenoidale medially. The posterior margin of the lesser wing is free and concave. It is related to the sphenoid-parietal sinus.
- The medial end of the posterior margin ends into the anterior clinoid process, which gives attachment to the free margin of tentorium cerebelli.
Middle Cranial Fossa
The middle cranial fossa is narrow in the middle and expanded laterally. It lodges hypophysis cerebri in the middle and temporal lobes of the brain on each side.
Boundaries
- The anterior boundary of the middle cranial fossa separates the anterior and middle fossae from each other.
- It is formed by the posterior border of the lesser wing of the sphenoid, anterior clinoid process and anterior border of the sulcus chiasmaticus.
- The posterior boundary separates it from the posterior cranial fossa.
- It is formed by the superior border of the petrous part of the temporal bone, posterior clinoid process, and dorsum sellae.
- On each side, the middle cranial fossa is bounded by the greater wing of the sphenoid, the squamous part of the temporal bone, and the parietal bone.
The floor of the Middle Cranial Fossa
It is shaped like a butterfly and consists of median and lateral parts.
Median Part of the Floor of the Middle Cranial Fossa
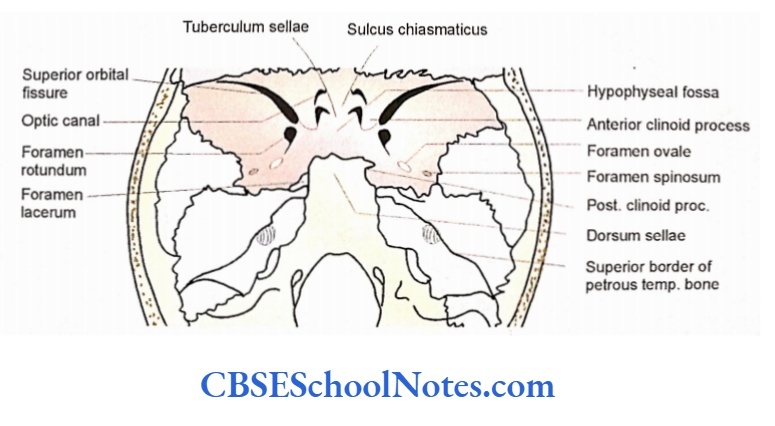
- The median part is formed by the body of the sphenoid. Most anteriorly sulcus chiasmaticus is present.
- It is a transverse groove, which becomes continuous laterally with the optic canal. The optic chiasma lies posterior to this groove.
- Each optic canal opens into orbit thus connecting the middle cranial fossa with orbit.
- It is bounded by anterior and posterior roots of the lesser wing and body of the sphenoid. This canal gives passage to the optic nerve, meninges, and ophthalmic artery.
- Behind the sulcus chiasmaticus, a saddle-shaped depression is present on the superior surface of the body of the sphenoid. It is known as sella turcica.
- The sella turcica consists of tuberculum shellac, hypophyseal fossa, and dorsum sellae from anterior to posterior. The tuberculum sellae is the median elevation just behind the sulcus chiasmaticus.
- It receives the attachment of the anterior margin of the diaphragm sellae. The hypophyseal fossa is a deep depression posterior to the tuberculum sellae. It lodges hypophysis cerebri. Deep to the hypophyseal fossa lies the sphenoidal air sinus.
- The dorsum sellae is a square-like vertical plate of bone posterior to the hypophyseal fossa. The superior border of the dorsum sellae, on each side forms the posterior clinoid process which gives attachment to the attached margin of the tentorium cerebelli. While the superior border itself gives attachment to the posterior margin of diaphragma sellae.
- On each side of the body of the sphenoid, there is the presence of a shallow groove called a carotid groove. This groove extends from the foramen lacerum to the medial side of the anterior clinoid process. It lodges the internal carotid artery.
Lateral Part of the Floor of Middle Cranial Fossa
Laterally the floor of the middle cranial fossa is formed by three bones, i.e., the cranial surface of the greater wing of the sphenoid, and squamous, and petrous parts of the temporal bone. Following fissures, foramina, and grooves are observed on the floor of the fossa.
The superior orbital fissure is a triangular oblique cleft present most anteriorly in the middle cranial fossa. It connects the middle fossa with the orbit.
The fissure is bounded above by the lesser wing of the sphenoid, below by the greater wing, and medially by the body of the sphenoid.
We have already seen that the fissure is divided into three parts by the attachment of a tendinous ring on the orbital surface of the fissure. The structures pass through three subdivisions of the superior orbital fissures.
The foramen rotundum is situated in the greater wing of the sphenoid just inferomedial to the medial end of the superior orbital fissure.
It opens anteriorly into the pterygopalatine fossa and transmits the maxillary nerve.
The foramen ovale is situated in the greater wing of the sphenoid posterolateral to the foramen rotundum. It opens into the infratemporal fossa and transmits the mandibular nerve.
The foramen spinosum is also present in the greater wing of the sphenoid, posterolateral to the foramen ovale, and communicates with the infratemporal fossa.
It gives passage to the middle meningeal artery and other structures.
Sometimes the emissary sphenoidal foramen is present between foramen rotundum and foramen ovale.
It transmits the emissary vein. Similarly, sometimes a foramen is present between foramen ovale and spinosum, which transmits lesser petrosal nerve. It is called as foramen innominatum.
The foramen lacerum is situated posteromedial to foramen ovale, between the body of the sphenoid and the apex of the petrous temporal bone.
The carotid canal opens in its posterolateral part. The carotid artery traverses the upper part of the foramen lacerum. The pterygoid canal opens in its anterior margin and gives passage to the nerve of the pterygoid canal.
In the lateral part of the floor, the markings of the middle meningeal vessels are seen. The groove runs forward and laterally from the foramen spinosum and later divides into two anterior and posterior branches of the middle meningeal artery.
The anterior surface of the petrous temporal bone forms the posterior wall of the middle cranial fossa. Near the apex, a shallow depression is seen. It is known as trigeminal impression for the trigeminal ganglion.
Arcuate eminence is a prominent elevation deep to which lies the superior semicircular canal.
The area lateral to the eminence is formed by the thin plate of bone called tegmen tympani.
This forms the roof of the middle ear cavity and auditory tube. The anterior surface of the petrous temporal bone presents two grooves running downwards and medially.
The upper and medial groove begins at the hiatus for the greater superficial petrosal nerve and runs towards the foramen lacerum. It lodges a greater superficial petrosal nerve.
The lower and lateral groove begins at the hiatus for the lesser petrosal nerve and runs towards the foramen ovale.
It lodges lesser petrosal nerves.
The superior border of the petrous bone is grooved for the lodgement of the superior petrosal sinus. Near the apex of the petrous temporal bone, this border is 184 crossed by the trigeminal nerve. This border also gives attachment to the tentorium cerebelli.
Posterior Cranial Fossa
The posterior cranial fossa is the deepest of the three fossae and lodges the hindbrain (cerebellum, pons, and medulla).
Bones Forming the Posterior Cranial Fossa
- Posterior part of the body of the sphenoid.
- Occipital bone.
- The posterior surface of the petrous temporal bone.
- Mastoid part of the temporal bone.
- Posteroinferior angle of parietal bone.
Sutures and Fissures of the Posterior Cranial Fossa
- The lower end of lambdoid suture between parietal and occipital bone.
- The parieto-mastoid suture.
- The occipito-mastoid suture.
- Petro-occipital suture.
Boundaries
The middle and posterior cranial fossa are separated from each other by the dorsum sellae, posterior clinoid process, and superior border of the petrous temporal bone.
On the lateral side, this fossa is bounded by the mastoid part of the temporal bone and the postero-inferior angle of the parietal bone.
Posteriorly, it is bounded by the squamous part of the occipital bone. The Floor of the Posterior Cranial Fossa The floor can be divided into median and lateral parts.
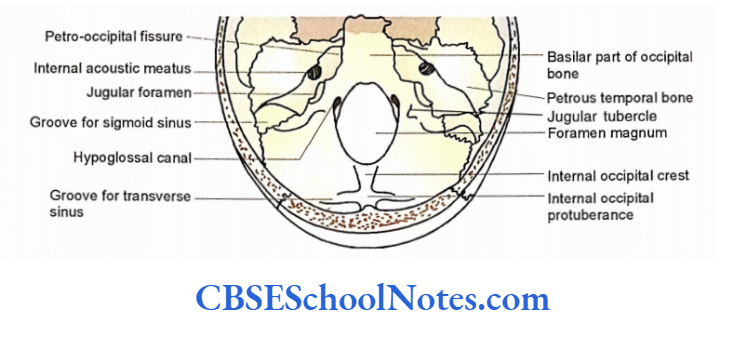
The Median Part of the Floor
The median part of the floor presents the most striking structure, i.e., the foramen magnum. The part anterior to the foramen magnum is called as clivus. The parts posterior to the foramen magnum are the internal occipital crest and internal occipital protuberance.
- The clivus is the sloping surface of the bone formed by the fusion of the basal part of the occipital bone and the body of the sphenoid.
- The lateral border of the basilar part of the occipital bone is separated by the petrous temporal bone by a petrooccipital fissure, which lodges the inferior petrosal sinus.
- The basilar part of the clivus gives attachment to the membrane tectoria, the upper band of the cruciate ligament, and the apical ligament of dens.
- The foramen magnum is a large oval-shaped central opening on the floor of the posterior fossa. Structures passing through this foramen.
- On each side of the foramen magnum, the inner opening of the hypoglossal canal lies just above its lateral margin. It transmits the hypoglossal nerves and vessels. The jugular tubercle is situated between the jugular foramen and the hypoglossal canal.
- It is related to the 9th, 10th, and 11th cranial nerves. Sometimes the posterior condylar canal is also present behind the jugular foramen and lateral to the jugular tubercle. It transmits the emissary vein.
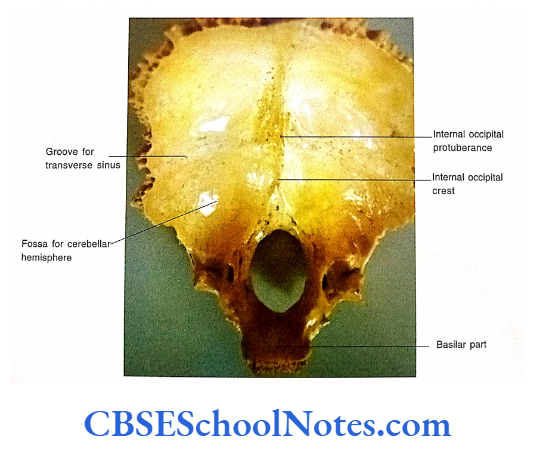
- The internal occipital crest is a ridge present in the midline, which extends between the foramen magnum and internal occipital protuberance. It gives attachment to the falx cerebelli.
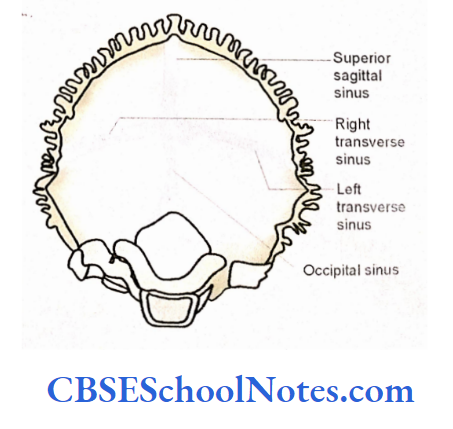
- The internal occipital protuberance is situated opposite the external occipital protuberance. On each side, it is related to the transverse sinus. It is also related to the confluence of dural venous sinuses.
The Lateral Part of the Floor
- The posterior surface of the petrous temporal bone, in its middle, shows the opening of the internal acoustic meatus.
- It transmits the facial and vestibulocochlear nerves and labyrinthine vessels. Posterolateral to the internal meatus there lies an oblique slit which leads upwards into a canal called the aqueduct of the vestibule. It lodges succus and ductus endolymphaticus.
- The right and left transverse sulci run laterally from each side of the internal occipital protuberance. The right sulcus is more prominent. The transverse sulcus lodges the transverse sinus.
- Each transverse sulcus curves downwards at the mastoid angle of the parietal bone as the sigmoid sulcus. The sigmoid sulcus runs downwards and medially with an S-shaped curve.
- It grooves the petrous and mastoid part of the temporal bone to reach the posterior end of the jugular foramen.
- The jugular foramen is situated between the posterior end of the petro-occipital fissure and the terminal end of the sigmoid sulcus Above it is bounded by the petrous temporal bone and below by the jugular process of the occipital bone. It is divided into anterior, middle, and posterior parts.
Nasal Cavity
The nasal cavity is divided into right and left halves by vertical median septum (i.e., the nasal septum). Each half of the cavity consists of an anterior opening, i.e., the anterior nasal aperture, a posterior nasal aperture, a lateral wall, a medial wall, a roof, and a floor.
Anterior and Posterior Nasal Apertures
The anterior nasal apertures open on the norma frontalis, while both posterior nasal apertures open on the base of the skull just above the posterior margin of the bony palate.
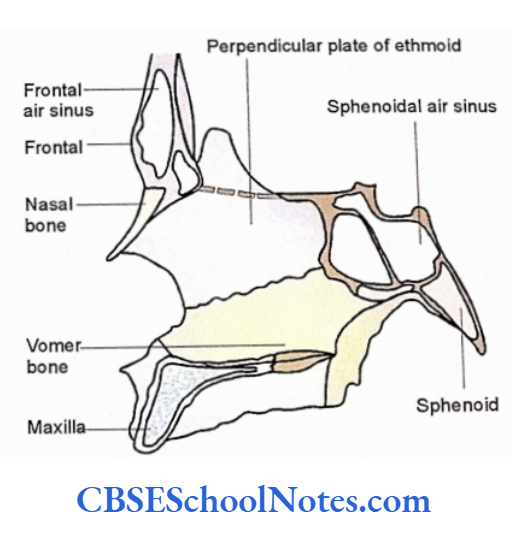
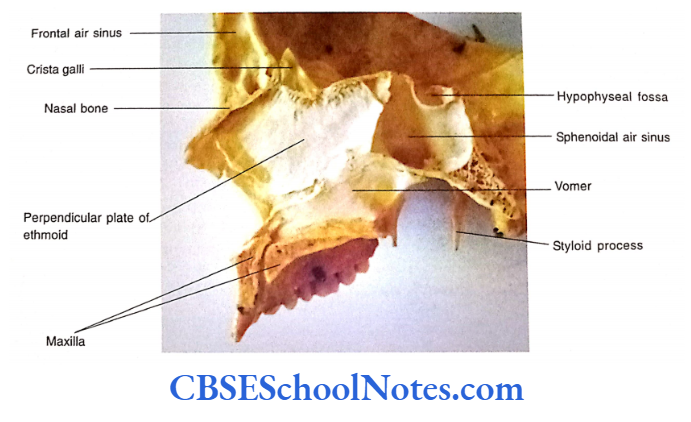
The Medial Wall
The medial wall, anterosuperiorly, is formed by the perpendicular plate of the ethmoid. While posteroinferiorly it is formed by the vomer bone. In the living condition, the anterior gap in the bony septum is filled by septal cartilage.
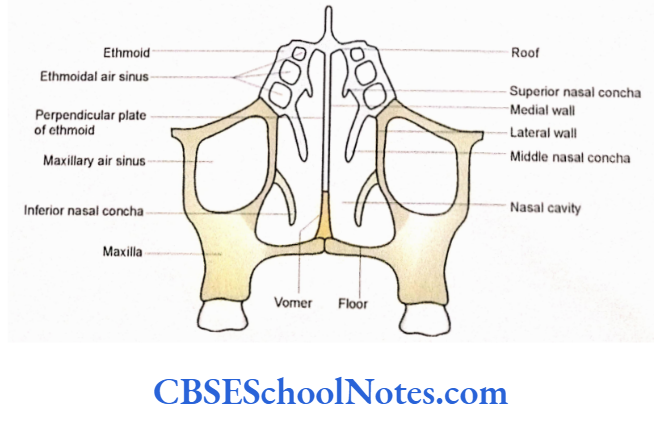
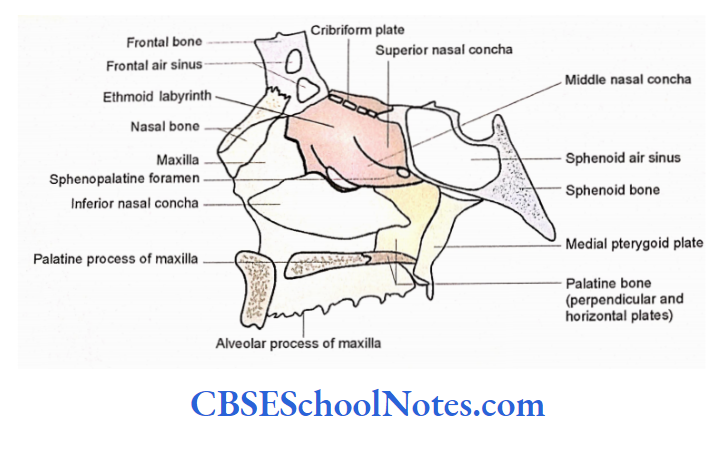
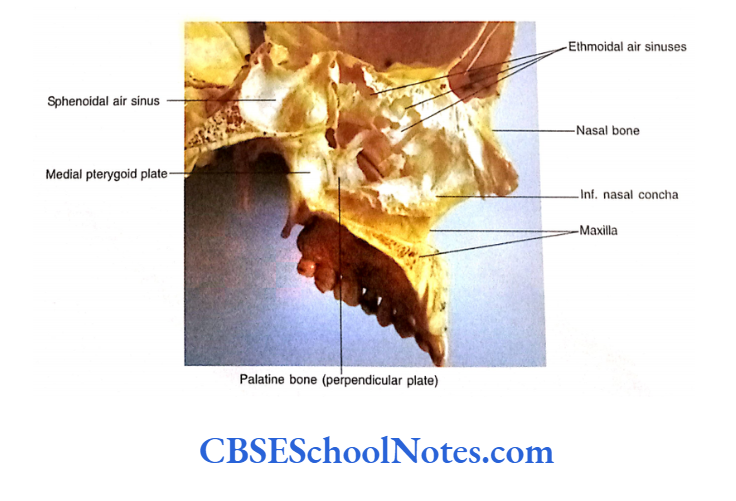
The Lateral Wall
The lateral wall is formed by three irregular bony projections, i.e., superior, middle, and inferior conchae.
These conchae run anterol posteriorly and lie one above the other. The spaces deep into the conchae are called meatuses, i.e., superior, middle, and inferior meatuses. The area above the superior concha is called a sphenoethmoidal recess. The following bones form the lateral wall of the nose.
- Ethmoid—The superior and middle conchae are part of the ethmoid bone.
- The inferior concha is a separate bone.
- Perpendicular plate of the palatine bone.
- Maxilla—All the above three bones are attached to the nasal surface of the maxilla.
- A part of the nasal surface of the maxilla remains free on the anterior and inferior part of the lateral wall of the nose
Roof
From anterior to posterior, the roof is formed by nasal bone, frontal bone, cribriform plate of the ethmoid, anterior surface of a body of the sphenoid, and ala of the vomer.
The nasal cavity communicates with the anterior cranial fossa through numerous apertures in the cribriform plate of the ethmoid bone.
Floor
It is formed by the palatine process of It is formed by the palatine process of In the anterior part of the floor there is the upper opening of the incisive canal.
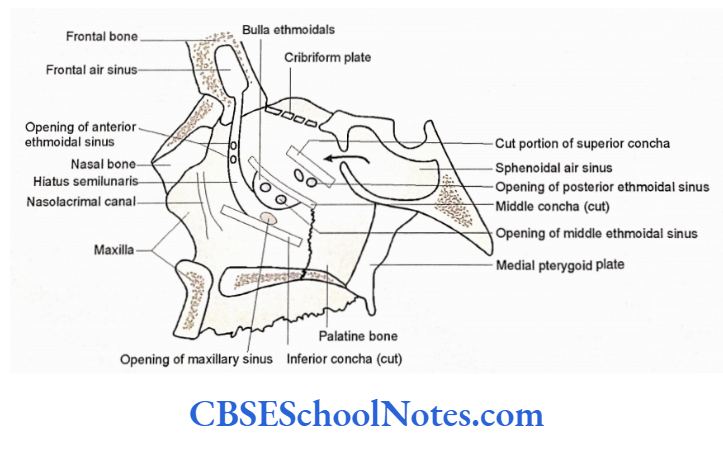
Further Details of Lateral Wall
Sphenoethmoidal Recess
It is situated above the superior concha and receives the opening of the sphenoid air sinus.
Superior Meatus
It is situated between the superior and middle conchae. It receives the opening of the posterior ethmoidal sinuses.
Middle Meatus
It is situated between the middle and inferior conchae. Deep to middle concha is a rounded prominence called the bulla ethmoidale.
It is produced by the middle ethmoidal air sinuses. The middle ethmoidal sinuses open on the bulla.
Antero-inferior to the bulla is a curved plate of bone called an uncinate process. It runs downwards and backward. The curved space between the uncinate process and bulla is called hiatus semilunaris. The hiatus semilunaris is continuous above and anteriorly into the infundibulum.
The infundibulum is continuous with the frontal air sinus. The anterior ethmoidal sinus also opens in the infundibulum. The maxillary air sinus opens behind the bulla at the posterior end of the hiatus semilunaris.
Inferior Meatus
It is present deep into the inferior concha and receives the opening of the nasolacrimal duct.
Sphenopalatine Foramen is present behind the superior concha and transmits the sphenopalatine artery and nasal branches of the pterygopalatine ganglion.
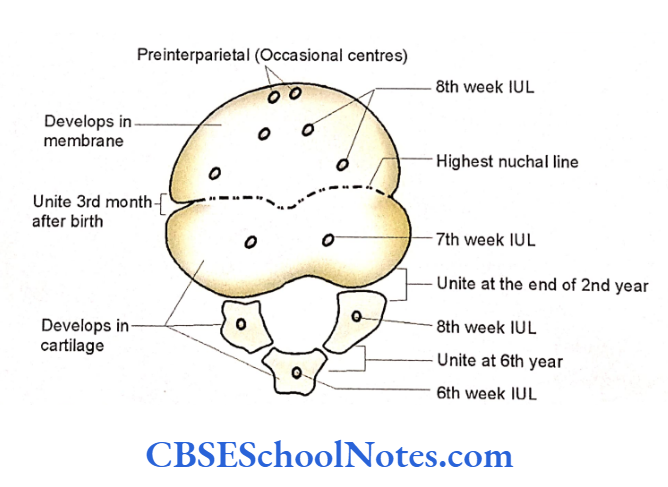
Skull Of The Newborn
The size of the cranium (brain box) is larger as compared to the facial skeleton. The brain box (calvaria) is large because of the rapid growth of the cerebrum.
The bones of the vault are ossified in membrane while the bones of the base of the skull are ossified in cartilage.
The size of the face at birth is small due to the following facts:
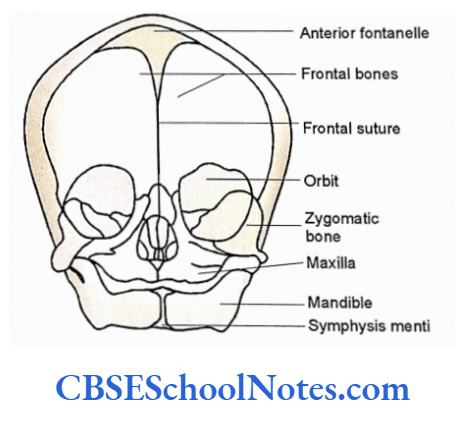
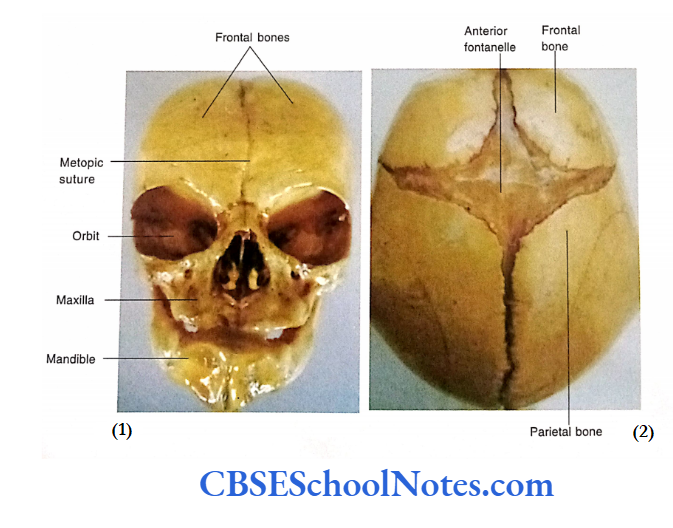
Norma Frontalis
- The glabella and superciliary arches are not well developed.
- The frontal bone is present in two halves, i.e., right and left separated by frontal suture.
- Small size of mandible and maxilla.
- Rudimentary maxillary air sinus.
- Non-eruption of teeth.
- The small size of the nasal cavity.
- The germs of developing teeth in the superior alveolar process are near the orbital floor.
- The paranasal sinuses are rudimentary or absent.
- The two halves of the mandible are united by the fibrous tissue at symphysis menti. These halves join each other at the end of the first year.
The Base Of The Cranium
- The cranial base is relatively short.
- Occipital and sphenoid bones are joined with each other by the cartilaginous joint.
- The squamous, lateral, and basilar parts of the occipital bone are separated from each other.
- The styloid process is not fused with the temporal bone.
- The mandibular fossa is flat and its articular tubercle is underdeveloped.
- The stylomastoid foramen is exposed on the lateral surface.
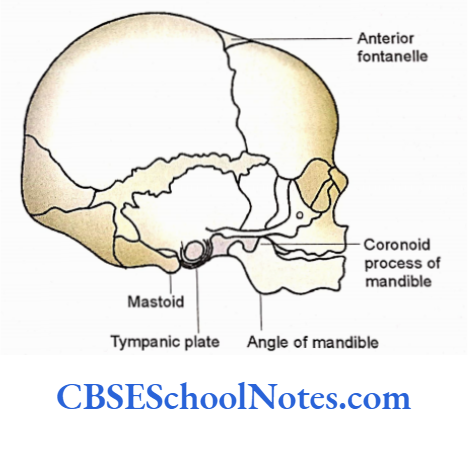
The Lateral View
- The mastoid process is absent
- The tympanic plate is represented by a C-shaped plate.
- The tympanic membrane is attached obliquely and exposed as the bony part of the external acoustic meatus is yet not developed.
- The cavities of the internal ear, middle ear, Lateral View Anterior fontanelle mastoid antrum, and three ear ossicles are of adult size at birth. However, the petrous temporal bone is much smaller.
- The angle of the mandible is obtuse 140 degrees
- The coronoid process is above the level of the head of the mandible
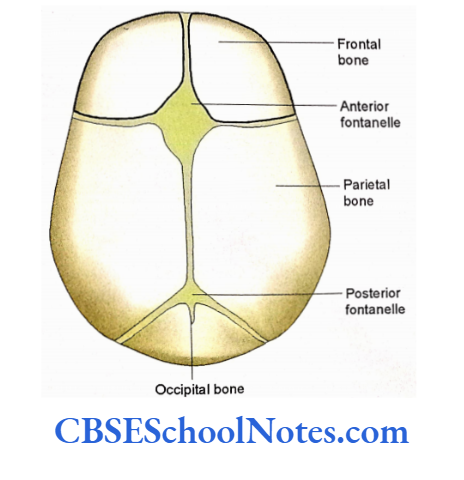
Norma Verticalis
- The bones of the vault are ossified in the membrane.
- The angles of the parietal bones are still membranous. Thus there are six fontanelles at four angles of both the parietal bones.
- The unpaired median fontanelles are called anterior and posterior fontanelles.
- Two lateral pairs of fontanelles are sphenoidal and mastoid fontanelle.
- The anterior fontanelle lies at the junction of sagittal, coronal, and frontal sutures.
- The posterior fontanelle lies at the junction of sagittal and lambdoid sutures.
- The sphenoidal and mastoid fontanelles are at the sphenoidal and mastoid angles of the parietal bones.
Anterior Fontanelle
The anterior fontanelle is present at the junction of frontal, coronal, and sagittal sutures hence, diamond-shaped. It measures about 4 cm in anteroposterior and 2.5 cm in transverse dimensions.
Deep to the anterior fontanelle lies superior sagittal sinus. It is usually closed between 18 months and 2 years of age.
Clinical Significance
- The bulging of the fontanelle indicates increased intracranial pressure.
- The depressed fontanelle indicates dehydration.
- As the superior sagittal sinus lies just deep to it blood can be withdrawn from the sinus.
- The intravenous transfusion of fluid or drugs is also possible through the superior sagittal sinus.
- The CSF can also be withdrawn from the lateral ventricle of the brain. For this a needle is introduced downwards and laterally at the lateral angle of the fontanelle.
- The fact, that the anterior fontanelle closes by the age of 2 years, is utilized to determine the age of the child.
- At the time of birth, fontanelle allows some overlap of the bones of the cranial vault. This helps in the reduction in the size of the foetal head during birth.
Hyoid Bone
Hyoid is a U-shaped bone present in the upper part of the neck.
It is not attached to any other bone but hangs at the level of the 3rd cervical vertebra with the help of muscles and ligaments. The hyoid bone consists of a central body and greater and lesser cornua.
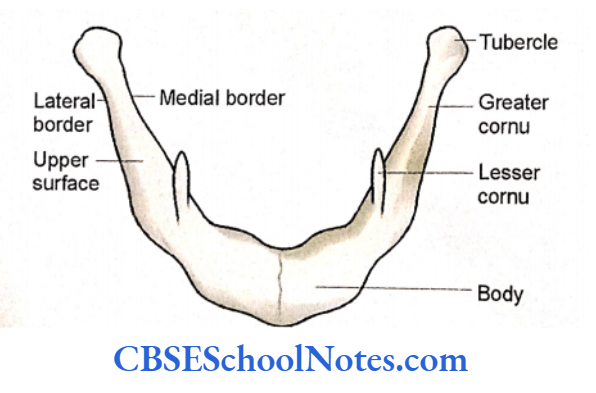
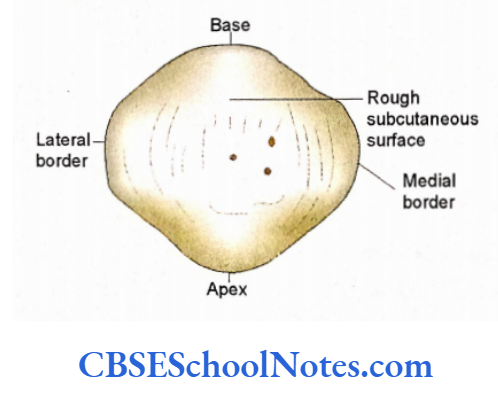
Hyoid Bone Body
The body is rectangular and has an anterior and a posterior surface.
The anterior surface is convex and faces anterosuperiorly. A median ridge divides it into right and left halves. The posterior surface is concave and smooth.
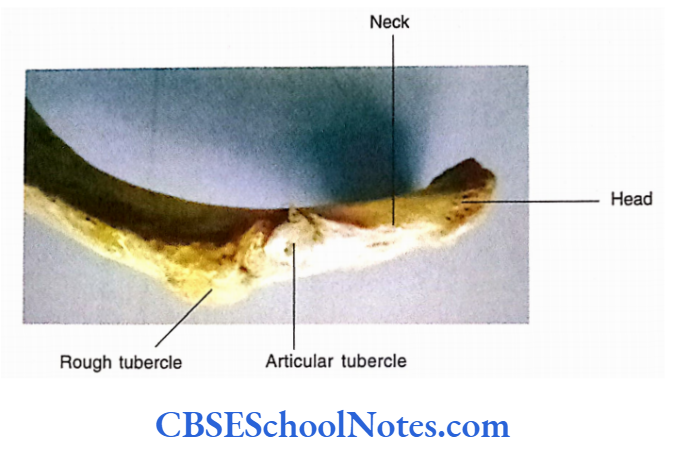
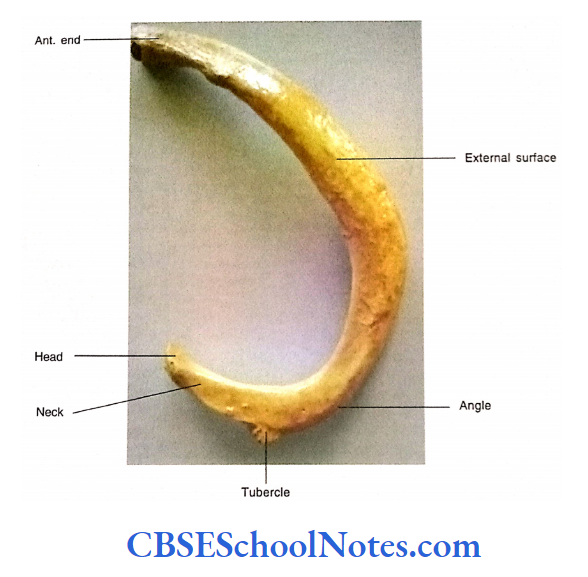
Hyoid Bone Greater Cornua
Each end of the body is continuous posterolaterally as greater cornu. The greater cornu is flattened. It has two surfaces (upper and lower) and two borders (medial and lateral). The posterior end of the greater cornu is enlarged to form a tubercle.
Hyoid Bone Lesser Cornua
The lesser cornua are small conical projections attached to the bone at the junction of the body and greater cornu on each side.
Each cornu projects upwards and laterally. The lesser cornu may form a synovial joint with the greater cornu.
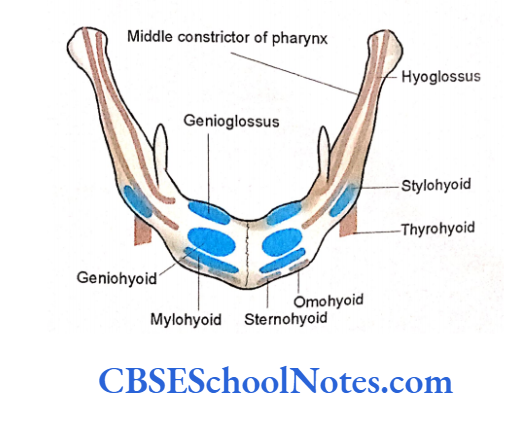
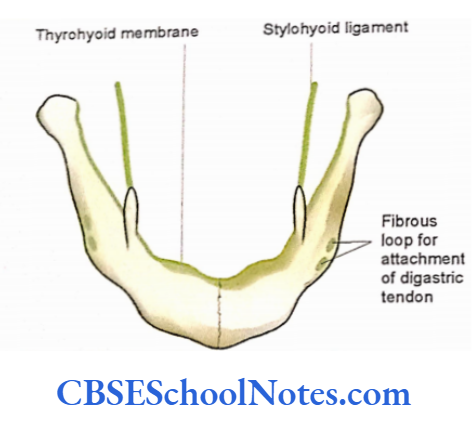
Hyoid Bone Particular Features
Attachments of muscles on the anterosuperior aspect are shown. Attachments of ligaments and membranes.
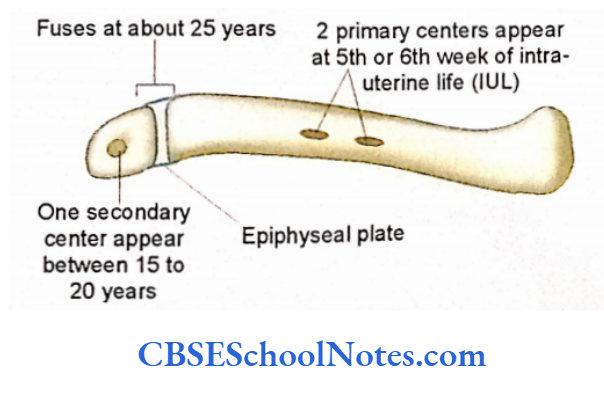
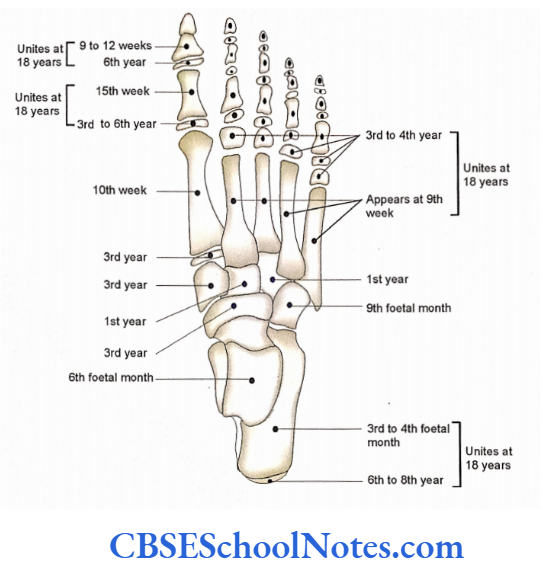
Hyoid Bone Ossification
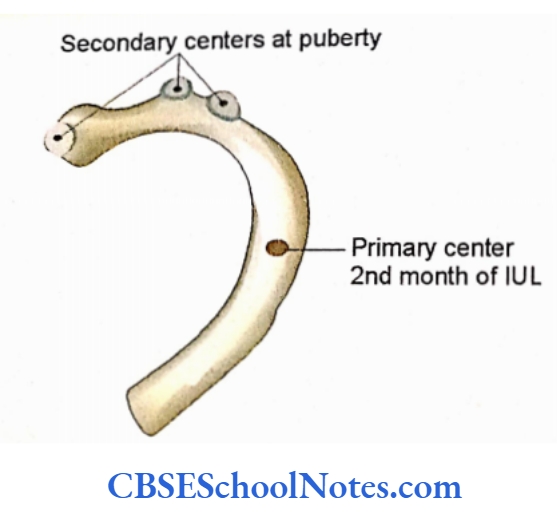
The hyoid bone ossifies in cartilage by six centers. One center appears in each greater cornua at the end of intrauterine life. Soon after birth two centers appear for the body. One center appears in each lesser cornua at puberty.
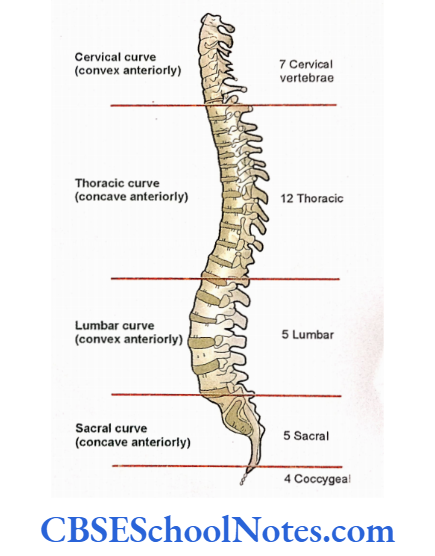
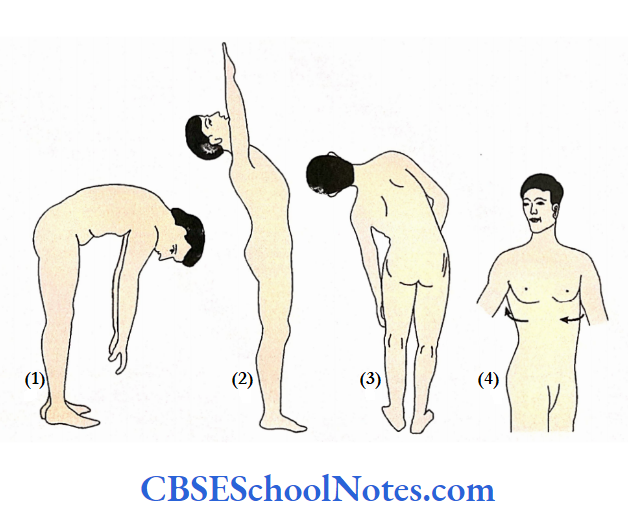
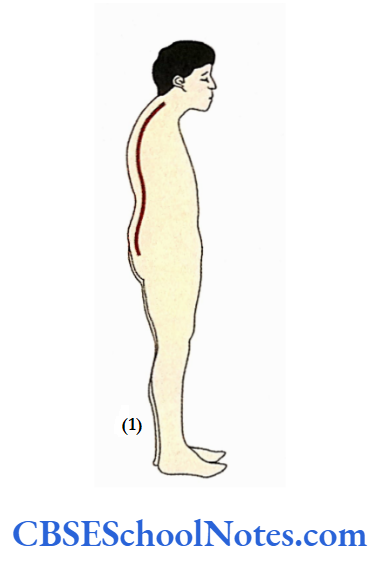
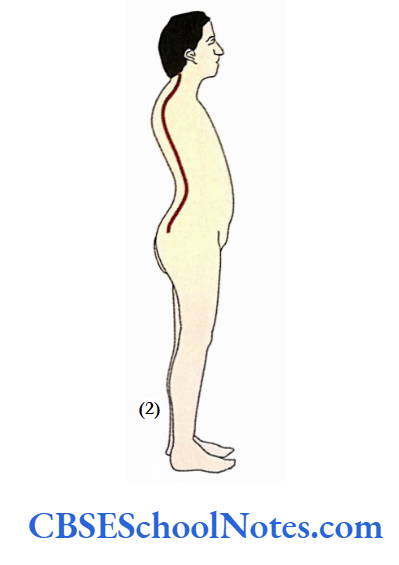
Cervical Vertebrae
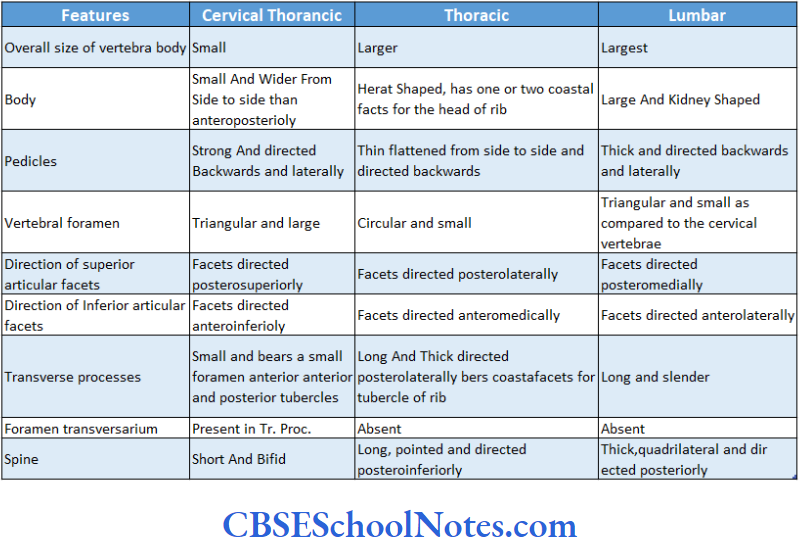
The cervical part of the vertebral column is highly mobile and its curvature is convex anteriorly. It is made up of 7 cervical vertebrae. A cervical vertebra is characteri¬ zed by the presence of a foramen in each transverse process (foramen transversarium). The 1st, 2nd, and 7th vertebrae are atypical, while 3rd to 6th vertebrae are typical.
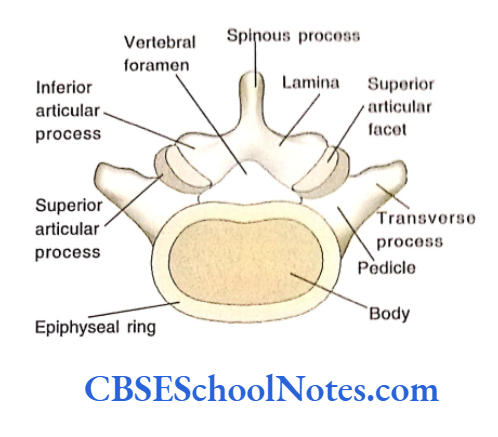
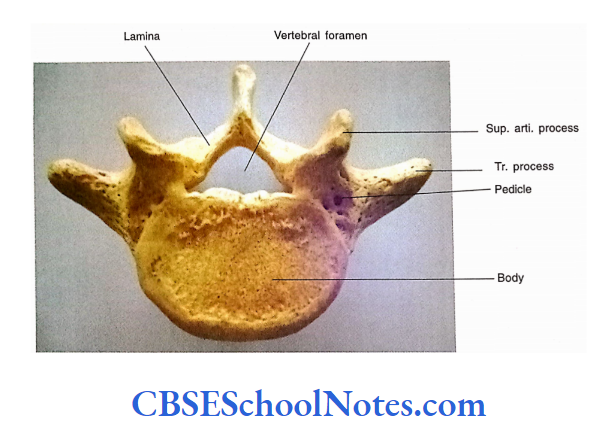
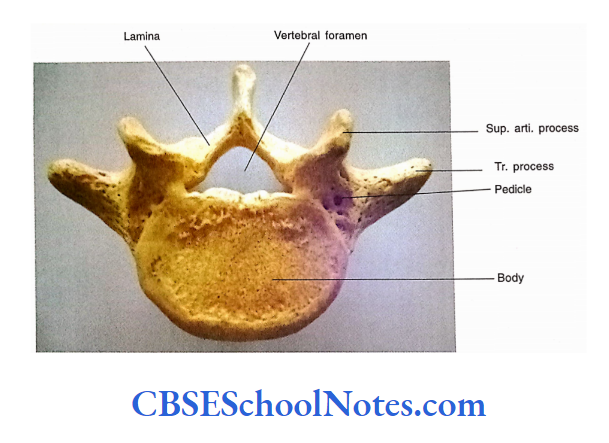
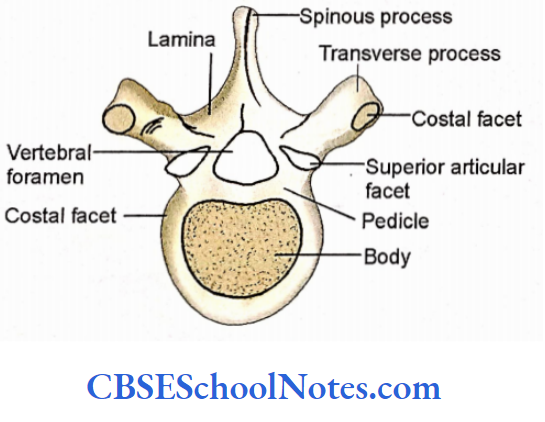
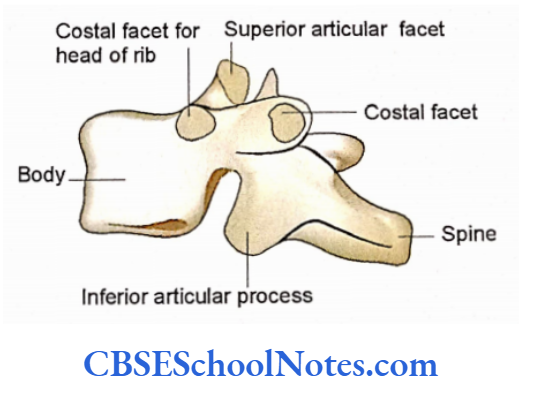
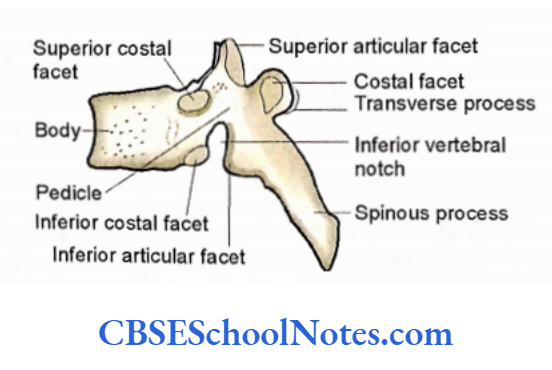
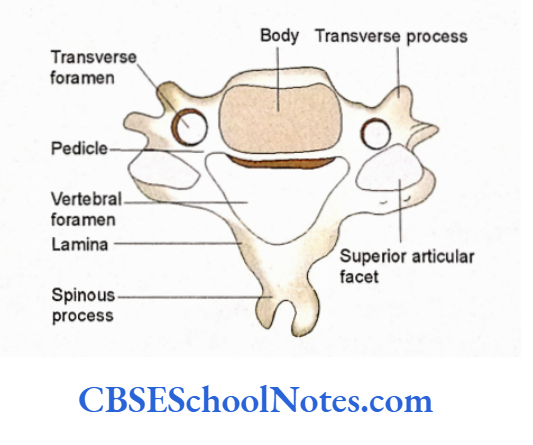
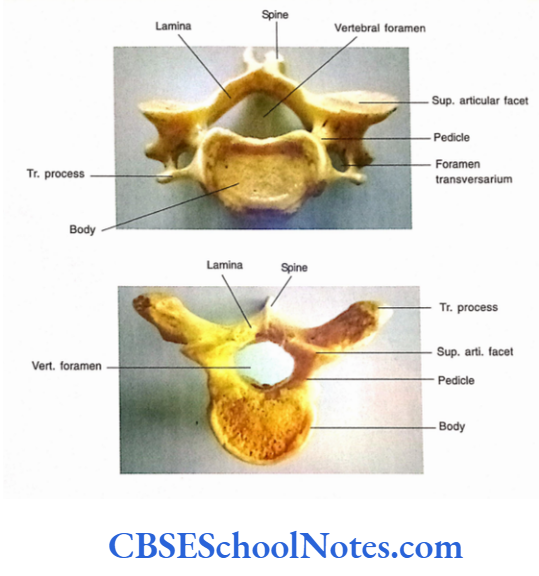
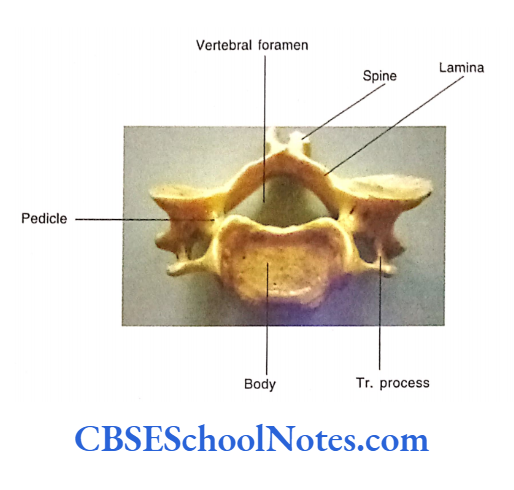
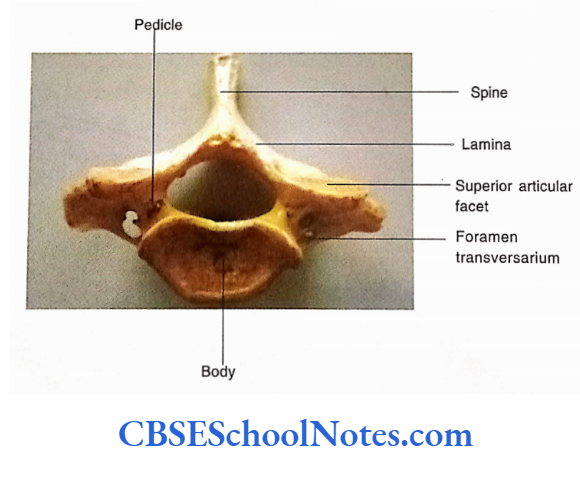
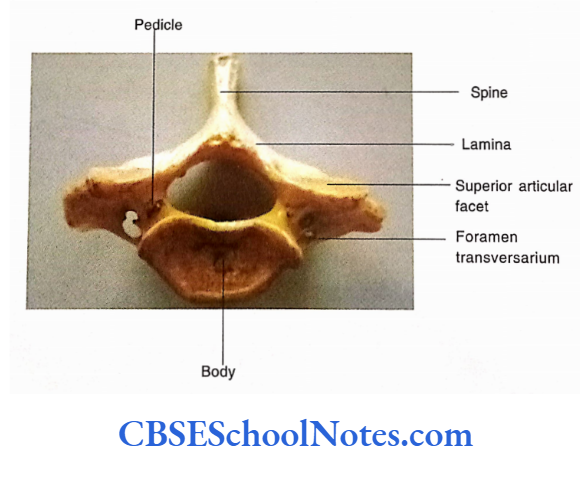
Typical Cervical Vertebrae
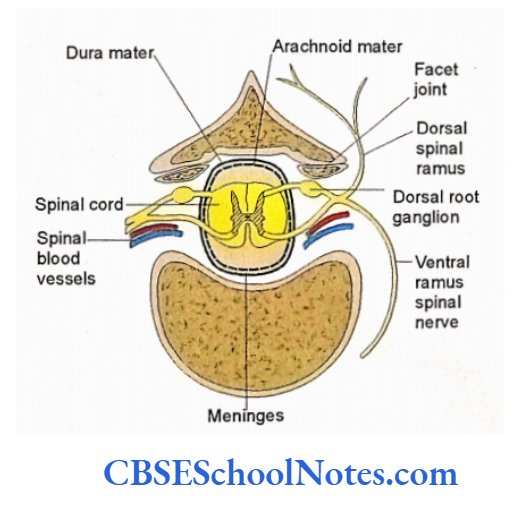
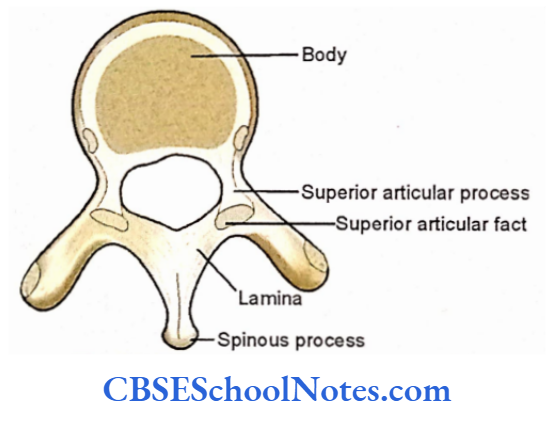
A typical cervical vertebra consists of a body and vertebral arch. The body and vertebral arch enclose a vertebral foramen, which lodges the spinal cord and its meninges.
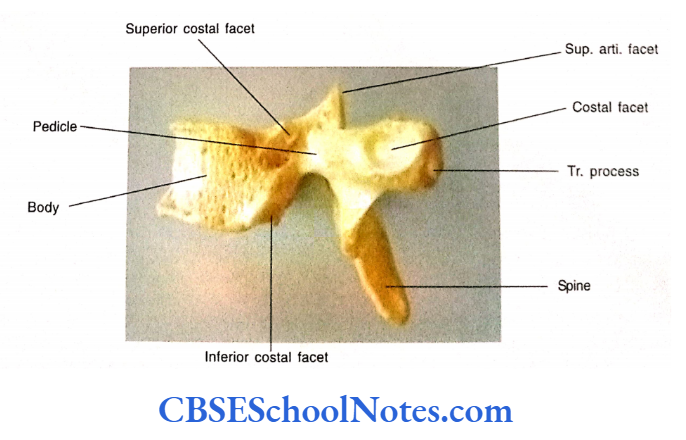
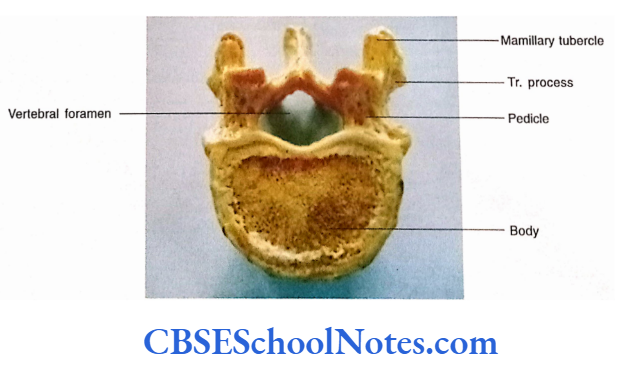
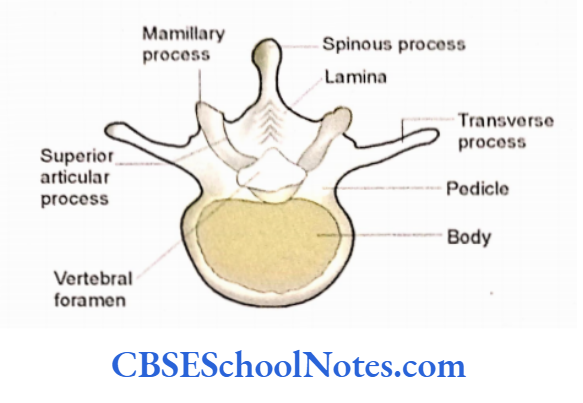
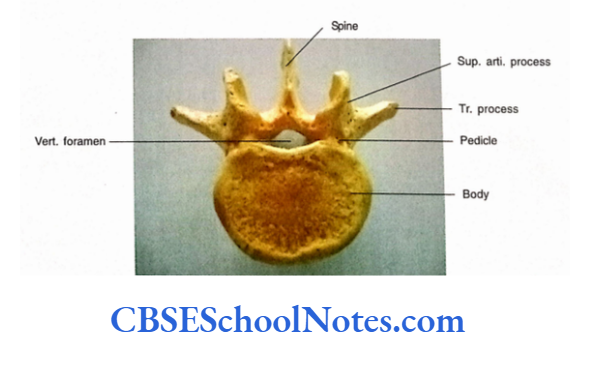
Cervical Vertebrae Body
- The body of the cervical vertebra is the smallest among all vertebrae. The shape of the cervical vertebra is oval, its anteroposterior diameter is less than side to side.
- The superior surface of the body is concave from side to side because of the presence of an upward-projecting lip on either side.
- The inferior surface is convex from side to side. The anterior border of the inferior surface projects downwards as a lip.
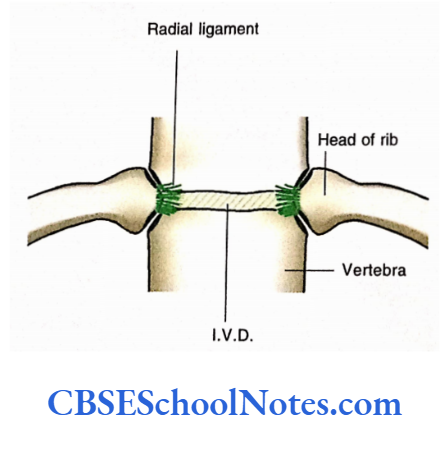
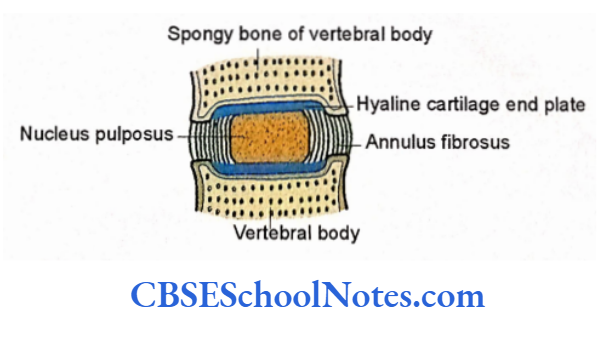
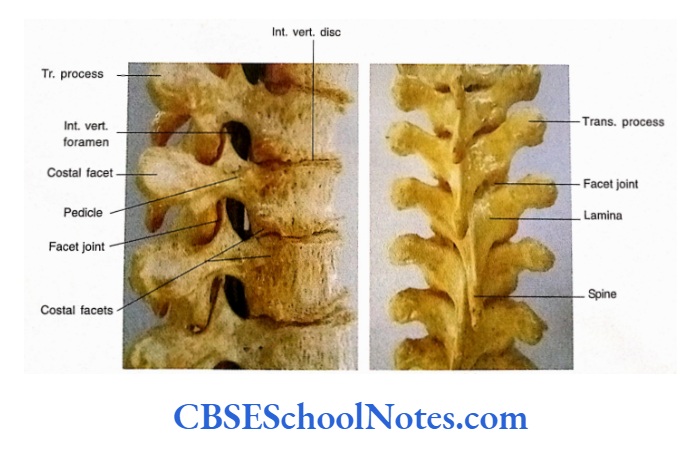
- The bodies of the adjacent vertebrae are connected by the intervertebral disc and a pair of synovial unconvertebral joints on each side of the disc.
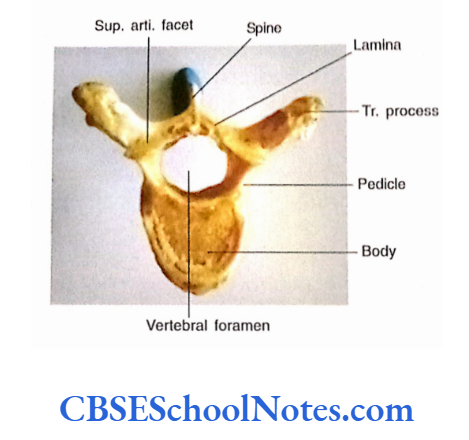
- The vertebral foramen is large and triangular.
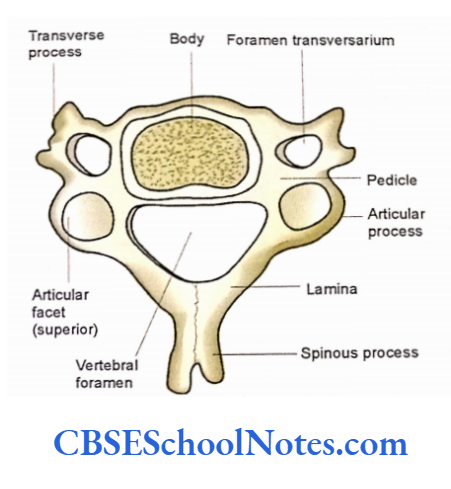
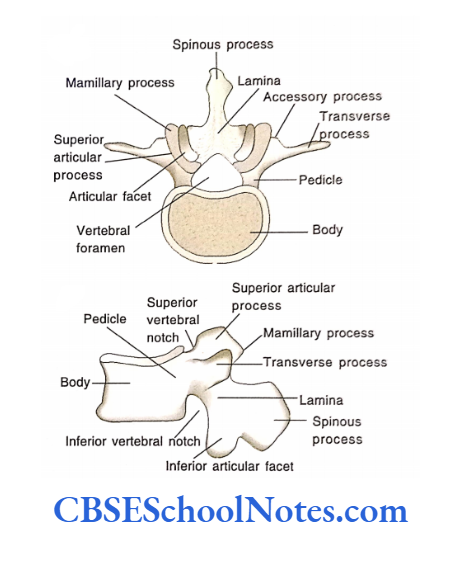
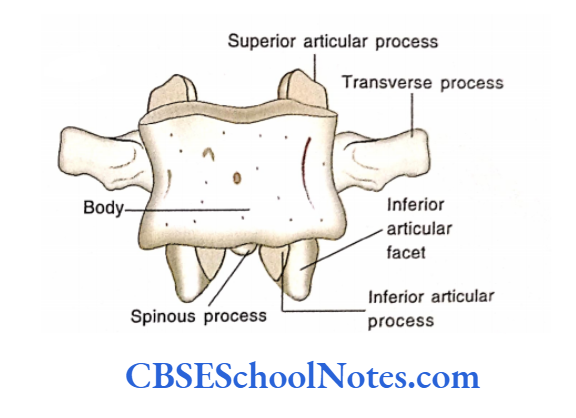
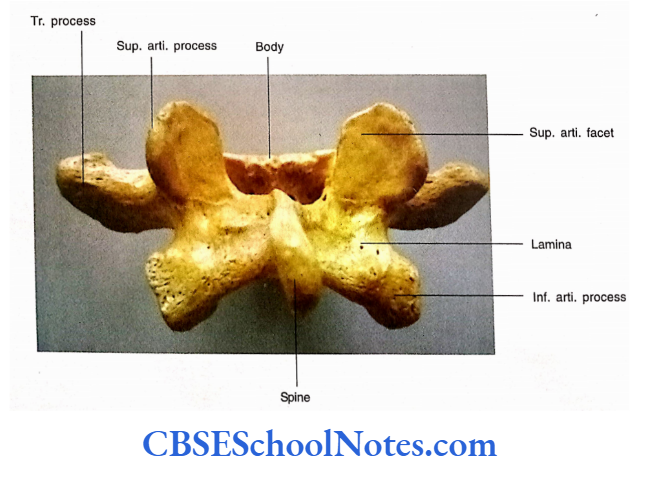
Vertebral Arch
It consists of pedicles, laminae, superior and inferior articular processes, transverse processes, and spine
Pedicles
These are rounded bars that arise from the posterolateral part of the body. They are directed backward and laterally hence, the vertebral foramen is large and triangular.
Lamina
Laminae are thin plates of bone. They are directed backward and medially from pedicles to meet each other in the midline at the base of the spinous process.
Spinous Process
It is short and bifid.
Articular Process
- The superior and inferior articular processes are present at the junction of pedicles and laminae and form a continuous articular pillar.
- The superior articular facet faces upwards and backward while the inferior facet faces downwards and forwards.
- The superior articular process articulates with the inferior articular process of the above vertebra.
- Between superior and inferior articular facets articular process is in the form of a bar and is known as an articular pillar.
- Besides bodies, the articular processes (articular pillar) also carry a considerable load on the head and neck.
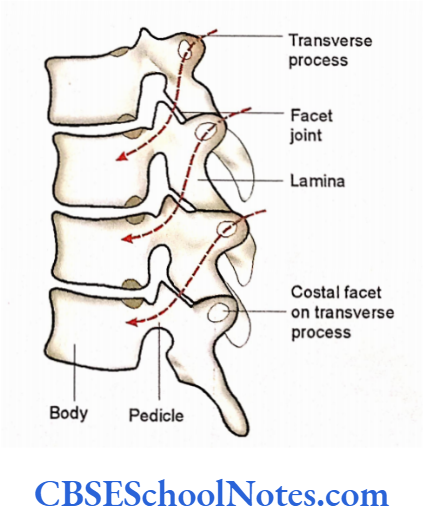
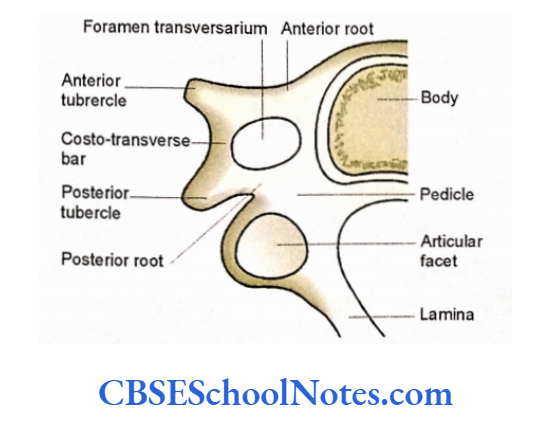
Transverse Processes
- These are short and directed laterally. Each transverse process bears a foramen transversarium.
- Each process presents anterior and posterior roots (anterior and posterior to the foramen), anterior and posterior tubercles (at the lateral end of anterior and posterior roots), and an intertubercular bar (costotransverse bar) which is present lateral to the foramen.
- The anterior root, anterior tubercle, intertubercular bar and posterior tubercle represent the costal element (element of rib). The posterior root represents the true transverse process.
- The foramen transversarium of the cervical vertebrae (except C7) transmits the vertebral artery, sympathetic nerve plexus, and vertebral vein.
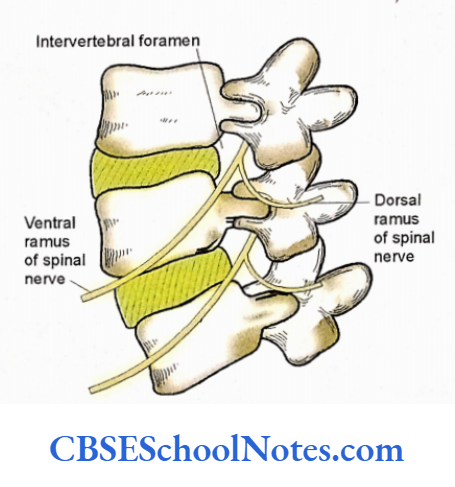
- The upper surface of the costotransverse bar is grooved and lodges the ventral ramus of the corresponding cervical nerve.
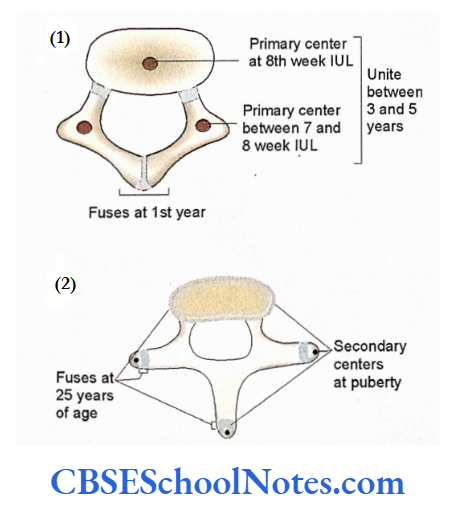
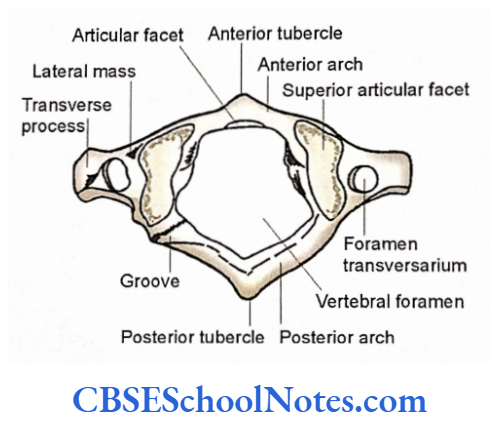
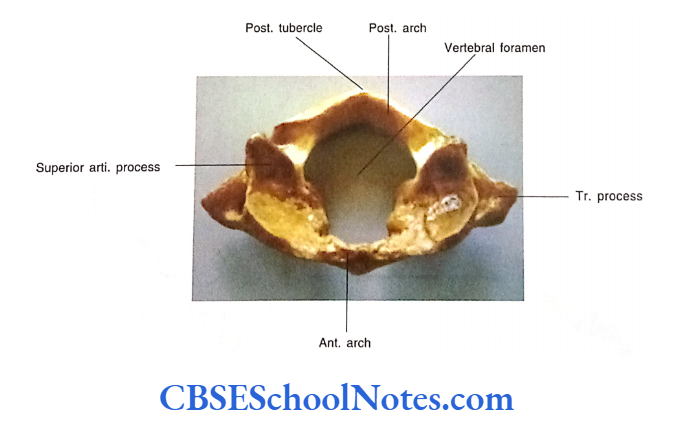
The First Cervical Vertebra
The first cervical vertebra is also known as the atlas.
It is easily identified from the rest of the other cervical vertebrae because:
- It is ring-shaped.
- It has nobody.
- It is the widest of all other cervical vertebrae.
- It has no spinous process.
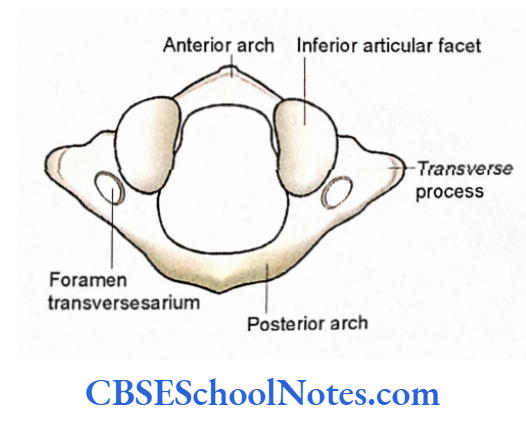
The bone has two large masses (lateral masses) joined anteriorly by a short anterior arch and joined posteriorly by a much longer posterior arch.
The superior surface of each lateral mass bears an elongated kidney-shaped concave articular facet for articulation with the occipital condyle (to form atlanto-occipital joint).
Anatomical Position
Hold the bone in such a way that the concave superior articular surface of the lateral masses faces upwards. The short anterior arch should face anteriorly.
General Features
Lateral Mass
- Each lateral mass has a superior articular facet and an inferior articular facet. The superior facet is concave and kidney-shaped. The inferior facet is oval and flat.
- The inferior facet faces downwards and medially and articulates with the superior articular surface of the axis (2nd cervical vertebra) to form the lateral atlantoaxial joint.
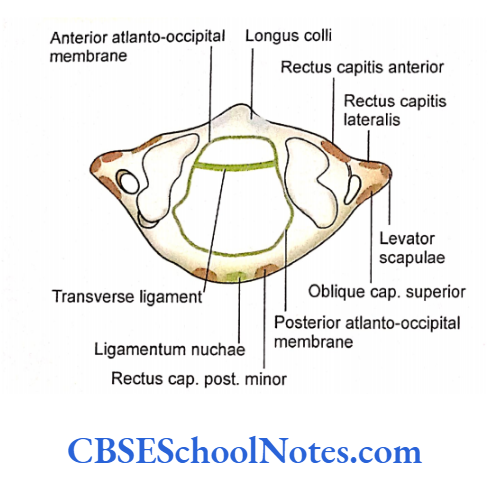
- The medial surface of each lateral mass bears a tubercle for the attachment of the transverse ligament of the atlas.
The Anterior Arch
- It shows the presence of a small anterior tubercle in the midline.
- An oval articular facet is present on the posterior surface in the midline. This facet articulates with the dens of the 2nd cervical vertebra to form the median atlantoaxial joint.
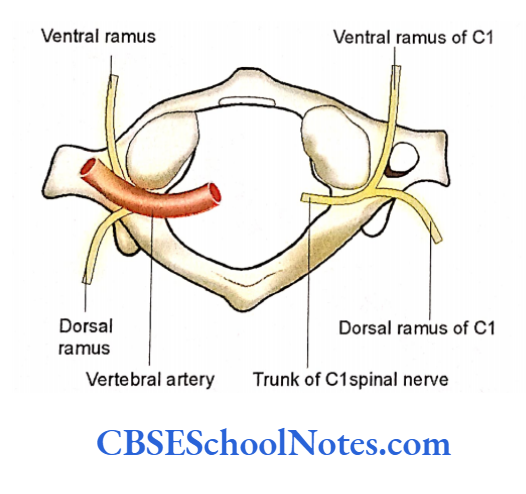
The Posterior Arch
- The posterior arch is much longer than the anterior and bears a posterior tubercle on its posterior surface in the midline. It represents the rudimentary spinous process.
- There is the presence of a shallow groove on its superior surface posterior to each lateral mass. The groove lodges the vertebral artery and the first cervical spinal nerve.
The Transverse Process
The transverse process projects laterally from the lateral mass. It has foramen transversarium which transmits vertebral artery, vein, and sympathetic nerve.
Particular Features
- Attachments of ligaments, membranes, and muscles.
- Relations of blood vessels and nerves are
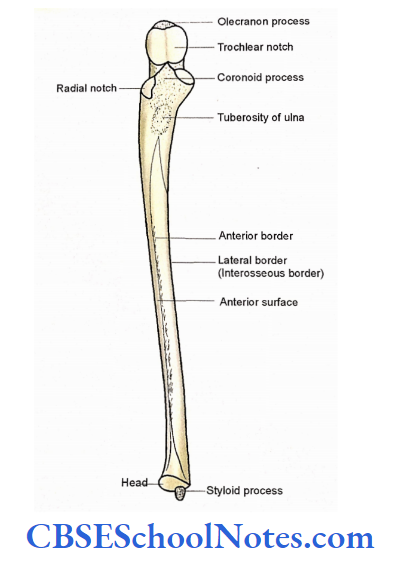
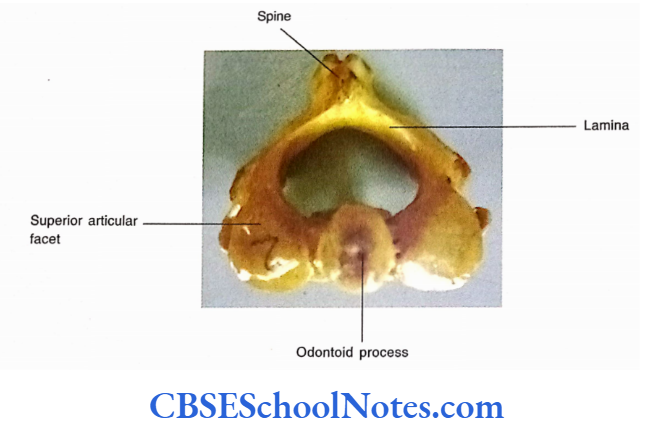
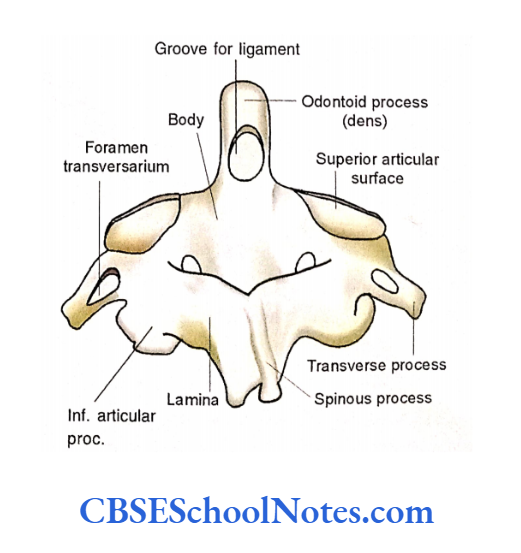
- The Second Cervical Vertebra proc.
- This vertebra is also known as the axis. It can be easily identified from the rest of the vertebrae because of the presence of dens or odontoid processes.
- The den is a blunt conical tooth-like process that projects superiorly from the body. The spinous process is long, strong, and bifid and projects posteriorly.
Anatomical Position
Hold the bone in such a way that the body of the vertebra lies anteriorly and the odontoid process faces upwards. The bifid spinous process should face posteriorly.
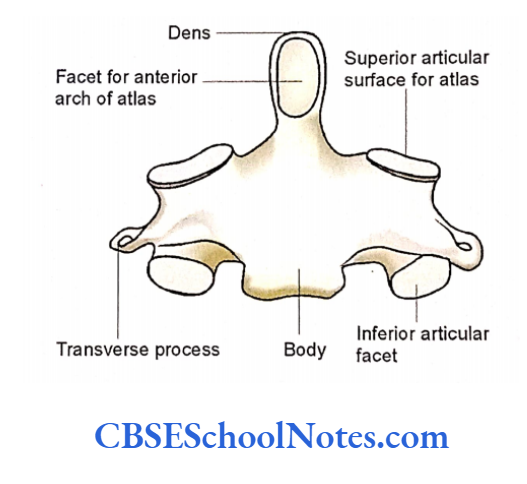
General Features
- The odontoid process is about 1.5 cm long. Its anterior surface bears a small oval facet for articulation with the anterior arch of the atlas. The posterior surface shows a groove, which lodges the transverse ligament of the atlas.
- The upper end of the body bears dens, while the lower surface articulates with the third cervical vertebra through the vertebral disc.
- Superior articular facets are situated lateral to the odontoid process. These are large oval facets, that articulate with the corresponding inferior facets of the atlas vertebra. Each facet is sloping and partly situated on the body and partly on the pedicle.
- The transverse processes are small and lie lateral to the superior articular facets.
- The pedicle, lamina, and spine are massive and very strong. The spine is bifid.
- The inferior articular process is present at the junction of the pedicle and lamina. Its articular facet faces downwards and forwards.
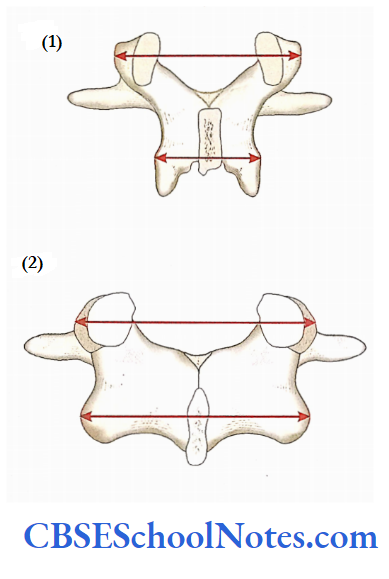
Seventh Cervical Vertebra
- This vertebra is easily identified from the other cervical vertebrae due to the presence of a very long, horizontal spinous process, which is not bifid (ends in a single tubercle).
- As the tip of the spinous process (tubercle) can be easily felt under the skin it is also called vertebra prominence. The transverse processes are large and have prominent posterior tubercles.
- The foramen transversarium is small because it does not provide passage to the vertebral artery. It transmits to the accessory vertebral vein only.